1. Introduction
Tinnitus is a condition associated with a continuous noise in the ears or head and can arise as a symptom of many different medical disorders. The condition is very common with a prevalence of 10–15% [
1], but the fundamental mechanisms of tinnitus are still incompletely understood. Although many patients are not unduly troubled, others find the disorder life-changing. These severe cases of tinnitus can be accompanied by anxiety, depression, insomnia, and concentration problems, all of which can impair quality of life.
There is little evidence for effective tinnitus treatments and no licensed pharmacological therapy has been found. The Cochrane Library currently lists nine completed systematic reviews on different tinnitus treatments; namely Tinnitus Retraining Therapy (TRT), Cognitive Behavioral Therapy (CBT), hyperbaric oxygen therapy, sound therapy (masking), hearing aids, repetitive Transcranial Magnetic Stimulation (rTMS), ginkgo biloba, anticonvulsants, and antidepressants (
www.cochranelibrary.com (accessed on 16 September 2021)). In patients with severe and profound sensorineural hearing loss, it was demonstrated that cochlear implantation can lead to a long-lasting reduction of tinnitus symptoms (see e.g., [
2]). However, in the vast majority of tinnitus patients, the hearing loss is not so severe that a cochlear implant is clinically advised. For this general tinnitus patient population, no uniformly effective treatment for tinnitus is identified. One of the important reasons for the lack of clinical evidence is the large heterogeneity of tinnitus cases. Elgoyhen et al. [
3] highlighted the large patient heterogeneity to be one of the major reasons for inconsistent results in studies on tinnitus. Tinnitus can be described on various dimensions such as its etiology, perceptual characteristics of the sound (i.e., pitch and loudness), time since onset, continuous or intermittent sound perception, levels of conscious awareness and perceived distress, and comorbidities. A review by Baguley and colleagues [
4] identified at least 13 different types of causal factors that can be responsible for tinnitus. Hearing loss is the most commonly known risk factor and can result from acute noise trauma, occupational or leisure noise exposure or age-related hearing loss. Somatic tinnitus has been suggested as another cause for tinnitus, where altered muscle tension in the neck or jaw can contribute to the development of tinnitus [
5].
In addition, there is a complex bidirectional interaction between tinnitus and stress. Tinnitus patients often perceive their tinnitus as stressful, intrusive and annoying and a considerable subgroup develops insomnia, attentional and psychological problems such as anxiety or depression as a consequence of the ongoing tinnitus perception [
6,
7]. A bidirectional interaction is suggested because stress can also aggravate tinnitus perception. Many patients report that the onset of their tinnitus was preceded by stressful events [
8,
9,
10]. The stress level and the affective state mediate the relationship between the loudness of the tinnitus and the individually perceived distress of tinnitus [
11]. Furthermore, dynamics of emotions are associated with the course of tinnitus over time [
12], which adds to the complex interaction of tinnitus distress, tinnitus loudness, stress, and emotional perception. This complex interaction was also observed during the first wave of the COVID-19 pandemic. Beukes et al. 2020 [
13] and Schlee et al. 2020 [
14] both investigated the influence of the pandemic on the individual suffering by the chronic tinnitus patients and reported highly hetereogeneous results.
The challenge in tinnitus research is to address this patient heterogeneity by carefully considering the inter-subject differences of the chronic tinnitus patients and draw generalizable logical conclusions from it. It is, therefore, important to analyse the idiosyncratic influence of different factors on the individually perceived tinnitus, apply statistical analysis on the single subject level—and derive nomothetic models at the group level that can be generalized to a larger patient group.
With this analysis, we want to propose a methodological approach that applies statistical analysis at a single case level to consider the patient’s heterogeneity and synthesizes the results at a group level. During a period of six weeks, the patients applied an intervention where it was suspected that the impact on the tinnitus will be heterogeneous. Information about the tinnitus, stress, emotional states, neck and jaw muscle tensions were collected on a daily basis with high ecological validity in the daily environment of the tinnitus patients. The trajectories of tinnitus and related factors were analyzed at a single subject level, categorized into different patient groups, and all results described at the group level. A prerequisite for statistical analysis at the subject level is a large number of data samples over a longer period of time. We used an Ecological Momentary Assessment (EMA) research design where the participants are asked to fill out a short questionnaire one or more times a day. The questionnaire is delivered by a smartphone app to the smartphone owned by the participants and notifications where send as reminders on a regular basis.
