
A Practical Guide for the Management of Steroid Induced Hyperglycaemia in the Hospital


Abstract
:1. Introduction
2. Prevalence of Steroid Induced Hyperglycaemia in the Hospital
3. Impact of Steroid Induced Hyperglycaemia
4. Definition of Steroid Induced Hyperglycaemia
5. Treatment Targets
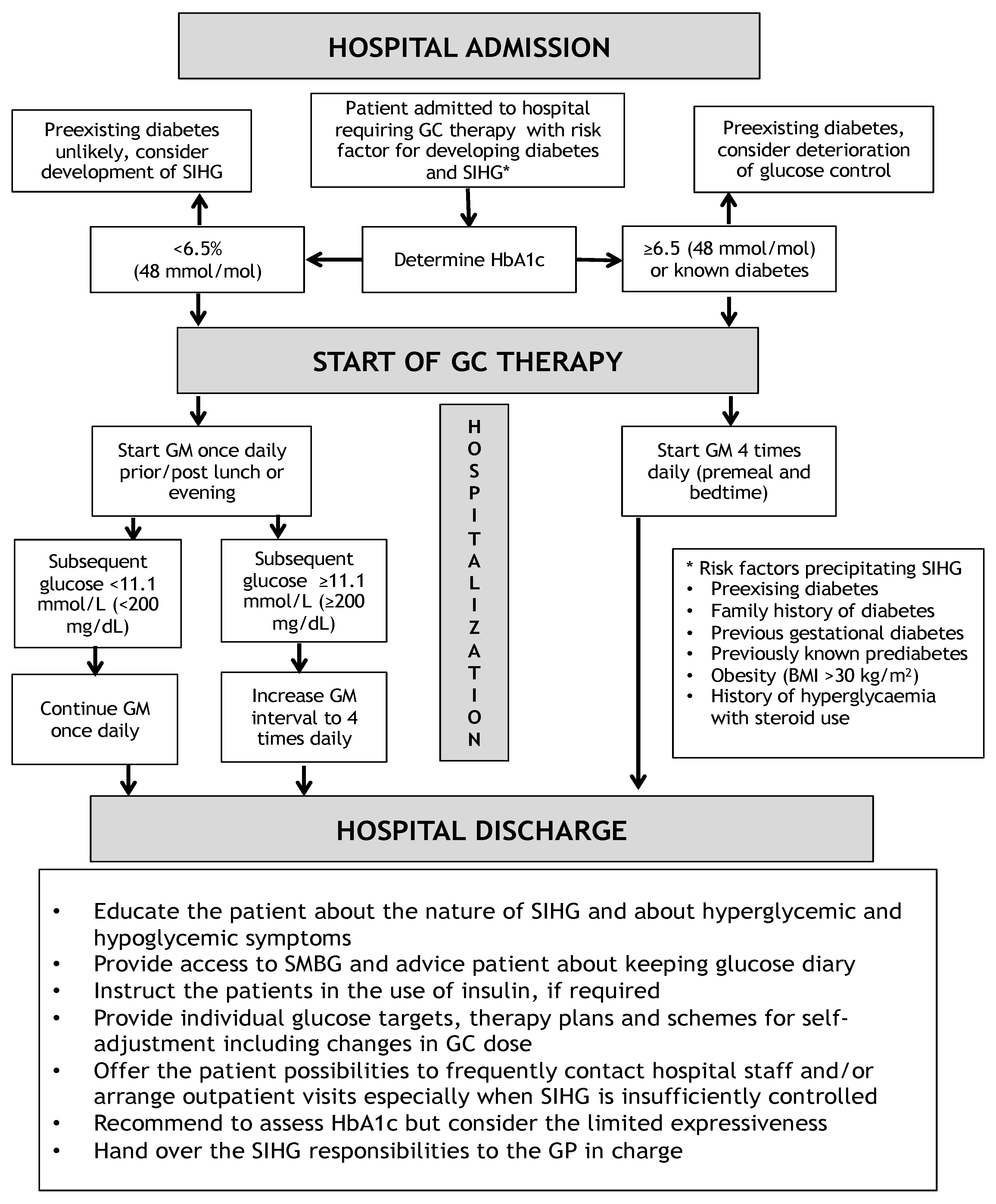
6. Admission to the Hospital
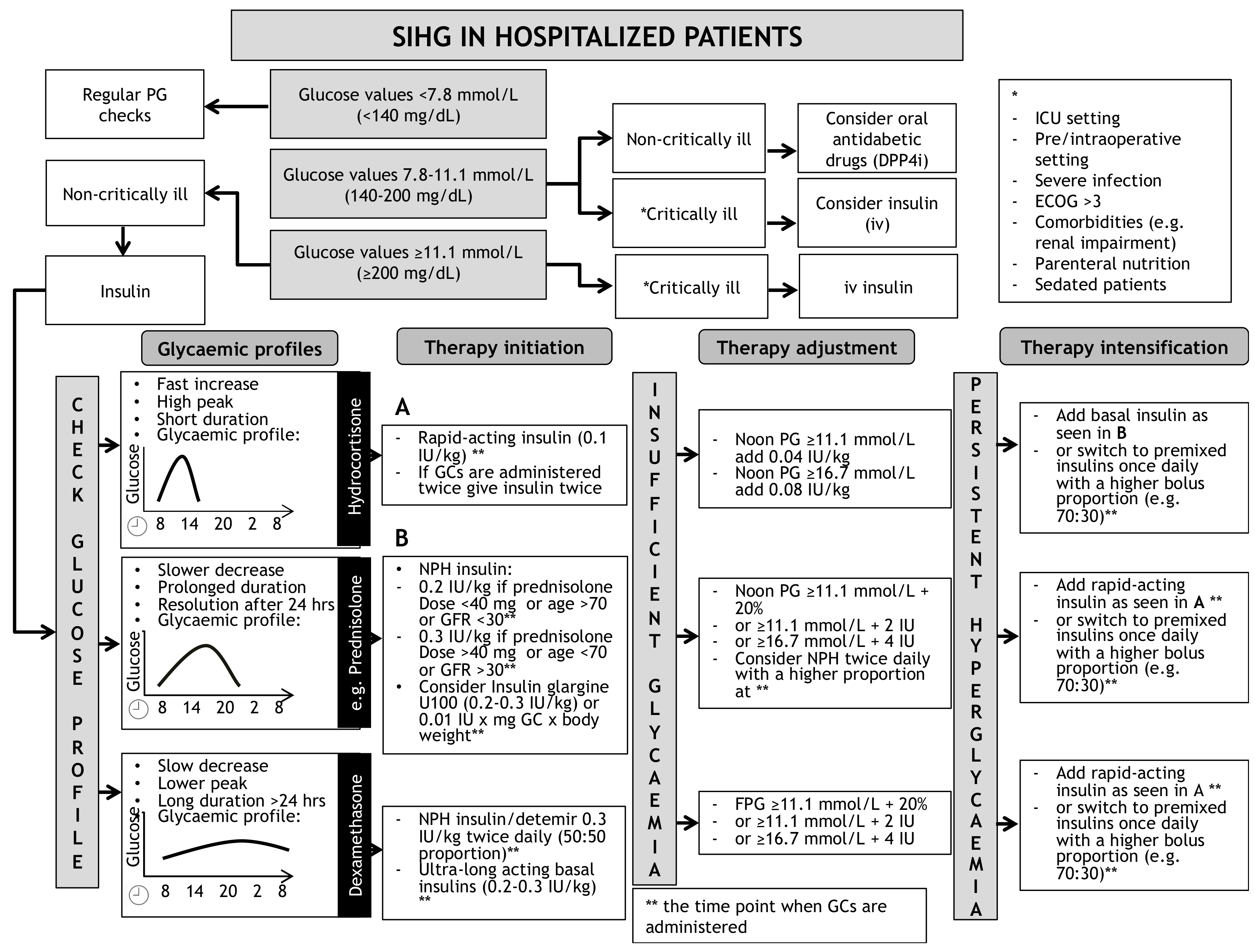
7. Initiation of Glucose Lowering Therapy
8. Treatment of Steroid Induced Hyperglycaemia in the Hospital
8.1. Oral Antihyperglycaemic Agents
8.2. GC Dependent Glucose Increase and the Choice of Insulin Therapy
8.2.1. Scenario 1: Short-Acting Glucocorticoids (Hydrocortisone)
8.2.2. Scenario 2: Intermediate-Acting Glucocorticoids (Predniso(lo)ne and Methylprednisolone)
8.2.3. Scenario 3: Long-Acting Glucocorticoids (Dexamethasone)
8.3. Insulin Intensification and Adjustments
8.3.1. Adjustment of Basal Insulin Therapy
8.3.2. Adjustment of Rapid-Acting Insulin Therapy
8.3.3. Adjustment of Basal-Bolus Insulin
8.3.4. Adjustment of Insulin Therapy in Patients with Type 1 Diabetes (T1DM)
- PE of 20 mg → 10% increase in TDD
- PE of 40 mg → 20% increase in TDD
- PE of 60 mg → 30% increase in TDD
- Adjustments of insulin therapy when short-acting steroids (hydrocortisone) are used:
- ○
- If short acting GCs are used, then an increase of rapid-acting insulin at the time point of GC intake might be sufficient. A correctional rapid-acting insulin dose can be administered in case of persistent hyperglycaemia after 3–4 h when the rapid-acting insulin action has tapered off. As a consequence, the ratio of rapid-acting to basal insulin will exceed the usual 50:50 ratio.
