
Sleeve Gastrectomy and Roux-En-Y Gastric Bypass. Two Sculptors of the Pancreatic Islet

 , ,
, ,
Abstract
:1. Introduction
2. Methods and Results
3. Discussion
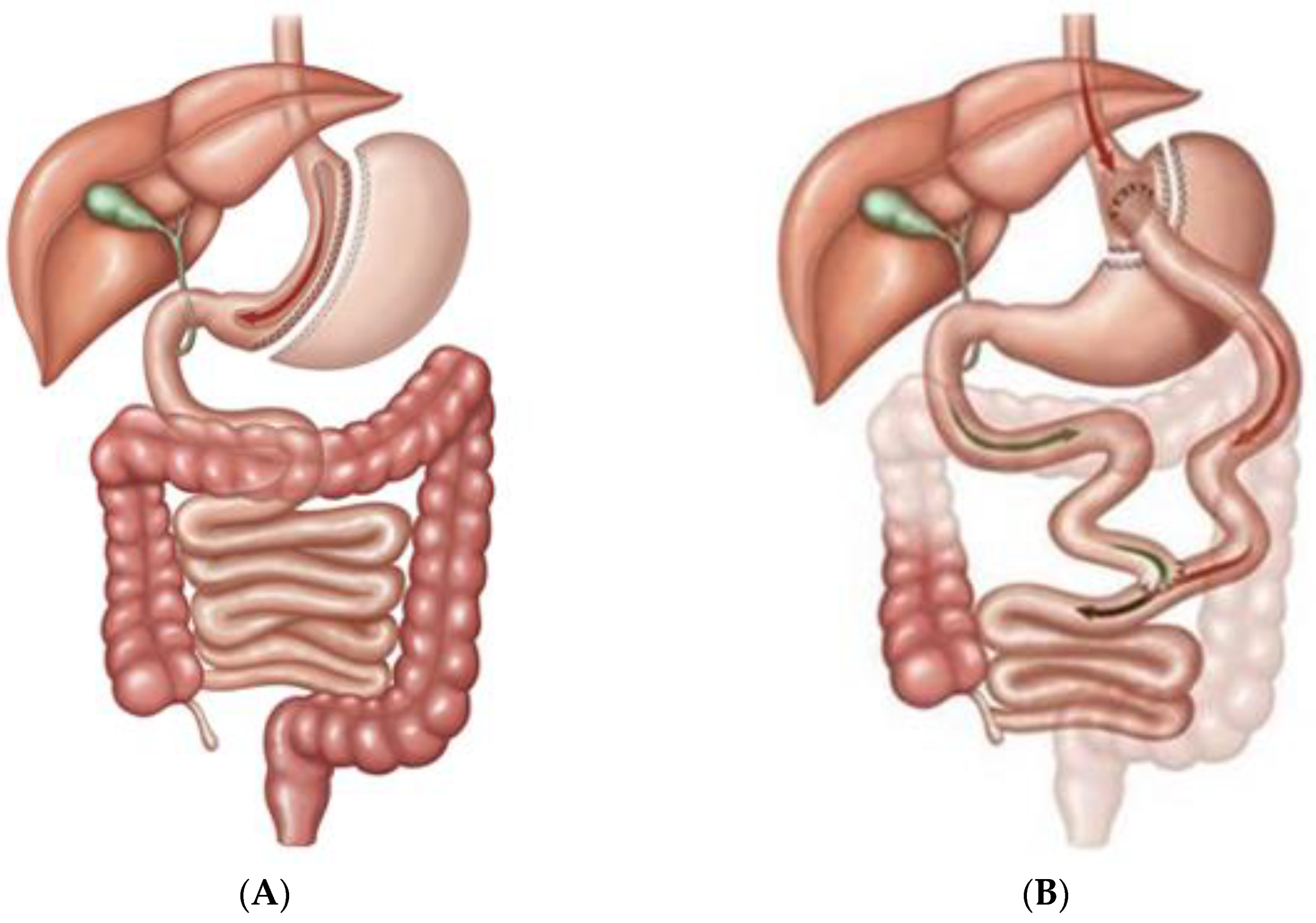
3.1. The Sleeve Gastrectomy and the Islet Architecture
3.2. The Roux-en-Y Gastric Bypass and the Islet Architecture
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mingrone, G.; Panunzi, S.; De Gaetano, A.; Guidone, C.; Iaconelli, A.; Leccesi, L.; Nanni, G.; Pomp, A.; Castagneto, M.; Ghirlanda, G.; et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N. Engl. J. Med. 2012, 366, 1577–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schauer, P.R.; Bhatt, D.L.; Kirwan, J.P.; Wolski, K.; Aminian, A.; Brethauer, S.A.; Navaneethan, S.D.; Singh, R.P.; Pothier, C.E.; Nissen, S.E.; et al. Bariatric surgery versus intensive medical therapy for diabetes 5-year outcomes. N. Engl. J. Med. 2017, 376, 641–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heneghan, H.M.; Nissen, S.; Schauer, P.R. Gastrointestinal Surgery for Obesity and Diabetes: Weight Loss and Control of Hyperglycemia. Curr. Atheroscler. Rep. 2012, 14, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Miras, A.D.; le Roux, C.W. Mechanisms underlying weight loss after bariatric surgery. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 575–584. [Google Scholar] [CrossRef]
- Larraufie, P.; Roberts, G.P.; McGavigan, A.K.; Kay, R.G.; Li, J.; Leiter, A.; Melvin, A.; Biggs, E.K.; Ravn, P.; Davy, K.; et al. Important Role of the GLP-1 Axis for glucose homeostasis after bariatric surgery. Cell. Rep. 2019, 26, 1399–1408. [Google Scholar] [CrossRef] [Green Version]
- Frezza, E.E.; Chiriva-Internati, M.; Wachtel, M.S. Analysis of the results of sleeve gastrectomy for morbid obesity and the role of ghrelin. Surg. Today 2008, 38, 481–483. [Google Scholar] [CrossRef]
- Camacho-Ramírez, A.; Prada-Oliveira, J.A.; Ribelles-García, A.; Almorza-Gomar, D.; Pérez-Arana, G.M. The leading role of peptide tyrosine tyrosine in glycemic control after roux-en-y gastric bypass in rats. Obes. Surg. 2020, 30, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Honka, H.; Koffert, J.; Kauhanen, S.; Kudomi, N.; Hurme, S.; Mari, A.; Lindqvist, A.; Wierup, N.; Parkkola, R.; Groop, L.; et al. Liver blood dynamics after bariatric surgery: The effects of mixed-meal test and incretin infusions. Endocr. Connect. 2018, 7, 888–896. [Google Scholar] [CrossRef] [Green Version]
- Münzberg, H.; Laque, A.; Yu, S.; Rezai-Zadeh, K.; Berthou, H.R. Appetite and body weight regulation after bariatric surgery. Obes. Rev. 2015, 16, 77–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitriadis, G.K.; Randeva, M.S.; Miras, A.D. Potential Hormone Mechanisms of Bariatric Surgery. Curr. Obes. Rep. 2017, 6, 253–265. [Google Scholar] [CrossRef] [Green Version]
