
Peri-Surgical Inflammatory Profile Associated with Mini-Invasive or Standard Open Lumbar Interbody Fusion Approaches

 ,
, 
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Surgery Description
2.4. Biochemical and Hematological Characterization
2.5. Statistical Analysis
3. Results
3.1. Patients
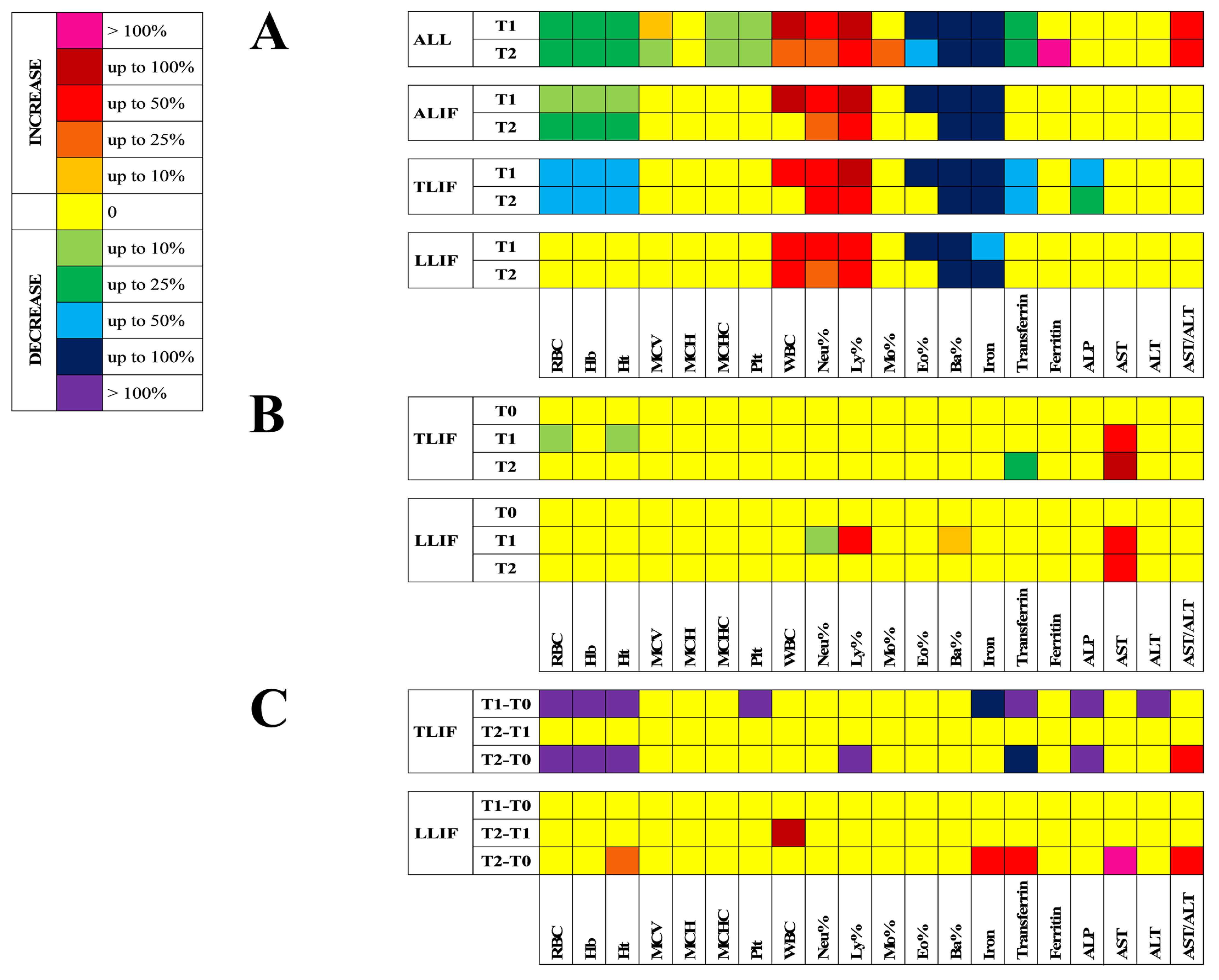
3.2. Hematological and Clinical Chemistry Profile
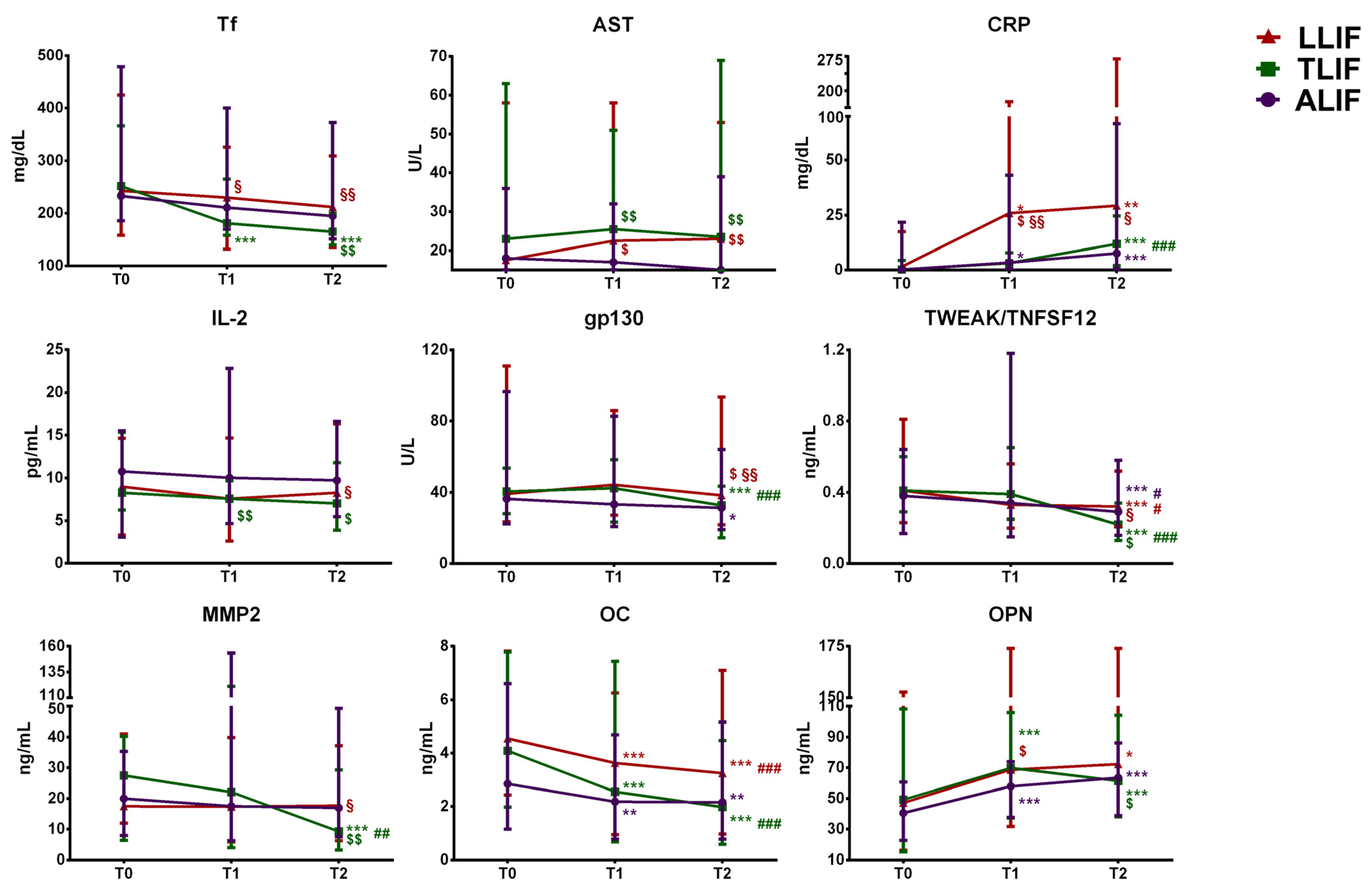
3.3. Inflammatory Mediators Profile
3.3.1. Non-Specific Markers of Systemic Inflammation
3.3.2. Members of the TNF/TNFR Superfamily
3.3.3. B- and T-Cell Cytokines
3.3.4. Cytokine Receptors and Co-Receptors
3.3.5. Class II Cytokines
3.3.6. Matrix Metalloproteinases and Tissue Remodeling Factors
3.3.7. Bone Markers
4. Discussion
4.1. Hematological Profile
4.2. Clinical Chemistry Profile
4.3. Inflammatory Mediators Profile
4.4. Bone Turnover Profile
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lombardi, G.; Grasso, D.; Berjano, P.; Banfi, G.; Lamartina, C. Is minimally invasive surgery also minimally pro-inflammatory? Muscular markers, inflammatory parameters and cytokines to quantify the operative invasiveness assessment in spine fusion. Eur. J. Inflamm. 2014, 12, 237–249. [Google Scholar] [CrossRef]
- Kaplan, J.R.; Lee, Z.; Eun, D.D.; Reese, A.C. Complications of Minimally Invasive Surgery and Their Management. Curr. Urol. Rep. 2016, 17, 47. [Google Scholar] [CrossRef] [PubMed]
- Kambin, P.; Zhou, L. Arthroscopic discectomy of the lumbar spine. Clin. Ortop. Relat. Res. 1997, 33, 49–57. [Google Scholar] [CrossRef]
- Foley, K.T.; Holly, L.T.; Schwender, J.D. Minimally invasive lumbar fusion. Spine 2003, 28, S26–S35. [Google Scholar] [CrossRef]
- Berjano, P.; Balsano, M.; Buric, J.; Petruzzi, M.; Lamartina, C. Direct lateral access lumbar and thoracolumbar fusion: Preliminary results. Eur. Spine J. 2012, 21 (Suppl. 1), S37–S42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berjano, P.; Damilano, M.; Lamartina, C. Sagittal alignment correction and reconstruction of lumbar post-traumatic kyphosis via MIS lateral approach. Eur. Spine J. 2012, 21, 2718–2720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berjano, P.; Lamartina, C. Far lateral approaches (XLIF) in adult scoliosis. Eur. Spine J. 2013, 22 (Suppl. 2), 242–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.T.; Lee, S.H.; Suk, K.S.; Bae, S.C. The quantitative analysis of tissue injury markers after mini-open lumbar fusion. Spine 2006, 31, 712–716. [Google Scholar] [CrossRef]
- Hofstetter, C.P.; Hofer, A.S.; Wang, M.Y. Economic impact of minimally invasive lumbar surgery. World J. Orthop. 2015, 6, 190–201. [Google Scholar] [CrossRef] [PubMed]
- Cummock, M.D.; Vanni, S.; Levi, A.D.; Yu, Y.; Wang, M.Y. An analysis of postoperative thigh symptoms after minimally invasive transpsoas lumbar interbody fusion. J. Neurosurg. Spine 2011, 15, 11–18. [Google Scholar] [CrossRef]
