
Effects of Probiotics, Prebiotics, and Synbiotics on Uremic Toxins, Inflammation, and Oxidative Stress in Hemodialysis Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Registration and Protocol
2.2. Eligibility Criteria
2.3. Information Sources and Search Strategy
2.4. Study Selection and Data Collection
2.5. Data Items
2.6. Risk of Bias Assessment
2.7. Data Analysis
3. Results
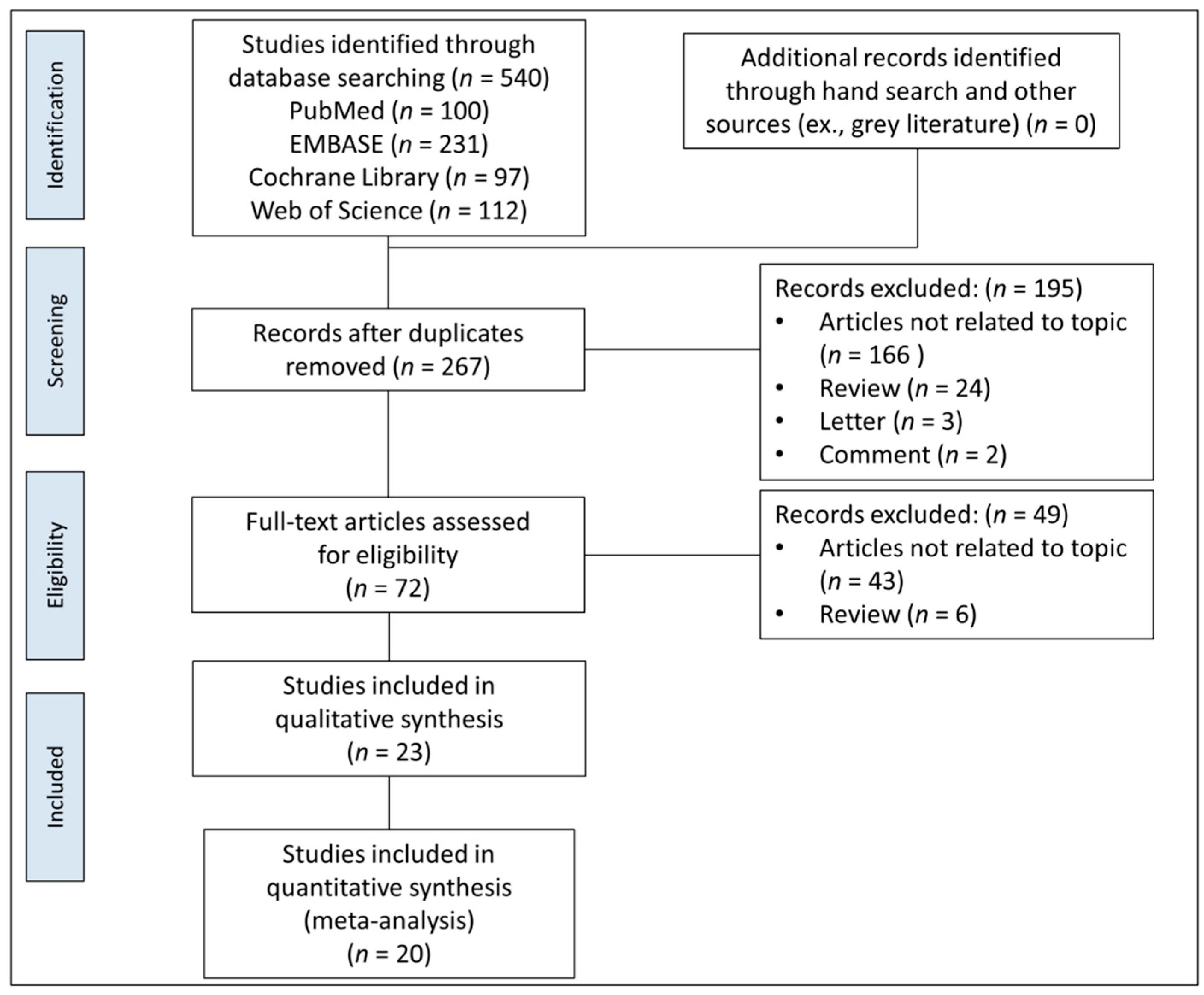
3.1. Search and Selection of Studies
3.2. Characteristics of Included Studies
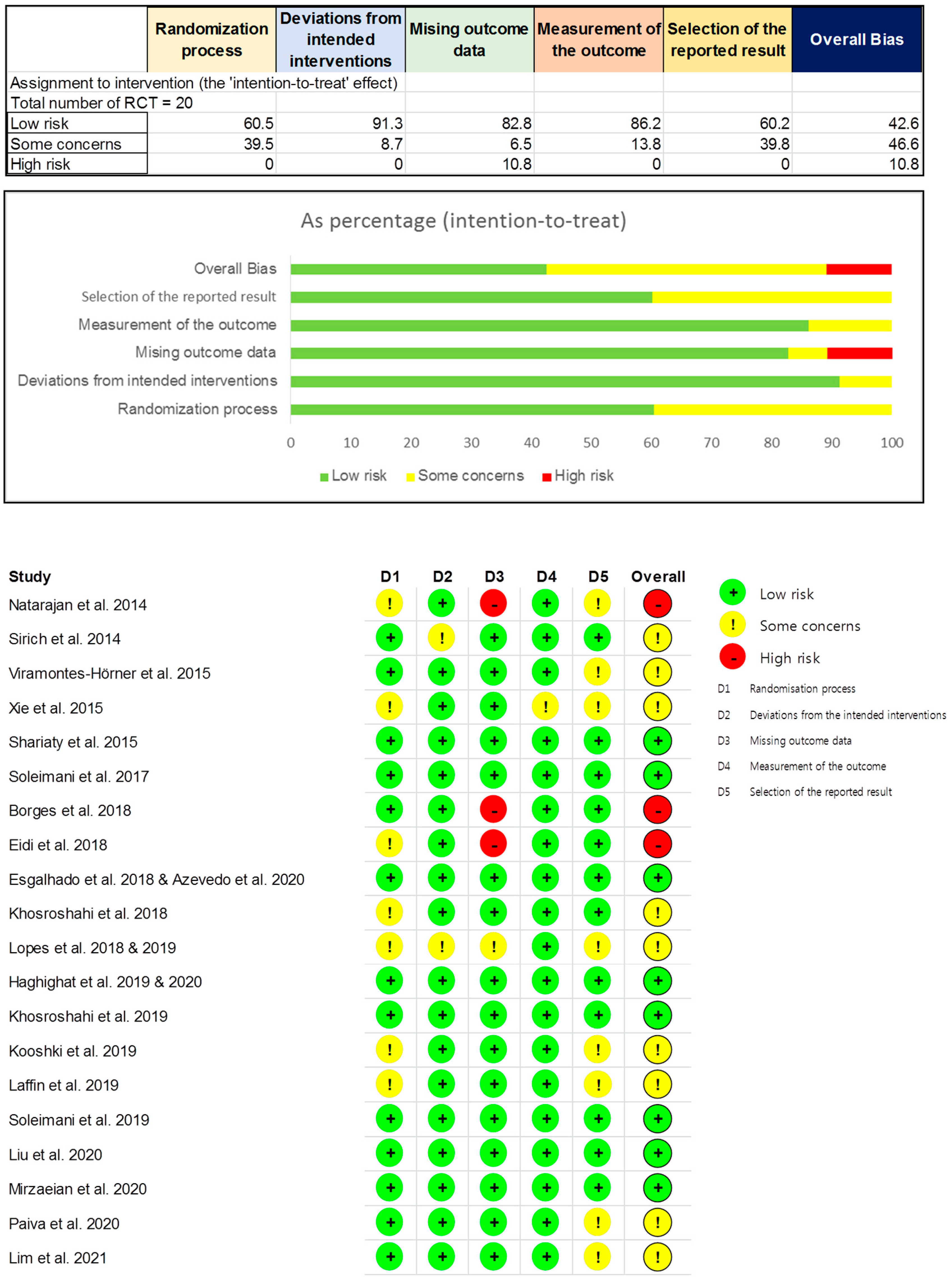
3.3. Quality Assessment
3.4. Meta-Analysis
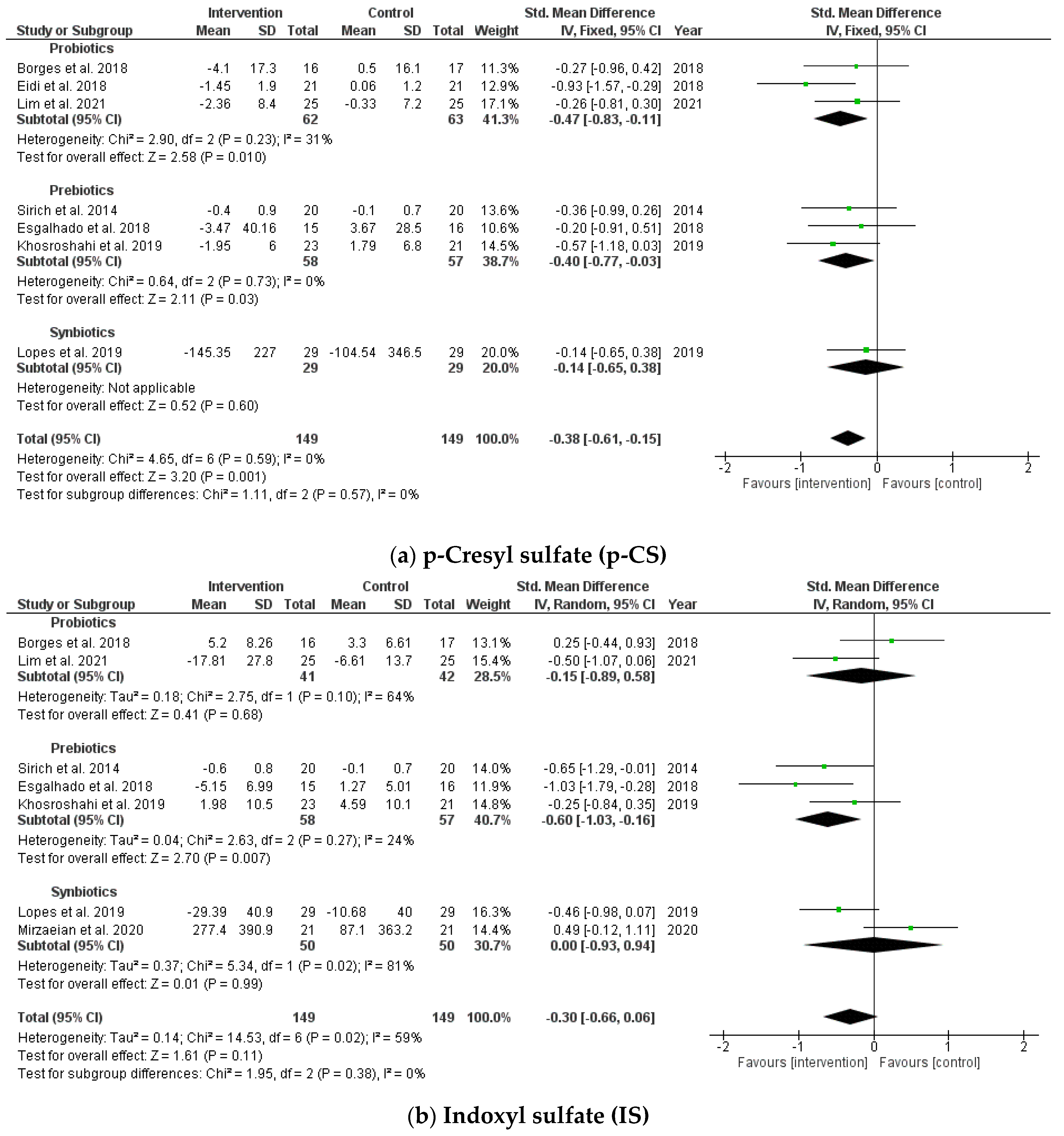
3.4.1. Effects on Circulating Uremic Toxins
3.4.2. Effects on Endotoxins
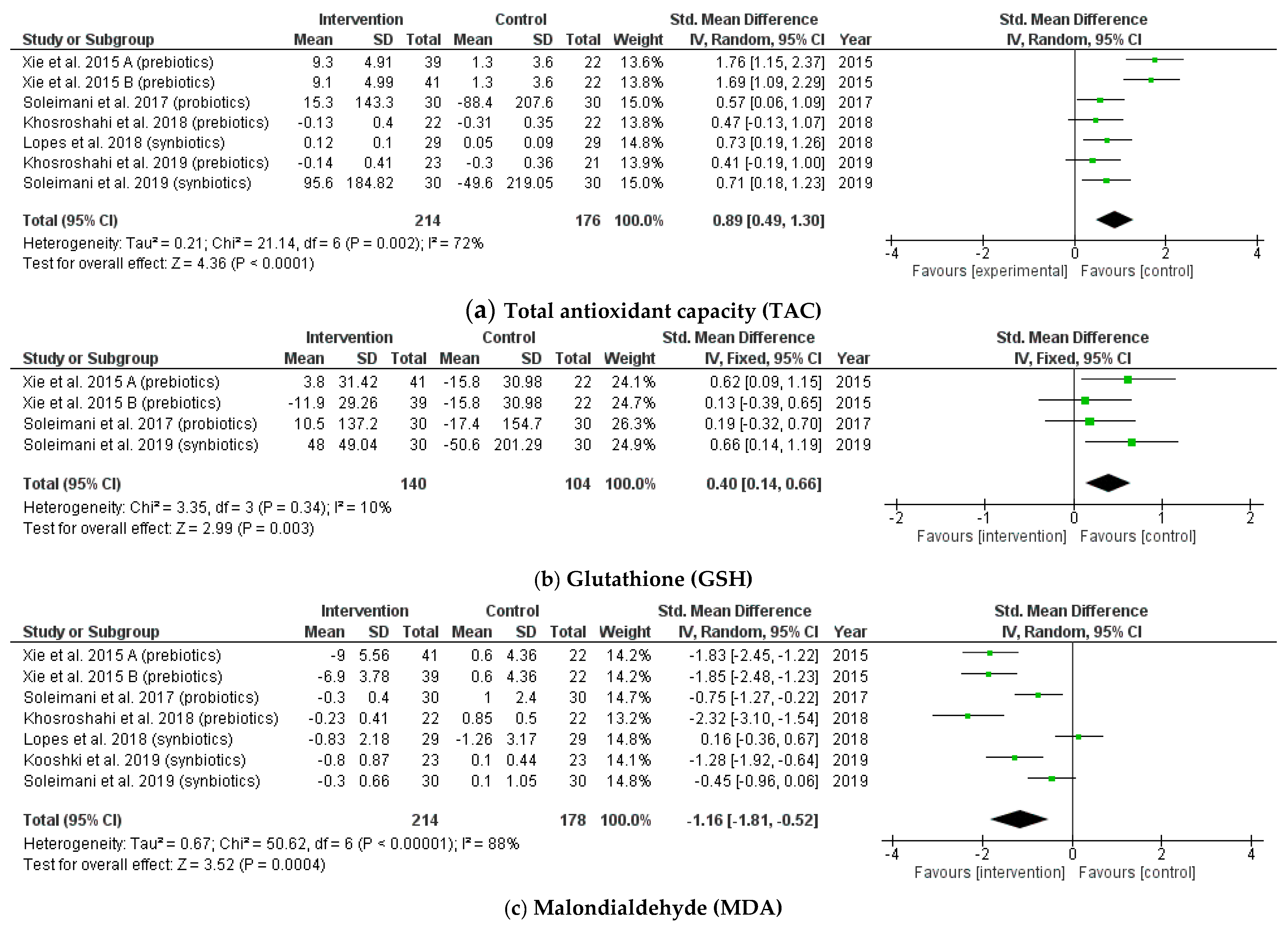
3.4.3. Effects on Biomarkers of Oxidative Stress
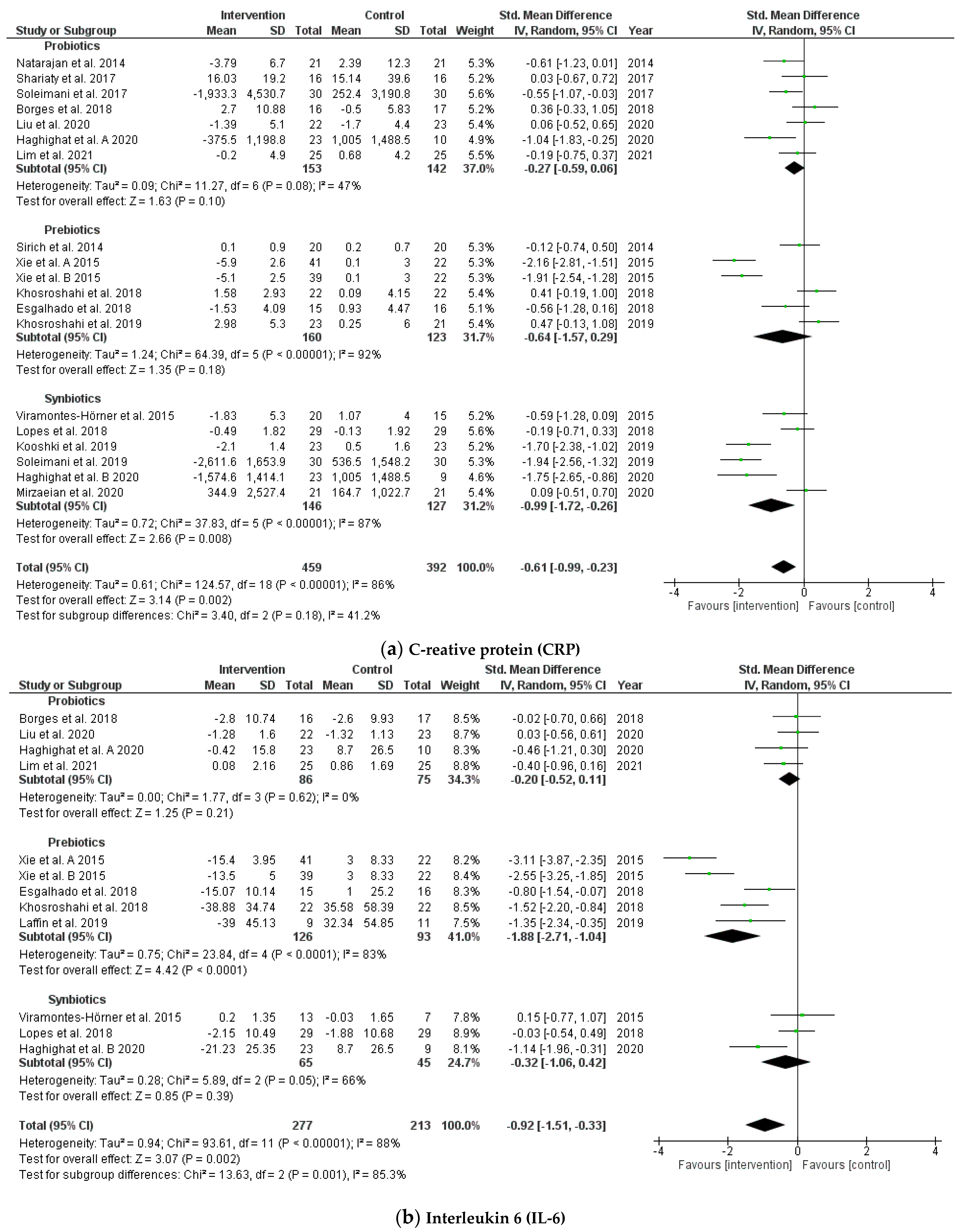
3.4.4. Effects on Biomarkers of Inflammation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Detailed Search Strategies | Records Founded |
|---|---|---|
| MEDLINE/PUBMED | (“probiotics”(MeSH Terms) OR probiotics(Text Word) OR “prebiotics”(MeSH Terms) OR prebiotics(Text Word) OR “dietary fiber”(MeSH Terms) OR Dietary Fiber(Text Word) OR “resistant starch”(MeSH Terms) OR Resistant Starch(Text Word) OR “synbiotics”(MeSH Terms) OR synbiotics(Text Word)) AND (“renal dialysis”(MeSH Terms) OR hemodialysis(Text Word)) | 100 |
| EMBASE | (‘probiotic agent’ OR ‘prebiotic agent’ OR ‘dietary fiber’ OR ‘resistant starch’ OR ‘synbiotic agent’) AND hemodialysis | 231 |
| Cochrane Library | (probiotics OR prebiotics OR “dietary fiber” OR “resistant starch” OR synbiotics) AND hemodialysis | 97 |
| Web of Science | (probiotics OR prebiotics OR “dietary fiber” OR “resistant starch” OR synbiotics) AND hemodialysis | 112 |
References
- Yang, T.; Richards, E.M.; Pepine, C.J.; Raizada, M.K. The gut microbiota and the brain-gut-kidney axis in hypertension and chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 442–456. [Google Scholar] [CrossRef]
- Kim, M.G.; Yang, J.; Jo, S.K. Intestinal microbiota and kidney diseases. Kidney Res. Clin. Pract. 2021, 40, 335–343. [Google Scholar] [CrossRef]
- Himmelfarb, J.; Vanholder, R.; Mehrotra, R.; Tonelli, M. The current and future landscape of dialysis. Nat. Rev. Nephrol. 2020, 16, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Jourde-Chiche, N.; Dou, L.; Cerini, C.; Dignat-George, F.; Vanholder, R.; Brunet, P. (Eds.) PROGRESS IN UREMIC TOXIN RESEARCH: Protein-Bound Toxins—Update 2009. Seminars in Dialysis; Wiley Online Library: Hoboken, NJ, USA, 2009. [Google Scholar]
- Santosa, S.; Farnworth, E.; Jones, P.J. Probiotics and their potential health claims. Nutr. Rev. 2006, 64, 265–274. [Google Scholar] [CrossRef]
