
Persistent Post-COVID-19 Syndrome in Hemodialyzed Patients—A Longitudinal Cohort Study from the North of Poland

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
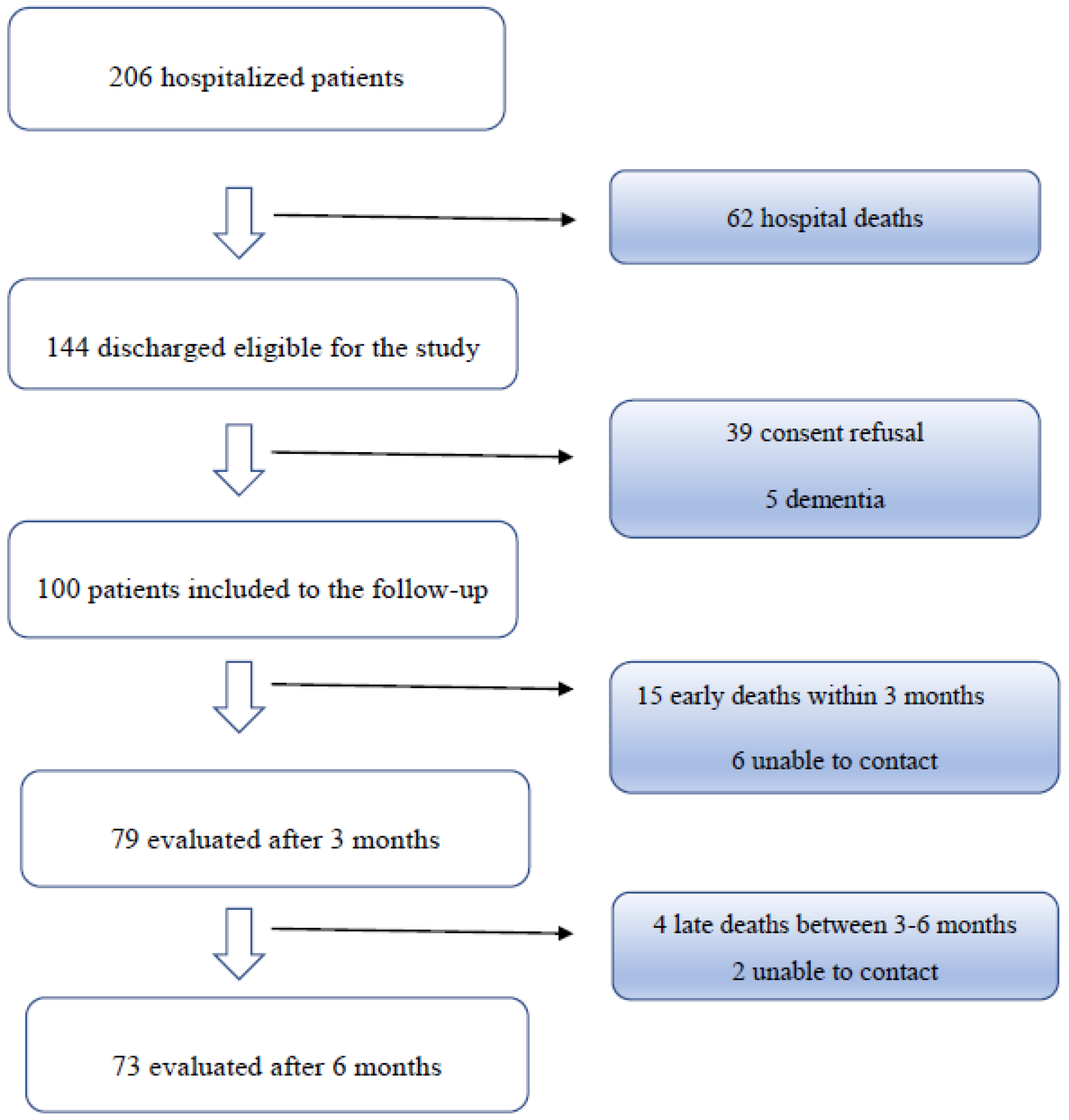
3. Results
3.1. Patients
3.2. Self-Reported Symptoms (SRSQ)
3.3. Self-Reported Dyspnea (mMRC)
3.4. Health Related Quality of Life (EuroQoL)
3.5. Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Willi, S.; Luthold, R.; Hunt, A.; Hanggi, N.V.; Sejdiu, D.; Scaff, C.; Bender, N.; Staub, K.; Schlagenhauf, P. COVID-19 sequelae in adults aged less than 50 years: A systematic review. Travel Med. Infect. Dis. 2021, 40, 101995. [Google Scholar] [CrossRef]
- Maestre-Muniz, M.M.; Arias, A.; Mata-Vazquez, E.; Martin-Toledano, M.; Lopez-Larramona, G.; Ruiz-Chicote, A.M.; Nieto-Sandoval, B.; Lucendo, A.J. Long-Term Outcomes of Patients with Coronavirus Disease 2019 at One Year after Hospital Discharge. J. Clin. Med. 2021, 10, 2945. [Google Scholar] [CrossRef]
- Shah, W.; Hillman, T.; Playford, E.D.; Hishmeh, L. Managing the long term effects of covid-19: Summary of NICE, SIGN, and RCGP rapid guideline. BMJ 2021, 372, n136. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M.; Noordzij, M.; Pena, M.J.; Vries, H.; et al. COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Nephrol. Dial. Transpl. 2020, 35, 1973–1983. [Google Scholar] [CrossRef]
- Puchalska-Reglińska, E.; Debska-Slizien, A.; Biedunkiewicz, B.; Tylicki, P.; Polewska, K.; Rutkowski, B.; Gellert, R.; Tylicki, L. Extremely high mortality in COVID-19 hemodialyzed patients before the anti-SARS-CoV-2 vaccination era. Large database from the North of Poland. Pol. Arch. Intern. Med. 2021, 131, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Mahler, D.A.; Wells, C.K. Evaluation of clinical methods for rating dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- PHOSP-COVID Collaborative Group; Evans, R.; McAuley, H.; Harrison, E.; Shikotra, A.; Singapuri, A.; Sereno, M.; Elneima, O.; Docherty, A.; Lone, N.; et al. Physical, cognitive and mental health impacts of COVID-19 following hospitalisation—A multi-centre prospective cohort study. medRxiv 2021. [Google Scholar] [CrossRef]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.; Cuapio, A.; Villapol, S. More than 50 Long-term effects of COVID-19: A systematic review and meta-analysis. medRxiv 2021. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; Palacios-Cena, D.; Gomez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- The Office for National Statistics (ONS). Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/technicalarticleupdatedestimatesoftheprevalenceofpostacutesymptomsamongpeoplewithcoronaviruscovid19intheuk/26april2020to1august2021 (accessed on 21 September 2021).