- Villavicencio, A.T.; Burneikiene, S.; Roeca, C.M.; Nelson, E.L.; Mason, A. Minimally invasive versus open transforaminal lumbar interbody fusion. Surg. Neurol. Int. 2010, 1, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardi, G.; Lanteri, P.; Colombini, A.; Banfi, G. Blood biochemical markers of bone turnover: Pre-analytical and technical aspects of sample collection and handling. Clin. Chem. Lab. Med. 2012, 50, 771–789. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, G.; Barbaro, M.; Locatelli, M.; Banfi, G. Novel bone metabolism-associated hormones: The importance of the pre-analytical phase to for understanding their physiological roles. Endocrine 2017, 56, 460–484. [Google Scholar] [CrossRef]
- Campagner, A.; Berjano, P.; Lamartina, C.; Langella, F.; Lombardi, G.; Cabitza, F. Assessment and prediction of spine surgery invasiveness with machine learning techniques. Comput. Biol. Med. 2020, 121, 103796. [Google Scholar] [CrossRef]
- Banfi, G.; Colombini, A.; Lombardi, G.; Lubkowska, A. Metabolic markers in sports medicine. Adv. Clin. Chem. 2012, 56, 1–54. [Google Scholar]
- Chikhani, M.; Evans, D.L.; Blatcher, A.W.; Jackson, A.P.; Guha, I.N.; Aithal, G.P.; Moppett, I.K. The effect of prone positioning with surgical bolsters on liver blood flow in healthy volunteers. Anaesthesia 2016, 71, 550–555. [Google Scholar] [CrossRef] [Green Version]
- Kawaguchi, Y.; Matsui, H.; Tsuji, H. Changes in serum creatine phosphokinase MM isoenzyme after lumbar spine surgery. Spine 1997, 22, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Brancaccio, P.; Lippi, G.; Maffulli, N. Biochemical markers of muscular damage. Clin. Chem. Lab. Med. 2010, 48, 757–767. [Google Scholar] [CrossRef]
- Pathak, A.; Agrawal, A. Evolution of C-Reactive Protein. Front. Immunol. 2019, 10, 943. [Google Scholar] [CrossRef] [Green Version]
- Spolski, R.; Li, P.; Leonard, W.J. Biology and regulation of IL-2: From molecular mechanisms to human therapy. Nat. Rev. Immunol. 2018, 18, 648–659. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, Y.; Wang, Q.; Li, C.; Deng, H.; Si, C.; Xiong, H. Interleukin-35 in immune-related diseases: Protection or destruction. Immunology 2019, 157, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wieland, E.; Shipkova, M. Lymphocyte surface molecules as immune activation biomarkers. Clin. Biochem. 2016, 49, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A.; Kim, S.H. IL-32, a novel cytokine with a possible role in disease. Ann. Rheum. Dis. 2006, 65 (Suppl. 3), iii61–iii64. [Google Scholar] [CrossRef] [PubMed]
- Uciechowski, P.; Dempke, W.C.M. Interleukin-6: A Masterplayer in the Cytokine Network. Oncology 2020, 98, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Patron, C.; Kassiri, Z.; Leung, D. Modulation of Systemic Metabolism by MMP-2: From MMP-2 Deficiency in Mice to MMP-2 Deficiency in Patients. Compr. Physiol. 2016, 6, 1935–1949. [Google Scholar] [CrossRef]
- Lombardi, G.; Perego, S.; Luzi, L.; Banfi, G. A four-season molecule: Osteocalcin. Updates in its physiological roles. Endocrine 2015, 48, 394–404. [Google Scholar] [CrossRef]