- de Moreno de LeBlanc, A.; LeBlanc, J.G. Effect of probiotic administration on the intestinal microbiota, current knowledge and potential applications. World J. Gastroenterol. 2014, 20, 16518–16528. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krumbeck, J.A.; Maldonado-Gomez, M.X.; Ramer-Tait, A.E.; Hutkins, R.W. Prebiotics and synbiotics: Dietary strategies for improving gut health. Curr. Opin. Gastroenterol. 2016, 32, 110–119. [Google Scholar] [CrossRef]
- Markowiak, P.; Śliżewska, K. Effects of Probiotics, Prebiotics, and Synbiotics on Human Health. Nutrients 2017, 9, 1021. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kaewput, W.; Hatch, S.T.; Bathini, T.; Sharma, K.; Wijarnpreecha, K.; Ungprasert, P.; D’Costa, M.; Mao, M.A.; Cheungpasitporn, W. Effects of Probiotics on Inflammation and Uremic Toxins Among Patients on Dialysis: A Systematic Review and Meta-Analysis. Dig. Dis. Sci. 2019, 64, 469–479. [Google Scholar] [CrossRef]
- McFarlane, C.; Ramos, C.I.; Johnson, D.W.; Campbell, K.L. Prebiotic, Probiotic, and Synbiotic Supplementation in Chronic Kidney Disease: A Systematic Review and Meta-analysis. J. Ren. Nutr. 2019, 29, 209–220. [Google Scholar] [CrossRef] [Green Version]
- March, D.S.; Jones, A.W.; Bishop, N.C.; Burton, J.O. The Efficacy of Prebiotic, Probiotic, and Synbiotic Supplementation in Modulating Gut-Derived Circulatory Particles Associated With Cardiovascular Disease in Individuals Receiving Dialysis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Ren. Nutr. 2020, 30, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M. Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2 (Updated February 2021); Cochrane Collaboration: Melbourne, Australia, 2021. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Eidi, F.; Poor-Reza Gholi, F.; Ostadrahimi, A.; Dalili, N.; Samadian, F.; Barzegari, A. Effect of Lactobacillus Rhamnosus on serum uremic toxins (phenol and P-Cresol) in hemodialysis patients: A double blind randomized clinical trial. Clin. Nutr. ESPEN 2018, 28, 158–164. [Google Scholar] [CrossRef]
- Esgalhado, M.; Kemp, J.A.; Azevedo, R.; Paiva, B.R.; Stockler-Pinto, M.B.; Dolenga, C.J.; Borges, N.A.; Nakao, L.S.; Mafra, D. Could resistant starch supplementation improve inflammatory and oxidative stress biomarkers and uremic toxins levels in hemodialysis patients? A pilot randomized controlled trial. Food Funct. 2018, 9, 6508–6516. [Google Scholar] [CrossRef]
- Azevedo, R.; Esgalhado, M.; Kemp, J.A.; Regis, B.; Cardozo, L.F.M.F.; Nakao, L.S.; de Brito, J.S.; Mafra, D. Resistant starch supplementation effects on plasma indole 3-acetic acid and aryl hydrocarbon receptor mRNA expression in hemodialysis patients: Randomized, double blind and controlled clinical trial. J. Bras. Nefrol. 2020, 42, 273–279. [Google Scholar] [CrossRef]
