
Health-Related Quality of Life, Depressive Symptoms, Anxiety, and Somatization Symptoms in Male and Female Patients with Chronic Tinnitus


Abstract
:1. Introduction
- Both female and male patients with chronic tinnitus report impairments in mental- and physical HRQoL.
- Compared to male patients with chronic tinnitus, female patients report higher levels of TRD, anxiety, depressive symptoms, somatization symptoms, and lower HRQoL.
- Within each gender, HRQoL is negatively influenced by TRD, anxiety, depressive symptoms, and somatization symptoms.
- Within each gender, the impact of TRD on HRQoL is completely mediated by psychological constructs (anxiety, depressive symptoms and somatization symptoms).
- [Exploratory] The observed indirect effects differ between female and male patients.
2. Method
Procedure
3. Materials
3.1. Tinnitus Questionnaire—German Version (TQ)
3.2. Hospital Anxiety and Depression Scale–German Version (HADS)
3.3. Somatic Symptom Scale-8–German Version (SSS-8)
3.4. Short-Form Health Survey—German Version (SF-12)
4. Participants
5. Statistical Analyses
6. Results
6.1. Serial Mediation Analyses
6.1.1. Mental HRQoL in Female Patients with Chronic Tinnitus
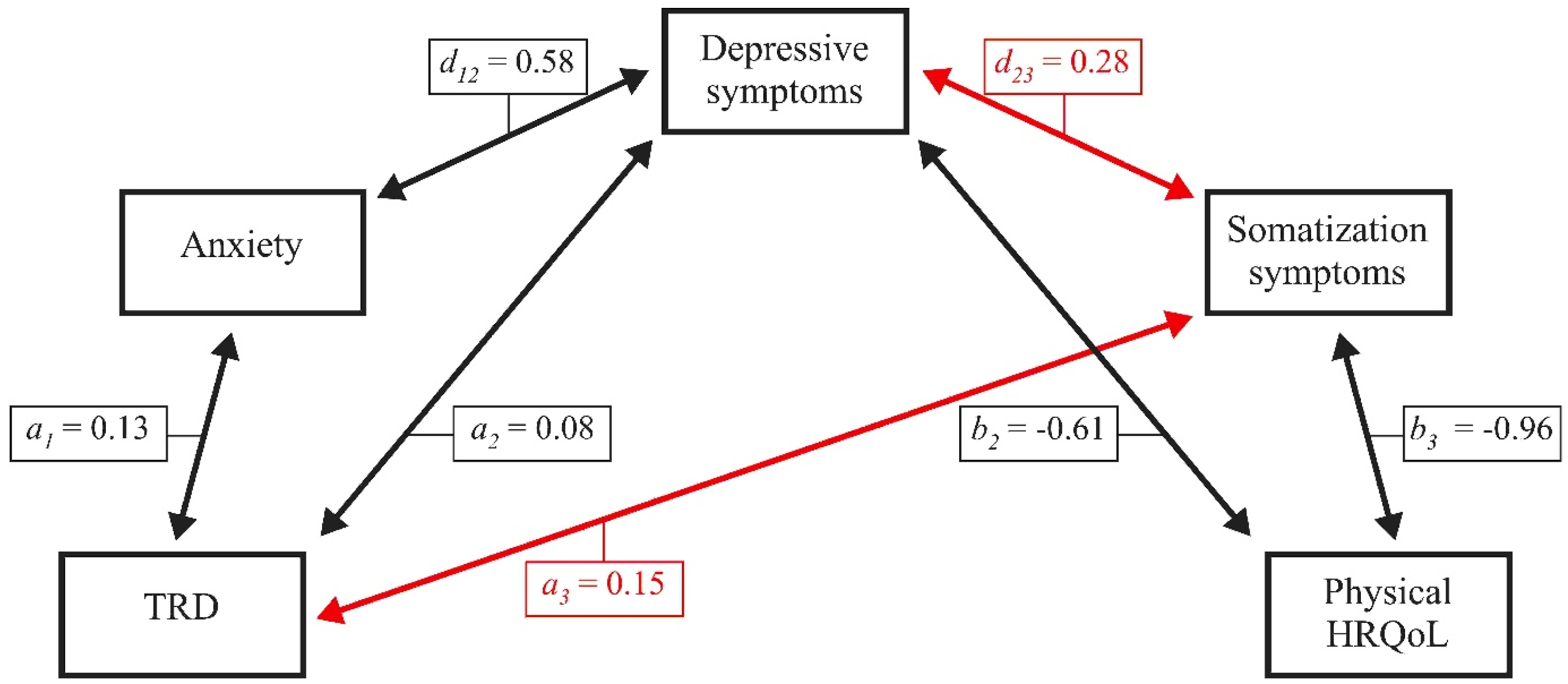
6.1.2. Physical HRQoL in Female Patients with Chronic Tinnitus
6.1.3. Mental HRQoL in Male Patients with Chronic Tinnitus
6.1.4. Physical HRQoL in Male Patients with Chronic Tinnitus
7. Discussion
8. Limitations
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear. Res. 2016, 337, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Boecking, B.; Brueggemann, P.; Mazurek, B. Tinnitus: Psychosomatische Aspekte. HNO 2019, 67, 137–152. [Google Scholar] [CrossRef]
- Langguth, B.; Kreuzer, P.M.; Kleinjung, T.; De Ridder, D. Tinnitus: Causes and clinical management. Lancet Neurol. 2013, 12, 920–930. [Google Scholar] [CrossRef]
- Salazar, J.; Meisel, K.; Smith, E.R.; Quiggle, A.; McCoy, D.B.; Amans, M.R. Depression in Patients with Tinnitus: A Systematic Review. Otolaryngol. Neck Surg. 2019, 161, 28–35. [Google Scholar] [CrossRef]
- Zöger, S.; Svedlund, J.; Holgers, K.-M. Relationship between Tinnitus Severity and Psychiatric Disorders. Psychosomatic 2006, 47, 282–288. [Google Scholar] [CrossRef] [PubMed]
- McCormack, A.; Edmondson-Jones, M.; Fortnum, H.; Dawes, P.D.; Middleton, H.; Munro, K.J.; Moore, D.R. Investigating the association between tinnitus severity and symptoms of depression and anxiety, while controlling for neuroticism, in a large middle-aged UK population. Int. J. Audiol. 2015, 54, 599–604. [Google Scholar] [CrossRef]
- Pattyn, T.; Eede, F.V.D.; Vanneste, S.; Cassiers, L.; Veltman, D.; Van De Heyning, P.; Sabbe, B. Tinnitus and anxiety disorders: A review. Hear. Res. 2016, 333, 255–265. [Google Scholar] [CrossRef]
- Zöger, S.; Svedlund, J.; Holgers, K.-M. Psychiatric Disorders in Tinnitus Patients without Severe Hearing Impairment: 24 Month Follow-up of Patients at an Audiological Clinic. Audiology 2001, 40, 133–140. [Google Scholar] [CrossRef]
- Hiller, W.; Janca, A.; Burke, K.C. Association between tinnitus and somatoform disorders. J. Psychosom. Res. 1997, 43, 613–624. [Google Scholar] [CrossRef]
- Sahin, C.; Aras, H.I.; Yılmaz, M.S. Somatoform disorders in patients with chronic subjective tinnitus. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3603–3607. [Google Scholar] [CrossRef]