- Banfi, G.; Lombardi, G.; Colombini, A.; Lippi, G. Bone metabolism markers in sports medicine. Sports Med. 2010, 40, 697–714. [Google Scholar] [CrossRef]
- Lombardi, G.; Sanchis-Gomar, F.; Perego, S.; Sansoni, V.; Banfi, G. Implications of exercise-induced adipo-myokines in bone metabolism. Endocrine 2016, 54, 284–305. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Surgical Approach | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ALL | ALIF | TLIF | LLIF | |||||||||
| T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | |
| RBC (1012/L) | 4.70 (3.42–6.33) | 4.27 (2.91–5.35) *** | 3.96 (2.77–5.31) ***, ### | 4.59 (3.85–5.68) | 4.30 (3.30–5.01) * | 3.96 (2.82–4.77) * | 4.88 (4.15–6.33) | 3.90 (2.91–4.74) ***, $$ | 3.43 (2.77–4.73) *** | 4.51 (3.42–6.02) | 4.33 (3.24–5.35) §§§ | 4.22 (3.08–5.31) §§§ |
| Hb (g/L) | 13.6 (9.6–17.8) | 12.1 (7.9–16.6) *** | 11.5 (8.0–16.2) ***, ### | 13.5 (9.6–17.8) | 12.3 (9.1–15.2) * | 11.6 (8.3–14.1) *** | 14.9 (11.1–16.8) | 11.4 (7.9–14.2) *** | 10.3 (8.0–14.0) *** | 13.5 (10.3–17.2) | 12.3 (8.9–16.6) § | 11.9 (8.6–16.2) §§ |
| Ht (%) | 40.8 (30.3–49.8) | 36.5 (25.7–45.6) *** | 34.3 (24.5–46.3) ***, ### | 40.4 (32.1–49.8) | 36.5 (30.2–42.8) * | 34.4 (25.6–41.0) *** | 42.9 (35.0–48.0) | 33.3 (25.7–41.0) ***, $ | 30.3 (24.5–40.5) *** | 39.9 (30.3–45.1) | 39.1 (27.2–45.6) §§ | 37.3 (26.6–46.3) §§ |
| MCV (fL) | 88.6 (61.0–99.6) | 88.8 (60.5–100.3) *** | 88.4 (61.8–101.6) *** | 87.3 (67.9–98.0) | 87.70 (69.1–98.1) | 87.9 (68.2–97.4) | 89.3 (64.3–99.6) | 89.6 (64.6–100.3) | 89.0 (64.6–101.6) | 88.6 (61.0–96.0) | 88.8 (60.5–96.7) | 88.4 (61.8–97.6) |
| MCH (pg) | 29.6 (19.9–36.6) | 29.8 (19.8–35.6) | 29.7 (19.9–34.9) | 29.4 (20.3–33.1) | 29.6 (20.7–33.4) | 29.6 (20.4–32.9) | 30.4 (20.2–34.3) | 30.0 (19.8–33.5) | 29.8 (20.0–34.3) | 29.9 (19.9–36.6) | 30.1 (20.1–35.6) | 30.1 (19.9–34.9) |
| MCHC (g/L) | 33.8 (29.9–38.1) | 33.5 (29.9–36.9) *** | 33.4 (29.8–35.8) *** | 33.8 (29.9–36.6) | 33.7 (29.9–36.0) | 33.5 (29.8–35.1) | 33.8 (31.4–35.9) | 33.3 (30.7–35.4) | 32.9 (30.9–35.4) | 34.1 (32.5–38.1) | 33.7 (31.9–36.9) | 33.5 (32.2–35.8) |
| Plt (109/L) | 228 (104–462) | 215 (120–440) *** | 207 (113–458) ***, ## | 226 (139–462) | 223 (137–440) | 208 (138–458) | 220 (132–334) | 209 (121–285) | 194 (113–377) | 233 (104–381) | 215 (120–304)) | 212 (132–294) |
| WBC (109/L) | 6.81 (3.48–12.9) | 10.28 (6.26–17.91) *** | 8.63 (3.49–15.93) ***, ### | 7.07 (3.59–12.9) | 12.20 (6.73–17.91) *** | 7.78 (5.07–15.93) # | 7.17 (4.22–10.47) | 10.66 (6.27–15.39) *** | 9.06 (4.87–10.71) # | 6.63 (3.48–10.74) | 9.21 (6.26–15.45) *** | 8.90 (3.49–13.63) ** |
| Neu (%) | 57.3 (27.1–83.8) | 76.3 (52.8–90.4) *** | 68.6 (50.2–91.2) *** ### | 61.05 (43.4–83.8) | 79.2 (64.8–90.4) *** | 69.7 (50.2–81.1) *, ## | 53.9 (33.1–76.0) | 76.0 (60.0–90.3) *** | 70.0 (52.0–81.9) *** | 58.1 (27.1–69.2) | 73.9 (52.8–86.9) ***, $ | 64.4 (53.5–91.2) *** |
