Concurrent Use of Renal Replacement Therapy during Extracorporeal Membrane Oxygenation Support: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Demographic Analysis
3.1.1. Observational Studies
3.1.2. RCT
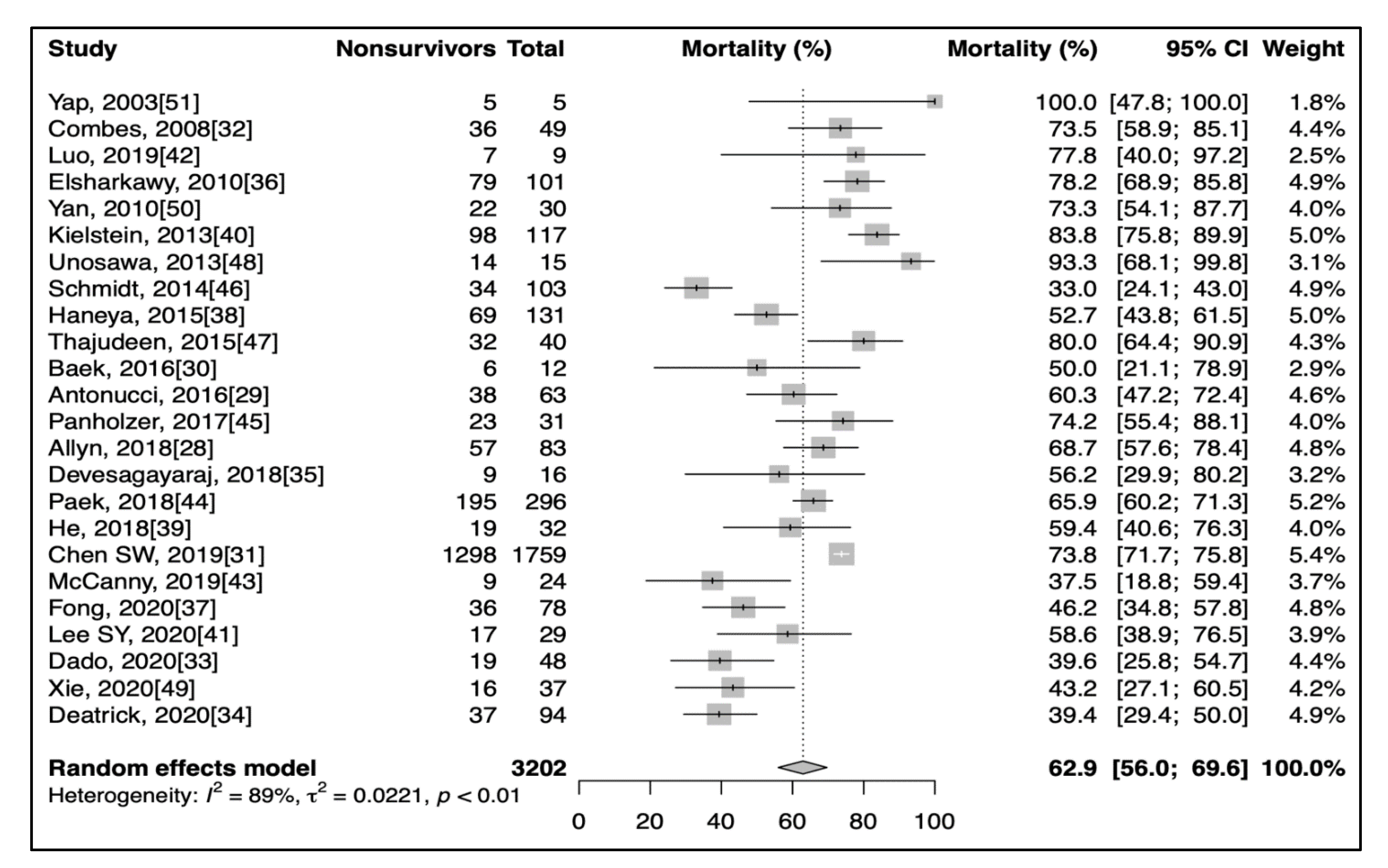
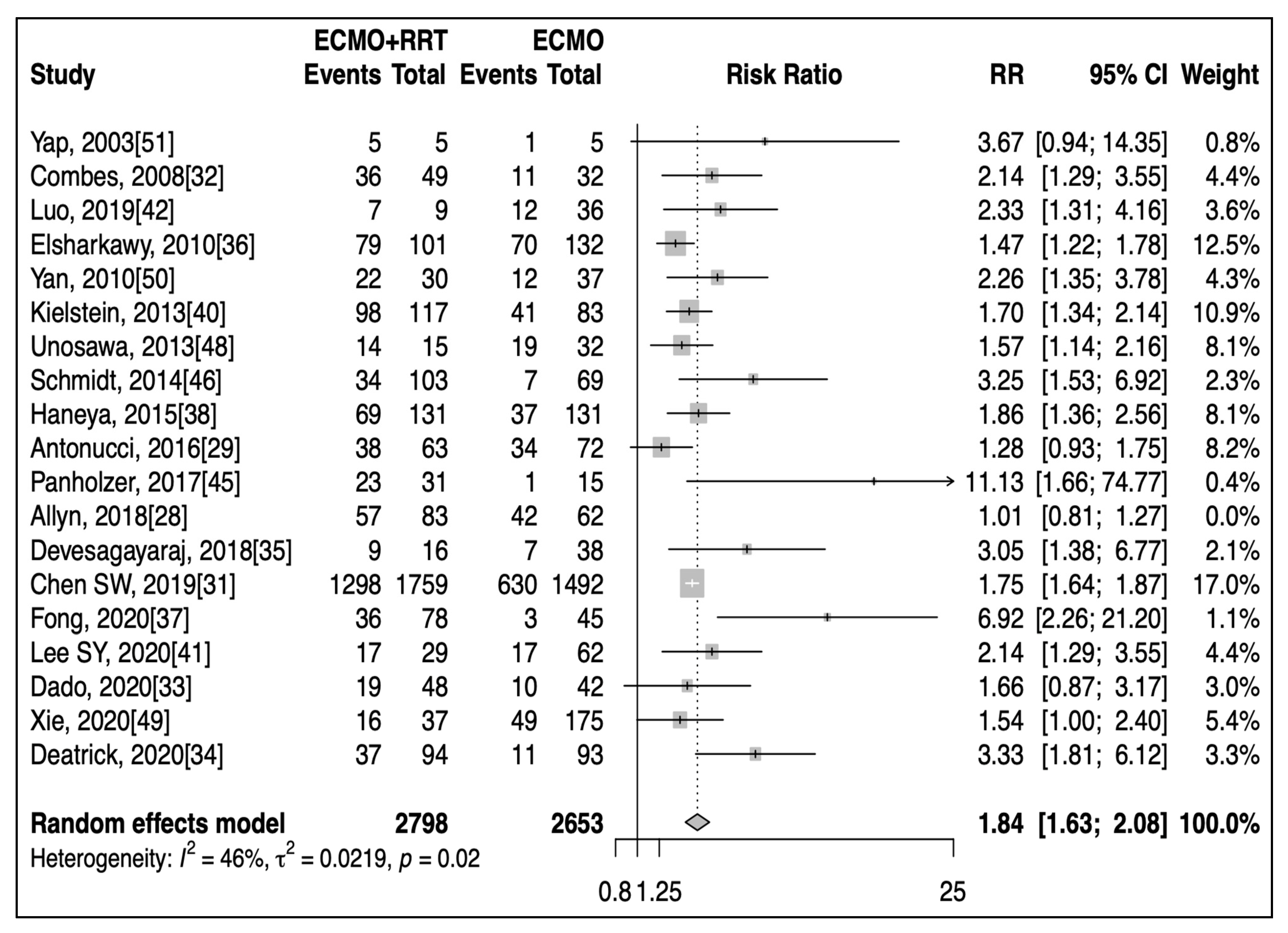
3.2. Primary Outcome
3.2.1. Observational Studies
3.2.2. RCT
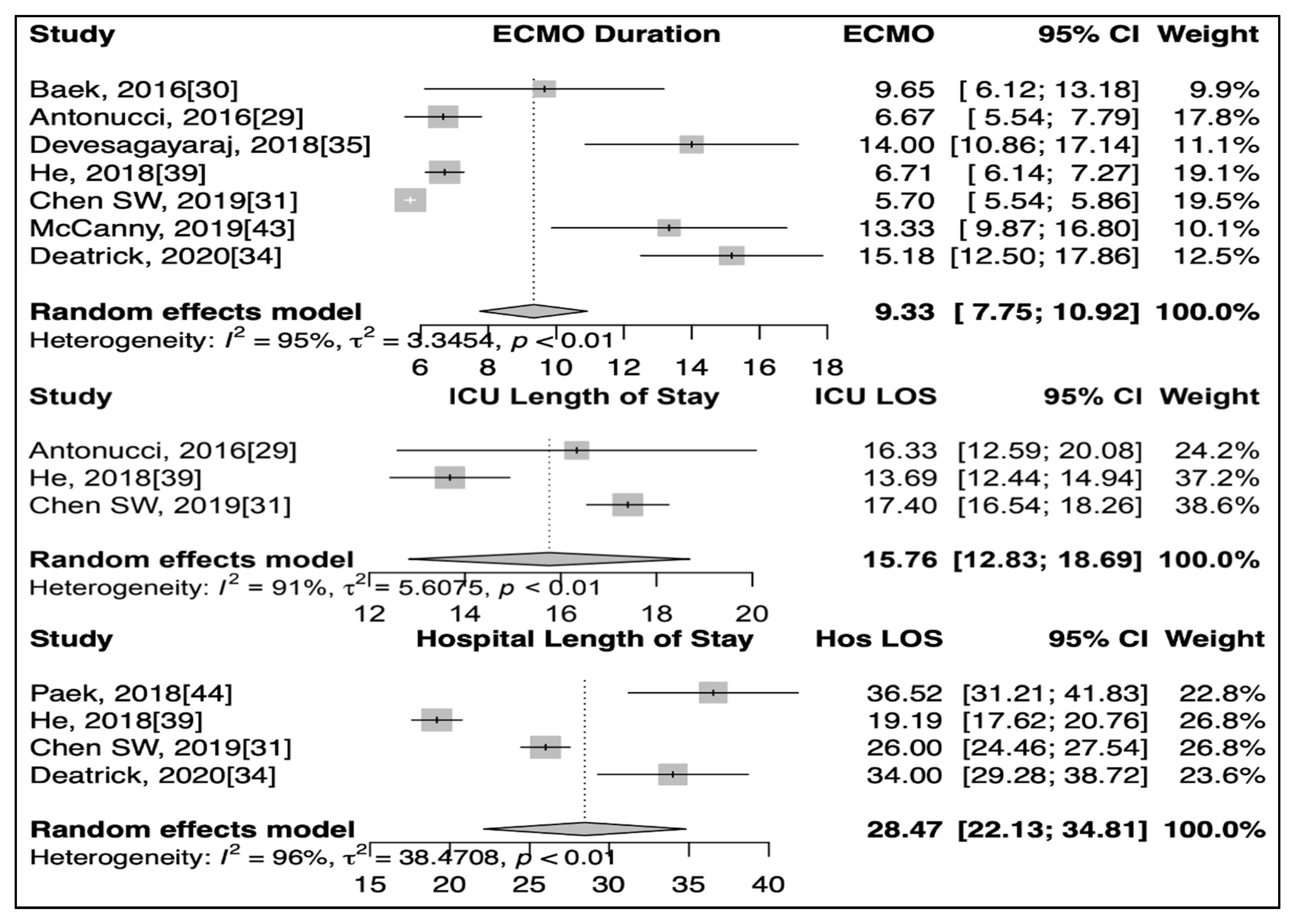
3.3. Secondary Outcomes
3.3.1. Observational Studies
3.3.2. RCT
3.4. Meta-Regression Analysis
3.5. Pre-ECMO Vs. Post-ECMO RRT
3.6. Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, Y.C.; Tsai, F.C.; Fang, J.T.; Yang, C.W. Acute kidney injury in adults receiving extracorporeal membrane oxygenation. J. Formos. Med. Assoc. 2014, 113, 778–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villa, G.; Katz, N.; Ronco, C. Extracorporeal Membrane Oxygenation and the Kidney. Cardiorenal. Med. 2015, 6, 50–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostermann, M.; Connor, M., Jr.; Kashani, K. Continuous renal replacement therapy during extracorporeal membrane oxygenation: Why, when and how? Curr. Opin. Crit. Care 2018, 24, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Millar, J.E.; Fanning, J.P.; McDonald, C.I.; McAuley, D.F.; Fraser, J.F. The inflammatory response to extracorporeal membrane oxygenation (ECMO): A review of the pathophysiology. Crit. Care 2016, 20, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hei, F.; Lou, S.; Li, J.; Yu, K.; Liu, J.; Feng, Z.; Zhao, J.; Hu, S.; Xu, J.; Chang, Q.; et al. Five-year results of 121 