- Wallhäusser-Franke, E.; D’Amelio, R.; Glauner, A.; Delb, W.; Servais, J.J.; Hörmann, K.; Repik, I. Transition from Acute to Chronic Tinnitus: Predictors for the Development of Chronic Distressing Tinnitus. Front. Neurol. 2017, 8, 605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biehl, R.; Boecking, B.; Brueggemann, P.; Grosse, R.; Mazurek, B. Personality Traits, Perceived Stress, and Tinnitus-Related Distress in Patients with Chronic Tinnitus: Support for a Vulnerability-Stress Model. Front. Psychol. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Siboni, F.S.; Alimoradi, Z.; Atashi, V.; Alipour, M.; Khatooni, M. Quality of life in different chronic diseases and its related factors. Int. J. Prev. Med. 2019, 10, 65. [Google Scholar] [CrossRef]
- Ge, L.; Ong, R.; Yap, C.-W.; Heng, B.H. Effects of chronic diseases on health-related quality of life and self-rated health among three adult age groups. Nurs. Health Sci. 2019, 21, 214–222. [Google Scholar] [CrossRef]
- Daly, E.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Gaynes, B.N.; Warden, D.; Morris, D.W.; Luther, J.F.; Farabaugh, A.; Cook, I.; et al. Health-related quality of life in depression: A STAR*D report. Ann. Clin. Psychiatry Off. J. Am. Acad. Clin. Psychiatr. 2010, 22, 43–55. [Google Scholar]
- Salaffi, F.; Sarzi-Puttini, P.; Girolimetti, R.; Atzeni, F.; Gasparini, S.; Grassi, W. Health-related quality of life in fibromyalgia patients: A comparison with rheumatoid arthritis patients and the general population using the SF-36 health survey. Clin. Exp. Rheumatol. 2010, 27 (Suppl. 56), S67–S74. [Google Scholar]
- Comer, J.S.; Blanco, C.; Hasin, D.S.; Liu, S.M.; Grant, B.F.; Turner, J.B.; Olfson, M. Health-related quality of life across the anxiety disorders: Results from the national epidemiologic survey on alcohol and related conditions (NESARC). J. Clin. Psychiatry 2011, 72, 43–50. [Google Scholar] [CrossRef]
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? Pharmacoeconomics 2016, 34, 645–649. [Google Scholar] [CrossRef]
- Rapley, M. Quality of Life Research: A Critical Introduction; Sage: London, UK, 2003. [Google Scholar]
- Drexler, D.; López-Paullier, M.; Rodio, S.; González, M.; Geisinger, D.; Pedemonte, M. Impact of reduction of tinnitus intensity on patients’ quality of life. Int. J. Audiol. 2015, 55, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Prestes, R.; Gil, D. Impact of tinnitus on quality of life, loudness and pitch match, and high-frequency audiometry. Int. Tinnitus J. 2009, 15, 134–138. [Google Scholar]
- Park, H.-M.; Jung, J.; Kim, J.-K.; Lee, Y.-J. Tinnitus and Its Association with Mental Health and Health-Related Quality of Life in an Older Population: A Nationwide Cross-Sectional Study. J. Appl. Gerontol. 2020. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Cisler, J.M.; Tolin, D.F. Quality of life in the anxiety disorders: A meta-analytic review. Clin. Psychol. Rev. 2007, 27, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Papakostas, G.I.; Petersen, T.; Mahal, Y.; Mischoulon, D.; Nierenberg, A.A.; Fava, M. Quality of life assessments in major depressive disorder: A review of the literature. Gen. Hosp. Psychiatry 2004, 26, 13–17. [Google Scholar] [CrossRef]
- Saarni, S.I.; Suvisaari, J.; Sintonen, H.; Pirkola, S.; Koskinen, S.; Aromaa, A.; Lönnqvist, J. Impact of psychiatric disorders on health-related quality of life: General population survey. Br. J. Psychiatry 2007, 190, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Nickel, R.; Egle, U.T.; Eysel, P.; Rompe, J.D.; Zöllner, J.; Hoffmann, S.O. Health-Related Quality of Life and Somatization in Patients with Long-Term Low Back Pain: A Prospective Study with 109 Patients. Spine 2001, 26, 2271–2277. [Google Scholar] [CrossRef] [PubMed]