- Meek, C.L.; Lewis, H.B.; Reimann, F.; Gribble, F.M.; Park, A.J. The effect of bariatric surgery on gastrointestinal and pancreatic peptide hormones. Peptides 2016, 77, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Ariyasu, H.; Takaya, K.; Tagami, T.; Ogawa, Y.; Hosoda, K.; Akamizu, T.; Suda, M.; Koh, T.; Natsui, K.; Toyooka, S. Stomach is a major source of circulating ghrelin, and feeding state determines plasma ghrelin-like immunoreactivity levels in humans. J. Clin. Endocrinol. Metab. 2001, 86, 4753–4758. [Google Scholar] [CrossRef]
- Kalinowski, P.; Paluszkiewicz, R.; Wróblewski, T.; Remiszewski, P.; Grodzicki, M.; Bartoszewicz, Z.; Krawczyk, M. Ghrelin, leptin, and glycemic control after sleeve gastrectomy versus Roux-en-Y gastric bypass-results of a randomized clinical trial. Surg. Obes. Relat. Dis. 2017, 13, 181–188. [Google Scholar] [CrossRef]
- Popovic, V.; Miljic, D.; Pekic, S.; Pesko, P.; Djurovic, M.; Doknic, M.; Damjanovic, S.; Micic, D.; Cvijovic, G.; Glodic, J.; et al. Low plasma ghrelin level in gastrectomized patients is accompanied by enhanced sensitivity to the ghrelin-induced growth hormone release. J. Clin. Endocrinol. Metab. 2005, 90, 2187–2191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camacho-Ramírez, A.; Mayo-Ossorio, M.A.; Pacheco-García, J.M.; Almorza-Gomar, D.; Ribelles-García, A.; Belmonte-Núñez, A.; Prada-Oliveira, J.A.; Pérez-Arana, M. Pancreas is a preeminent source of ghrelin after sleeve gastrectomy in Wistar rats. Histol. Histopathol. 2020, 35, 801–809. [Google Scholar] [CrossRef]
- Baena-Nieto, G.; Lomas-Romero, I.M.; Mateos, R.M.; Leal-Cosme, N.; Perez-Arana, G.; Aguilar-Diosdado, M. Ghrelin mitigates β-cell mass loss during insulitis in an animal model of autoimmune diabetes mellitus, the BioBreeding/Worcester rat. Diabetes Metab. Res. Rev. 2017, 33, e2813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullally, J.A.; Febres, G.J.; Bessler, M.; Korner, J. Sleeve Gastrectomy and Roux-en-Y gastric bypass achieve similar early improvements in beta-cell function in obese patients with Type 2 Diabetes. Sci. Rep. 2019, 9, 1880. [Google Scholar] [CrossRef] [Green Version]
- Ugi, S.; Morino, K.; Yamaguchi, T.; Yamamoto, H.; Kaida, S.; Miyazawa, I.; Sato, D.; Sekine, O.; Fujita, Y.; Kashiwagi, A.; et al. Preserving beta-cell function is the major determinant of diabetes remission following laparoscopic sleeve gastrectomy in Japanese obese diabetic patients. Endocr. J. 2019, 66, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Garibay, D.; McGavigan, A.K.; Lee, S.A.; Ficorilli, J.V.; Cox, A.L.; Michael, M.D.; Sloop, K.W.; Cummings, B.P. Beta-cell glucagon-like peptide-1 receptor contributes to improved glucose tolerance after vertical sleeve gastrectomy. Endocrinology 2016, 157, 3405–3409. [Google Scholar] [CrossRef] [Green Version]
- Garibay, D.; Lou, J.; Lee, S.A.; Zaborska, K.E.; Weissman, M.H.; Sloma, E.; Donahue, L.; Miller, A.D.; White, A.C.; Michael, A.D.; et al. β Cell GLP-1R signaling alters α cell proglucagon processing after vertical sleeve gastrectomy in mice. Cell Rep. 2018, 23, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Douros, J.D.; Lewis, A.G.; Smith, E.P.; Niu, J.; Capozzi, M.; Wittmann, A.; Campbell, J.; Tong, J.; Wagner, C.; Mahbod, P.; et al. Share enhanced glucose control following vertical sleeve gastrectomy does not require a beta-Cell Glucagon-Like Peptide 1 Receptor. Diabetes 2018, 67, 1504–1511. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Cao, H.; Sheng, C.; Sun, H.; Song, K.; Qu, S. Upregulated Pdx1 and MafA contribute to β-cell function improvement by sleeve gastrectomy. Obes. Surg. 2016, 26, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Grong, E.; Kulseng, B.; Arbo, I.B.; Nord, C.; Eriksson, M.; Ahlgren, U.; Mårvik, R. Sleeve gastrectomy, but not duodenojejunostomy, preserves total beta-cell mass in Goto-Kakizaki rats evaluated by three-dimensional optical projection tomography. Surg. Endosc. 2016, 30, 532–542. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhong, M.W.; Liu, Y.; Sun, D.; Wei, M.; Huang, X.; Cheng, Y.G.; Wu, Q.Z.; Wu, D.; Zhang, X.Q.; et al. Diabetes recurrence after metabolic surgeries correlates with re-impaired insulin sensitivity rather than beta-cell function. World J. Gastroenterol. 2017, 23, 3468–3479. [Google Scholar] [CrossRef]
- Bancalero-de los Reyes, J.; Camacho-Ramírez, A.; Fernández-Vivero, J.; Ribelles-García, A.; Macías-Rodríguez, M.; Almorza-Gomar, D.; Carrasco-Molinillo, C.; Mayo-Ossorio, M.A.; Prada-Oliveira, J.A.; Perez-Arana, G. Glucagon-producing cell expansion in Wistar rats. Changes to islet architecture after sleeve gastrectomy. Obes. Surg. 2021, 31, 2241–2249. [Google Scholar] [CrossRef]
- Huising, M.O.; Lee, S.; Van der Meulen, T. Evidence for a neogenic niche at the periphery of pancreatic islets. Bioessays 2018, 40, e1800119. [Google Scholar] [CrossRef] [PubMed]
- Damsteegt, E.L.; Hassan, Z.; Hewawasam, N.V.; Sarnsamak, K.; Jones, P.M.; Hauge-Evans, A. Novel Role for Somatostatin in the Survival of Mouse Pancreatic Beta Cells AC. Cell Physiol. Biochem. 2019, 52, 486–502. [Google Scholar] [CrossRef] [Green Version]
- Alán, L.; Olejár, T.; Cahová, M.; Zelenka, J.; Berková, Z.; Smětáková, M.; Saudek, F.; Matěj, R.; Ježek, P. Delta Cell Hyperplasia in Adult Goto-Kakizaki (GK/MolTac) Diabetic Rats. J. Diabetes Res. 2015, 2015, 385395. [Google Scholar] [CrossRef] [Green Version]
- DiGruccio, M.R.; Mawla, A.M.; Donaldson, C.J.; Noguchi, G.M.; Vaughan, J.; Cowing-Zitron, C.; van der Meulen, T.; Huising, M.O. Comprehensive alpha, beta and delta cell transcriptomes reveal that ghrelin selectively activates delta cells and promotes somatostatin release from pancreatic islets. Mol. Metab. 2016, 5, 449–458. [Google Scholar] [CrossRef]
- Hayoz, C.; Hermann, T.; Raptis, D.A.; Brönnimann, A.; Peterli, R.; Zuber, M. Comparison of metabolic outcomes in patients undergoing laparoscopic roux-en-Y gastric bypass versus sleeve gastrectomy -a systematic review and meta-analysis of randomised controlled trials. Swiss Med. Wkly. 2018, 148, w14633. [Google Scholar] [CrossRef]
