
The Rapid Atrial Swirl Sign for Ultrasound-Guided Tip Positioning of Retrograde-Tunneled Hemodialysis Catheters: A Cross-Sectional Study from a Single Center



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Setting
2.2. Catheter Placement Procedure and Material
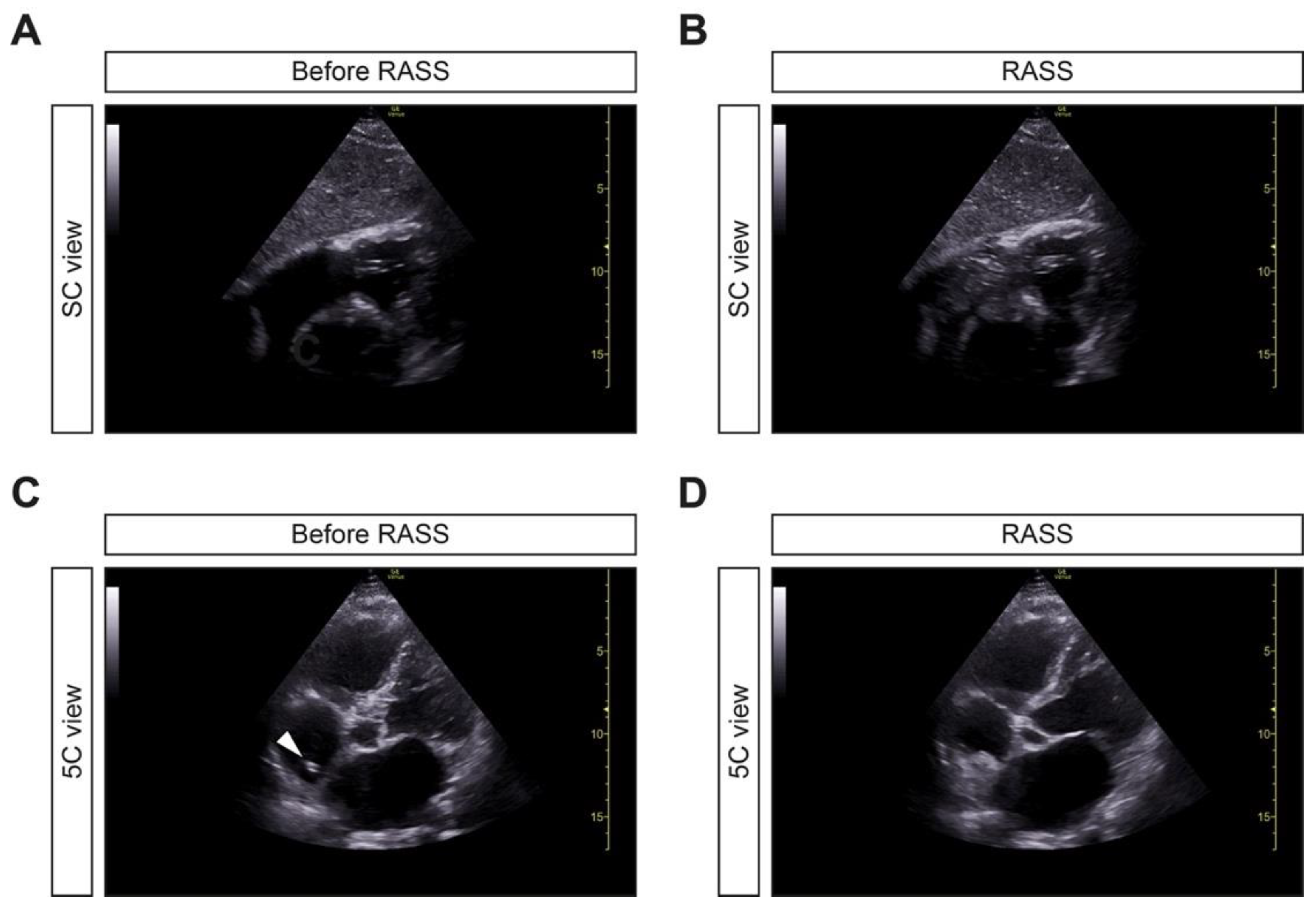
2.3. Ultrasound Visualization and RASS
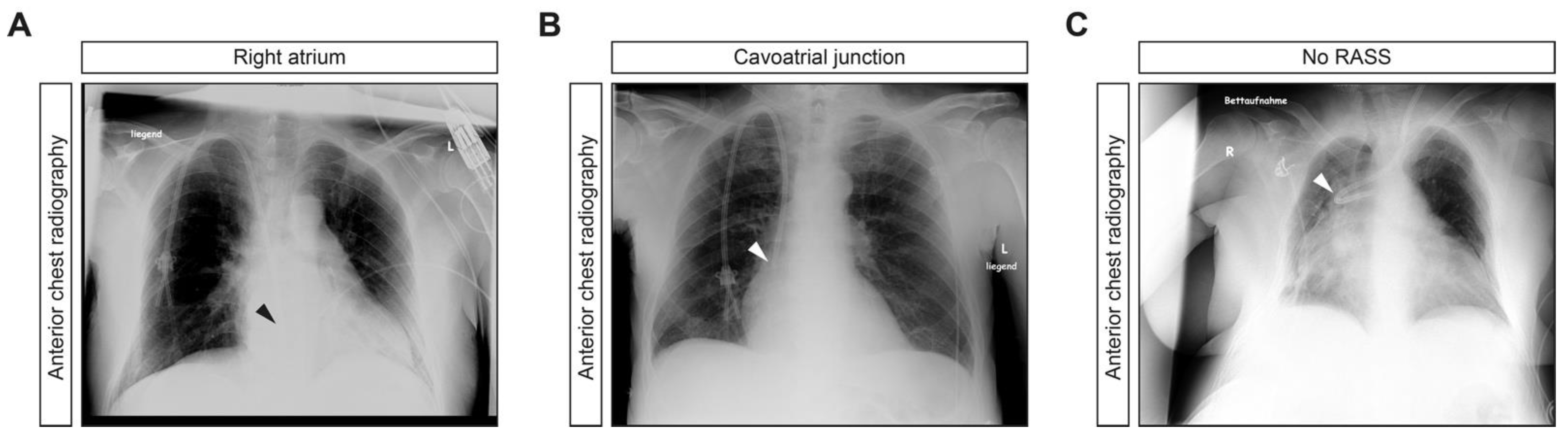
2.4. Post Procedural Assessment
2.5. Patient Consent and Ethics Approval
2.6. Statistical Analysis
3. Results
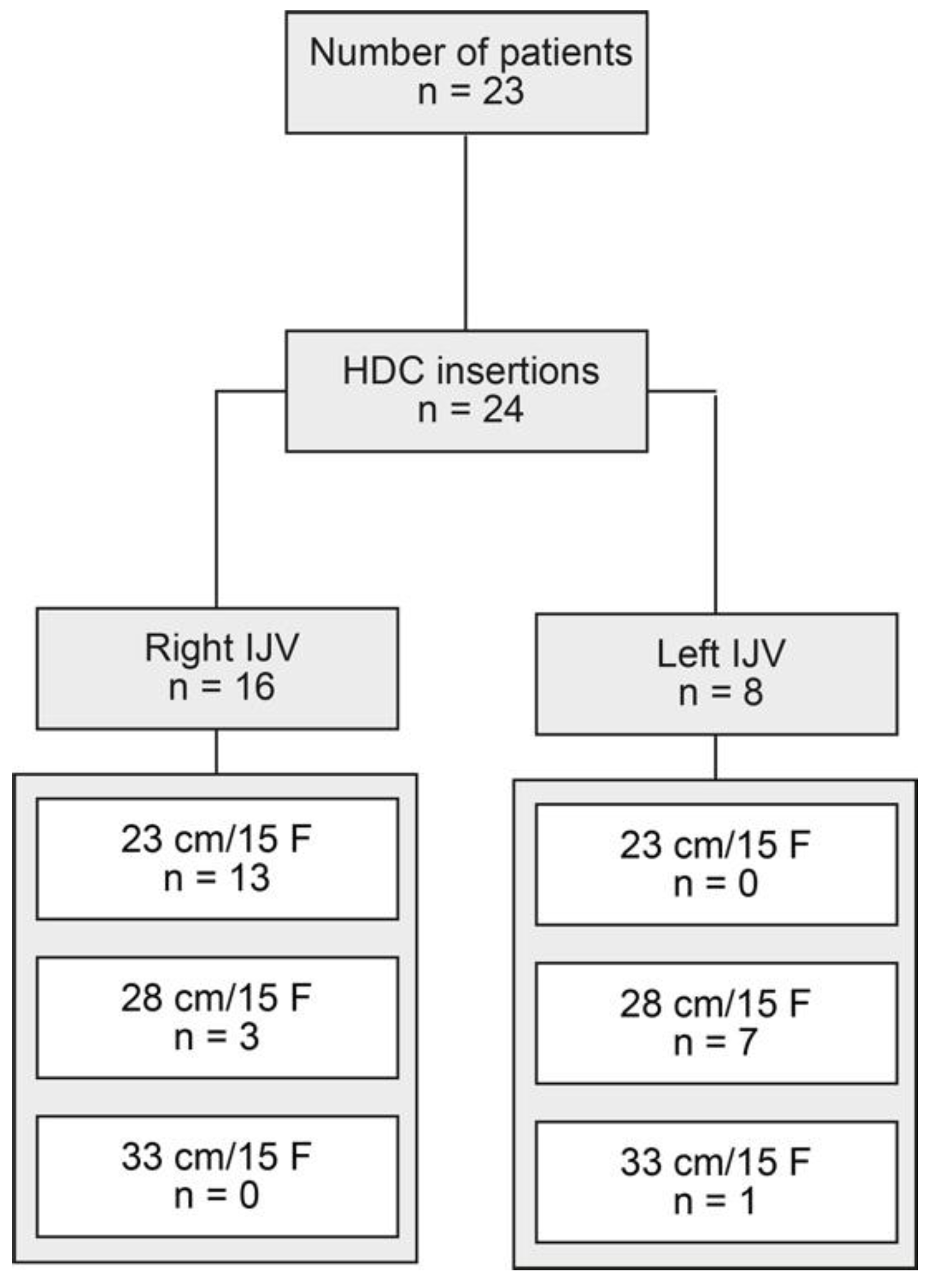
3.1. Study Population
3.2. Application of RAAS for Retrograde-Tunneled HDC Tip Positioning
3.3. Post-Procedural Complications after Retrograde-Tunneled HDC Placement
3.4. Post-Insertion HDC Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Thurlow, J.S.; Joshi, M.; Yan, G.; Norris, K.C.; Agodoa, L.Y.; Yuan, C.M.; Nee, R. Global Epidemiology of End-Stage Kidney Disease and Disparities in Kidney Replacement Therapy. Am. J. Nephrol. 2021, 52, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Griffin, B.R.; Liu, K.D.; Teixeira, J.P. Critical Care Nephrology: Core Curriculum 2020. Am. J. Kidney Dis. 2020, 75, 435–452. [Google Scholar] [CrossRef] [PubMed]
- Lok, C.E.; Huber, T.S.; Lee, T.; Shenoy, S.; Yevzlin, A.S.; Abreo, K.; Allon, M.; Asif, A.; Astor, B.C.; Glickman, M.H.; et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am. J. Kidney Dis. 2020, 75 (Suppl. 