- Wolf, L.D.; Hentz, J.G.; Ziemba, K.S.; Kirlin, K.A.; Noe, K.H.; Hoerth, M.T.; Crepeau, A.Z.; Sirven, J.I.; Drazkowski, J.F.; Locke, D.E. Quality of Life in Psychogenic Nonepileptic Seizures and Epilepsy: The Role of Somatization and Alexithymia. Epilepsy Behav. 2015, 43, 81–88. [Google Scholar] [CrossRef]
- Dirkzwager, A.J.; Verhaak, P.F. Patients with Persistent Medically Unexplained Symptoms in General Practice: Characteristics and Quality of Care. BMC Family Practice 2007, 8, 1–10. [Google Scholar] [CrossRef]
- Zeman, F.; Koller, M.; Langguth, B.; Landgrebe, M.; Tinnitus Research Initiative Database Study Group. Which tinnitus-related aspects are relevant for quality of life and depression: Results from a large international multicentre sample. Health Qual. Life Outcomes 2014, 12, 7. [Google Scholar] [CrossRef] [Green Version]
- Weidt, S.; Delsignore, A.; Meyer, M.; Rufer, M.; Peter, N.; Drabe, N.; Kleinjung, T. Which tinnitus-related characteristics affect current health-related quality of life and depression? A cross-sectional cohort study. Psychiatry Res. 2016, 237, 114–121. [Google Scholar] [CrossRef]
- Belli, S.; Belli, H.; Bahcebasi, T.; Ozcetin, A.; Alpay, E.; Ertem, U. Assessment of Psychopathological Aspects and Psychiatric Comorbidities in Patients Affected by Tinnitus. Eur. Arch. Otorhinolaryngol. 2008, 265, 279–285. [Google Scholar] [CrossRef]
- Gül, A.I.; Özkırış, M.; Aydin, R.; Şimşek, G.; Saydam, L. Coexistence of anxiety sensitivity and psychiatric comorbidities in patients with chronic tinnitus. Neuropsychiatr. Dis. Treat. 2015, 11, 413. [Google Scholar] [CrossRef] [Green Version]
- Ziai, K.; Moshtaghi, O.; Mahboubi, H.; Djalilian, H.R. Tinnitus Patients Suffering from Anxiety and Depression: A Review. Int. Tinnitus J. 2017, 21, 68–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oertelt-Prigione, S.; Regitz-Zagrosek, V. Sex and Gender Aspects in Clinical Medicine; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Regitz-Zagrosek, V. Sex and gender differences in health: Science & Society Series on Sex and Science. EMBO Rep. 2012, 13, 596–603. [Google Scholar]
- Kroenke, K.; Spitzer, R.L. Gender Differences in the Reporting of Physical and Somatoform Symptoms. Psychosom. Med. 1998, 60, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender Differences in Depression in Representative National Samples: Meta-Analyses of Diagnoses and Symptoms. Psychol. Bull. 2017, 143, 783. [Google Scholar] [CrossRef] [PubMed]
- Bonsaksen, T. Exploring gender differences in quality of life. Ment. Health Rev. J. 2012, 17, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Gamma, A.; Angst, J. Concurrent Psychiatric Comorbidity and Multimorbidity in a Community Study: Gender Differences and Quality of Life. Eur. Arch. Psychiatry Clin. Neurosci. 2001, 251, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Colillas-Malet, E.; Prat, G.; Espelt, A.; Juvinyà, D. Gender differences in health-related quality of life in people with severe mental illness. PLoS ONE 2020, 15, e0229236. [Google Scholar] [CrossRef] [PubMed]
- Garay, A.; Tapia, J.; Anguita, M.; Formiga, F.; Almenar, L.; Crespo-Leiro, M.G.; Manzano, L.; Muñiz, J.; Chaves, J.; De Frutos, T. Gender Differences in Health-Related Quality of Life in Patients with Systolic Heart Failure: Results of the VIDA Multicenter Study. J. Clin. Med. 2020, 9, 2825. [Google Scholar] [CrossRef]