| Ly (%) | 33.1 (11.7–50.6)) | 16.1 (4.4–36.1) *** | 20.5 (5.5–36.1) ***, ### | 28.5 (11.7–46.0) | 12.9 (4.7–24.4) *** | 19.0 (11.4–35.3) **, ## | 35.4 (17.9–47.6) | 15.1 (4.4–31.4) *** | 19.6 (12.4–35.9) *** | 32.3 (22.7–50.6) | 18.1 (7.5–36.1) ***, $ | 24.1 (5.5–36.1) *** |
| Mo (%) | 7.6 (3.8–13.5) | 7.7 (3.0–12.6) | 8.5 (3.3–13.5) * | 7.6 (4.3–11.0) | 8.4 (3.0–12.4) | 8.2 (5.9–13.1) | 7.7 (4.9–13.5) | 8.0 (5.3–11.6) | 9.0 (5.6–13.5) | 7.6 (3.8–12.8) | 7.5 (3.3–12.6) | 8.4 (3.3–12.7) |
| Eo (%) | 1.9 (0.1–14.20) | 0.1 (0.0–3.8) *** | 1.3 (0.0–7.7) *, ### | 1.3 (0.1–7.6) | 0.1 (0.0–3.4) ** | 1.3 (0.0–4.3) # | 2.0 (0.3–14.2) | 0.1 (0.0–1.4) ** | 1.3 (0.0–7.7) | 1.9 (0.7–9.7) | 0.7 (0.0–3.8) **, § | 1.6 (0.0–5.8) |
| Ba (%) | 0.3 (0.0–1.6) | 0.1 (0.0–0.5) *** | 0.1 (0.0–0.4) *** | 0.3 (0.0–1.6) | 0.1 (0.0–0.4) ** | 0.1 (0.0–0.3) * | 0.3 (0.1–1.1) | 0.1 (0.0–0.3) *** | 0.1 (0.0–0.4) * | 0.4 (0.2–0.7) | 0.1 (0.0–0.5) ***, $, § | 0.1 (0.0–0.4) *** |
| Surgical Approach | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ALL | ALIF | TLIF | LLIF | |||||||||
| T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | |
| Iron (μg/dL)) | 99.0 (29.0–226.0) | 40.0 (13.0–113.0) *** | 23.0 (7.0–106.0) *** | 103.0 (29.0–176.0) | 40.0 (17.0–113.0) *** | 23.0 (11.0–87.0) *** | 108.0 (36.0–226.0) | 30.0 (13.0–60.0) *** | 16.0 (8.0–64.0) *** | 83.5 (29.0–174.0) | 45.0 (22.0–94.0) *** | 36.0 (7.0–106.0) ***, § |
| Transferrin (mg/dL) | 245 (158–479) | 210 (132–400) ** | 194 (135–375) *** | 233 (186–479) | 211 (170–400) | 195 (151–373) | 252 (186–367) | 181 (158–265) *** | 165 (140–200) ***, $$ | 243.5 (158–425) | 230.5 (132–326) § | 212 (135–309) §§§ |
| Ferritin (ng/mL) | 62.1 (2.0–666.0) | 127.0 (7.0–858.0) | 126.8 (9.0–1000) * | 60.80 (2.0–501.0) | 117.9 (7.0–718.0) | 121.0 (9.0–1000.0) | 67.0 (7.0–666.0) | 128.0 (23.0–858.0) | 174.0 (66.0–915.0) | 64.4 (5.0–465.8) | 114.0 (9.0–795.2) | 135.5 (11.0–711.4) |
| ALP (U/L) | 64.5 (29.0–105.0) | 53.5 (28.0–109.0) | 53.5 (25.0–119.0) | 48.0 (41.0–105) | 46.5 (30.0–109.0) | 49.0 (25.0–119.0) | 69.0 (40.0–104.0) | 48.0 (28.0–74.0) ** | 53.0 (35.0–70.0) ** | 61.0 (29.0–103.0) | 60.0 (30.0–105.0) | 61.0 (31.0–97.0) |
| AST (U/L) | 18.0 (9.0–63.0) | 19.5 (10.0–58.0) | 21.0 (9.0–69.0) | 18.0 (9.0–36.0) | 17.0 (10.0–32.0) | 13.5 (11.0–39.0) | 23.0 (10.0–63.0) | 25.5 (12.0–51.0) $$ | 23.5 (9.0–69.0) $$ | 17.5 (11.0–58.0) | 22.5 (12.0–58.0) $ | 23.0 (12.0–53.0) $$ |
| ALT (U/L) | 17.5 (5.0–116) | 16.0 (6.0–89.0) | 16.0 (6.0–87.0) | 16.0 (8.0–49.0) | 12.5 (6.0–41.0) | 12.0 (6.0–47.0) | 19.0 (5.0–83.0) | 16.5 (9.0–66.0) | 16.0 (6.0–43.0) | 19.0 (9.0–116.0) | 19.5 (9.0–89.0) | 18.0 (9.0–87.0) |
| AST/ALT | 0.9 (0.4–3.9) | 1.2 (0.6–2.7) * | 1.3 (0.5–3.2) * | 1.0 (0.6–1.8) | 1.1 (0.6–2.2) | 1.1 (0.5–2.2) | 0.9 (0.4–2.6) | 1.3 (0.7–2.7) | 1.3 (0.7–3.2) | 0.9 (0.4–3.9) | 1.2 (0.7–2.3) | 1.3 (0.5–2.3) |
| Surgical Approach | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ALL | ALIF | TLIF | LLIF | |||||||||
| T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | |
| Acute phase | ||||||||||||