consecutive patients treated with extracorporeal membrane oxygenation at Fu Wai Hospital. Artif. Organs 2011, 35, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Kilburn, D.J.; Shekar, K.; Fraser, J.F. The Complex Relationship of Extracorporeal Membrane Oxygenation and Acute Kidney Injury: Causation or Association? BioMed Res. Int. 2016, 2016, 1094296. [Google Scholar] [CrossRef] [Green Version]
- Thiagarajan, R.R.; Barbaro, R.P.; Rycus, P.T.; Mcmullan, D.M.; Conrad, S.A.; Fortenberry, J.D.; Paden, M.L.; ELSO Member Centers. Extracorporeal Life Support Organization Registry International Report 2016. ASAIO J. 2017, 63, 60–67. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Laupland, K.B.; Doig, C.J.; Mortis, G.; Fick, G.H.; Mucenski, M.; Godinez-Luna, T.; Svenson, L.W.; Rosenal, T. Prognosis for long-term survival and renal recovery in critically ill patients with severe acute renal failure: A population-based study. Crit. Care 2005, 9, R700-9. [Google Scholar] [CrossRef] [Green Version]
- Vaara, S.T.; Korhonen, A.M.; Kaukonen, K.M.; Nisula, S.; Inkinen, O.; Hoppu, S.; Laurila, J.J.; Mildh, L.; Reinikainen, M.; Lund, V.; et al. Fluid overload is associated with an increased risk for 90-day mortality in critically ill patients with renal replacement therapy: Data from the prospective FINNAKI study. Crit. Care 2012, 16, R197. [Google Scholar] [CrossRef] [Green Version]