- Crispino, P.; Gino, M.; Barbagelata, E.; Ciarambino, T.; Politi, C.; Ambrosino, I.; Ragusa, R.; Marranzano, M.; Biondi, A.; Vacante, M. Gender Differences and Quality of Life in Parkinson’s Disease. Int. J. Environ. Res. Public Health 2021, 18, 198. [Google Scholar] [CrossRef]
- Basso, L.; Boecking, B.; Brueggemann, P.; Pedersen, N.L.; Canlon, B.; Cederroth, C.R.; Mazurek, B. Gender-Specific Risk Factors and Comorbidities of Bothersome Tinnitus. Front. Neurosci. 2020, 14. [Google Scholar] [CrossRef] [PubMed]
- Niemann, U.; Boecking, B.; Brueggemann, P.; Mazurek, B.; Spiliopoulou, M. Gender-Specific Differences in Patients With Chronic Tinnitus—Baseline Characteristics and Treatment Effects. Front. Neurosci. 2020, 14, 487. [Google Scholar] [CrossRef]
- Seydel, C.; Haupt, H.; Szczepek, A.J.; Klapp, B.F.; Mazurek, B. Long-Term Improvement in Tinnitus after Modified Tinnitus Retraining Therapy Enhanced by a Variety of Psychological Approaches. Audiol. Neurootol. 2010, 15, 69–80. [Google Scholar] [CrossRef]
- Fioretti, A.; Natalini, E.; Riedl, D.; Moschen, R.; Eibenstein, A. Gender Comparison of Psychological Comorbidities in Tinnitus Patients–Results of a Cross-Sectional Study. Front. Neurosci. 2020, 14, 704. [Google Scholar] [CrossRef] [PubMed]
- Han, T.S.; Jeong, J.-E.; Park, S.-N.; Kim, J.J. Gender Differences Affecting Psychiatric Distress and Tinnitus Severity. Clin. Psychopharmacol. Neurosci. 2019, 17, 113. [Google Scholar] [CrossRef] [Green Version]
- Dineen, R.; Doyle, J.; Bench, J. Audiological and Psychological Characteristics of a Group of Tinnitus Sufferers, Prior to Tinnitus Management Training. Br. J. Audiol. 1997, 31, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Goebel, G.; Hiller, W. Tinnitus-Fragebogen:(TF); ein Instrument zur Erfassung von Belastung und Schweregrad bei Tinnitus; Handanweisung; Hogrefe, Verlag für Psychologie: Göttingen, Germany, 1998. [Google Scholar]
- Milerová, J.; Anders, M.; Dvořák, T.; Sand, P.G.; Königer, S.; Langguth, B. The influence of psychological factors on tinnitus severity. Gen. Hosp. Psychiatry 2013, 35, 412–416. [Google Scholar] [CrossRef]
- Seydel, C.; Haupt, H.; Olze, H.; Szczepek, A.J.; Mazurek, B. Gender and chronic tinnitus: Differences in tinnitus-related distress depend on age and duration of tinnitus. Ear Hear. 2013, 34, 661–672. [Google Scholar] [CrossRef]
- Hermann, C.; Buss, U.; Snaith, R.P. HADS-D: Hospital Anxiety and Depression Scale (German Version); Hans Huber: Bern, Germany, 1995; Volume 1, p. 995. [Google Scholar]
- Hinz, A.; Brähler, E. Normative values for the Hospital Anxiety and Depression Scale (HADS) in the general German population. J. Psychosom. Res. 2011, 71, 74–78. [Google Scholar] [CrossRef]
- Langvik, E.; Hjemdal, O.; Nordahl, H.M. Personality traits, gender differences and symptoms of anhedonia: What does the Hospital Anxiety and Depression Scale (HADS) measure in nonclinical settings? Scand. J. Psychol. 2016, 57, 144–151. [Google Scholar] [CrossRef] [Green Version]
- Gierk, B.; Kohlmann, S.; Kroenke, K.; Spangenberg, L.; Zenger, M.; Brähler, E.; Löwe, B. The Somatic Symptom Scale–8 (SSS-8): A Brief Measure of Somatic Symptom Burden. JAMA Intern. Med. 2014, 174, 399–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipowski, Z.J. Somatization: The concept and its clinical application. Am. J. Psychiatry 1988, 145, 1358–1368. [Google Scholar] [CrossRef]
- Rief, W.; Barsky, A.J. Psychobiological perspectives on somatoform disorders. Psychoneuroendocrinology 2005, 30, 996–1002. [Google Scholar] [CrossRef]