| CRP (mg/dL) | 0.50 (0.02–21.71) | 5.21 (0.46–208.5) *** | 17.72 (0.45–271.4) ***, ### | 0.15 (0.02–21.71) | 3.31 (0.46–43.00) * | 7.50 (0.45–66.67) *** | 0.20 (0.03–4.29) | 3.09 (1.16–7.76) | 11.86 (2.0–24.64) ***, ### | 1.465 (0.03–17.45) | 25.84 (1.09–208.5) *, $, §§ | 29.30 (1.01–271.4) **, § |
| sCD163 (ng/mL) | 84.75 (26.65–299.49) | 80.82 (27.49–610.36) | 63.31 (18.99–458.94) ***, ## | 74.65 (32.05–255.90) | 67.13 (32.11–411-27) ** | 57.96 (23.80–187-48) | 97.96 (44.39–152-49) | 84.73 (18.99–86.33) *** | 58.86 (18.99–86.33) ***, ### | 78.11 (26.65–299.49) | 84.00 (26.65–610.36) | 79.59 (26.34–458.94) § |
| IL-8 (pg/mL) | 42.65 (16.75–76.84) | 42.65 (16.22–119.80) | 37.73 (8.70–67.51) | 46.61 (16.75–76-84) | 43.28 (22.64–69.15) | 39.77 (16.75–61.38) # | 36.88 (22.64–53.75) | 36.46 (16.75–56.75) | 33.14 (8.70–64.22) | 46.12 (22.64–73.05) | 42.65 (16.22–119.8) | 42.04 (16.22–67.51) |
| IL-11 (pg/mL) | 0.62 (0.05–3.22) | 0.62 (0.05–3.22) | 0.89 (0.07–6.16) **, # | 0.53 (0.05–2.38) | 0.62 (0.05–2.83) | 0.65 (0.08–2.32) | 0.76 (0.07–1.76) | 0.80 (0.05–2.85) * | 0.90 (0.07–3.44) | 0.57 (0.07–3.22) | 0.50 (0.05–3.22) | 1.05 (0.09–6.16) |
| IL-12p40 (pg/mL) | 53.08 (16.00–129.70) | 50.48 (16.00–190.70) | 51.02 (13.47–144.30) | 63.64 (30.53–91.10) | 57.44 (36.14–190.70) | 51.02 (31.02–91.10) | 49.94 (36.51–75.37) | 45.49 (25.80–91.02) | 48.68 (20.97–127.50) | 52.74 (27.40–96.00) | 46.24 (18.12–96.00) | 55.05 (19.94–144.30) |
| IL-12p70 (pg/mL) | 2.41 (0.10–9.82) | 2.09 (0.10–6.70) | 2.33 (0.10–6.31) | 3.18 (0.10–5.53) | 3.21 (1.21–6.70) | 2.73 (0.10–3.98) | 2.55 (0.71–4.21) | 2.10 (1.77–4.76) | 2.41 (0.90–3.69) | 2.41 (1.13–9.82) | 2.25 (0.81–4.76) | 2.41 (1.45–6.31) # |
| IL-27 (pg/mL) | 13.82 (0.10–42.46) | 10.44 (0.10–46.38) | 13.82 (0.10–65.63) | 5.53 (0.10–39.49) | 5.53 (0.10–46.38) | 13.82 (0.10–39.49) | 13.82 (0.10–39.06) | 14.24 (0.10–32.18) | 13.82 (0.10–45.83) | 14.24 (0.10–42.46) | 10.44 (0.10–45.83) | 17.90 (0.10–65.63) # |
| PTX-3 (ng/mL) | 0.62 (0.15–8.12) | 2.22 (0.19–11.73) *** | 1.15 (0.13–5.78) *, ### | 0.60 (0.34–2.94) | 2.05 (0.62–5.70) *** | 1.08 (0.58–4.13) *, ## | 0.50 (0.22–0.80) | 2.99 (0.66–6.05) *** | 1.09 (0.60–3.24) ***, ### | 0.74 (0.15–2.65) | 2.23 (0.19–11.73) ** | 1.50 (0.13–5.78) * |
| TNF superfamily | ||||||||||||
| APRIL/TNFSF13 (ng/mL) | 52.63 (12.98–137.73) | 57.43 (76.48–161.60) | 56.16 (8.95–109.40) | 50.10 (12.98–94.83) | 55.65 (7.65–99.83) * | 55.86 (30.05–92.12) | 57.28 (30.05–92.12) | 62.21 (44.27–128.39) * | 52.20 (32.11–109.40) # | 48.39 (21.54–109.76) | 51.45 (14.20–127.76) | 56.84 (30.86–108.90) |
| BAFF/TNFSF13B (ng/mL) | 7.86 (3.72–30.06) | 8.52 (3.90–23.18) * | 5.99 (3.27–16.74) ## | 6.48 (3.72–23.85) | 7.27 (4.16–21.73) | 6.85 (4.16–14.79) | 7.86 (5.85–11.90) | 8.57 (4.74–12.60) | 8.23 (3.90–13.19) | 8.05 (4.59–30.06) | 9.94 (3.90–23.18) | 7.99 (3.85–16.74) |
| LIGHT/TNFSF14 (pg/mL) | 1.73 (0–257.4) | 3.53 (1.5–146.1) | 15.12 (1.5–277.4) **, # | 1.73 (1.73–257.40) | 9.83 (1.73–61.47) | 11.44 (1.73–185.30) | 1.73 (1.73–127.20) | 20.86 (1.73–50.41) ** | 46.95 (1.73–277.40) | 3.58 (1.50–146.30) | 27.82 (1.73–146.10) | 56.02 (1.73–253.30) |