- Doll, N.; Kiaii, B.; Borger, M.; Bucerius, J.; Krämer, K.; Schmitt, D.V.; Walther, T.; Mohr, F.W. Five-year Results of 219 Consecutive Patients Treated with Extracorporeal Membrane Oxygenation for Refractory Postoperative Cardiogenic Shock. Ann. Thorac. Surg. 2004, 77, 151–157; discussion 157. [Google Scholar] [CrossRef]
- Smedira, N.G.; Moazami, N.; Golding, C.M.; McCarthy, P.M.; Apperson-Hansen, C.; Blackstone, E.H.; Cosgrove, D.M., 3rd. Clinical Experience with 202 Adults Receiving Extracorporeal Membrane Oxygenation for Cardiac Failure: Survival at Five Years. J. Thorac. Cardiovasc. Surg. 2001, 122, 92–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, C.C.; Chang, C.H.; Fan, P.C.; Ho, H.T.; Jenq, C.C.; Kao, K.C.; Chiu, L.C.; Lee, S.Y.; Hsu, H.H.; Tian, Y.C.; et al. Prognosis of Patients with Acute Respiratory Distress Syndrome on Extracorporeal Membrane Oxygenation: The Impact of Urine Output on Mortality. Ann. Thorac. Surg. 2014, 97, 1939–1944. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Paek, J.H.; Song, J.H.; Lee, H.; Jhee, J.H.; Park, S.; Yun, H.R.; Kee, Y.K.; Han, S.H.; Yoo, T.H.; et al. Permissive fluid volume in adult patients undergoing extracorporeal membrane oxygenation treatment. Crit. Care 2018, 22, 270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramanathan, K.; Tan, C.S.; Rycus, P.; MacLaren, G. Extracorporeal membrane oxygenation for poisoning in adult patients: Outcomes and predictors of mortality. Intensive Care Med. 2017, 43, 1538–1539. [Google Scholar] [CrossRef] [PubMed]
- De Lange, D.W.; Sikma, M.A.; Meulenbelt, J. Extracorporeal membrane oxygenation in the treatment of poisoned patients. Clin. Toxicol. 2013, 51, 385–393. [Google Scholar] [CrossRef]