- Marinaci, T.; Carpinelli, L.; Venuleo, C.; Savarese, G.; Cavallo, P. Emotional distress, psychosomatic symptoms and their relationship with institutional responses: A survey of Italian frontline medical staff during the Covid-19 pandemic. Heliyon 2020, 6, e05766. [Google Scholar] [CrossRef]
- Becker, J.; Zwerenz, R.; Johansson, R.; Frederick, R.J.; Andersson, G.; Beutel, M.E. Using a transdiagnostic, psychodynamic online self-help intervention to maintain inpatient psychosomatic treatment effects: Study protocol of a feasibility study. Internet Interv. 2016, 5, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barsky, A.J. Assessing Somatic Symptoms in Clinical Practice. JAMA Intern. Med. 2014, 174, 407–408. [Google Scholar] [CrossRef]
- Wirtz, M.A.; Morfeld, M.; Glaesmer, H.; Brähler, E. Normierung des SF-12 Version 2.0 zur Messung der gesundheitsbezogenen Lebensqualität in einer deutschen bevölkerungsrepräsentativen Stichprobe. Diagnostica 2018, 64, 215–226. [Google Scholar] [CrossRef]
- Galenkamp, H.; Stronks, K.; Mokkink, L.B.; Derks, E.M. Measurement invariance of the SF-12 among different demographic groups: The HELIUS study. PLoS ONE 2018, 13, e0203483. [Google Scholar] [CrossRef] [Green Version]
- Lenhard, W.; Lenhard, A. Hypothesis Tests for Comparing Correlations; Psychometrica: Bibergau, Germany, 2014. [Google Scholar]
- Lenhard, W.; Lenhard, A. Berechnung von Effektstärken [Calculation of Effect Sizes]. Dettelbach: Psychometrica. 2016. Available online: https://www.psychometrica.de/effektstaerke.html (accessed on 15 February 2020).
- Sawilowsky, S.S. New Effect Size Rules of Thumb. J. Mod. Appl. Stat. Methods 2009, 8, 597–599. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analyses. A Regression-Based Approch, 2nd ed.; The Guildford Press: Guildford, UK, 2018. [Google Scholar]
- Hardt, J.; Buchwald, D.; Wilks, D.; Sharpe, M.; Nix, W.; Egle, U. Health-related quality of life in patients with chronic fatigue syndrome. J. Psychosom. Res. 2001, 51, 431–434. [Google Scholar] [CrossRef]
- Andersson, G. Psychological aspects of tinnitus and the application of cognitive–behavioral therapy. Clin. Psychol. Rev. 2002, 22, 977–990. [Google Scholar] [CrossRef]
- Fuller, T.; Cima, R.; Langguth, B.; Mazurek, B.; Vlaeyen, J.W.; Hoare, D.J. Cognitive behavioural therapy for tinnitus. Cochrane Database Syst. Rev. 2020, 1, CD012614. [Google Scholar] [CrossRef]
- Landry, E.; Sandoval, X.C.R.; Simeone, C.N.; Tidball, G.; Lea, J.; Westerberg, B.D. Systematic Review and Network Meta-analysis of Cognitive and/or Behavioral Therapies (CBT) for Tinnitus. Otol. Neurotol. 2020, 41, 153–166. [Google Scholar] [CrossRef]
- Cima, R.F.F.; Mazurek, B.; Haider, H.; Kikidis, D.; Lapira, A.; Noreña, A.; Hoare, D.J. A multidisciplinary European guideline for tinnitus: Diagnostics, assessment, and treatment. HNO 2019, 67 (Suppl. 1), 10–42. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, B.; Ahmed, A.; Aqeel, M.; Akhtar, T.; Salim, S. Impact of tinnitus perception on psychological distress in male and female tinnitus patients. Found. Univ. J. Psychol. 2017, 1, 56–77. [Google Scholar]