- de Paiva, B.R.; Esgalhado, M.; Borges, N.A.; Kemp, J.A.; Alves, G.; Leite, P.E.C.; Macedo, R.; Cardozo, L.F.M.F.; de Brito, J.S.; Mafra, D. Resistant starch supplementation attenuates inflammation in hemodialysis patients: A pilot study. Int. Urol. Nephrol. 2020, 52, 549–555. [Google Scholar] [CrossRef]
- Liu, S.; Liu, H.; Chen, L.; Liang, S.S.; Shi, K.; Meng, W.; Xue, J.; He, Q.; Jiang, H. Effect of probiotics on the intestinal microbiota of hemodialysis patients: A randomized trial. Eur. J. Nutr. 2020, 59, 3755–3766. [Google Scholar] [CrossRef] [PubMed]
- Lim, P.S.; Wang, H.F.; Lee, M.C.; Chiu, L.S.; Wu, M.Y.; Chang, W.C.; Wu, T.K. The Efficacy of Lactobacillus-Containing Probiotic Supplementation in Hemodialysis Patients: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Ren. Nutr. 2021, 31, 189–198. [Google Scholar] [CrossRef]
- Natarajan, R.; Pechenyak, B.; Vyas, U.; Ranganathan, P.; Weinberg, A.; Liang, P.; Mallappallil, M.C.; Norin, A.J.; Friedman, E.A.; Saggi, S.J. Randomized Controlled Trial of Strain-Specific Probiotic Formulation (Renadyl) in Dialysis Patients. BioMed Res. Int. 2014, 2014, 568571. [Google Scholar] [CrossRef] [PubMed]
- Sirich, T.L.; Plummer, N.S.; Gardner, C.D.; Hostetter, T.H.; Meyer, T.W. Effect of increasing dietary fiber on plasma levels of colon-derived solutes in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1603–1610. [Google Scholar] [CrossRef] [Green Version]
- Viramontes-Hörner, D.; Márquez-Sandoval, F.; Martín-del-Campo, F.; Vizmanos-Lamotte, B.; Sandoval-Rodríguez, A.; Armendáriz-Borunda, J.; García-Bejarano, H.; Renoirte-López, K.; García-García, G. Effect of a symbiotic gel (Lactobacillus acidophilus + Bifidobacterium lactis + inulin) on presence and severity of gastrointestinal symptoms in hemodialysis patients. J. Ren. Nutr. 2015, 25, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.M.; Ge, Y.Y.; Huang, X.; Zhang, Y.Q.; Li, J.X. Effects of fermentable dietary fiber supplementation on oxidative and inflammatory status in hemodialysis patients. Int. J. Clin. Exp. Med. 2015, 8, 1363–1369. [Google Scholar] [PubMed]
- Shariaty, Z.; Shan, G.R.M.; Farajollahi, M.; Amerian, M.; Pour, N.B. The effects of probiotic supplement on hemoglobin in chronic renal failure patients under hemodialysis: A randomized clinical trial. J. Res. Med. Sci. 2017, 22, 74. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, A.; Zarrati Mojarrad, M.; Bahmani, F.; Taghizadeh, M.; Ramezani, M.; Tajabadi-Ebrahimi, M.; Jafari, P.; Esmaillzadeh, A.; Asemi, Z. Probiotic supplementation in diabetic hemodialysis patients has beneficial metabolic effects. Kidney Int. 2017, 91, 435–442. [Google Scholar] [CrossRef]