- Adjustments of insulin therapy when intermediate-acting steroids (e.g., prednisolone) are used:
- ○
- Approach A: An increased dose of rapid-acting insulin at the time of intermediate-acting prednisolone administration might be appropriate aiming to achieve glucose control at noon.
- ○
- Approach B: In case of pre-existing therapy with intermediate-acting basal-insulins (NPH insulin or insulin detemir) that are usually injected twice daily, a dose increases at the time point of GC intake (usually in the morning) is recommended.
- ○
- Approach C: In patients previously using (ultra-)long acting basal-insulins (insulin glargine U100/U300 or insulin degludec), approach A might be sufficient; in case of an expected long-term GC treatment, these patients might benefit most from a switch to intermediate-acting basal insulins (NPH insulin, insulin detemir. In such case, the basal insulin should be injected twice daily with a proportionally higher dose at the time point when the GC agent is administered.
- Adjustments of insulin therapy when long-acting steroids (e.g., dexamethasone) are used:
- ○
- Long-acting GCs will trigger continuous and long-lasting hyperglycaemia over 24 h, thus it might be suitable to adjust the total daily basal-insulin dose according to the GC dose as outlined above.
8.3.5. The Critically Ill Patient
9. Discharge from the Hospital
10. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coutinho, A.E.; Chapman, K.E. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol. Cell Endocrinol. 2011, 335, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Trence, D.L. Management of patients on chronic glucocorticoid therapy: An endocrine perspective. Prim. Care 2003, 30, 593–605. [Google Scholar] [CrossRef]
- van Raalte, D.H.; Diamant, M. Steroid diabetes: From mechanism to treatment? Neth. J. Med. 2014, 72, 62–72. [Google Scholar] [PubMed]
- Bonaventura, A.; Montecucco, F. Steroid-induced hyperglycemia: An underdiagnosed problem or clinical inertia? A narrative review. Diabetes Res. Clin. Pract. 2018, 139, 203–220. [Google Scholar] [CrossRef] [Green Version]
- Geer, E.B.; Islam, J.; Buettner, C. Mechanisms of glucocorticoid-induced insulin resistance: Focus on adipose tissue function and lipid metabolism. Endocrinol. Metab. Clin. N. Am. 2014, 43, 75–102. [Google Scholar] [CrossRef] [Green Version]
- Gulliford, M.C.; Charlton, J.; Latinovic, R. Risk of diabetes associated with prescribed glucocorticoids in a large population. Diabetes Care 2006, 29, 2728–2729. [Google Scholar] [CrossRef] [Green Version]
- Fong, A.C.; Cheung, N.W. The high incidence of steroid-induced hyperglycaemia in hospital. Diabetes Res. Clin. Pract. 2013, 99, 277–280. [Google Scholar] [CrossRef]
- Liu, X.X.; Zhu, X.M.; Miao, Q.; Ye, H.Y.; Zhang, Z.Y.; Li, Y.M. Hyperglycemia induced by glucocorticoids in nondiabetic patients: A meta-analysis. Ann. Nutr. Metab. 2014, 65, 324–332. [Google Scholar] [CrossRef]
- Kwon, S.; Hermayer, K.L.; Hermayer, K. Glucocorticoid-induced hyperglycemia. Am. J. Med. Sci. 2013, 345, 274–277. [Google Scholar] [CrossRef]
- Tufton, N.; Ahmad, S.; Rolfe, C.; Rajkariar, R.; Byrne, C.; Chowdhury, T.A. New-onset diabetes after renal transplantation. Diabet. Med. 2014, 31, 1284–1292. [Google Scholar] [CrossRef]