- Noroozian, M.; Jafari, Z.; Shahmiri, E.; Omidvar, S.; Zendehbad, A.; Amini, N.; Radmehr, M.; Bagherian, M.; Yoonessi, A. Effect of Age, Gender and Hearing Loss on the Degree of Discomfort Due to Tinnitus. Basic Clin. Neurosci. J. 2017, 8, 435–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobo, W.V.; Yawn, B.P.; Sauver, J.S.; Grossardt, B.R.; Boyd, C.M.; Rocca, W.A. Prevalence of Combined Somatic and Mental Health Multimorbidity: Patterns by Age, Sex, and Race/Ethnicity. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2016, 71, 1483–1491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLean, C.P.; Asnaani, A.; Litz, B.T.; Hofmann, S.G. Gender Differences in Anxiety Disorders: Prevalence, Course of Illness, Comorbidity and Burden of Illness. J. Psychiatr. Res. 2011, 45, 1027–1035. [Google Scholar] [CrossRef] [Green Version]
- Riecher-Rössler, A. Sex and gender differences in mental disorders. Lancet Psychiatry 2017, 4, 8–9. [Google Scholar] [CrossRef]
- Remes, O.; Brayne, C.; Lafortune, L. The Prevalence of Anxiety Disorders across the Life Course: A Systematic Review of Reviews. Lancet 2014, 384, S66. [Google Scholar] [CrossRef] [Green Version]
- Piccinelli, M.; Wilkinson, G. Gender differences in depression: Critical review. Br. J. Psychiatry 2000, 177, 486–492. [Google Scholar] [CrossRef] [Green Version]
- WHO. Gender and Mental Health; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2017, 4, 146–158. [Google Scholar] [CrossRef]
- Parker, G.; Brotchie, H. Gender differences in depression. Int. Rev. Psychiatry 2010, 22, 429–436. [Google Scholar] [CrossRef]
- Krumm, S.; Checchia, C.; Koesters, M.; Kilian, R.; Becker, T. Men’s Views on Depression: A Systematic Review and Metasynthesis of Qualitative Research. Psychopathology 2017, 50, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Möller-Leimkühler, A.M. Barriers to help-seeking by men: A review of sociocultural and clinical literature with particular reference to depression. J. Affect. Disord. 2002, 71, 1–9. [Google Scholar] [CrossRef]
- Oliffe, J.L.; Kelly, M.T.; Bottorff, J.L.; Johnson, J.L.; Wong, S.T. “He’s More Typically Female Because He’s Not Afraid to Cry”: Connecting Heterosexual Gender Relations and Men’s Depression. In The Psychology of Gender and Health; Elsevier: Amsterdam, The Netherlands, 2017; pp. 177–197. [Google Scholar]
- Seidler, Z.E.; Dawes, A.J.; Rice, S.M.; Oliffe, J.L.; Dhillon, H.M. The role of masculinity in men’s help-seeking for depression: A systematic review. Clin. Psychol. Rev. 2016, 49, 106–118. [Google Scholar] [CrossRef]
- Thompson, A.E.; Anisimowicz, Y.; Miedema, B.; Hogg, W.; Wodchis, W.P.; Aubrey-Bassler, K. The influence of gender and other patient characteristics on health care-seeking behaviour: A QUALICOPC study. BMC Fam. Pract. 2016, 17, 38. [Google Scholar] [CrossRef] [Green Version]
- Whittle, E.L.; Fogarty, A.S.; Tugendrajch, S.; Player, M.J.; Christensen, H.; Wilhelm, K.; Hadzi-Pavlovic, D.; Proudfoot, J. Men, depression, and coping: Are we on the right path? Psychol. Men Masc. 2015, 16, 426–438. [Google Scholar] [CrossRef]
- Yousaf, O.; Grunfeld, E.; Hunter, M.S. A systematic review of the factors associated with delays in medical and psychological help-seeking among men. Health Psychol. Rev. 2015, 9, 264–276. [Google Scholar] [CrossRef]
- Boecking, B.; Von Sass, J.; Sieveking, A.; Schaefer, C.; Brueggemann, P.; Rose, M.; Mazurek, B. Tinnitus-related distress and pain perceptions in patients with chronic tinnitus–Do psychological factors constitute a link? PLoS ONE 2020, 15, e0234807. [Google Scholar] [CrossRef]
- Boecking, B.; Rose, M.; Brueggemann, P.; Mazurek, B. Two birds with one stone—Addressing depressive symptoms, emotional tension and worry improves tinnitus-related distress and affective pain perceptions in patients with chronic tinnitus. PLoS ONE 2021, 16, e0246747. [Google Scholar] [CrossRef]
