
Nociplastic Pain Criteria or Recognition of Central Sensitization? Pain Phenotyping in the Past, Present and Future

 , ,
, ,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. The Past
3. The Present
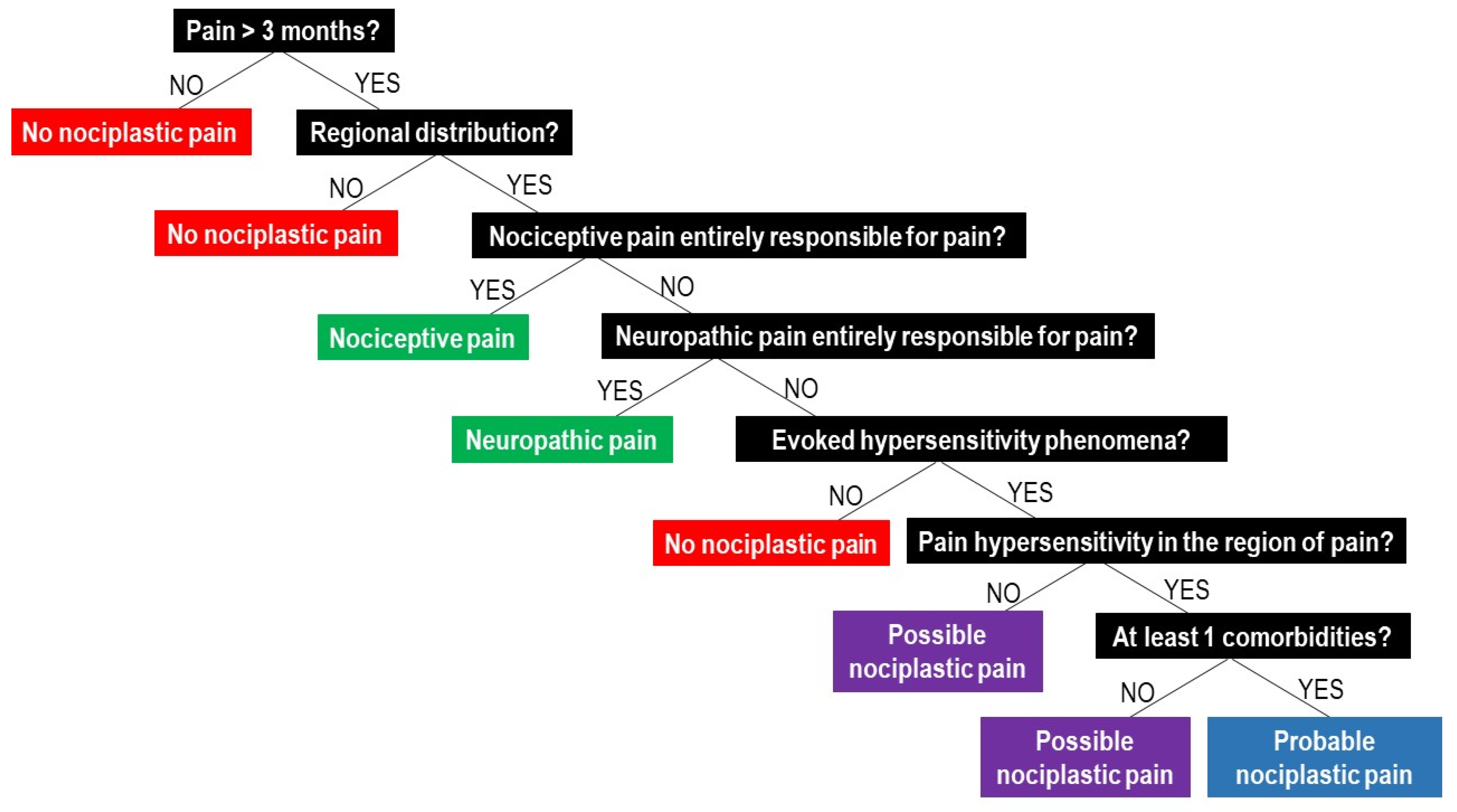
- (1)
- report pain of at least 3 months duration;
- (2)
- report a regional rather than discrete pain distribution;
- (3)
- report pain that cannot entirely be explained by nociceptive or neuropathic mechanisms;
- (4)
- show clinical signs of pain hypersensitivity (i.e., evoked pain hypersensitivity phenomena such as static or dynamic mechanical allodynia, heat or cold allodynia, and/or painful after-sensations after any of the mentioned evoked pain hypersensitivity assessments) that are at least present in the region of pain [44].