The new tinnitus treatment combines an auricular acupressure treatment with self-help intervention. While the auricular acupressure treatment for tinnitus is a new approach, self-help treatment in tinnitus has a long tradition with self-help groups organized by national tinnitus patient associations for several centuries. A systematic review by Nyenhuis et al. [
15] reported that self-help interventions reduced tinnitus distress and depression. However, an understanding of the intervention mechanism is still lacking. Greenwell and colleagues [
16] emphasize that more high-quality research on self-help with better reporting will be needed. In recent years, self-help interventions for tinnitus are implemented in various e-health applications. An overview is given by Kalle et al. 2018 [
17].
Based on pilot data, we assumed the treatment response to be heterogeneous with some participants benefiting from a robust reduction of tinnitus symptoms while other participants benefit only to a small extent or not at all. The aim of this study was to investigate the change of tinnitus and related symptoms during a six week treatment period applying statistical analysis on a single subject level and group level.
4. Discussion
Here we presented a longitudinal observational study on participants with chronic tinnitus that used a combined treatment of acupressure around the ear plus advice for self-help interventions. Over a period of six weeks, the participants reported about their tinnitus and related symptoms via a smartphone app, which allowed tracking of these symptoms with high temporal resolution. Over the period of six weeks, the participants provided on average 123.6 self-report questionnaires. As expected, there was a high within-subject variability of the tinnitus perception as well as a high between-subject variability with heterogenous responses to the tinnitus treatment. For the statistical analysis, we took advantage of a large amount of sampling points per subject, which allowed the fitting of regression models on a single subject model.
4.1. Change of Tinnitus Loudness and Distress
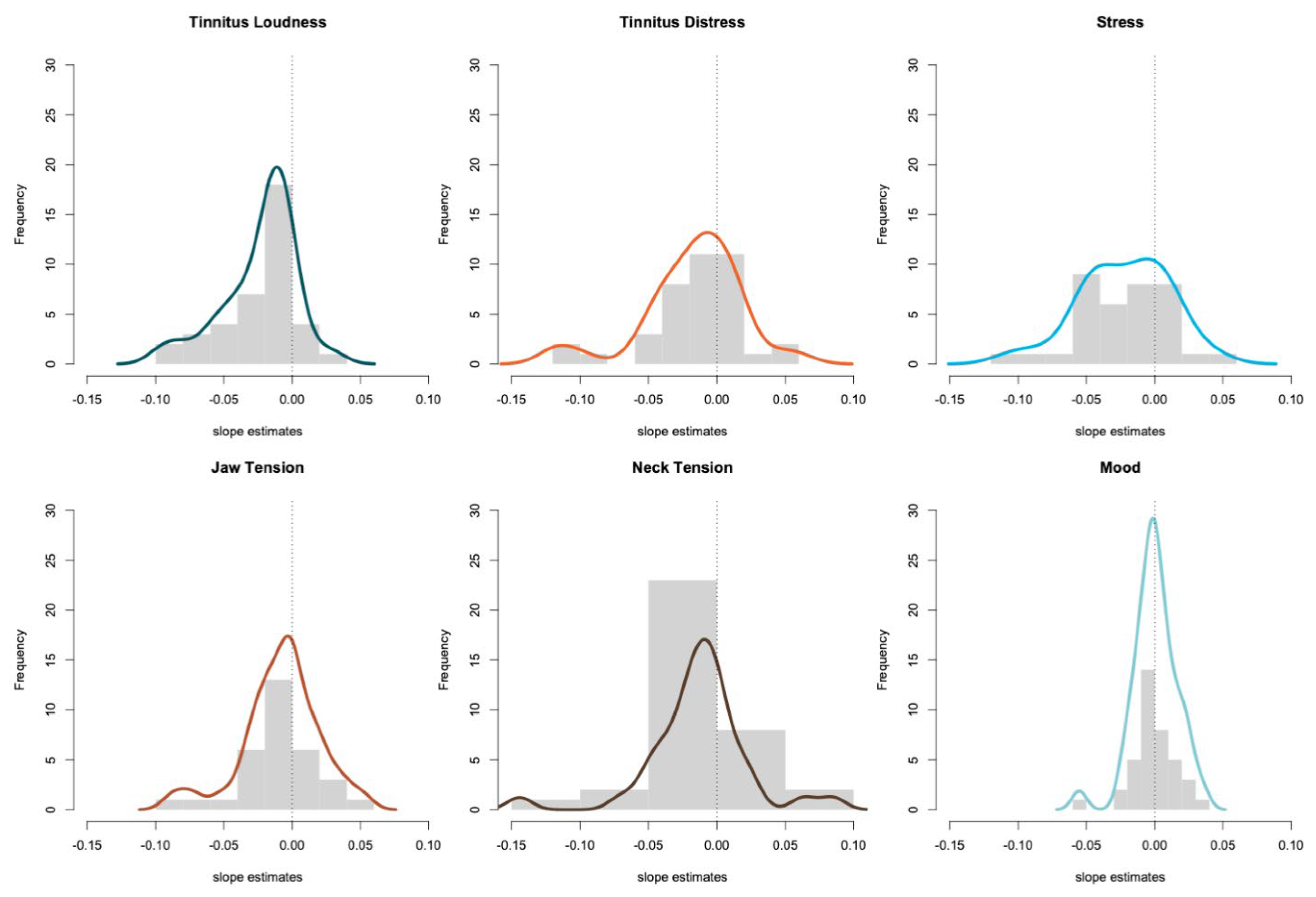
We observed a significant negative trend of tinnitus loudness in 15 out of 39 (38.5%) participants. A significant increase in loudness was detected in only one participant (2.6%). The data of the study group were compared to a matched control group to answer the question if such a change of tinnitus loudness can also occur under naturalistic conditions without intervention. The matched control group was selected from the TrackYourTinnitus study where the participants also used a smartphone app with an identical EMA design. Non-parametrical tests revealed a difference from the slopes for tinnitus loudness and stress between the groups.