- Stauber, M.N.; Aberer, F.; Oulhaj, A.; Mader, J.K.; Zebisch, A.; Pieber, T.R.; Neumeister, P.; Greinix, H.T.; Sill, H.; Sourij, H.; et al. Early Hyperglycemia after Initiation of Glucocorticoid Therapy Predicts Adverse Outcome in Patients with Acute Graft-versus-Host Disease. Biol. Blood Marrow. Transplant. 2017, 23, 1186–1192. [Google Scholar] [CrossRef] [Green Version]
- Simmons, L.R.; Molyneaux, L.; Yue, D.K.; Chua, E.L. Steroid-induced diabetes: Is it just unmasking of type 2 diabetes? ISRN Endocrinol. 2012, 2012, 910905. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Mackie, S.L.; Pujades-Rodriguez, M. Glucocorticoid dose-dependent risk of type 2 diabetes in six immune-mediated inflammatory diseases: A population-based cohort analysis. BMJ Open Diabetes Res. Care 2020, 8. [Google Scholar] [CrossRef]
- Andersen, Y.M.F.; Egeberg, A.; Ban, L.; Gran, S.; Williams, H.C.; Francis, N.A.; Knop, F.K.; Gislason, G.H.; Skov, L.; Thyssen, J.P. Association Between Topical Corticosteroid Use and Type 2 Diabetes in Two European Population-Based Adult Cohorts. Diabetes Care 2019, 42, 1095–1103. [Google Scholar] [CrossRef] [Green Version]
- Falciglia, M.; Freyberg, R.W.; Almenoff, P.L.; D’Alessio, D.A.; Render, M.L. Hyperglycemia-related mortality in critically ill patients varies with admission diagnosis. Crit Care Med. 2009, 37, 3001–3009. [Google Scholar] [CrossRef]
- Corsino, L.; Dhatariya, K.; Umpierrez, G. Management of Diabetes and Hyperglycemia in Hospitalized Patients. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., Dungan, K., Grossman, A., Hershman, J.M., Kaltsas, G., Koch, C., Kopp, P., et al., Eds.; MDText. com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Umpierrez, G.E.; Hellman, R.; Korytkowski, M.T.; Kosiborod, M.; Maynard, G.A.; Montori, V.M.; Seley, J.J.; Van den Berghe, G.; Endocrine, S. Management of hyperglycemia in hospitalized patients in non-critical care setting: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2012, 97, 16–38. [Google Scholar] [CrossRef] [Green Version]
- Aberer, F.; Kremser, S.; Mader, J.K.; Zinke-Cerwenka, W.; Greinix, H.; Tripolt, N.J.; Pieber, T.R.; Zebisch, A.; Sill, H.; Oulhaj, A.; et al. Hyperglycaemia within the first month after allogeneic haematopoietic stem-cell transplantation is an independent risk factor for overall survival in patients with acute myeloid leukaemia. Diabetes Metab. 2017, 43, 560–562. [Google Scholar] [CrossRef]
- Ali, N.A.; O’Brien, J.M., Jr.; Blum, W.; Byrd, J.C.; Klisovic, R.B.; Marcucci, G.; Phillips, G.; Marsh, C.B.; Lemeshow, S.; Grever, M.R. Hyperglycemia in patients with acute myeloid leukemia is associated with increased hospital mortality. Cancer 2007, 110, 96–102. [Google Scholar] [CrossRef]
- Derr, R.L.; Ye, X.; Islas, M.U.; Desideri, S.; Saudek, C.D.; Grossman, S.A. Association between hyperglycemia and survival in patients with newly diagnosed glioblastoma. J. Clin. Oncol. 2009, 27, 1082–1086. [Google Scholar] [CrossRef]
- Sonabend, R.Y.; McKay, S.V.; Okcu, M.F.; Yan, J.; Haymond, M.W.; Margolin, J.F. Hyperglycemia during induction therapy is associated with poorer survival in children with acute lymphocytic leukemia. J. Pediatr. 2009, 155, 73–78. [Google Scholar] [CrossRef]