- Chen, H.; Yu, R.G.; Yin, N.N.; Zhou, J.X. Combination of extracorporeal membrane oxygenation and continuous renal replacement therapy in critically ill patients: A systematic review. Crit. Care 2014, 18, 675. [Google Scholar] [CrossRef] [Green Version]
- Han, S.S.; Kim, H.J.; Lee, S.J.; Kim, W.J.; Hong, Y.; Lee, H.Y.; Song, S.Y.; Jung, H.H.; Ahn, H.S.; Ahn, I.M.; et al. Effects of Renal Replacement Therapy in Patients Receiving Extracorporeal Membrane Oxygenation: A Meta-Analysis. Ann. Thorac. Surg. 2015, 100, 1485–1495. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.J.Y.; Ong, J.A.; Syn, N.L.; Lorusso, R.; Tan, C.S.; MacLaren, G.; Ramanathan, K. Extracorporeal Membrane Oxygenation in Pregnant and Postpartum Women: A Systematic Review and Meta-Regression Analysis. J. Intensive Care Med. 2019. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Clopper, C.J.; Pearson, E.S. The Use of Confidence or Fiducial Limits Illustrated in the Case of the Binomial. Biometrika 1934, 26, 404–413. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence--inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Iorio, A.; Spencer, F.A.; Falavigna, M.; Alba, C.; Lang, E.; Burnand, B.; McGinn, T.; Hayden, J.; Williams, K.; Shea, B.; et al. Use of GRADE for assessment of evidence about prognosis: Rating confidence in estimates of event rates in broad categories of patients. BMJ 2015, 350, h870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GRADEpro App. Available online: https://www.gradepro.org (accessed on 10 October 2020).