| sTNFR-1 (ng/mL) | 2.19 (0.91–7.53) | 3.16 (1.34–12.02) *** | 2.97 (1.26–9.48) ***, # | 1.95 (0.91–7.53) | 2.38 (1.34–5.21) | 2.43 (1.26–5.34) | 2.55 (1.62–5.30) | 3.64 (1.88–8.46) **, $ | 3.14 (1.61–7.73) * | 2.13 (1.13–5.23) | 3.36 (1.98–12.02) *, $ | 3.12 (1.62–9.48) |
| sTNFR-2 (ng/mL) | 3.99 (1.70–9.85) | 5.73 (2.03–30.63) *** | 5.70 (2.41–26.93) *** | 3.67 (2.10–9.13) | 5.39 (2.03–13.89) *** | 5.19 (3.18–10.80) | 4.08 (1.70–9.10) | 5.43 (2.06–19.06) ** | 5.69 (2.62–12-25) ** | 3.49 (1.82–9.85) | 6.55 (2.08–30.63) * | 6.79 (2.14–26.93) * |
| sCD30 (ng/mL) | 0.39 (0.16–1.28) | 0.42 (0.18–1.40) | 0.39 (0.16–1.49) | 0.36 (0.16–1.02) | 0.35 (0.18–0.98) | 0.37 (0.16–0.74) | 0.42 (0.27–0.87) | 0.45 (0.23–0.97) $ | 0.39 (0.22–0.62) | 0.40 (0.22–1.28) | 0.49 (0.26–1.40) | 0.46 (0.27–1.49) $, § |
| TWEAK/TNFSF12 (ng/mL) | 0.40 (0.17–0.81) | 0.37 (0.15–1.18) | 0.27 (0.13–0.58) ***, ### | 0.38 (0.17–0.64) | 0.34 (0.15–1.18) | 0.29 (0.16–0.58) ***, # | 0.41 (0.29–0.60) | 0.39 (0.25–0.65) | 0.22 (0.13–0.34) ***, ###, $ | 0.41 (0.23–0.81) | 0.33 (0.20–0.56) * | 0.32 (0.21–0.52) ***, #, § |
| B- and T-cell cytokines | ||||||||||||
| IL-2 (pg/mL) | 8.91 (2.91–15.49) | 8.51 (2.61–22.81) | 8.69 (1.13–16.60) | 10.76 (3.05–15.49) | 10.01 (4.65–22.81) | 9.71 (5.44–16.60) | 8.25 (6.22–15.33) | 7.55 (4.65–9.67) $$ | 6.99 (3.86–11.79) § | 8.96 (3.31–14.62) | 7.55 (2.61–14.67) *, $ | 8.25 (5.43–16.31) |
| IL-32 (pg/mL) | 19.93 (1.05–72.57) | 19.23 (0.57–88.09) | 13.07 (1.050–77.75) # | 19.93 (1.05–64.78) | 17.23 (0.57–75.16) | 14.51 (1.05–42.07) | 9.78 (3.00–42.72) § | 14.54 (2.39–45.18) | 3.90 (2.39–45.18) | 31.62 (3.00–72.57) | 38.58 (3.00–88.09) | 22.98 (3.00–77.75) $, §§ |
| IL-34 (pg/mL) | 109.10 (20.00–669.90) | 151.60 (39.61–714.80) | 106.40 (20.00–613.70) | 77.97 (20.00–423.10) | 86.42 (20.00–273.40) | 120.60 (20.00–282.60) | 51.90 (51.90–214.20) | 120.60 (39.61–374.50) | 51.90 (39.61–342.00) | 151.40 (20.00–669.90) | 179.00 (39.61–714.80) $ | 123.20 (20.00–613.70) |
| IL-35 (pg/mL) | 287.1 (127.7–612.0) | 298.90 (145.8–661.2) | 302.30 (145.8–744.6) | 302.6 (141.5–45.1) | 304.6 (191.5–661.2) * | 302.6 (175.1–390.9) | 275.8 (145.8–375.9) | 283.4 (181.6–348.6) | 263.7 (181.6–523.5) | 319.3 (198.3–612.0) | 287.9 (153.8–425.1) * | 314.4 (198.3–744.6) |
| TSLP (pg/mL) | 35.45 (16.24–94.25) | 34.52 (16.20–180.60) | 37.76 (19.29–129.20) | 38.04 (16.24–60.56) | 36.80 (23.19–102.80) | 35.45 (23.19–55.41) | 34.10 (16.62–64.78) | 33.92 (20.25–66.62) * | 38.04 (23.86–68.44) * | 36.28 (23.92–94.25) | 33.15 (16.20–180.60) | 39.79 (19.29–129.20) |
| Cytokine receptors | ||||||||||||
| gp130 (ng/mL) | 39.20 (22.38–110.91) | 39.09 (20.77–85.96) | 33.87 (14.53–93.61) *, ### | 36.32 (22.38–96.58) | 33.25 (20.77–82.75) | 31.27 (19.16–64.04) * | 40.43 (27.99–53.59) | 42.35 (23.36–58.34) | 32.65 (14.53–43.47) ***, ### | 39.19 (23.56–110.91) | 44.26 (27.08–85.96) $ | 38.30 (21.82–93.61) $, §§ |