- Borges, N.A.; Carmo, F.L.; Stockler-Pinto, M.B.; de Brito, J.S.; Dolenga, C.J.; Ferreira, D.C.; Nakao, L.S.; Rosado, A.; Fouque, D.; Mafra, D. Probiotic Supplementation in Chronic Kidney Disease: A Double-blind, Randomized, Placebo-controlled Trial. J. Ren. Nutr. 2018, 28, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Khosroshahi, H.T.; Vaziri, N.D.; Abedi, B.; Asl, B.H.; Ghojazadeh, M.; Jing, W.; Vatankhah, A.M. Effect of high amylose resistant starch (HAM-RS2) supplementation on biomarkers of inflammation and oxidative stress in hemodialysis patients: A randomized clinical trial. Hemodial. Int. 2018, 22, 492–500. [Google Scholar] [CrossRef]
- Lopes, R.d.C.S.O.; de Lima, S.L.S.; da Silva, B.P.; Toledo, R.C.L.; de Castro Moreira, M.E.; Anunciação, P.C.; Walter, E.H.M.; Carvalho, C.W.P.; Queiroz, V.A.V.; Ribeiro, A.Q.; et al. Evaluation of the health benefits of consumption of extruded tannin sorghum with unfermented probiotic milk in individuals with chronic kidney disease. Food. Res. Int. 2018, 107, 629–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haghighat, N.; Mohammadshahi, M.; Shayanpour, S.; Haghighizadeh, M.H. Effect of Synbiotic and Probiotic Supplementation on Serum Levels of Endothelial Cell Adhesion Molecules in Hemodialysis Patients: A Randomized Control Study. Probiotics Antimicrob. Proteins 2019, 11, 1210–1218. [Google Scholar] [CrossRef]
- Khosroshahi, H.T.; Abedi, B.; Ghojazadeh, M.; Samadi, A.; Jouyban, A. Effects of fermentable high fiber diet supplementation on gut derived and conventional nitrogenous product in patients on maintenance hemodialysis: A randomized controlled trial. Nutr. Metab. 2019, 16, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kooshki, A.; Tofighiyan, T.; Miri, M. A synbiotic supplement for inflammation and oxidative stress and lipid abnormalities in hemodialysis patients. Hemodial. Int. 2019, 23, 254–260. [Google Scholar] [CrossRef]
- Laffin, M.R.; Tayebi Khosroshahi, H.; Park, H.; Laffin, L.J.; Madsen, K.; Kafil, H.S.; Abedi, B.; Shiralizadeh, S.; Vaziri, N.D. Amylose resistant starch (HAM-RS2) supplementation increases the proportion of Faecalibacterium bacteria in end-stage renal disease patients: Microbial analysis from a randomized placebo-controlled trial. Hemodial. Int. 2019, 23, 343–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, R.C.S.O.; Theodoro, J.M.V.; da Silva, B.P.; Queiroz, V.A.V.; de Castro Moreira, M.E.; Mantovani, H.C.; Hermsdorff, H.H.; Martino, H.S.D. Synbiotic meal decreases uremic toxins in hemodialysis individuals: A placebo-controlled trial. Food. Res. Int. 2019, 116, 241–248. [Google Scholar] [CrossRef] [Green Version]