The results for tinnitus distress; however, are weaker with only 11 participants (28.2%) showing a significant negative trend and four participants (10.3%) reporting a significant increase. The slopes of tinnitus distress were not significantly different from the slopes of the TrackYourTinnitus sample (all p > 0.05).
In summary, the effects of the combined treatment are stronger for the tinnitus loudness than for tinnitus distress, which is probably in favor for the tinnitus sufferers since a recent analysis by Rademaker et al. 2021 [
23] concluded that tinnitus patients consider loudness the most important outcome measure. With this study, we can only document the changes of tinnitus loudness and distress but cannot identify the underlying therapeutic mechanism. The acupressure device is designed to apply soft pressure at various pre- and post-auricular points. The material of the device is flexible and can be adjusted to the individual ear. This also means that the stimulated points around the ear can slightly differ from day to day depending on the handling of the user. To the best of our knowledge, there is currently no scientific research on acupressure around the ear for treating tinnitus. In principle, it is possible that the device stimulates muscles, fascia, or lymph nodes in this area. Especially in participants with a somatic tinnitus component, a treatment that affects the jaw and neck muscles, directly or indirectly, could be beneficial. The anterior auricular muscles, the superior auricular muscle, and the posterior auricular muscle are the most likely candidates that can be influenced by the acupressure device in use here. In addition, six intrinsic muscles exist. Liguan et al. 2018 [
24] outlined the neuronal connections of these muscles to the brainstem, limbic structures, and the cortex. The temporal fascia and the masseteric fascia are the most likely candidates to be influenced by the acupressure device. The posterior auricular lymph nodes and the preauricular lymph nodes are located in the region that can be stimulated by acupressure device; however, it is not clear if the gentle pressure by the acupressure device can have an effect of lymph drainage to these nodes. More research is needed to investigate the possible mechanisms on auricular acupressure treatment in chronic tinnitus. Future research needs also to disentangle the effects of acupressure and self-help tips. Therefore, it will be important to collect data if the participants read and understood the self-help tips and if they integrated the tip into their daily life. We want to mention here that there are various treatment options for somatic tinnitus currently under scientific evaluation including various devices (e.g., mandibular advancing device, MAD, [
25]) or physical therapy (e.g., Conservative Temporomandibular Therapy [
5]). We are optimistic that combined research efforts in this field can improve the scientific understanding of the somatic tinnitus and the therapeutic mechanisms for improving this condition.