Comparing the IASP Clinical Criteria for Nociplastic Pain with the 2014 Clinical Criteria for Predominant Central Sensitization Pain
4. The Future
4.1. Towards Precision Pain Medicine?
4.2. Research Agenda
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Terminology (Presented in Alphabetic Order)
| Term | Explanation |
| Central sensitization | A neurophysiological mechanism, defined as ‘amplification of neural signalling within the central nervous system that elicits pain hypersensitivity [7],’ potentially explains chronic, nonspecific pain. |
| Central nervous system sensitization | Refers to ‘central sensitization.’ |
| Chronic pain | Pain of at least 3 months duration. |
| Endogenous analgesia | The body’s ability to activate pain relief, with poor endogenous analgesia considered a feature of central sensitization [17]. |
| Neuropathic pain | Pain due to a lesion or a disease of the nervous system. |
| Nociceptive pain | Pain due to damage to non-neural tissue (e.g., musculoskeletal or visceral tissue). |
| Nociplastic pain | Pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing the pain [43]. |
| Nonspecific pain | Pain that cannot be explained by tissue damage, pathology or local dysfunctions. |
References
- Roberts, N.L.; Mountjoy-Venning, W.C.; Anjomshoa, M.; Banoub, J.A.M.; Yasin, Y.J. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021, 396, 2006–2017. [Google Scholar] [CrossRef]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Andersson, G.B. Epidemiological features of chronic low-back pain. Lancet 1999, 354, 581–585. [Google Scholar] [CrossRef]
- Waddell, G.; Burton, A.K. Occupational health guidelines for the management of low back pain at work: Evidence review. Occup. Med. 2001, 51, 124–135. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; Leysen, L.; Adriaenssens, N.; Aguilar Ferrandiz, M.E.; Devoogdt, N.; Tassenoy, A.; Ickmans, K.; Goubert, D.; van Wilgen, C.P.; Wijma, A.J.; et al. Pain following cancer treatment: Guidelines for the clinical classification of predominant neuropathic, nociceptive and central sensitization pain. Acta Oncol. 2016, 55, 659–663. [Google Scholar] [CrossRef] [Green Version]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Nijs, J.; Leysen, L.; Vanlauwe, J.; Logghe, T.; Ickmans, K.; Polli, A.; Malfliet, A.; Coppieters, I.; Huysmans, E. Treatment of central sensitization in patients with chronic pain: Time for change? Expert Opin. Pharmacother. 2019, 20, 1961–1970. [Google Scholar] [CrossRef]
- Merskey, H.; Bogduk, N. Part III: Pain Terms, A Current List with Definitions and Notes on Usage. In Classification of Chronic Pain, 2nd ed.; IASP Press: Seattle, WA, USA, 1994; pp. 209–214. [Google Scholar]
- Staud, R.; Craggs, J.G.; Perlstein, W.M.; Robinson, M.E.; Price, D.D. Brain activity associated with slow temporal summation of C-fiber evoked pain in fibromyalgia patients and healthy controls. Eur. J. Pain 2008, 12, 1078–1089. [Google Scholar] [CrossRef]
- van Ettinger-Veenstra, H.; Lundberg, P.; Alfoldi, P.; Sodermark, M.; Graven-Nielsen, T.; Sjors, A.; Engstrom, M.; Gerdle, B. Chronic widespread pain patients show disrupted cortical connectivity in default mode and salience networks, modulated by pain sensitivity. J. Pain Res. 2019, 12, 1743–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifert, F.; Maihofner, C. Central mechanisms of experimental and chronic neuropathic pain: Findings from functional imaging studies. Cell Mol. Life Sci. 2009, 66, 375–390. [Google Scholar] [CrossRef]