- Henningsen, P.; Zimmermann, T.; Sattel, H. Medically unexplained physical symptoms, anxiety, and depression: A meta-analytic review. Psychosom. Med. 2003, 65, 528–533. [Google Scholar] [CrossRef]
- Katon, W.; Kleinman, A.; Rosen, G. Depression and somatization: A review: Part I. Am. J. Med. 1982, 72, 127–135. [Google Scholar] [CrossRef]
- Sayar, K.; Ak, I. The predictors of somatization: A review. Bull. Clin. Psychophar. 2001, 11, 266–271. [Google Scholar]
- Cludius, B.; Mennin, D.; Ehring, T. Emotion regulation as a transdiagnostic process. Emotion 2020, 20, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Sloan, E.; Hall, K.; Moulding, R.; Bryce, S.; Mildred, H.; Staiger, P.K. Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: A systematic review. Clin. Psychol. Rev. 2017, 57, 141–163. [Google Scholar] [CrossRef]
- Aazh, H.; Landgrebe, M.; Danesh, A.A.; Moore, B.C. Cognitive Behavioral Therapy for Alleviating the Distress Caused by Tinnitus, Hyperacusis and Misophonia: Current Perspectives. Psychol. Res. Behav. Manag. 2019, 12, 991–1002. [Google Scholar] [CrossRef] [Green Version]
- Trevis, K.J.; McLachlan, N.M.; Wilson, S.J. Psychological mediators of chronic tinnitus: The critical role of depression. J. Affect. Disord. 2016, 204, 234–240. [Google Scholar] [CrossRef]
- Trevis, K.J.; McLachlan, N.M.; Wilson, S.J. A Systematic Review and Meta-Analysis of Psychological Functioning in Chronic Tinnitus. Clin. Psychol. Rev. 2018, 60, 62–86. [Google Scholar] [CrossRef] [PubMed]
- Dudley, R.; Kuyken, W. Formulation in cognitive behavioral therapy: ‘There is nothing either good or bad, but thinking makes it so’. In Formulation in Psychology and Psychotherapy: Making Sense of People’s Problems; Johnstone, L., Dallos, R., Eds.; Routledge: New York, NY, USA, 2006; pp. 17–46. [Google Scholar]
- Rolstad, S.; Adler, J.; Rydén, A. Response Burden and Questionnaire Length: Is Shorter Better? A Review and Meta-analysis. Value Health 2011, 14, 1101–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballard, E.D.; Yarrington, J.S.; Farmer, C.A.; Lener, M.S.; Kadriu, B.; Lally, N.; Zarate, C.A., Jr. Parsing the heterogeneity of depression: An exploratory factor analysis across commonly used depression rating scales. J. Affect. Disord. 2018, 231, 51–57. [Google Scholar] [CrossRef]
- Chen, L.-S.; Eaton, W.W.; Gallo, J.J.; Nestadt, G. Understanding the heterogeneity of depression through the triad of symptoms, course and risk factors: A longitudinal, population-based study. J. Affect. Disord. 2000, 59, 1–11. [Google Scholar] [CrossRef]
- Tull, M.; Gratz, K.L.; Salters, K.; Roemer, L. The Role of Experiential Avoidance in Posttraumatic Stress Symptoms and Symptoms of Depression, Anxiety, and Somatization. J. Nerv. Ment. Dis. 2004, 192, 754–761. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Female | Male | ||
|---|---|---|---|---|
| n | 191 | 161 | ||
| M | SD | M | SD | |
| Age | 53.32 | 11.13 | 51.85 | 11.65 |
| n | % | n | % | |
| Degree | ||||
| None | 2 | 1.0 | 2 | 1.2 |
| School | 59 | 30.9 | 56 | 34.8 |
| Apprenticeship | 42 | 22.0 | 25 | 17.4 |
| Polytechnic degree | 30 | 15.7 | 18 | 11.2 |
| University degree | 58 | 30.4 | 57 | 35.4 |
| Nationality | ||||
| German | 174 | 91.1 | 146 | 90.7 |
| Other | 17 | 8.9 | 15 | 9.3 |
| Relationship Status | ||||
| Single | 37 | 19.4 | 35 | 21.7 |
| Married/Partner | 114 | 59.7 | 112 | 69.6 |
| Divorced | 29 | 15.2 | 13 | 8.1 |
| Widowed | 11 | 5.8 | 1 | 0.6 |
| Work Status | ||||
| Employed | 133 | 69.6 | 116 | 72.0 |
| Unemployed | 58 | 30.4 | 45 | 28.0 |