- Soleimani, A.; Motamedzadeh, A.; Mojarrad, M.Z.; Bahmani, F.; Amirani, E.; Ostadmohammadi, V.; Tajabadi-Ebrahimi, M.; Asemi, Z.J.P. The effects of synbiotic supplementation on metabolic status in diabetic patients undergoing hemodialysis: A randomized, double-blinded, placebo-controlled trial. Probiotics Antimicrob. Proteins 2019, 11, 1248–1256. [Google Scholar] [CrossRef]
- Haghighat, N.; Mohammadshahi, M.; Shayanpour, S.; Haghighizadeh, M.H. Effects of Synbiotics and Probiotics Supplementation on Serum Levels of Endotoxin, Heat Shock Protein 70 Antibodies and Inflammatory Markers in Hemodialysis Patients: A Randomized Double-Blinded Controlled Trial. Probiotics Antimicrob. Proteins 2020, 12, 144–151. [Google Scholar] [CrossRef]
- Mirzaeian, S.; Saraf-Bank, S.; Entezari, M.H.; Hekmatdoost, A.; Feizi, A.; Atapour, A. Effects of synbiotic supplementation on microbiota-derived protein-bound uremic toxins, systemic inflammation, and biochemical parameters in patients on hemodialysis: A double-blind, placebo-controlled, randomized clinical trial. Nutrition 2020, 73, 110713. [Google Scholar] [CrossRef]
- Zheng, H.J.; Guo, J.; Wang, Q.H.; Wang, L.S.; Wang, Y.H.; Zhang, F.; Huang, W.J.; Zhang, W.T.; Liu, W.J.; Wang, Y.X. Probiotics, prebiotics, and synbiotics for the improvement of metabolic profiles in patients with chronic kidney disease: A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2021, 61, 577–598. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Canaud, B.; Eckardt, K.U.; Stenvinkel, P.; Wanner, C.; Zoccali, C. Oxidative stress in end-stage renal disease: An emerging threat to patient outcome. Nephrol. Dial. Transplant. 2003, 18, 1272–1280. [Google Scholar] [CrossRef]
- Liakopoulos, V.; Roumeliotis, S.; Gorny, X.; Dounousi, E.; Mertens, P.R. Oxidative Stress in Hemodialysis Patients: A Review of the Literature. Oxid. Med. Cell. Longev. 2017, 2017, 3081856. [Google Scholar] [CrossRef] [PubMed]
- Dou, L.; Bertrand, E.; Cerini, C.; Faure, V.; Sampol, J.; Vanholder, R.; Berland, Y.; Brunet, P. The uremic solutes p-cresol and indoxyl sulfate inhibit endothelial proliferation and wound repair. Kidney Int. 2004, 65, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Wang, M.; Wang, J.; Li, R.; Zhang, Y. Alterations to the Gut Microbiota and Their Correlation With Inflammatory Factors in Chronic Kidney Disease. Front. Cell. Infect. Microbiol. 2019, 9, 206. [Google Scholar] [CrossRef] [Green Version]
- Hobby, G.P.; Karaduta, O.; Dusio, G.F.; Singh, M.; Zybailov, B.L.; Arthur, J.M. Chronic kidney disease and the gut microbiome. Am. J. Physiol. Renal Physiol. 2019, 316, F1211–F1217. [Google Scholar] [CrossRef] [PubMed]