- Bosma, R.L.; Mojarad, E.A.; Leung, L.; Pukall, C.; Staud, R.; Stroman, P.W. FMRI of spinal and supra-spinal correlates of temporal pain summation in fibromyalgia patients. Hum. Brain Mapp. 2016, 37, 1349–1360. [Google Scholar] [CrossRef] [Green Version]
- Yarnitsky, D. Conditioned pain modulation (the diffuse noxious inhibitory control-like effect): Its relevance for acute and chronic pain states. Curr. Opin. Anaesthesiol. 2010, 23, 611–615. [Google Scholar] [CrossRef]
- Gebhart, G.F.; Schmidt, R.F. (Eds.) Endogenous Analgesia System. In Encyclopedia of Pain; Springer: Berlin/Heidelberg, Germany, 2013; p. 1144. [Google Scholar]
- Nijs, J.; Van Houdenhove, B.; Oostendorp, R.A. Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice. Man. Ther. 2010, 15, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central sensitisation in chronic pain conditions: Latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Van Oosterwijck, J.; Nijs, J.; Meeus, M.; Paul, L. Evidence for central sensitization in chronic whiplash: A systematic literature review. Eur. J. Pain 2013, 17, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Arendt-Nielsen, L.; Graven-Nielsen, T. Central sensitization in fibromyalgia and other musculoskeletal disorders. Curr. Pain Headache Rep. 2003, 7, 355–361. [Google Scholar] [CrossRef]
- Lluch, E.; Torres, R.; Nijs, J.; Van Oosterwijck, J. Evidence for central sensitization in patients with osteoarthritis pain: A systematic literature review. Eur. J. Pain 2014, 18, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Levy, D.; Jakubowski, M. Effects of sensitization of trigeminovascular neurons to triptan therapy during migraine. Rev. Neurol. 2005, 161, 658–660. [Google Scholar] [CrossRef]
- Chalaye, P.; Goffaux, P.; Bourgault, P.; Lafrenaye, S.; Devroede, G.; Watier, A.; Marchand, S. Comparing Pain Modulation and Autonomic Responses in Fibromyalgia and Irritable Bowel Syndrome Patients. Clin. J. Pain 2012, 28, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Meeus, M.; Van Oosterwijck, J.; Ickmans, K.; Moorkens, G.; Hans, G.; De Clerck, L.S. In the mind or in the brain? Scientific evidence for central sensitisation in chronic fatigue syndrome. Eur. J. Clin. Investig. 2012, 42, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Pas, R.; Ickmans, K.; Van Oosterwijck, S.; Van der Cruyssen, K.; Foubert, A.; Leysen, L.; Nijs, J.; Meeus, M. Hyperexcitability of the Central Nervous System in Children with Chronic Pain: A Systematic Review. Pain Med. 2018, 19, 2504–2514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roussel, N.A.; Nijs, J.; Meeus, M.; Mylius, V.; Fayt, C.; Oostendorp, R. Central sensitization and altered central pain processing in chronic low back pain: Fact or myth? Clin. J. Pain 2013, 29, 625–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfliet, A.; Kregel, J.; Cagnie, B.; Kuipers, M.; Dolphens, M.; Roussel, N.; Meeus, M.; Danneels, L.; Bramer, W.M.; Nijs, J. Lack of evidence for central sensitization in idiopathic, non-traumatic neck pain: A systematic review. Pain Phys. 2015, 18, 223–236. [Google Scholar]
- Meeus, M.; Vervisch, S.; De Clerck, L.S.; Moorkens, G.; Hans, G.; Nijs, J. Central sensitization in patients with rheumatoid arthritis: A systematic literature review. Semin. Arthritis Rheum. 2012, 41, 556–567. [Google Scholar] [CrossRef]
- Coombes, B.K.; Bisset, L.; Vicenzino, B. Thermal hyperalgesia distinguishes those with severe pain and disability in unilateral lateral epicondylalgia. Clin. J. Pain 2012, 28, 595–601. [Google Scholar] [CrossRef] [Green Version]
- Plinsinga, M.L.; Brink, M.S.; Vicenzino, B.; van Wilgen, C.P. Evidence of Nervous System Sensitization in Commonly Presenting and Persistent Painful Tendinopathies: A Systematic Review. J. Orthop. Sports Phys. Ther. 2015, 45, 864–875. [Google Scholar] [CrossRef] [Green Version]