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Santesso, N.; Carrasco-Labra, A.; Langendam, M.; Brignardello-Petersen, R.; Mustafa, R.A.; Heus, P.; Lasserson, T.; Opiyo, N.; Kunnamo, I.; Sinclair, D.; et al. Improving GRADE evidence tables part 3: Detailed guidance for explanatory footnotes supports creating and understanding GRADE certainty in the evidence judgments. J. Clin. Epidemiol. 2016, 74, 28–39. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Allyn, J.; Ferdynus, C.; Lo Pinto, H.; Bouchet, B.; Persichini, R.; Vandroux, D.; Puech, B.; Allou, N. Complication patterns in patients undergoing venoarterial extracorporeal membrane oxygenation in intensive care unit: Multiple correspondence analysis and hierarchical ascendant classification. PLoS ONE 2018, 13, e0203643. [Google Scholar] [CrossRef]
- Antonucci, E.; Lamanna, I.; Fagnoul, D.; Vincent, J.L.; De Backer, D.; Silvio Taccone, F. The Impact of Renal Failure and Renal Replacement Therapy on Outcome During Extracorporeal Membrane Oxygenation Therapy. Artif. Organs 2016, 40, 746–754. [Google Scholar] [CrossRef]
- Baek, J.K.; Lee, J.S.; Kim, T.H.; Kim, Y.H.; Han, D.J.; Hong, S.K. Four-Year Experience With Extracorporeal Membrane Oxygenation for Kidney Transplant Patients With Severe Refractory Cardiopulmonary Insufficiency. Transplant. Proc. 2016, 48, 2080–2083. [Google Scholar] [CrossRef]
- Chen, S.W.; Lu, Y.A.; Lee, C.C.; Chou, A.H.; Wu, V.C.; Chang, S.W.; Fan, P.C.; Tian, Y.C.; Tsai, F.C.; Chang, C.H. Long-term outcomes after extracorporeal membrane oxygenation in patients with dialysis-requiring acute kidney injury: A cohort study. PLoS ONE 2019, 14, e0212352. [Google Scholar] [CrossRef] [Green Version]
- Combes, A.; Leprince, P.; Luyt, C.E.; Bonnet, N.; Trouillet, J.L.; Léger, P.; Pavie, A.; Chastre, J. Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit. Care Med. 2008, 36, 1404–1411. [Google Scholar] [CrossRef] [PubMed]
- Dado, D.N.; Ainsworth, C.R.; Thomas, S.B.; Huang, B.; Piper, L.C.; Sams, V.G.; Batchinsky, A.; Morrow, B.D.; Basel, A.P.; Walter, R.J.; et al. Outcomes among Patients Treated with Renal Replacement Therapy during Extracorporeal Membrane Oxygenation: A Single-Center Retrospective Study. Blood Purif. 2020, 49, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Deatrick, K.B.; Mazzeffi, M.A.; Galvagno, S.M., Jr.; Boswell, K.; Kaczoroswki, D.J.; Rabinowitz, R.P.; Madathil, R.J.; Cornachione, C.R.; Herr, D.L.; Scalea, T.M.; et al. Breathing Life Back Into the Kidney-Continuous Renal Replacement Therapy and Veno-Venous Extracorporeal Membrane Oxygenation. ASAIO J. 2020. [Google Scholar] [CrossRef]
- Devasagayaraj, R.; Cavarocchi, N.C.; Hirose, H. Does acute kidney injury affect survival in adults with acute respiratory distress syndrome requiring extracorporeal membrane oxygenation? Perfusion 2018, 33, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Elsharkawy, H.A.; Li, L.; Esa, W.A.; Sessler, D.I.; Bashour, C.A. Outcome in patients who require venoarterial extracorporeal membrane oxygenation support after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2010, 24, 946–951. [Google Scholar] [CrossRef] [Green Version]