| Author, Year | Country | Type of Study | Population (M/F) | Mean Age (Years) | Mean BMI (kg/m2) | Hemodialysis | Intervention Group (n) | Control Group (n) | Outcome | Duration |
|---|---|---|---|---|---|---|---|---|---|---|
| Natarajan et al., 2014 [26] | USA | Randomized, double-blind, placebo-controlled crossover trial | 22 (16/8) | 54 | NA | NA | Probiotics: L. acidophilus KB 27, S. thermophilus KB 19, and B. longum KB 31 (n = 22) | Placebo (n = 22) | Hs-CRP, TIG | 2 months |
| Sirich et al., 2014 [27] | USA | Randomized, single-blind, placebo-controlled clinical trial | 40 (24/16) | 56 | 29 | HD, residual urea clearance ≤ 2 mL/min, non-missing HD section | Prebiotics: high-amylose corn starch 15 g/day (n = 20) | Placebo (n = 20) | p-CS, IS hs-CRP | 6 weeks |
| Viramontes-Hörner et al., 2015 [28] | Mexico | Randomized, double-blind, placebo-controlled clinical trial | 42 (32/10) | 40 | 23 | HD thrice-weekly, at least 3 months | Synbiotics: B. lactis Bi-07 and L. acidophilus NCFM; prebiotic fiber (inulin) (n = 22) | Placebo (n = 20) | hs-CRP, IL-6, TNF-α | 2 months |
| Xie et al., 2015 [29] | China | Randomized, placebo-controlled clinical trial | 124 (68/56) | 52 | 22 | HD thrice-weekly, 4 h/session, Kt/V > 1.2 (1.46 ± 0.13) | Prebiotics: 10 g/d fiber (Group A, n = 41), 20 g/d (Group B, n =39) | Placebo (n = 44) | hs-CRP, IL-6, TNF-α, IL-8, TAC, GSH, MDA, SOD | 6 weeks |
| Shariaty et al., 2017 [30] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 36 (20/16) | 58 | NA | HD thrice-weekly, 4 h/session | Probiotics: L. acidophilus, L. casei, L. rhamnosus, L. bulgaricus, B. breve, B. longum, S. thermophiles (500 mg/d) (n = 18) | Placebo (n = 18) | hs-CRP | 3 months |
| Soleimani et al., 2017 [31] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 60 (40/20) | 56 | 26 | HD for ≥1 year, Kt/V probiotics group 1.38± 0.24, placebo group 1.35 ± 0.20 | Probiotics: L. casei, L. acidophilus, and B. bifidum (n = 30) | Placebo (n = 30) | hs-CRP TAC, GSH, MDA | 12 weeks |
| Borges et al., 2018 [32] | Brazil | Randomized, double-blind, placebo-controlled clinical trial | 33 (21/12) | 52 | 25 | HD thrice-weekly, at least 6 months, 3−4.5 h/session | Probiotics: S. thermophilus, L. acidophilus, and B. longum (n = 16) | Placebo (n = 17) | p-CS, IS, IAA hs-CRP, IL-6 | 3 months |
| Eidi et al., 2018 [20] | Iran | Randomized, Triple-blind, placebo-controlled clinical trial | 42 (32/10) | 58 | 24 | HD at least 3 months, hemodialysis 8.41 ± 4.14 h per week, Kt/V 1.43 ± 0.14 | Probiotics: L. Rhamnosus (n = 21) | Placebo (n = 21) | p-CS, phenol | 4 weeks |
| Esgalhado et al., 2018 [21] | Brazil | Randomized, double-blind, placebo-controlled clinical trial | 31 (18/13) | 55 | 26 | HD for at least 6 months, Kt/V 1.4 ± 0.3 | Prebiotics: resistant starch (16 g/d) (n = 15) | Placebo (n = 16) | p-CS, IS hs-CRP, IL-6 | 4 weeks |