| sIL-6Rβ (ng/mL) | 6.90 (1.38–17.04) | 6.87 (1.49–32.87) | 5.70 (1.49–32.61) ### | 6.00 (1.38–12.69) | 6.13 (1.49–13.49) | 5.79 (1.49–11.39) * | 7.16 (4.26–11.50) | 6.92 (3.72–12.07) | 4.66 (2.03–8.96) ***, ### | 7.09 (3.58–17.04) | 7.28 (4.15–32.87) | 6.19 (3.57–32.61) #, § |
| Class II Cytokines | ||||||||||||
| IL-10 (pg/mL) | 20.91 (9.82–41.22) | 27.07 (15.65–50.28) *** | 23.11 (14.05–40.45) ***, # | 21.53 (10.45–27.60) | 27.11 (18.45–37.36) *** | 26.74 (17.63–34.19) *** | 20.05 (11.66–32.12) | 26.04 (17.21–50.28) *** | 24.14 (16.75–30.79) *** | 21.45 (9.82–41.22) | 27.39 (15.65–39.69) ** | 26.69 (14.05–40.45) ** |
| IL-19 (pg/mL) | 64.37 (41.37–86.96) | 64.85 (43.86–110.10) | 61.12 (38.71–108.50) | 61.01 (41.37–74.26) | 59.96 (49.46–110.10) | 57.45 (40.07–69.61) | 64.06 (49.46–86.96) | 69.78 (55.35–102.20) § | 64.06 (41.15–86.03) ## | 66.23 (47.17–82.08) | 58.65 (43.86–76.93) * | 61.12 (38.71–108.50) $ |
| IL-20 (pg/mL) | 56.86 (24.68–97.81) | 48.78 (23.72–85.47) ** | 48.75 (26.67–91.63) * | 60.92 (34.35–97.81) | 52.80 (38.84–85.47) | 48.75 (38.84–87.58) | 56.04 (24.68–74.35) | 47.53 (28.66–70.68) | 48.14 (26.67–81.73) | 60.31 (34.37–81.36) | 50.59 (23.72–77.26) * | 49.69 (34.37–91.63) |
| IL-22 (pg/mL) | 37.53 (8.73–87.88) | 37.87 (10.18–90.53) | 37.53 (8.73–123.00) | 37.53 (8.73–87.88) | 40.81 (23.77–90.53) * | 38.21 (25.18–99.84) | 37.53 (20.90–55.76) | 37.19 (26.59–50.64) | 32.12 (8.73–60.09) | 39.00 (14.96–80.02) | 35.94 (10.18–72.16) | 39.71 (17.38–123.00) |
| IL-26 (pg/mL) | 106.6 (36.9–323.9) | 136.1 (74.3–308.9) *** | 145.2 (67.1–254.0) *** | 98.8 (53.4–323.9) | 132.1 (98.7–308.9) *** | 134.3 (98.76–254.0) *** | 122.5 (57.9–243.1) | 148.8 (101.0–218.4) * | 146.5 (82.7–178.7) ** | 111.1 (36.9–173.2) | 133.4 (74.3–157.4) * | 140.5 (67.1–178.7) ***, ## |
| IL-28A/IFNλ2 (pg/mL) | 11.53 (1.44–98.33) | 13.93 (1.80–122.10) | 12.80 (1.80–80.05) | 33.21 (1.44–84.99) | 30.75 (1.80–89.94) | 52.08 (1.80–73.46) | 29.11 (1.80–98.33) | 18.71 (1.80–85.21) | 1.92 (1.80–80.05) $$ | 1.80 (1.80–60.72) | 1.80 (1.80–122.10) | 1.80 (1.80–68.12) $$ |
| IL-29/IFNλ1 (pg/mL) | 38.95 (5.20–72.92) | 38.95 (10.05–78.05) | 35.51 (5.20–92.96) | 44.89 (5.20–72.92) | 45.44 (10.05–78.05) | 37.89 (5.20–92.96) | 38.95 (10.05–53.24) | 38.95 (10.05–53.24) | 33.03 (10.05–56.88) | 35.33 (12.84–58.46) | 34.22 (12.84–60.68) $ | 35.33 (12.84–62.88) |
| IFNα2 (pg/mL) | 49.55 (32.01–95.10) | 48.03 (27.81–117.50) | 46.56 (25.12–137.00) | 55.65 (32.01–79.95) | 50.33 (38.58–117.50) | 50.33 (38.00–68.60) | 46.56 (30.24–54.14) | 46.56 (30.24–54.14) $ | 40.37 (25.12–77.03) | 51.13 (34.13–95.10) | 45.02 (27.81–76.17) *, $ | 48.06 (27.81–137.00) |
| IFNβ (pg/mL) | 16.92 (8.33–35.75) | 17.23 (2.39–41.13) | 14.72 (3.51–34.41) | 16.00 (10.90–35.75) | 17.16 (8.40–41.13) | 13.44 (3.51–27.56) | 16.92 (11.28–25.93) | 16.92 (9.88–25.03) | 14.09 (8.48–25.93) | 21.20 (8.33–32.41) | 21.37 (2.39–29.08) | 19.81 (8.82–34.41) |
| IFNγ (pg/mL) | 54.74 (17.95–87.71) | 49.91 (22.38–152.30) | 46.95 (13.35–113.7) | 62.22 (21.19–84.15) | 60.35 (29.97–152.3) | 57.37 (32.07–88.83) | 49.91 (17.95–72.97) | 48.51 (22.38–62.22) | 43.02 (13.35–96.49) | 62.22 (38.99–87.71) | 43.78 (22.44–94.78) * | 46.95 (29.19–113.70) |