- Sanchis, M.N.; Lluch, E.; Nijs, J.; Struyf, F.; Kangasperko, M. The role of central sensitization in shoulder pain: A systematic literature review. Semin. Arthritis Rheum. 2015, 44, 710–716. [Google Scholar] [CrossRef]
- Smart, K.M.; Blake, C.; Staines, A.; Doody, C. Self-reported pain severity, quality of life, disability, anxiety and depression in patients classified with ‘nociceptive’, ‘peripheral neuropathic’ and ‘central sensitisation’ pain. The discriminant validity of mechanisms-based classifications of low back (+/−eg) pain. Man. Ther. 2012, 17, 119–125. [Google Scholar] [CrossRef]
- Coombes, B.K.; Bisset, L.; Vicenzino, B. Cold hyperalgesia associated with poorer prognosis in lateral epicondylalgia: A 1-year prognostic study of physical and psychological factors. Clin. J. Pain 2015, 31, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Sterling, M.; Jull, G.; Kenardy, J. Physical and psychological factors maintain long-term predictive capacity post-whiplash injury. Pain 2006, 122, 102–108. [Google Scholar] [CrossRef]
- Kim, S.H.; Yoon, K.B.; Yoon, D.M.; Yoo, J.H.; Ahn, K.R. Influence of Centrally Mediated Symptoms on Postoperative Pain in Osteoarthritis Patients Undergoing Total Knee Arthroplasty: A Prospective Observational Evaluation. Pain Pract. Off. J. World Inst. Pain 2015, 15, E46–E53. [Google Scholar] [CrossRef] [PubMed]
- Aguilar Ferrandiz, M.E.; Nijs, J.; Gidron, Y.; Roussel, N.; Vanderstraeten, R.; Van Dyck, D.; Huysmans, E.; De Kooning, M. Auto-Targeted Neurostimulation Is Not Superior to Placebo in Chronic Low Back Pain: A Fourfold Blind Randomized Clinical Trial. Pain Phys. 2016, 19, E707–E719. [Google Scholar]
- Jull, G.; Sterling, M.; Kenardy, J.; Beller, E. Does the presence of sensory hypersensitivity influence outcomes of physical rehabilitation for chronic whiplash?—A preliminary RCT. Pain 2007, 129, 28–34. [Google Scholar] [CrossRef]
- Gwilym, S.E.; Oag, H.C.; Tracey, I.; Carr, A.J. Evidence that central sensitisation is present in patients with shoulder impingement syndrome and influences the outcome after surgery. J. Bone Jt. Surg. Br. Vol. 2011, 93, 498–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valencia, C.; Fillingim, R.B.; Bishop, M.; Wu, S.S.; Wright, T.W.; Moser, M.; Farmer, K.; George, S.Z. Investigation of central pain processing in postoperative shoulder pain and disability. Clin. J. Pain 2014, 30, 775–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, E.E.; Walsh, K.M.; Thompson, N.R.; Krishnaney, A.A. Central Sensitization Inventory as a Predictor of Worse Quality of Life Measures and Increased Length of Stay Following Spinal Fusion. World Neurosurg. 2017, 104, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Yarnitsky, D.; Crispel, Y.; Eisenberg, E.; Granovsky, Y.; Ben-Nun, A.; Sprecher, E.; Best, L.A.; Granot, M. Prediction of chronic post-operative pain: Pre-operative DNIC testing identifies patients at risk. Pain 2008, 138, 22–28. [Google Scholar] [CrossRef]
- Falla, D.; Hodges, P.W. Individualized Exercise Interventions for Spinal Pain. Exerc. Sport Sci. Rev. 2017, 45, 105–115. [Google Scholar] [CrossRef]
- Kosek, E.; Cohen, M.; Baron, R.; Gebhart, G.F.; Mico, J.A.; Rice, A.S.; Rief, W.; Sluka, A.K. Do we need a third mechanistic descriptor for chronic pain states? Pain 2016, 157, 1382–1386. [Google Scholar] [CrossRef]
- International Association for the Study of Pain (IASP). IASP Terminology. Available online: https://www.iasp-pain.org/terminology?navItemNumber=576#Centralsensitization (accessed on 28 March 2019).