- Inge, T.H.; Prigeon, R.L.; Elder, D.A.; Jenkins, T.M.; Cohen, R.M.; Xanthakos, S.A.; Benoit, S.C.; Dolan, L.M.; Daniels, S.R.; D’Alessio, D.A. Share insulin sensitivity and beta-cell function improve after gastric bypass in severely obese adolescents. J. Pediatr. 2015, 167, 1042–1048.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindqvist, A.; Spégel, P.; Ekelund, M.; Garcia Vaz, E.; Pierzynowski, S.; Gomez, M.F.; Mulder, H.; Hedenbro, J.; Groop, L.; Wierup, N. Gastric bypass improves β-cell function and increases β-cell mass in a porcine model. Diabetes 2014, 63, 1665–1671. [Google Scholar] [CrossRef] [Green Version]
- Patti, M.E.; Goldfine, A.B.; Hu, J.; Hoem, D.; Molven, A.; Goldsmith, J.; Schwesinger, W.H.; La Rosa, S.; Folli, F.; Kulkarni, R.N. Heterogeneity of proliferative markers in pancreatic beta-cells of patients with severe hypoglycemia following Roux-en-Y gastric bypass. Acta Diabetol. 2017, 54, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Guo, W.; Wu, J.; Gong, L.; Li, Q.; Xiao, X.; Zhang, J.; Wang, Z. Increased β-cell mass in obese rats after gastric bypass: A potential mechanism for improving glycemic control. Med. Sci. Monit. 2017, 23, 2151–2158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, M.; Laurenti, M.C.; Man, C.D.; Ma, J.; Cobelli, C.; Rizza, R.A.; Vella, A. Contribution of endogenous glucagon-like peptide-1 to changes in glucose metabolism and islet function in people with type 2 diabetes four weeks after Roux-en-Y gastric bypass (RYGB). Metabolism 2019, 93, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Mokadem, M.; Zechner, J.F.; Margolskee, R.F.; Drucker, D.J.; Aguirre, V. Effects of Roux-en-Y gastric bypass on energy and glucose homeostasis are preserved in two mouse models of functional glucagon-like peptide-1 deficiency. Mol. Metab. 2013, 3, 191–201. [Google Scholar] [CrossRef]
- Guida, C.; Stephen, S.D.; Watson, M.; Dempster, N.; Larraufie, P.; Marjot, T.; Cargill, T.; Rickers, L.; Pavlides, M.; Tomlinson, J.; et al. PYY plays a key role in the resolution of diabetes following bariatric surgery in humans. EBioMedicine 2019, 40, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Furuyama, K.; Chera, S.; van Gurp, L.; Oropeza, D.; Ghila, L.; Damond, N.; Vethe, H.; Paulo, J.A.; Joosten, A.M.; Berney, T.; et al. Diabetes relief in mice by glucose-sensing insulin-secreting human alpha-cells. Nature 2019, 567, 43–48. [Google Scholar] [CrossRef]
- Uchida, A.; Zechner, J.F.; Mani, B.K.; Park, W.M.; Aguirre, V.; Zigman, J.M. Altered ghrelin secretion in mice in response to diet-induced obesity and Roux-en-Y gastric bypass. Mol. Metab. 2014, 3, 717–730. [Google Scholar] [CrossRef]
- Quesada-Candela, C.; Tudurí, E.; Marroquí, L.; Alonso-Magdalena, P.; Quesada, I.; Nadal, A. Morphological and functional adaptations of pancreatic alpha-cells during late pregnancy in the mouse. Metabolism 2020, 102, 153963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinho, T.S.; Borges, C.C.; Aguila, M.B.; Mandarim-de-Lacerda, C.A. Intermittent fasting benefits on alpha- and beta-cell arrangement in diet-induced obese mice pancreatic islet. J. Diabetes Complicat. 2019, 26, 107497. [Google Scholar] [CrossRef] [PubMed]