- Zayet, S.; Zahra, H.; Royer, P.Y.; Tipirdamaz, C.; Mercier, J.; Gendrin, V.; Lepiller, Q.; Marty-Quinternet, S.; Osman, M.; Belfeki, N.; et al. Post-COVID-19 Syndrome: Nine Months after SARS-CoV-2 Infection in a Cohort of 354 Patients: Data from the First Wave of COVID-19 in Nord Franche-Comte Hospital, France. Microorganisms 2021, 9, 1719. [Google Scholar] [CrossRef] [PubMed]
- Wanga, V.; Chevinsky, J.R.; Dimitrov, L.V.; Gerdes, M.E.; Whitfield, G.P.; Bonacci, R.A.; Nji, M.A.M.; Hernandez-Romieu, A.C.; Rogers-Brown, J.S.; McLeod, T.; et al. Long-Term Symptoms Among Adults Tested for SARS-CoV-2—United States, January 2020–April 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Garg, M.; Maralakunte, M.; Garg, S.; Dhooria, S.; Sehgal, I.; Bhalla, A.S.; Vijayvergiya, R.; Grover, S.; Bhatia, V.; Jagia, P.; et al. The Conundrum of ‘Long-COVID-19’: A Narrative Review. Int. J. Gen. Med. 2021, 14, 2491–2506. [Google Scholar] [CrossRef] [PubMed]
- Goertz, Y.M.J.; Van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.C.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.E.; et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6, 00542-2020. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Bottino, R.; Carbone, A.; Rago, A.; Papa, A.A.; Golino, P.; Nigro, G. COVID-19 and Heart: From Clinical Features to Pharmacological Implications. J. Clin. Med. 2020, 9, 1944. [Google Scholar] [CrossRef] [PubMed]
- Chopra, V.; Flanders, S.A.; O’Malley, M.; Malani, A.N.; Prescott, H.C. Sixty-Day Outcomes Among Patients Hospitalized With COVID-19. Ann. Intern. Med. 2021, 174, 576–578. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Lupi, L.; Zaccone, G.; Italia, L.; Raffo, M.; Tomasoni, D.; Cani, D.S.; Cerini, M.; Farina, D.; Gavazzi, E.; et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 819–824. [Google Scholar] [CrossRef] [Green Version]
- Basic-Jukic, N.; Juric, I.; Furic-Cunko, V.; Katalinic, L.; Radic, J.; Bosnjak, Z.; Jelakovic, B.; Kastelan, Z. Follow-up of renal transplant recipients after acute COVID-19-A prospective cohort single-center study. Immun. Inflamm. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Surendra, N.K.; Abdul Manaf, M.R.; Hooi, L.S.; Bavanandan, S.; Mohamad Nor, F.S.; Shah Firdaus Khan, S.; Ong, L.M.; Abdul Gafor, A.H. Health related quality of life of dialysis patients in Malaysia: Haemodialysis versus continuous ambulatory peritoneal dialysis. BMC Nephrol. 2019, 20, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zyoud, S.H.; Daraghmeh, D.N.; Mezyed, D.O.; Khdeir, R.L.; Sawafta, M.N.; Ayaseh, N.A.; Tabeeb, G.H.; Sweileh, W.M.; Awang, R.; Al-Jabi, S.W. Factors affecting quality of life in patients on haemodialysis: A cross-sectional study from Palestine. BMC Nephrol. 2016, 17, 44. [Google Scholar] [CrossRef] [Green Version]