2), S1–S164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korsten, P.; Mavropoulou, E.; Wienbeck, S.; Ellenberger, D.; Patschan, D.; Zeisberg, M.; Vasko, R.; Tampe, B.; Müller, G.A. The “rapid atrial swirl sign” for assessing central venous catheters: Performance by medical residents after limited training. PLoS ONE 2018, 13, e0199345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passos, R.D.H.; Ribeiro, M.; da Conceicao, L.; Ramos, J.G.R.; Ribeiro, J.C.; Batista, P.B.P.; Dutra, M.M.D.; Rouby, J.J. Agitated saline bubble-enhanced ultrasound for the positioning of cuffed, tunneled dialysis catheters in patients with end-stage renal disease. J. Vasc. Access 2019, 20, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Elias, R.M.; Makida, S.C.D.S.; Abensur, H.; Castro, M.C.M.; Moyses, R.; Pereira, B.J.; De Oliveira, R.B.; Luders, C.; Egidio, R.J. Insertion of Tunneled Hemodialysis Catheters without Fluoroscopy. J. Vasc. Access 2010, 11, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Bream, P.R., Jr. Update on Insertion and Complications of Central Venous Catheters for Hemodialysis. Semin. Interv. Radiol. 2016, 33, 31–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peritoneal Dialysis Adequacy 2006 Work Group. Clinical practice guidelines for hemodialysis adequacy, update 2006. Am. J. Kidney Dis. 2006, 48 (Suppl. 1), S91–S97. [Google Scholar] [CrossRef] [PubMed]
- Yevzlin, A.; Song, G.; Sanchez, R.; Becker, Y. Fluoroscopically guided vs modified traditional placement of tunneled hemodialysis catheters: Clinical outcomes and cost analysis. J. Vasc. Access 2007, 8, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, D.L.; Balter, S.; Schueler, B.A.; Wagner, L.K.; Strauss, K.J.; Vano, E. Clinical Radiation Management for Fluoroscopically Guided Interventional Procedures. Radiology 2010, 257, 