- Palepu, S.; Prasad, G.V. New-onset diabetes mellitus after kidney transplantation: Current status and future directions. World J. Diabetes 2015, 6, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Baker, E.H.; Janaway, C.H.; Philips, B.J.; Brennan, A.L.; Baines, D.L.; Wood, D.M.; Jones, P.W. Hyperglycaemia is associated with poor outcomes in patients admitted to hospital with acute exacerbations of chronic obstructive pulmonary disease. Thorax 2006, 61, 284–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newton, C.A.; Smiley, D.; Bode, B.W.; Kitabchi, A.E.; Davidson, P.C.; Jacobs, S.; Steed, R.D.; Stentz, F.; Peng, L.; Mulligan, P.; et al. A comparison study of continuous insulin infusion protocols in the medical intensive care unit: Computer-guided vs. standard column-based algorithms. J. Hosp. Med. 2010, 5, 432–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhatariya, K. Should inpatient hyperglycaemia be treated? BMJ 2013, 346, f134. [Google Scholar] [CrossRef]
- American Diabetes, A. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef]
- Perez, A.; Jansen-Chaparro, S.; Saigi, I.; Bernal-Lopez, M.R.; Minambres, I.; Gomez-Huelgas, R. Glucocorticoid-induced hyperglycemia. J. Diabetes 2014, 6, 9–20. [Google Scholar] [CrossRef]
- Suh, S.; Park, M.K. Glucocorticoid-Induced Diabetes Mellitus: An Important but Overlooked Problem. Endocrinol. Metab. 2017, 32, 180–189. [Google Scholar] [CrossRef]
- American Diabetes, A. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S73–S84. [Google Scholar] [CrossRef]
- American Diabetes, A. 15. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S211–S220. [Google Scholar] [CrossRef]
- Dhatariya, K., II. Does dexamethasone-induced hyperglycaemia contribute to postoperative morbidity and mortality? Br. J. Anaesth. 2013, 110, 674–675. [Google Scholar] [CrossRef] [Green Version]
- Sinclair, A.J.; Dashora, U.; George, S.; Dhatariya, K.; Group, J.-I.W. Joint British Diabetes Societies for Inpatient Care (JBDS-IP) Clinical Guideline Inpatient care of the frail older adult with diabetes: An Executive Summary. Diabet. Med. 2020, 37, 1981–1991. [Google Scholar] [CrossRef]
- Roberts, A.; James, J.; Dhatariya, K.; Joint British Diabetes Societies for Inpatient, C. Management of hyperglycaemia and steroid (glucocorticoid) therapy: A guideline from the Joint British Diabetes Societies (JBDS) for Inpatient Care group. Diabet. Med. 2018, 35, 1011–1017. [Google Scholar] [CrossRef]
- Dhatariya, K.E.; James, J.; Kong, M.F.; Berrington, R.; Joint British Diabetes Society (JBDS) for Inpatient Care Group; Guidelines Writing Group. Diabetes at the front door. A guideline for dealing with glucose related emergencies at the time of acute hospital admission from the Joint British Diabetes Society (JBDS) for Inpatient Care Group. Diabet. Med. 2020, 37, 1578–1589. [Google Scholar] [CrossRef]
- Imatoh, T.; Sai, K.; Hori, K.; Segawa, K.; Kawakami, J.; Kimura, M.; Saito, Y. Development of a novel algorithm for detecting glucocorticoid-induced diabetes mellitus using a medical information database. J. Clin. Pharm. Ther. 2017, 42, 215–220. [Google Scholar] [CrossRef]
- van Genugten, R.E.; van Raalte, D.H.; Muskiet, M.H.; Heymans, M.W.; Pouwels, P.J.; Ouwens, D.M.; Mari, A.; Diamant, M. Does dipeptidyl peptidase-4 inhibition prevent the diabetogenic effects of glucocorticoids in men with the metabolic syndrome? A randomized controlled trial. Eur. J. Endocrinol. 2014, 170, 429–439. [Google Scholar] [CrossRef] [Green Version]
- van Raalte, D.H.; van Genugten, R.E.; Linssen, M.M.; Ouwens, D.M.; Diamant, M. Glucagon-like peptide-1 receptor agonist treatment prevents glucocorticoid-induced glucose intolerance and islet-cell dysfunction in humans. Diabetes Care 2011, 34, 412–417. [Google Scholar] [CrossRef] [Green Version]