| Khosroshahi et al., 2018 [33] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 44 (28/16) | 56 | 23 | Chronic hemodialysis | Prebiotics: high amylose resistant starch (HAM-RS2), 20 g/d (the first 4-weeks) and 25 g/d (the second 4-weeks) (n = 22) | Placebo (n = 22) | hs-CRP, IL-6, TNF-α, IL-1β TAC, MDA | 8 weeks |
| Lopes et al., 2018 [34] | Brazil | Randomized, single-blind, placebo-controlled clinical trial | 58 (38/20) | 63 | 24 | HD thrice weekly, 4 h/session | Synbiotics: 40 g of extruded sorghum + 100 mL of unfermented probiotic milk (n = 29) | 40 g of extruded corn +100 mL of pasteurized milk (n = 29) | hs-CRP, IL-6, TNF-α, IL-10 TAC, MDA, SOD | 7 weeks |
| Haghighat et al., 2019 [35] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 65 (34/31) | 46 | 23 | HD thrice weekly, at least 3 months, 3−4.5 h/session, mL/min, Kt/V 1.46 ± 0.28 | Probiotics: L. acidophilus T16,B. lactis BIA-6, B. bifidum BIA 6 and B. longum LAF-5 (n = 23) Synbiotics: probiotics + prebiotics (n = 23) | Placebo (n = 19) | VCAM-1, CK18, ICAM-1 | 12 weeks |
| Khosroshahi et al., 2019 [36] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 50 (29/21) | 55 | 24 | HD thrice-weekly for at least 6 months | Prebiotics: high amylose resistant starch (HAM-RS2) 20 g/d (the first 4 weeks) and 25 g/d (the second 4 weeks) (n = 23) | Placebo (n = 21) | p-CS, IS hs-CRP TAC | 8 weeks |
| Kooshki et al., 2019 [37] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 46 (21/25) | 63 | 24 | HD thrice-weekly, 4 h/session | Synbiotics: L. coagulans and fructo-oligosaccharides 100 mg, 2 tablets/d (n = 23) | Placebo (n = 23) | hs-CRP MDA | 8 weeks |
| Laffin et al., 2019 [38] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 20 (13/7) | 55 | NA | NA | Prebiotics: high amylose resistant starch (HAM-RS2) 20 g/d (the first 4 weeks) and 25 g/d (the second 4 weeks) (n = 9) | Placebo (n = 11) | IL-6, TNFα | 8 weeks |
| Lopes et al., 2019 [39] | Brazil | Randomized, single-blind, placebo-controlled clinical trial | 58 (38/20) | 63 | 24 | HD thrice weekly, 4 h/session | Synbiotics: 40 g of extruded sorghum + 100 mL of unfermented probiotic milk (n = 29) | 40 g of extruded corn +100 mL of pasteurized milk (n = 29) | p-CS, IS, IAA | 7 weeks |
| Soleimani et al., 2019 [40] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 60 (42/18) | 63 | 26 | NA | Synbiotics: L. acidophilus, L. casei, and B. bifidum; prebiotic fiber(inulin) (n = 30) | Placebo (n = 30) |
hs-CRP TAC, GSH, MDA | 12 weeks |
| Azevedo et al., 2020 [22] | Brazil | Randomized, double-blind, placebo-controlled clinical trial | 31 (18/13) | 55 | NA | NA | Prebiotics: resistant starch (16 g/d) (n = 15) | Placebo (n = 16) | IAA | 4 weeks |