321–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero, J.R.; Frey, J.L.; Schwamm, L.H.; Demaerschalk, B.M.; Chaliki, H.P.; Parikh, G.; Burke, R.F.; Babikian, V.L. Cerebral ischemic events associated with ’bubble study’ for identification of right to left shunts. Stroke 2009, 40, 2343–2348. [Google Scholar] [CrossRef] [PubMed]
- Bassett, G.; Lin, J.; Tran, M.; Sistino, J. Evaluating the potential risks of bubble studies during echocardiography. Perfusion 2014, 30, 219–223. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Data | Value |
| Median age (IQR)—years | 71 (56–76) |
| Female sex—no. (%) | 7 (30.4) |
| Median height (IQR)—cm | 172 (166–180) |
| Median BW (IQR)—kg | 85 (75.5–104) |
| Median BMI (IQR)—kg/m2 | 30.5 (23.9–33.6) |
| History of previous catheterization—no. (%) | 2 (8.7) |
| Etiology of ESKD | Value |
| Diabetic nephropathy—no. (%) | 7 (30.4) |
| Cardiorenal syndrome—no. (%) | 3 (13) |
| ANCA GN—no. (%) | 2 (8.7) |
| Septic shock—no. (%) | 2 (8.7) |
| Multiple myeloma/cast nephropathy—no. (%) | 2 (8.7) |
| IgAN—no. (%) | 1 (4.3) |
| Hypertensive nephropathy—no. (%) | 1 (4.3) |
| Cardiogenic shock—no. (%) | 1 (4.3) |
| Hemorrhagic shock—no. (%) | 1 (4.3) |
| Chemotherapy nephrotoxicity—no. (%) | 1 (4.3) |
| Fibrillary GN | 1 (4.3) |
| ADPKD | 1 (4.3) |
| Laboratory Data | Value |
| Median platelet count (IQR)—×1000/μL | 211 (108.3–317) |
| Median INR (IQR)—ratio | 1.15 (1–1.2) |
| Median aPTT (IQR)—seconds | 30 (28–34.3) |
| Hemoglobin—g/dL | 8.4 (7.7–9.5) |
| Vascular Access | Value |
| Right IJV—no. (%) | 16 (66.7) |
| Left IJV—no. (%) | 8 (33.3) |
| Catheter Length/Diameter | Value |