- Seelig, E.; Meyer, S.; Timper, K.; Nigro, N.; Bally, M.; Pernicova, I.; Schuetz, P.; Muller, B.; Korbonits, M.; Christ-Crain, M. Metformin prevents metabolic side effects during systemic glucocorticoid treatment. Eur. J. Endocrinol. 2017, 176, 349–358. [Google Scholar] [CrossRef]
- Willi, S.M.; Kennedy, A.; Brant, B.P.; Wallace, P.; Rogers, N.L.; Garvey, W.T. Effective use of thiazolidinediones for the treatment of glucocorticoid-induced diabetes. Diabetes Res. Clin. Pract. 2002, 58, 87–96. [Google Scholar] [CrossRef]
- Pernicova, I.; Kelly, S.; Ajodha, S.; Sahdev, A.; Bestwick, J.P.; Gabrovska, P.; Akanle, O.; Ajjan, R.; Kola, B.; Stadler, M.; et al. Metformin to reduce metabolic complications and inflammation in patients on systemic glucocorticoid therapy: A randomised, double-blind, placebo-controlled, proof-of-concept, phase 2 trial. Lancet Diabetes Endocrinol. 2020, 8, 278–291. [Google Scholar] [CrossRef]
- He, J.; Xu, C.; Kuang, J.; Liu, Q.; Jiang, H.; Mo, L.; Geng, B.; Xu, G. Thiazolidinediones attenuate lipolysis and ameliorate dexamethasone-induced insulin resistance. Metabolism 2015, 64, 826–836. [Google Scholar] [CrossRef]
- Gerards, M.C.; Venema, G.E.; Patberg, K.W.; Kross, M.; Potter van Loon, B.J.; Hageman, I.M.G.; Snijders, D.; Brandjes, D.P.M.; Hoekstra, J.B.L.; Vriesendorp, T.M.; et al. Dapagliflozin for prednisone-induced hyperglycaemia in acute exacerbation of chronic obstructive pulmonary disease. Diabetes Obes. Metab. 2018, 20, 1306–1310. [Google Scholar] [CrossRef] [Green Version]
- Wallace, M.D.; Metzger, N.L. Optimizing the Treatment of Steroid-Induced Hyperglycemia. Ann. Pharmacother. 2018, 52, 86–90. [Google Scholar] [CrossRef]
- Liu, D.; Ahmet, A.; Ward, L.; Krishnamoorthy, P.; Mandelcorn, E.D.; Leigh, R.; Brown, J.P.; Cohen, A.; Kim, H. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin. Immunol. 2013, 9, 30. [Google Scholar] [CrossRef] [Green Version]
- Barbot, M.; Ceccato, F.; Scaroni, C. Diabetes Mellitus Secondary to Cushing’s Disease. Front. Endocrinol. 2018, 9, 284. [Google Scholar] [CrossRef] [PubMed]
- Tamez-Perez, H.E.; Quintanilla-Flores, D.L.; Rodriguez-Gutierrez, R.; Gonzalez-Gonzalez, J.G.; Tamez-Pena, A.L. Steroid hyperglycemia: Prevalence, early detection and therapeutic recommendations: A narrative review. World J. Diabetes 2015, 6, 1073–1081. [Google Scholar] [CrossRef]
- Clore, J.N.; Thurby-Hay, L. Glucocorticoid-induced hyperglycemia. Endocr. Pract. 2009, 15, 469–474. [Google Scholar] [CrossRef]
- Khowaja, A.; Alkhaddo, J.B.; Rana, Z.; Fish, L. Glycemic Control in Hospitalized Patients with Diabetes Receiving Corticosteroids Using a Neutral Protamine Hagedorn Insulin Protocol: A Randomized Clinical Trial. Diabetes Ther. 2018, 9, 1647–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radhakutty, A.; Stranks, J.L.; Mangelsdorf, B.L.; Drake, S.M.; Roberts, G.W.; Zimmermann, A.T.; Stranks, S.N.; Thompson, C.H.; Burt, M.G. Treatment of prednisolone-induced hyperglycaemia in hospitalized patients: Insights from a randomized, controlled study. Diabetes Obes. Metab. 2017, 19, 571–578. [Google Scholar] [CrossRef]
- Ruiz de Adana, M.S.; Colomo, N.; Maldonado-Araque, C.; Fontalba, M.I.; Linares, F.; Garcia-Torres, F.; Fernandez, R.; Bautista, C.; Olveira, G.; de la Cruz, J.L.; et al. Randomized clinical trial of the efficacy and safety of insulin glargine vs. NPH insulin as basal insulin for the treatment of glucocorticoid induced hyperglycemia using continuous glucose monitoring in hospitalized patients with type 2 diabetes and respiratory disease. Diabetes Res. Clin. Pract. 2015, 110, 158–165. [Google Scholar] [CrossRef]