- Fong, K.M.; Au, S.Y.; Ng, G.W.Y.; Leung, A.K.H. Positive fluid balance and mortality in adult patients treated with extracorporeal membrane oxygenation: A retrospective study. J. Intensive Care Soc. 2020, 21, 210–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haneya, A.; Diez, C.; Philipp, A.; Bein, T.; Mueller, T.; Schmid, C.; Lubnow, M. Impact of Acute Kidney Injury on Outcome in Patients With Severe Acute Respiratory Failure Receiving Extracorporeal Membrane Oxygenation. Crit. Care Med. 2015, 43, 1898–1906. [Google Scholar] [CrossRef]
- He, P.; Zhang, S.; Hu, B.; Wu, W. Retrospective study on the effects of the prognosis of patients treated with extracorporeal membrane oxygenation combined with continuous renal replacement therapy. Ann. Transl. Med. 2018, 6, 455. [Google Scholar] [CrossRef]
- Kielstein, J.T.; Heiden, A.M.; Beutel, G.; Gottlieb, J.; Wiesner, O.; Hafer, C.; Hadem, J.; Reising, A.; Haverich, A.; Kühn, C.; et al. Renal function and survival in 200 patients undergoing ECMO therapy. Nephrol. Dial. Transplant. 2013, 28, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Jeon, K.H.; Lee, H.J.; Kim, J.B.; Jang, H.J.; Kim, J.S.; Kim, T.H.; Park, J.S.; Choi, R.K.; Choi, Y.J. Complications of veno-arterial extracorporeal membrane oxygenation for refractory cardiogenic shock or cardiac arrest. Int. J. Artif. Organs 2020, 43, 37–44. [Google Scholar] [CrossRef]
- Luo, X.J.; Wang, W.; Hu, S.S.; Sun, H.S.; Gao, H.W.; Long, C.; Song, Y.H.; Xu, J.P. Extracorporeal membrane oxygenation for treatment of cardiac failure in adult patients. Interact. Cardiovasc. Thorac. Surg. 2009, 9, 296–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCanny, P.; Smith, M.W.; O’Brien, S.G.; Buscher, H.; Carton, E.G. Fluid Balance and Recovery of Native Lung Function in Adult Patients Supported by Venovenous Extracorporeal Membrane Oxygenation and Continuous Renal Replacement Therapy. ASAIO J. 2019, 65, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Paek, J.H.; Park, S.; Lee, A.; Park, S.; Chin, H.J.; Na, K.Y.; Lee, H.; Park, J.T.; Kim, S. Timing for initiation of sequential continuous renal replacement therapy in patients on extracorporeal membrane oxygenation. Kidney Res. Clin. Pract. 2018, 37, 239–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panholzer, B.; Meckelburg, K.; Huenges, K.; Hoffmann, G.; von der Brelie, M.; Haake, N.; Pilarczyk, K.; Cremer, J.; Haneya, A. Extracorporeal membrane oxygenation for acute respiratory distress syndrome in adults: An analysis of differences between survivors and non-survivors. Perfusion 2017, 32, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Bailey, M.; Kelly, J.; Hodgson, C.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V.; Bellomo, R.; Pilcher, D. Impact of fluid balance on outcome of adult patients treated with extracorporeal membrane oxygenation. Intensive Care Med. 2014, 40, 1256–1266. [Google Scholar] [CrossRef]
- Thajudeen, B.; Kamel, M.; Arumugam, C.; Ali, S.A.; John, S.G.; Meister, E.E.; Mosier, J.M.; Raz, Y.; Madhrira, M.; Thompson, J.; et al. Outcome of patients on combined extracorporeal membrane oxygenation and continuous renal replacement therapy: A retrospective study. Int. J. Artif. Organs 2015, 38, 133–137. [Google Scholar] [CrossRef]
- Unosawa, S.; Sezai, A.; Hata, M.; Nakata, K.; Yoshitake, I.; Wakui, S.; Kimura, H.; Takahashi, K.; Hata, H.; Shiono, M. Long-term outcomes of patients undergoing extracorporeal membrane oxygenation for refractory postcardiotomy cardiogenic shock. Surg. Today 2013, 43, 264–270. [Google Scholar] [CrossRef]