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.A.; Rice, A.S.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Torres-Cueco, R.; van Wilgen, C.P.; Girbes, E.L.; Struyf, F.; Roussel, N.; van Oosterwijck, J.; Daenen, L.; Kuppens, K.; Vanwerweeen, L.; et al. Applying modern pain neuroscience in clinical practice: Criteria for the classification of central sensitization pain. Pain Phys. 2014, 17, 447–457. [Google Scholar] [CrossRef]
- Smart, K.M.; Blake, C.; Staines, A.; Doody, C. Clinical indicators of ‘nociceptive’, ‘peripheral neuropathic’ and ‘central’ mechanisms of musculoskeletal pain. A Delphi survey of expert clinicians. Man. Ther. 2010, 15, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Smart, K.M.; Blake, C.; Staines, A.; Doody, C. The Discriminative validity of “nociceptive,” “peripheral neuropathic,” and “central sensitization” as mechanisms-based classifications of musculoskeletal pain. Clin. J. Pain 2011, 27, 655–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smart, K.M.; Blake, C.; Staines, A.; Thacker, M.; Doody, C. Mechanisms-based classifications of musculoskeletal pain: Part 1 of 3: Symptoms and signs of central sensitisation in patients with low back (+/−leg) pain. Man. Ther. 2012, 17, 336–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lluch Girbes, E.; Duenas, L.; Barbero, M.; Falla, D.; Baert, I.A.; Meeus, M.; Sanchez-Frutos, J.; Aguilella, L.; Nijs, J. Expanded Distribution of Pain as a Sign of Central Sensitization in Individuals With Symptomatic Knee Osteoarthritis. Phys. Ther. 2016, 96, 1196–1207. [Google Scholar] [CrossRef] [Green Version]
- Margolis, R.B.; Tait, R.C.; Krause, S.J. A rating system for use with patient pain drawings. Pain 1986, 24, 57–65. [Google Scholar] [CrossRef]
- Margolis, R.B.; Chibnall, J.T.; Tait, R.C. Test-retest reliability of the pain drawing instrument. Pain 1988, 33, 49–51. [Google Scholar] [CrossRef]
- Caseiro, M.; Woznowski-Vu, A.; De Oliveira, A.S.; Reis, F.J.J.; Wideman, T.H. From Paper to Digitalized Body Map: A Reliability Study of the Pain Area. Pain Pract. 2019, 19, 602–608. [Google Scholar] [CrossRef]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The development and psychometric validation of the central sensitization inventory. Pain Pract. Off. J. World Inst. Pain 2012, 12, 276–285. [Google Scholar] [CrossRef] [Green Version]
- Scerbo, T.; Colasurdo, J.; Dunn, S.; Unger, J.; Nijs, J.; Cook, C. Measurement Properties of the Central Sensitization Inventory: A Systematic Review. Pain Pract. Off. J. World Inst. Pain 2018, 18, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.R.; Nijs, J.; Yeowell, G.; Holmes, P.; Goodwin, P.C. Trait Sensitivity, Anxiety and Personality are predictive of Central Sensitisation Symptoms in Patients with Chronic Low Back Pain. Pain Pract. 2019, 19, 800–810. [Google Scholar] [CrossRef] [PubMed]
- Lluch, E.; Nijs, J.; Courtney, C.A.; Rebbeck, T.; Wylde, V.; Baert, I.; Wideman, T.H.; Howells, N.; Skou, S.T. Clinical descriptors for the recognition of central sensitization pain in patients with knee osteoarthritis. Disabil. Rehabil. 2018, 40, 2836–2845. [Google Scholar] [CrossRef]
- Nijs, J.; Apeldoorn, A.; Hallegraeff, H.; Clark, J.; Smeets, R.; Malfliet, A.; Girbes, E.L.; De Kooning, M.; Ickmans, K. Low back pain: Guidelines for the clinical classification of predominant neuropathic, nociceptive, or central sensitization pain. Pain Phys. 2015, 18, E333–E346. [Google Scholar] [CrossRef] [PubMed]
- Levesque, A.; Riant, T.; Ploteau, S.; Rigaud, J.; Labat, J.J. Clinical Criteria of Central Sensitization in Chronic Pelvic and Perineal Pain (Convergences PP Criteria): Elaboration of a Clinical Evaluation Tool Based on Formal Expert Consensus. Pain Med. 2018, 19, 2009–2015. [Google Scholar] [CrossRef] [PubMed]
- Arendt-Nielsen, L. Central sensitization in humans: Assessment and pharmacology. Handb. Exp. Pharmacol. 2015, 227, 79–102. [Google Scholar] [CrossRef] [PubMed]
- Chua, N.H.; van Suijlekom, H.A.; Vissers, K.C.; Arendt-Nielsen, L.; Wilder-Smith, O.H. Differences in sensory processing between chronic cervical zygapophysial joint pain patients with and without cervicogenic headache. Cephalalgia Int. J. Headache 2011, 31, 953–963. [Google Scholar] [CrossRef]