- Aberer, F.; Mader, J.K.; Holzgruber, J.; Trummer, C.; Schwetz, V.; Pandis, M.; Pferschy, P.N.; Greinix, H.; Tripolt, N.J.; Pieber, T.R.; et al. Feasibility and safety of using an automated decision support system for insulin therapy in the treatment of steroid-induced hyperglycemia in patients with acute graft-versus-host disease: A randomized trial. J. Diabetes Investig. 2019, 10, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Seggelke, S.A.; Gibbs, J.; Draznin, B. Pilot study of using neutral protamine Hagedorn insulin to counteract the effect of methylprednisolone in hospitalized patients with diabetes. J. Hosp. Med. 2011, 6, 175–176. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Li, G. Inpatient use of glucocorticoids may mediate the detrimental effect of new-onset hyperglycemia on COVID-19 severity. Diabetes Res. Clin. Pract. 2020, 168, 108441. [Google Scholar] [CrossRef]
- Morieri, M.L.; Fadini, G.P.; Boscari, F.; Fioretto, P.; Maran, A.; Busetto, L.; Crepaldi, M.C.; Vedovato, M.; Bonora, B.M.; Selmin, E.; et al. Hyperglycemia, glucocorticoid therapy, and outcome of COVID-19. Diabetes Res. Clin. Pract. 2020, 168, 108449. [Google Scholar] [CrossRef]
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [Google Scholar] [CrossRef]
- Fadini, G.P.; Morieri, M.L.; Boscari, F.; Fioretto, P.; Maran, A.; Busetto, L.; Bonora, B.M.; Selmin, E.; Arcidiacono, G.; Pinelli, S.; et al. Newly-diagnosed diabetes and admission hyperglycemia predict COVID-19 severity by aggravating respiratory deterioration. Diabetes Res. Clin. Pract. 2020, 168, 108374. [Google Scholar] [CrossRef]
- Rayman, G.; Lumb, A.N.; Kennon, B.; Cottrell, C.; Nagi, D.; Page, E.; Voigt, D.; Courtney, H.C.; Atkins, H.; Higgins, K.; et al. Dexamethasone therapy in COVID-19 patients: Implications and guidance for the management of blood glucose in people with and without diabetes. Diabet. Med. 2021, 38, e14378. [Google Scholar] [CrossRef]
- Zenz, S.; Mader, J.K.; Regittnig, W.; Brunner, M.; Korsatko, S.; Boulgaropoulos, B.; Magnes, C.; Raml, R.; Narath, S.H.; Eller, P.; et al. Impact of C-Peptide Status on the Response of Glucagon and Endogenous Glucose Production to Induced Hypoglycemia in T1DM. J. Clin. Endocrinol. Metab. 2018, 103, 1408–1417. [Google Scholar] [CrossRef] [Green Version]
- Bevier, W.C.; Zisser, H.C.; Jovanovic, L.; Finan, D.A.; Palerm, C.C.; Seborg, D.E.; Doyle, F.J., 3rd. Use of continuous glucose monitoring to estimate insulin requirements in patients with type 1 diabetes mellitus during a short course of prednisone. J. Diabetes Sci. Technol. 2008, 2, 578–583. [Google Scholar] [CrossRef] [Green Version]
- Dashora, U.K.; Taylor, R. Maintaining glycaemic control during high-dose prednisolone administration for hyperemesis gravidarum in Type 1 diabetes. Diabet. Med. 2004, 21, 298–299. [Google Scholar] [CrossRef]
- Best, C.J.; Thosani, S.; Ortiz, M.; Levesque, C.; Varghese, S.S.; Lavis, V.R. Co-Managing Patients with Type 1 Diabetes and Cancer. Curr. Diab. Rep. 2016, 16, 73. [Google Scholar] [CrossRef] [PubMed]