- Xie, H.; Yang, F.; Hou, D.; Wang, X.; Wang, L.; Wang, H.; Hou, X. Risk factors of in-hospital mortality in adult postcardiotomy cardiogenic shock patients successfully weaned from venoarterial extracorporeal membrane oxygenation. Perfusion 2020, 35, 417–426. [Google Scholar] [CrossRef]
- Yan, X.; Jia, S.; Meng, X.; Dong, P.; Jia, M.; Wan, J.; Hou, X. Acute kidney injury in adult postcardiotomy patients with extracorporeal membrane oxygenation: Evaluation of the RIFLE classification and the Acute Kidney Injury Network criteria. Eur. J. Cardiothorac. Surg. 2010, 37, 334–338. [Google Scholar] [CrossRef]
- Yap, H.J.; Chen, Y.C.; Fang, J.T.; Huang, C.C. Combination of continuous renal replacement therapies (CRRT) and extracorporeal membrane oxygenation (ECMO) for advanced cardiac patients. Ren. Fail. 2003, 25, 183–193. [Google Scholar] [CrossRef]
- Li, C.; Wang, H.; Liu, N.; Jia, M.; Hou, X. The Effect of Simultaneous Renal Replacement Therapy on Extracorporeal Membrane Oxygenation Support for Postcardiotomy Patients with Cardiogenic Shock: A Pilot Randomized Controlled Trial. J. Cardiothorac. Vasc. Anesth. 2019, 33, 3063–3072. [Google Scholar] [CrossRef] [PubMed]
- Pappalardo, F.; Montisci, A. Veno-arterial extracorporeal membrane oxygenation (VA ECMO) in postcardiotomy cardiogenic shock: How much pump flow is enough? J. Thorac. Dis. 2016, 8, E1444–E1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Summary, ECLS Registry Report. July 2020. Available online: https://www.elso.org/registry/statistics/InternationalSummary.aspx (accessed on 15 November 2020).
- Mohan, B.; Singh, B.; Gupta, V.; Ralhan, S.; Gupta, D.; Puri, S.; Goyal, A.; Aslam, N.; Tandon, R.; Wander, G.S. Outcome of patients supported by extracorporeal membrane oxygenation for aluminum phosphide poisoning: An observational study. Indian Heart J. 2016, 68, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorusso, R.; Centofanti, P.; Gelsomino, S.; Barili, F.; Di Mauro, M.; Orlando, P.; Botta, L.; Milazzo, F.; Actis Dato, G.; Casabona, R. Venoarterial Extracorporeal Membrane Oxygenation for Acute Fulminant Myocarditis in Adult Patients: A 5-Year Multi-Institutional Experience. Ann. Thorac. Surg. 2016, 101, 919–926. [Google Scholar] [CrossRef] [Green Version]
- Shintani, A.K.; Girard, T.D.; Eden, S.K.; Arbogast, P.G.; Moons, K.G.; Ely, E.W. Immortal time bias in critical care research: Application of time-varying Cox regression for observational cohort studies. Crit. Care Med. 2009, 37, 2939–2945. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Lertjitbanjong, P.; Aeddula, N.R.; Bathini, T.; Watthanasuntorn, K.; Srivali, N.; Mao, M.A.; Kashani, K. Incidence and Impact of Acute Kidney Injury in Patients Receiving Extracorporeal Membrane Oxygenation: A Meta-Analysis. J. Clin. Med. 2019, 8, 981. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Outcome | ||||||
|---|---|---|---|---|---|---|
| Author/Year | Study Type, Sample Size | Country | ECMO/RRT | Mortality | ICU/Hospital LOS | ECMO Duration |
| Allyn, 2018 [28] | Cohort, 145 | France | + | + | −/− | − |
| Antonucci, 2016 [29] | Cohort, 135 | Belgium | + | + | +/− | + |
| Baek, 2016 [30] | Cohort, 12 | Korea | + | + | −/− | + |
| Chen, 2019 [31] | Cohort, 3251 | Taiwan | + | + | +/+ | + |