| 23 cm/15 F—no. (%) | 13 (54.2) |
| 28 cm/15 F—no. (%) | 10 (41.7) |
| 33 cm/15 F—no. (%) | 1 (4.2) |
| Chest Radiography Position | RASS | No RASS |
|---|---|---|
| Right atrium—no. (%) | 18 (75) | 0 (0) |
| Cavoatrial junction—no. (%) | 5 (20.8) | 0 (0) |
| Subclavian-caval junction—no. (%) | 0 (0) | 1 (4.2) |
| Complications | Value |
|---|---|
| Arterial puncture—no. (%) | 0 (0) |
| Pneumothorax—no. (%) | 0 (0) |
| Hemothorax—no. (%) | 0 (0) |
| Minor bleeding—no. (%) | 2 (8.3) |
| Dialysis Parameters | Value |
|---|---|
| Malfunction—no. (%) | 0 (0) |
| Median blood flow (IQR)—mL/min | 200 (200–250) |
| Median TMP (IQR)—mmHg | 40 (20–60) |
| Median venous pressure (IQR)—mmHg | 100 (80–120) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korsten, P.; Kuczera, T.; Wallbach, M.; Tampe, B. The Rapid Atrial Swirl Sign for Ultrasound-Guided Tip Positioning of Retrograde-Tunneled Hemodialysis Catheters: A Cross-Sectional Study from a Single Center. J. Clin. Med. 2021, 10, 3999. https://doi.org/10.3390/jcm10173999
Korsten P, Kuczera T, Wallbach M, Tampe B. The Rapid Atrial Swirl Sign for Ultrasound-Guided Tip Positioning of Retrograde-Tunneled Hemodialysis Catheters: A Cross-Sectional Study from a Single Center. Journal of Clinical Medicine. 2021; 10(17):3999. https://doi.org/10.3390/jcm10173999
Chicago/Turabian StyleKorsten, Peter, Tim Kuczera, Manuel Wallbach, and Björn Tampe. 2021. "The Rapid Atrial Swirl Sign for Ultrasound-Guided Tip Positioning of Retrograde-Tunneled Hemodialysis Catheters: A Cross-Sectional Study from a Single Center" Journal of Clinical Medicine 10, no. 17: 3999. https://doi.org/10.3390/jcm10173999