4.2. Changes of Tensions in the Jaw and Neck Muscles
A significant decrease of tensions in the jaw muscles was observed in 40.6% of the participants and a decrease of neck muscle tension in 38.9%. A significant increase of jaw muscle tension was detected in 18.8% and an increase in neck muscle tensions in 11.1%. The distribution of the slope estimates for the jaw tensions was not significantly different from zero while the slope estimates for the neck tensions were significantly lower than zero, with a small effect size of −0.356. Since the jaw and neck muscles have not been investigated in the TrackYourTinnitus study, it was not possible to compare these results to a matched control group. It is, therefore, not possible to decide whether the changes are a result of the intervention or merely reflect a natural fluctuation of the symptom. With visual inspection of the single subject data, it can be hypothesized that there are participants with a temporal relationship between neck muscle tensions and tinnitus symptoms in a way that small increases in muscle tension precede an increase of tinnitus. This will be subject to further research using time series analysis.
4.3. Changes in Mood
With all the statistical analysis that we calculated here, there was no hint that the mood of the participants changed systematically toward either direction. There was only a small number of patients with a significant trend, three participants (7.7%) toward a more negative mood and four participants (10.3%) toward a more positive mood. The slope estimates were not significantly different from zero and the effect size negligible (0.010).
4.4. Changes of Stress
A significant decrease in the stress level was observed during the six weeks period. A significant negative trend of stress was found in 38.9% participants and a positive trend in only 5.6% of the participants. The distribution of the slope estimates was significantly different from zero with a medium to strong effect size of −0.675. The slopes of stress estimates were significantly lower than the slopes of the TrackYourTinnitus sample. The magnitude of stress changes is therefore comparable to the magnitude of changes in tinnitus loudness. This was surprising to us, especially since the reduction of stress is stronger than the reduction of tinnitus distress.
One explanation could be that the reduction of tinnitus loudness leads to a reduction of the stress level of the participant. In this case, we should see a correlation between tinnitus loudness and stress, which was not the case. Post-hoc analysis showed an average correlation between tinnitus loudness and stress of 0.29 while the average correlation between tinnitus loudness and tinnitus distress was 0.71. However, it has to be mentioned here that a correlation analysis only tests for linear relationships. At the moment, we cannot rule out that there is a more complex non-linear or temporal relationship between stress and tinnitus loudness. Another explanation could be that the repeated sampling of stress questionnaires helped the participants to better reflect on their own stress level and develop strategies for effective coping. In this case, the matched control group, which also filled out the questionnaires on stress, should also show a reduction of stress. This, however, was not the case. Therefore, we hypothesize that the stress reduction is a consequence of the intervention—either by the self-help tips or the acupressure. The library of self-help tips consisted of 50 different tips and seven of these tips contained recommendations for coping with stress. It is, therefore, likely that this kind of self-help interventions helped the participants to reduce the general stress level. Additionally, the auricular acupressure is a likely candidate for reducing the stress level. Cha and colleagues [
26] conducted a randomized trial with auricular acupressure over a two-week period and reported a reduction of the self-rated stress level together with a reduction of the blood cortisol level. It is, therefore, possible that the combination of self-help tips and acupressure triggered the decrease of stress in the participants. To find out which part of the intervention contributed to the improvement, it will be of high importance to conduct a randomized clinical study with a cross-over design to systematically vary the application of the two treatment components and assess the clinical improvements and the compliance of the participants with the respective intervention.
4.5. Limitations
One limitation of this observational study design is the lack of a randomized control group. Although a matched control group was used for comparison, a selection bias cannot be ruled out. Therefore, more research is strongly encouraged to investigate the efficacy of the treatment with study designs that allow determining the magnitude of the treatment effect and test if the changes are clinically meaningful. A randomized control trial will be needed to investigate the treatment effects under controlled conditions and reduced bias. In addition, it will be important for the scientific understanding of the intervention to investigate the clinical efficacy of the different treatment components. Based on this data, it is not possible to identify the therapeutic effect of the treatment and it is currently unknown if there is a direct therapeutic effect to the tinnitus or if indirect effects account for the tinnitus improvement. Furthermore, an analysis over a longer time period could reveal long-term changes and test if the improvement persists over time. Such a long-term study should include non-linear analysis to model the asymptotic decline of symptoms toward the zero lines. Given the large he
Heterogeneity of treatment effects among the participants, more research is needed to identify early predictors for the treatment response. A better scientific understanding of the underlying mechanisms of the auricular acupressure and self-help intervention could help to further improve the efficacy of the combinational treatment.








{kind=link}
{kind=link}
{kind=link}