- Finan, P.H.; Buenaver, L.F.; Bounds, S.C.; Hussain, S.; Park, R.J.; Haque, U.J.; Campbell, C.M.; Haythornthwaite, J.A.; Edwards, R.R.; Smith, M.T. Discordance between pain and radiographic severity in knee osteoarthritis: Findings from quantitative sensory testing of central sensitization. Arthritis Rheum. 2013, 65, 363–372. [Google Scholar] [CrossRef] [Green Version]
- La Touche, R.; Paris-Alemany, A.; Hidalgo-Pérez, A.; López-de-Uralde-Villanueva, I.; Angulo-Diaz-Parreño, S.; Muñoz-García, D. Evidence for Central Sensitization in Patients with Temporomandibular Disorders: A Systematic Review and Meta-analysis of Observational Studies. Pain Pract. Off. J. World Inst. Pain 2018, 18, 388–409. [Google Scholar] [CrossRef]
- Pfau, D.B.; Krumova, E.K.; Treede, R.D.; Baron, R.; Toelle, T.; Birklein, F.; Eich, W.; Geber, C.; Gerhardt, A.; Weiss, T.; et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Reference data for the trunk and application in patients with chronic postherpetic neuralgia. Pain 2014, 155, 1002–1015. [Google Scholar] [CrossRef]
- Meacham, K.; Shepherd, A.; Mohapatra, D.P.; Haroutounian, S. Neuropathic Pain: Central vs. Peripheral Mechanisms. Curr. Pain Headache Rep. 2017, 21, 28. [Google Scholar] [CrossRef] [PubMed]
- Chesterton, L.S.; Sim, J.; Wright, C.C.; Foster, N.E. Interrater reliability of algometry in measuring pressure pain thresholds in healthy humans, using multiple raters. Clin. J. Pain 2007, 23, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Cathcart, S.; Pritchard, D. Reliability of pain threshold measurement in young adults. J. Headache Pain 2006, 7, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, A.A. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain 1987, 30, 115–126. [Google Scholar] [CrossRef]
- Malfliet, A.; Bilterys, T.; Van Looveren, E.; Meeus, M.; Danneels, L.; Ickmans, K.; Cagnie, B.; Mairesse, O.; Neu, D.; Moens, M.; et al. The added value of cognitive behavioral therapy for insomnia to current best evidence physical therapy for chronic spinal pain: Protocol of a randomized controlled clinical trial. Braz. J. Phys. 2019, 23, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.D.; Jensen, T.S.; Campbell, J.N.; Cruccu, G.; Dostrovsky, J.O.; Griffin, J.W.; Hansson, P.; Hughes, R.; Nurmikko, T.; Serra, J. Neuropathic pain: Redefinition and a grading system for clinical and research purposes. Neurology 2008, 70, 1630–1635. [Google Scholar] [CrossRef]
- National Research Council Committee on, The National Academies Collection: Reports funded by National Institutes of Health. In Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease; National Academies Press: Washington, DC, USA, 2011.
- Nijs, J.; Paul van Wilgen, C.; Van Oosterwijck, J.; van Ittersum, M.; Meeus, M. How to explain central sensitization to patients with ’unexplained’ chronic musculoskeletal pain: Practice guidelines. Man. Ther. 2011, 16, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; D’Hondt, E.; Clarys, P.; Deliens, T.; Polli, A.; Malfliet, A.; Coppieters, I.; Willaert, W.; Tumkaya Yilmaz, S.; Elma, Ö.; et al. Lifestyle and Chronic Pain across the Lifespan: An Inconvenient Truth? PM R J. Inj. Funct. Rehabil. 2020, 12, 410–419. [Google Scholar] [CrossRef]
- Nijs, J.; Mairesse, O.; Neu, D.; Leysen, L.; Danneels, L.; Cagnie, B.; Meeus, M.; Moens, M.; Ickmans, K.; Goubert, D. Sleep Disturbances in Chronic Pain: Neurobiology, Assessment, and Treatment in Physical Therapist Practice. Phys. Ther. 2018, 98, 325–335. [Google Scholar] [CrossRef]
- Okifuji, A.; Hare, B.D. The association between chronic pain and obesity. J. Pain Res. 2015, 8, 399–408. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; Loggia, M.L.; Polli, A.; Moens, M.; Huysmans, E.; Goudman, L.; Meeus, M.; Vanderweeen, L.; Ickmans, K.; Clauw, D. Sleep disturbances and severe stress as glial activators: Key targets for treating central sensitization in chronic pain patients? Expert Opin. Ther. Targets 2017, 21, 817–826. [Google Scholar] [CrossRef]