- Heleniak, Z.; Cieplinska, M.; Szychlinski, T.; Rychter, D.; Jagodzinska, K.; Klos, A.; Kuzmiuk, I.; Tylicka, M.J.; Tylicki, L.; Rutkowski, B.; et al. Nonsteroidal anti-inflammatory drug use in patients with chronic kidney disease. J. Nephrol. 2017, 30, 781–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakimowicz-Tylicka, M.; Chmielewski, M.; Kuzmiuk-Glembin, I.; Skonieczny, P.; Dijakiewicz, G.; Zdrojewska, G.; Rutkowski, B.; Tylicki, L.; Debska Slizien, A. Dietary supplement use among patients with chronic kidney disease. Acta Biochim. Pol. 2018, 65, 319–324. [Google Scholar] [CrossRef]
- Chazot, C.; Wabel, P.; Chamney, P.; Moissl, U.; Wieskotten, S.; Wizemann, V. Importance of normohydration for the long-term survival of haemodialysis patients. Nephrol. Dial. Transpl. 2012, 27, 2404–2410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamney, P.W.; Kramer, M.; Rode, C.; Kleinekofort, W.; Wizemann, V. A new technique for establishing dry weight in hemodialysis patients via whole body bioimpedance. Kidney Int. 2002, 61, 2250–2258. [Google Scholar] [CrossRef] [Green Version]
- Yan, Z.; Yang, M.; Lai, C.L. Long COVID-19 Syndrome: A Comprehensive Review of Its Effect on Various Organ Systems and Recommendation on Rehabilitation Plans. Biomedicines 2021, 9, 966. [Google Scholar] [CrossRef]
- Ribeiro, H.S.; Rodrigues, A.E.; Cantuaria, J.; Inda-Filho, A.; Bennett, P.N. Post-COVID-19 rehabilitation: A special look at chronic kidney disease patients. Ren. Replace. Ther. 2021, 7, 33. [Google Scholar] [CrossRef]


{kind=link}
| n | 79 |
| Age years | 70 (64–76.5) |
| Male gender | 39 (49.37) |
| BMI kg/m2 | 26.1 (21.6–28.9) |
| Hemodialysis vintage months | 40 (17.5–88) |
| Charlson Comorbidity Index | 7 (6–9) |
| Fragility index | 4 (3–5) |
| Diabetes mellitus | 40 (50.63) |
| Arterial hypertension | 74 (93.7) |
| Total duration of hospitalization days | 17 (13–21) |
| Disease severity *: | |
| COVID-19 asymptomatic | 2/54 (3.7%) |
| COVID-19 without pneumonia | 7/54 (16.7%) |
| COVID-19 pneumonia | 45/54 (83.3%) |
| COVID-19 with pneumonia requiring oxygen therapy | 24/54 (48.1%) |
| Specific treatments *: | |
| Plasma of convalescents | 9/54 (16.7%) |
| Remdesivir | 6/54 (11.1%) |
| Corticosteroids | 24/54 (44.4) |
| Declared Persistent or New Symptoms | 3 Months n = 79 n (%) | 6 Months n = 73 n (%) |