| Matrix metalloproteinases and tissue remodeling factors | ||||||||||||
| MMP-1 (ng/mL) | 0.76 (0.26–3.00) | 0.67 (0.05–3.46) | 0.81 (0.24–2.71) | 0.80 (0.29–2.47) | 0.97 (0.05–2.56) | 0.80 (0.24–2.22) | 0.77 (0.44–2.22) | 0.61 (0.24–2.90) | 0.82 (2.90–1.84) | 0.73 (0.26–3.00) | 0.55 (0.18–3.46) | 0.62 (0.31–2.71) |
| MMP-2 (ng/mL) | 20.69 (6.34–41.00) | 17.76 (3.96–153.49) | 14.37 (3.19–49.31) **, # | 19.94 (7.88–35.26) | 17.46 (6.22–153.49) | 16.95 (7.51–49.31) | 27.45 (6.34–40.25) | 22.06 (3.96–121.13) | 9.23 (3.19–29.30) ***, #, $$ | 17.43 (11.99–41.00) | 17.32 (5.84–39.84) | 17.66 (6.28–37.10) § |
| MMP-3 (ng/mL) | 6.66 (1.83–27.98) | 7.37 (2.04–188.25) | 11.69 (3.33–450.14) | 7.27 (2.52–16.93) | 7.50 (3.16–49.20) *** | 15.88 (3.89–38.10) | 7.49 (1.83–16.67) | 6.58 (3.26–31.28) * | 11.97 (4.59–46.64) # | 5.13 (2.07–27.97) | 7.08 (2.04–188.25) | 6.13 (3.33–450.14) |
| Chit3like1/YKL-40 (ng/mL) | 6.24 (1.76–24.50) | 13.96 (2.95–96.45) *** | 9.05 (2.48–42.36) ***, ### | 5.39 (1.76–24.50) | 12.97 (4.31–30.34) *** | 8.57 (2.48–21.47) ***, ### | 6.42 (3.03–17.44) | 14.94 (2.95–28.47) *** | 8.52 (4.43–25.14) ***, ### | 8.04 (2.76–23.10) | 15.45 (4.38–96.45) *** | 10.75 (4.00–42.36) ***, ### |
| Bone markers | ||||||||||||
| OC (ng/mL) | 3.99 (1.15–7.82) | 2.57 (0.67–7.45) *** | 2.40 (0.58–7.10) *** | 2.85 (1.15–6.60) | 2.18 (0.78–4.69) ** | 2.16 (0.78–5.16) ** | 4.09 (1.98–7.78) | 2.55 (0.67–7.45) * | 1.98 (0.58–4.47) ***, # | 4.55 (2.43–7.82) | 3.63 (0.95–6.26) *** | 3.25 (0.97–7.10) ***, $, §§ |
| OPN (ng/mL) | 45.10 (15.11–152.74) | 64.70 (31.83–105.83) *** | 64.09 (37.98–174.03) *** | 40.50 (22.60–60.65) | 57.86 (37.55–73.79) *** | 63.44 (38.86–86.10) *** | 49.17 (15.11–108.03) | 69.79 (37.27–105.83) ***, $ | 61.42 (37.97–104.02) *** | 47.07 (16.18–152.74) | 68.63 (31.83–174.03) $ | 72.27 (38.34–174.03) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombardi, G.; Berjano, P.; Cecchinato, R.; Langella, F.; Perego, S.; Sansoni, V.; Tartara, F.; Regazzoni, P.; Lamartina, C. Peri-Surgical Inflammatory Profile Associated with Mini-Invasive or Standard Open Lumbar Interbody Fusion Approaches. J. Clin. Med. 2021, 10, 3128. https://doi.org/10.3390/jcm10143128
Lombardi G, Berjano P, Cecchinato R, Langella F, Perego S, Sansoni V, Tartara F, Regazzoni P, Lamartina C. Peri-Surgical Inflammatory Profile Associated with Mini-Invasive or Standard Open Lumbar Interbody Fusion Approaches. Journal of Clinical Medicine. 2021; 10(14):3128. https://doi.org/10.3390/jcm10143128
Chicago/Turabian StyleLombardi, Giovanni, Pedro Berjano, Riccardo Cecchinato, Francesco Langella, Silvia Perego, Veronica Sansoni, Fulvio Tartara, Pietro Regazzoni, and Claudio Lamartina. 2021. "Peri-Surgical Inflammatory Profile Associated with Mini-Invasive or Standard Open Lumbar Interbody Fusion Approaches" Journal of Clinical Medicine 10, no. 14: 3128. https://doi.org/10.3390/jcm10143128