- Nugraha, B.; Karst, M.; Engeli, S.; Gutenbrunner, C. Brain-derived neurotrophic factor and exercise in fibromyalgia syndrome patients: A mini review. Rheumatol. Int. 2012, 32, 2593–2599. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Tumkaya Yilmaz, S.; Elma, Ö.; Tatta, J.; Mullie, P.; Vanderweeën, L.; Clarys, P.; Deliens, T.; Coppieters, I.; Weltens, N.; et al. Nutritional intervention in chronic pain: An innovative way of targeting central nervous system sensitization? Expert Opin. Ther. Targets 2020, 24, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Wijma, A.J.; van Wilgen, C.P.; Meeus, M.; Nijs, J. Clinical biopsychosocial physiotherapy assessment of patients with chronic pain: The first step in pain neuroscience education. Physiother. Theory Pract. 2016, 32, 368–384. [Google Scholar] [CrossRef] [PubMed]
- Wilks, T. The Use of Vignettes in Qualitative Research into Social Work Values. Qual. Soc. Work 2004, 3, 78–87. [Google Scholar] [CrossRef]
- Jindal, A.; Ctori, I.; Fidalgo, B.; Dabasia, P.; Balaskas, K.; Lawrenson, J.G. Impact of optical coherence tomography on diagnostic decision-making by UK community optometrists: A clinical vignette study. Ophthalmic Physiol. Opt. 2019, 39, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Haider, I.; Luetsch, K. Pharmacists’ advice and clinical reasoning in relation to cardiovascular disease risk factors-A vignette case study. Res. Soc. Adm. Pharm. RSAP 2020, 16, 568–573. [Google Scholar] [CrossRef]
- Ulrich Connie, M.; Ratcliffe Sarah, J. Hypothetical Vignettes in Empirical Bioethics Research. In Empirical Methods for Bioethics: A Primer; Liva, J., Laura, A.S., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2007; Volume 11, pp. 161–181. [Google Scholar]
- St Marie, B.; Jimmerson, A.; Perkhounkova, Y.; Herr, K. Developing and Establishing Content Validity of Vignettes for Health Care Education and Research. West. J. Nurs. Res. 2021, 43, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Steiner, P.M.; Atzmüller, C.; Su, D. Designing Valid and Reliable Vignette Experiments for Survey Research: A Case Study on the Fair Gender Income Gap. J. Methods Meas. Soc. Sci. 2016, 7, 52–94. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.R.; Dworkin, R.H.; Turk, D.C.; Angst, M.S.; Dionne, R.; Freeman, R.; Hansson, P.; Haroutounian, S.; Arendt-Nielsen, L.; Attal, N.; et al. Patient phenotyping in clinical trials of chronic pain treatments: IMMPACT recommendations. Pain 2016, 157, 1851–1871. [Google Scholar] [CrossRef]
- Fillingim, R.B.; Loeser, J.D.; Baron, R.; Edwards, R.R. Assessment of Chronic Pain: Domains, Methods, and Mechanisms. J. Pain Off. J. Am. Pain Soc. 2016, 17, T10–T20. [Google Scholar] [CrossRef] [Green Version]
- Staud, R. New evidence for central sensitization in patients with fibromyalgia. Curr. Rheumatol. Rep. 2004, 6, 259. [Google Scholar] [CrossRef]
- King, C.D.; Wong, F.; Currie, T.; Mauderli, A.P.; Fillingim, R.B.; Riley, J.L., 3rd. Deficiency in endogenous modulation of prolonged heat pain in patients with Irritable Bowel Syndrome and Temporomandibular Disorder. Pain 2009, 143, 172–178. [Google Scholar] [CrossRef] [Green Version]
- King, C.D.; Sibille, K.T.; Goodin, B.R.; Cruz-Almeida, Y.; Glover, T.L.; Bartley, E.; Riley, J.L.; Herbert, M.S.; Sotolongo, A.; Schmidt, J.; et al. Experimental pain sensitivity differs as a function of clinical pain severity in symptomatic knee osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1243–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemley, K.J.; Hunter, S.K.; Bement, M.K. Conditioned pain modulation predicts exercise-induced hypoalgesia in healthy adults. Med. Sci. Sports Exerc. 2015, 47, 176–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaegter, H.B.; Handberg, G.; Graven-Nielsen, T. Similarities between exercise-induced hypoalgesia and conditioned pain modulation in humans. Pain 2014, 155, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Vaegter, H.B.; Handberg, G.; Graven-Nielsen, T. Isometric exercises reduce temporal summation of pressure pain in humans. Eur. J. Pain 2015, 19, 973–983. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.R.; Goodwin, P.C.; Yeowell, G. Exploring the pre-morbid contexts in which central sensitisation developed in individuals with non-specific chronic low back pain. A qualitative study. Braz. J. Phys. Ther. 2019, 23, 516–526. [Google Scholar] [CrossRef]