- Umpierrez, G.E.; Klonoff, D.C. Diabetes Technology Update: Use of Insulin Pumps and Continuous Glucose Monitoring in the Hospital. Diabetes Care 2018, 41, 1579–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mader, J.K.; Brix, J.; Aberer, F.; Vonbank, A.; Resl, M.; Pieber, T.R.; Stechemesser, L.; Sourij, H. Hospital diabetes management (Update 2019). Wien. Klin. Wochenschr. 2019, 131, 200–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, E.; Devendra, S. Steroid-induced hyperglycaemia in primary care. Lond. J. Prim. Care 2015, 7, 103–106. [Google Scholar] [CrossRef] [Green Version]
- Group, R.C.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Gandhi, G.Y.; Murad, M.H.; Flynn, D.N.; Erwin, P.J.; Cavalcante, A.B.; Bay Nielsen, H.; Capes, S.E.; Thorlund, K.; Montori, V.M.; Devereaux, P.J. Effect of perioperative insulin infusion on surgical morbidity and mortality: Systematic review and meta-analysis of randomized trials. Mayo Clin. Proc. 2008, 83, 418–430. [Google Scholar] [CrossRef] [Green Version]
- Sampson, M.J.; Dozio, N.; Ferguson, B.; Dhatariya, K. Total and excess bed occupancy by age, specialty and insulin use for nearly one million diabetes patients discharged from all English Acute Hospitals. Diabetes Res. Clin. Pract. 2007, 77, 92–98. [Google Scholar] [CrossRef]
- Evans, N.R.; Dhatariya, K.K. Assessing the relationship between admission glucose levels, subsequent length of hospital stay, readmission and mortality. Clin. Med. 2012, 12, 137–139. [Google Scholar] [CrossRef] [Green Version]
- Investigators, N.-S.S.; Finfer, S.; Liu, B.; Chittock, D.R.; Norton, R.; Myburgh, J.A.; McArthur, C.; Mitchell, I.; Foster, D.; Dhingra, V.; et al. Hypoglycemia and risk of death in critically ill patients. N. Engl. J. Med. 2012, 367, 1108–1118. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Glucocorticoids | Approximate Equivalent Dose (mg) | Plasma Peak Concentration (minutes) | Elimination Half-Life (hours) | Duration of Action (hours) | Hyperglycaemic Effects (hours) | |||
|---|---|---|---|---|---|---|---|---|
| Onset | Peak | Resolution | ||||||
| Short-acting | Hydrocortisone | 20 | 10 | 2 | 8–12 | 1 | 3 | 6 |
| Intermediate-acting | Predniso(lo)ne | 5 | 60–180 | 2.5 | 12–36 | 4 | 8 | 12–16 |
| Methylprednisolone | 4 | 60 | 2.5 | 12–36 | 4 | 8 | 12–16 | |
| Long-acting | Dexamethasone | 0.75 | 60–120 | 4 | 36–72 | 8 | variable | 24–36 |
| Glucocorticoids | Hyperglycaemic Effects (hours) | Glucose Profiles (GC Given Once Daily [8 a.m.]) | Glucose Profiles (GC Given Twice Daily [8 a.m. and 20 p.m.]) | |||
|---|---|---|---|---|---|---|
| Onset | Peak | Resolution | ||||
| Short-acting | Hydrocortisone | 1 | 3 | 6 |  |  |
| Intermediate-acting | Predniso(lo)ne | 4 | 8 | 12–16 |  |  |
| Methylprednisolone | 4 | 8 | 12–16 | |||
| Long-acting | Dexamethasone | 8 | variable | 24–36 |  | n.a. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aberer, F.; Hochfellner, D.A.; Sourij, H.; Mader, J.K. A Practical Guide for the Management of Steroid Induced Hyperglycaemia in the Hospital. J. Clin. Med. 2021, 10, 2154. https://doi.org/10.3390/jcm10102154
Aberer F, Hochfellner DA, Sourij H, Mader JK. A Practical Guide for the Management of Steroid Induced Hyperglycaemia in the Hospital. Journal of Clinical Medicine. 2021; 10(10):2154. https://doi.org/10.3390/jcm10102154
Chicago/Turabian StyleAberer, Felix, Daniel A. Hochfellner, Harald Sourij, and Julia K. Mader. 2021. "A Practical Guide for the Management of Steroid Induced Hyperglycaemia in the Hospital" Journal of Clinical Medicine 10, no. 10: 2154. https://doi.org/10.3390/jcm10102154