| Variable | Female | Male | ||
|---|---|---|---|---|
| n | 191 | 161 | ||
| M | SD | M | SD | |
| PTA right | 22.77 | 12.77 | 23.42 | 15.79 |
| PTA left | 22.88 | 14.10 | 23.88 | 13.62 |
| n | % | n | % | |
| Hearing impairment_right | ||||
| None | 141 | 73.8 | 118 | 73.3 |
| Slight | 39 | 20.4 | 27 | 16.8 |
| Moderate | 9 | 4.7 | 8 | 5.0 |
| Severe | 1 | 0.5 | 3 | 1.9 |
| Profound | 1 | 0.5 | 1 | 0.6 |
| Hearing impairment_left | ||||
| None | 141 | 73.8 | 112 | 69.9 |
| Slight | 38 | 19.9 | 33 | 20.5 |
| Moderate | 7 | 3.7 | 12 | 7.5 |
| Severe | 2 | 1.0 | 1 | 0.6 |
| Profound | 1 | 0.5 | 0 | 0 |
| Subjectively perceived hearing impairment | ||||
| Yes | 122 | 63.9 | 88 | 54.7 |
| No | 69 | 36.1 | 73 | 45.3 |
| Duration of tinnitus | ||||
| <½ year | 21 | 11.0 | 16 | 9.9 |
| ½–1 year | 46 | 24.1 | 30 | 18.6 |
| 1–2 years | 23 | 12.0 | 19 | 11.8 |
| 2–4 years | 35 | 18.4 | 17 | 10.6 |
| >4 years | 66 | 34.6 | 79 | 49.1 |
| Localisation | ||||
| left | 36 | 18.8 | 20 | 12.4 |
| right | 35 | 18.3 | 30 | 18.6 |
| binaural | 113 | 34.6 | 106 | 65.8 |
| PTA Right | PTA Left | TQ | HADS-A | HADS-D | PCS | MCS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | M | F | M | F | M | F | M | F | M | F | M | F | M | |
| PTA left | 0.650*** | 0.711*** | ||||||||||||
| TQ | 0.242** | 0.216** | 0.331*** | 0.230** | ||||||||||
| HADS-A | 0.547*** | 0.596*** | ||||||||||||
| HADS-D | 0.182*,† | 0.175*,† | 0.572*** | 0.619*** | 0.660*** | 0.719*** | ||||||||
| PCS | −0.272*** | −0.318** | −0.164* | −0.585***,† | −0.425***,† | −0.470*** | −0.497*** | −0.608*** | −0.546*** | |||||
| MCS | −0.564*** | −0.585*** | −0.660*** | −0.746*** | −0.750*** | −0.744*** | 0.675*** | 0.627*** | ||||||
| SSS-8 | 0.164* | 0.596*** | 0.474*** | 0.469*** | 0.544*** | 0.518*** | 0.498*** | −0.756*** | −0.678*** | −0.596*** | −0.609*** | |||
| HADS-A | HADS-D | ||||||
| M | SD | M | SD | df | t | d | |
| Female | 8.87 | 3.81 | 7.21 | 4.42 | 190 | 6.67 ** | 0.43 |
| Male | 7.40 | 4.15 | 6.50 | 4.56 | 160 | 3.48 *** | 0.21 |
| MCS | PCS | ||||||
| M | SD | M | SD | df | t | d | |
| Female | 36.43 | 10.37 | 39.87 | 9.88 | 190 | −5.68 *** | 0.36 |
| Male | 39.03 | 10.81 | 43.06 | 9.23 | 160 | −5.67 *** | 0.39 |
| Women | Men | |||||
|---|---|---|---|---|---|---|
| M | SD | M | SD | t(350) | d | |
| TQ | 42.46 | 16.22 | 37.01 | 15.92 | −3.17 ** | −0.34 |
| HADS-A | 8.87 | 3.80 | 7.40 | 4.15 | −3.44 ** | −0.37 |
| HADS-D | 7.21 | 4.42 | 6.50 | 4.56 | −1.48 | |
| SSS-8 | 12.96 | 5.79 | 10.09 | 6.05 | 3.68 *** | −0.49 |
| MCS | 36.09 | 10.31 | 39.26 | 10.95 | 2.78 ** | 0.30 |
| PCS | 39.44 | 9.91 | 43.23 | 9.35 | −4.52 *** | 0.40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boecking, B.; Biehl, R.; Brueggemann, P.; Mazurek, B. Health-Related Quality of Life, Depressive Symptoms, Anxiety, and Somatization Symptoms in Male and Female Patients with Chronic Tinnitus. J. Clin. Med. 2021, 10, 2798. https://doi.org/10.3390/jcm10132798
Boecking B, Biehl R, Brueggemann P, Mazurek B. Health-Related Quality of Life, Depressive Symptoms, Anxiety, and Somatization Symptoms in Male and Female Patients with Chronic Tinnitus. Journal of Clinical Medicine. 2021; 10(13):2798. https://doi.org/10.3390/jcm10132798
Chicago/Turabian StyleBoecking, Benjamin, Raphael Biehl, Petra Brueggemann, and Birgit Mazurek. 2021. "Health-Related Quality of Life, Depressive Symptoms, Anxiety, and Somatization Symptoms in Male and Female Patients with Chronic Tinnitus" Journal of Clinical Medicine 10, no. 13: 2798. https://doi.org/10.3390/jcm10132798