- Egloff, N.; Maecker, F.; Stauber, S.; Sabbioni, M.E.; Tunklova, L.; von Känel, R. Nondermatomal somatosensory deficits in chronic pain patients: Are they really hysterical? PAIN 2012, 153, 1847–1851. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.; Nijs, J.; Smart, K.; Holmes, P.; Yeowell, G.; Goodwin, P. Prevalence of Extreme Trait Sensory Profiles and Personality types in Non-specific Chronic Low Back Pain with Predominant Central Sensitisation: Secondary analysis of an international observational study. Pain Phys. 2019, 22, 182–190. [Google Scholar]


{kind=link}
| IASP 2021 Clinical Criteria for Nociplastic Pain [44] | 2014 Clinical Criteria for Predominant Central Sensitization Pain [45] |
|---|---|
| Mandatory criteria | |
| Patients have to report pain of at least 3 months duration. | Patients have to report pain of at least 3 months duration. |
| Patients have to report a regional rather than discrete pain distribution. | Patients have to present diffuse pain that spreads outside the segmental area of primary nociception. |
| Patients have to report pain that cannot entirely be explained by nociceptive mechanisms. | The pain should be considered disproportionate to what one would expect based on the available tissue damage or presumed source of nociception. |
| Patients have to report pain that cannot entirely be explained by neuropathic mechanisms. | Exclusion of neuropathic pain as the dominant pain mechanism. |
| Patients have to show clinical signs of pain hypersensitivity (i.e., evoked pain hypersensitivity phenomena such as static or dynamic mechanical allodynia, heat or cold allodynia, and/or painful after-sensations after any of the mentioned evoked pain hypersensitivity assessments) that are present at least in the region of pain. | - |
| Optional criteria | |
| Patients present with a history of pain hypersensitivity in the region of pain (i.e., sensitivity to touch, movement, pressure or heat/cold). | - |
| Patients present at least one of the defined comorbidities (increased sensitivity to sound, light and/or odours, sleep disturbance with frequent nocturnal awakenings, fatigue or cognitive problems). | A score of at least 40/100 on the Central Sensitization Inventory. |
| Comorbidities Included in the 2021 IASP Clinical Criteria for Nociplastic Pain | Central Sensitization Inventory Items |
|---|---|
| Increased sensitivity to light and/or sound and/or odours | I am sensitive to bright lights (Q7). Certain smells, such as perfumes, make me feel dizzy and nauseated (Q20). |
| Sleep disturbance with frequent nocturnal awakenings | I feel tired and unrefreshed when I wake up from sleeping (Q1). I do not sleep well (Q12). My legs feel uncomfortable and restless when I am trying to go to sleep at night (Q22). |
| Fatigue | I get tired very easily when I am physically active (Q8). I have low energy (Q17). |
| Cognitive problems such as difficulty to focus attention, memory disturbances, etc. | I have difficulty concentrating (Q13). I have difficulty remembering things (Q23). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nijs, J.; Lahousse, A.; Kapreli, E.; Bilika, P.; Saraçoğlu, İ.; Malfliet, A.; Coppieters, I.; De Baets, L.; Leysen, L.; Roose, E.; et al. Nociplastic Pain Criteria or Recognition of Central Sensitization? Pain Phenotyping in the Past, Present and Future. J. Clin. Med. 2021, 10, 3203. https://doi.org/10.3390/jcm10153203
Nijs J, Lahousse A, Kapreli E, Bilika P, Saraçoğlu İ, Malfliet A, Coppieters I, De Baets L, Leysen L, Roose E, et al. Nociplastic Pain Criteria or Recognition of Central Sensitization? Pain Phenotyping in the Past, Present and Future. Journal of Clinical Medicine. 2021; 10(15):3203. https://doi.org/10.3390/jcm10153203
Chicago/Turabian StyleNijs, Jo, Astrid Lahousse, Eleni Kapreli, Paraskevi Bilika, İsmail Saraçoğlu, Anneleen Malfliet, Iris Coppieters, Liesbet De Baets, Laurence Leysen, Eva Roose, and et al. 2021. "Nociplastic Pain Criteria or Recognition of Central Sensitization? Pain Phenotyping in the Past, Present and Future" Journal of Clinical Medicine 10, no. 15: 3203. https://doi.org/10.3390/jcm10153203