| Combes, 2008 [32] | Cohort, 81 | France | + | + | −/− | − |
| Dado, 2020 [33] | Cohort, 90 | USA | + | + | −/− | − |
| Deatrick, 2020 [34] | Cohort, 187 | USA | + | + | −/+ | + |
| Devasagayaraj, 2018 [35] | Cohort, 54 | USA | + | + | −/− | + |
| Elsharkawy, 2010 [36] | Cohort, 233 | USA | + | + | −/− | − |
| Fong, 2020 [37] | Cohort, 123 | HK SAR | + | + | −/− | − |
| Haneya, 2015 [38] | Cohort, 262 | Germany | + | + | −/− | − |
| He, 2018 [39] | Cohort, 32 | China | + | + | +/+ | + |
| Kielstein, 2013 [40] | Cohort, 200 | Germany | + | + | −/− | − |
| Lee SY, 2020 [41] | Cohort, 91 | Korea | + | + | −/− | − |
| Luo, 2009 [42] | Cohort, 45 | China | + | + | −/− | − |
| McCanny, 2019 [43] | Cohort, 24 | Ireland | + | + | −/− | + |
| Paek, 2018 [44] | Cohort, 296 | Korea | + | + | −/+ | − |
| Panholzer, 2017 [45]. | Cohort, 46 | Germany | + | + | −/− | − |
| Schmidt, 2014 [46] | Cohort, 172 | Australia | + | + | −/− | − |
| Thajudeen, 2015 [47] | Cohort, 40 | USA | + | + | −/− | − |
| Unosawa, 2013 [48] | Cohort, 47 | Japan | + | + | −/− | − |
| Xie, 2020 [49] | Cohort, 212 | China | + | + | −/− | − |
| Yan, 2010 [50] | Cohort, 67 | China | + | + | −/− | − |
| Yap, 2003 [51] | Case-control, 10 | Taiwan | + | + | −/− | − |
| Li, 2019 [52] | RCT, 41 | China | + | + | +/+ | + |
| Covariates | Studies | Odds Ratio | Lower CI | Upper CI | p Value |
|---|---|---|---|---|---|
| VA-ECMO | 24 | 1.23 | 1.04 | 1.46 | 0.02 |
| ECMO duration | 7 | 0.97 | 0.95 | 0.98 | <0.001 |
| Lactate | 7 | 1.08 | 0.95 | 1.24 | 0.22 |
| Age | 9 | 1.01 | 0.99 | 1.03 | 0.35 |
| Male | 10 | 0.82 | 0.17 | 3.94 | 0.81 |
| Sample size | 24 | 1.00 | 1.00 | 1.00 | 0.73 |
| No. of Studies | Certainty Assessment | Effect | Certainty | Importance | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | No. of Events | No. of Individuals | Rate (95% CI) | |||
| Mortality between patients supported with concurrent ECMO and RRT | |||||||||||
| 24 | observational studies | not serious | not serious a | not serious | not serious b | none | 2175 | 3202 | 63.0% (56.0% to 69.6%) | ⊕⊕⊕⊕ HIGH | CRITICAL |
| ICU Length of Stay | |||||||||||
| 3 | observational studies | not serious | serious c | not serious | serious d | none | - | 1854 | 15.76 days (12.83 to 18.69) | ⊕⊕◯◯ LOW | IMPORTANT |
| Hospital Length of Stay | |||||||||||
| 4 | observational studies | not serious | serious c | not serious | serious d,e | none | - | 2181 | 29.00 days (21.74 to 36.26) | ⊕⊕◯◯ LOW | IMPORTANT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitra, S.; Ling, R.R.; Tan, C.S.; Shekar, K.; MacLaren, G.; Ramanathan, K. Concurrent Use of Renal Replacement Therapy during Extracorporeal Membrane Oxygenation Support: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 241. https://doi.org/10.3390/jcm10020241
Mitra S, Ling RR, Tan CS, Shekar K, MacLaren G, Ramanathan K. Concurrent Use of Renal Replacement Therapy during Extracorporeal Membrane Oxygenation Support: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(2):241. https://doi.org/10.3390/jcm10020241
Chicago/Turabian StyleMitra, Saikat, Ryan Ruiyang Ling, Chuen Seng Tan, Kiran Shekar, Graeme MacLaren, and Kollengode Ramanathan. 2021. "Concurrent Use of Renal Replacement Therapy during Extracorporeal Membrane Oxygenation Support: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 2: 241. https://doi.org/10.3390/jcm10020241