- Longuet, C.; Robledo, A.M.; Dean, E.D.; Dai, C.; Ali, S.; McGuinness, I.; de Chavez, V.; Vuguin, P.M.; Charron, M.J.; Powers, A.C.; et al. Liver-specific disruption of the murine glucagon receptor produces alpha-cell hyperplasia: Evidence for a circulating alpha-cell growth factor. Diabetes 2013, 62, 1196–1205. [Google Scholar] [CrossRef] [Green Version]
- Patel, K.; Levesque, K.; Mark, V.; Pierini, E.; Rojas, B.; Ahlers, M.; Shah, A.; Laferrère, B. Proinsulin associates with poor β-cell function, glucose-dependent insulinotropic peptide, and insulin resistance in persistent type 2 diabetes after Roux-en-Y gastric bypass in humans. J. Diabetes 2020, 12, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Mitchell, J.E.; Steffen, K.; Engel, S.; Wiisanen, R.; Garcia, L.; Malik, S.A. Recognition and management of hyperinsulinemic hypoglycemia after bariatric surgery. Obes. Res. Clin. Pract. 2016, 10, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Swisa, A.; Glaser, B.; Dor, Y. Metabolic stress and compromised identity of pancreatic beta cells. Front. Genet. 2017, 8, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgia, A.; Asnis, M.C.C.; Febres, G.; Tsang, A.; Bessler, M.; Korner, J. Roux-en-Y Gastric Bypass is associated with hyperinsulinemia but not increased maximal β-cell. Funct. J. Endocr. Soc. 2019, 3, 632–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Research Field (JCR) | Number of Articles Obtained | Number and % of Articles Selected |
|---|---|---|
| Endocrinology & Metabolism | 223 | 22 (46.80%) |
| Surgery | 91 | 6 (12.76%) |
| Cell Biology | 29 | 4 (8.50%) |
| Medicine General & Internal | 27 | 4 (8.50%) |
| Biochemistry & Molecular Biology | 21 | 2 (4.25%) |
| Multidisciplinary Sciences | 14 | 2 (4.25%) |
| Medical Research & Experimental | 11 | 2 (4.25%) |
| Gastroenterology & Hepatology | 11 | 2 (4.25%) |
| Genetics & Heredity | 4 | 1 (2.12%) |
| Pediatrics | 3 | 1 (2.12%) |
| Peripheral Vascular disease | 1 | 1 (2.12%) |
| Total of Research fields | 435 | 47 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Arana, G.-M.; Fernández-Vivero, J.; Camacho-Ramírez, A.; Díaz Gómez, A.; Bancalero de los Reyes, J.; Ribelles-García, A.; Almorza-Gomar, D.; Carrasco-Molinillo, C.; Prada-Oliveira, J.-A. Sleeve Gastrectomy and Roux-En-Y Gastric Bypass. Two Sculptors of the Pancreatic Islet. J. Clin. Med. 2021, 10, 4217. https://doi.org/10.3390/jcm10184217
Pérez-Arana G-M, Fernández-Vivero J, Camacho-Ramírez A, Díaz Gómez A, Bancalero de los Reyes J, Ribelles-García A, Almorza-Gomar D, Carrasco-Molinillo C, Prada-Oliveira J-A. Sleeve Gastrectomy and Roux-En-Y Gastric Bypass. Two Sculptors of the Pancreatic Islet. Journal of Clinical Medicine. 2021; 10(18):4217. https://doi.org/10.3390/jcm10184217
Chicago/Turabian StylePérez-Arana, Gonzalo-Martín, José Fernández-Vivero, Alonso Camacho-Ramírez, Alfredo Díaz Gómez, José Bancalero de los Reyes, Antonio Ribelles-García, David Almorza-Gomar, Carmen Carrasco-Molinillo, and José-Arturo Prada-Oliveira. 2021. "Sleeve Gastrectomy and Roux-En-Y Gastric Bypass. Two Sculptors of the Pancreatic Islet" Journal of Clinical Medicine 10, no. 18: 4217. https://doi.org/10.3390/jcm10184217