|---|---|---|
| Fatigue or muscle weakness | 48 (60.76) | 35 (47.94) * |
| Palpitations | 32 (40.51) | 22 (30.14) * |
| Nausea | 32 (40.51) | 20 (27.40) * |
| Hair loss | 24 (30.38) | 18 (24.66) * |
| Decreased appetite | 22 (27.85) | 15 (20.55) * |
| Sleep difficulties | 21 (26.58) | 21 (28.77) * |
| Myalgia | 20 (25.32) | 15 (20.55) * |
| Dizziness | 20 (25.32) | 15 (20.55) * |
| Vomiting | 20 (25.32) | 14 (19.17) * |
| Headache | 17 (21.52) | 17 (23.29) * |
| Low grade fever | 16 (20.25) | 6 (8.22) ** |
| Diarrhea | 16 (20.25) | 6 (8.21) ** |
| Joint pain | 14 (17.72) | 16 (21.92) * |
| Taste disorder | 13 (16.46) | 8 (10.96) * |
| Smell disorder | 12 (15.19) | 7 (9.59) * |
| Chest pain | 11 (13.92) | 13 (17.81) * |
| Sore throat or difficult to swallow | 10 (12.66) | 6 (8.22) * |
| Skin rash | 2 (2.53) | 2 (2.74) * |
| Before | 3 Months | 6 Months | p Value | |
|---|---|---|---|---|
| mMRC score | 1.42 ± 0.84 | 1.99 ± 1.25 | 1.67 ± 1.05 | p < 0.001 |
| mMRC score ≥ 1 | 17/79 (21.52%) | 34/79 (43.03%) | 25/73 (34.25%) | p = 0.015 |
| Patient weight kg | 75.7 ± 18.4 | 72.5 ± 16.6 | 72.8 ± 17.3 | p < 0.001 |
| Before COVID-19 | 3 Months | 6 Months | |
|---|---|---|---|
| Mobility | 38 (48.1) | 29 (36.7) | 28 (38.4) |
| Self-care | 58 (73.5) | 52 (65.8) | 50 (68.5) |
| Usual activity | 40 (50.6) | 33 (41.8) | 37 (50.7) |
| Pain or discomfort | 62 (78.5) | 47 (59.5) | 52 (71.2) * |
| Anxiety | 67 (84.8) | 58 (73.4) | 53 (72.6) *** |
| EQ-VAS 0–100 | 69.9 ± 17.6 | 61.1 ± 18.5 | 64.4 ± 16.2 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Och, A.; Tylicki, P.; Polewska, K.; Puchalska-Reglińska, E.; Parczewska, A.; Szabat, K.; Biedunkiewicz, B.; Dębska-Ślizień, A.; Tylicki, L. Persistent Post-COVID-19 Syndrome in Hemodialyzed Patients—A Longitudinal Cohort Study from the North of Poland. J. Clin. Med. 2021, 10, 4451. https://doi.org/10.3390/jcm10194451
Och A, Tylicki P, Polewska K, Puchalska-Reglińska E, Parczewska A, Szabat K, Biedunkiewicz B, Dębska-Ślizień A, Tylicki L. Persistent Post-COVID-19 Syndrome in Hemodialyzed Patients—A Longitudinal Cohort Study from the North of Poland. Journal of Clinical Medicine. 2021; 10(19):4451. https://doi.org/10.3390/jcm10194451
Chicago/Turabian StyleOch, Aleksander, Piotr Tylicki, Karolina Polewska, Ewelina Puchalska-Reglińska, Aleksandra Parczewska, Krzysztof Szabat, Bogdan Biedunkiewicz, Alicja Dębska-Ślizień, and Leszek Tylicki. 2021. "Persistent Post-COVID-19 Syndrome in Hemodialyzed Patients—A Longitudinal Cohort Study from the North of Poland" Journal of Clinical Medicine 10, no. 19: 4451. https://doi.org/10.3390/jcm10194451