| Haghighat et al., 2020 [41] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 65 (34/31) | 46 | 23 | HD thrice weekly, at least 3 months, 3−4.5 h/session, Kt/V Synbiotics group 1.37 ± 0.29, Probiotics group 1.46 ± 0.25, Placebo 1.57 ± 0.28 | Probiotics: L. acidophilus T16, B. bifidum BIA 6, B. longum LAF-5, and B. lactis BIA-6 (n = 23) Synbiotics: probiotics + prebiotics (n = 23) | Placebo (n = 19) |
Endotoxin hs-CRP, IL-6 | 12 weeks |
| Liu et al., 2020 [24] | China | Randomized, double-blind, placebo-controlled clinical trial | 50 (28/22) | 48 | 20 | HD for at least 3 months | Probiotics: B. longum, L. acidophilus, E. faecalis 210 mg, twice daily (n = 22) | Placebo (n = 23) | Endotoxin hs-CRP, IL-6, TNF-α, E-selectin, ICAM-1 | 6 months |
| Mirzaeian et al., 2020 [42] | Iran | Randomized, double-blind, placebo-controlled clinical trial | 42 (30/12) | 60 | 24.72 | HD thrice weekly, at least 6 months, for no less then 4 h each time | Synbiotics: L. casei, L. acidophilus, L. rhamnosus, L. bulgaricus, B. breve, B. longum and S. thermophiles; fructo-oligosaccharide. Two synbiotic capsules daily (n = 21) | Placebo (n = 21) | IS, phenol hs-CRP | 8 weeks |
| Paiva et al., 2020 [23] | Brazil | Randomized, double-blind, placebo-controlled clinical trial | 16 (9/7) | 55 | 26 | HD for more than 6 months, Kt/V 1.4 ± 0.2 | Prebiotics: resistant starch (16 g/d) (n = 8) | Placebo (n = 8) | IP-10, PDGF, RANTES | 4 weeks |
| Lim et al., 2021 [25] | Taiwan | Randomized, double-blind, placebo-controlled clinical trial | 50 (20/30) | 59 | 24.5 | HD thrice weekly, for at least 6 months, 4 h/session, Kt/V 1.79 ± 0.21 1.84 ± 0.20 | Probiotics: Lactococcus lactis subsp. Lactis LL358, L. salivarius LS159, and L. pentosus LPE588 (n = 25) | Placebo (n = 25) | p-CS, IS, hs-CRP, IL-6, TNF-α | 6 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.T.U.; Kim, H.W.; Kim, W. Effects of Probiotics, Prebiotics, and Synbiotics on Uremic Toxins, Inflammation, and Oxidative Stress in Hemodialysis Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 4456. https://doi.org/10.3390/jcm10194456
Nguyen TTU, Kim HW, Kim W. Effects of Probiotics, Prebiotics, and Synbiotics on Uremic Toxins, Inflammation, and Oxidative Stress in Hemodialysis Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2021; 10(19):4456. https://doi.org/10.3390/jcm10194456
Chicago/Turabian StyleNguyen, Thi Thuy Uyen, Hyeong Wan Kim, and Won Kim. 2021. "Effects of Probiotics, Prebiotics, and Synbiotics on Uremic Toxins, Inflammation, and Oxidative Stress in Hemodialysis Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 10, no. 19: 4456. https://doi.org/10.3390/jcm10194456