Continuous Maternal Hemodynamics Monitoring at Delivery Using a Novel, Noninvasive, Wireless, PPG-Based Sensor

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
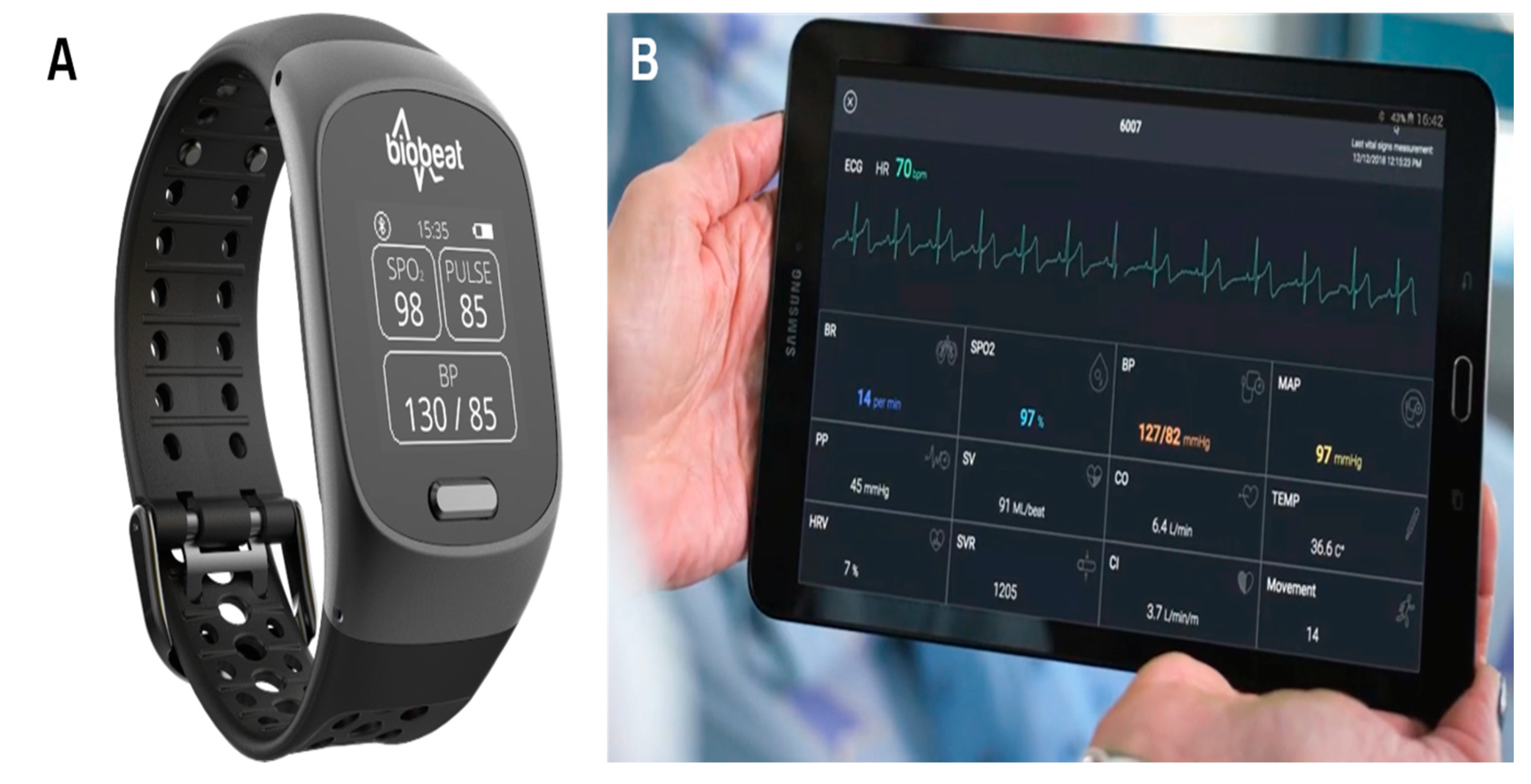
2.2. The PPG-Based Remote Patient Monitoring Device
2.3. Data Collection
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
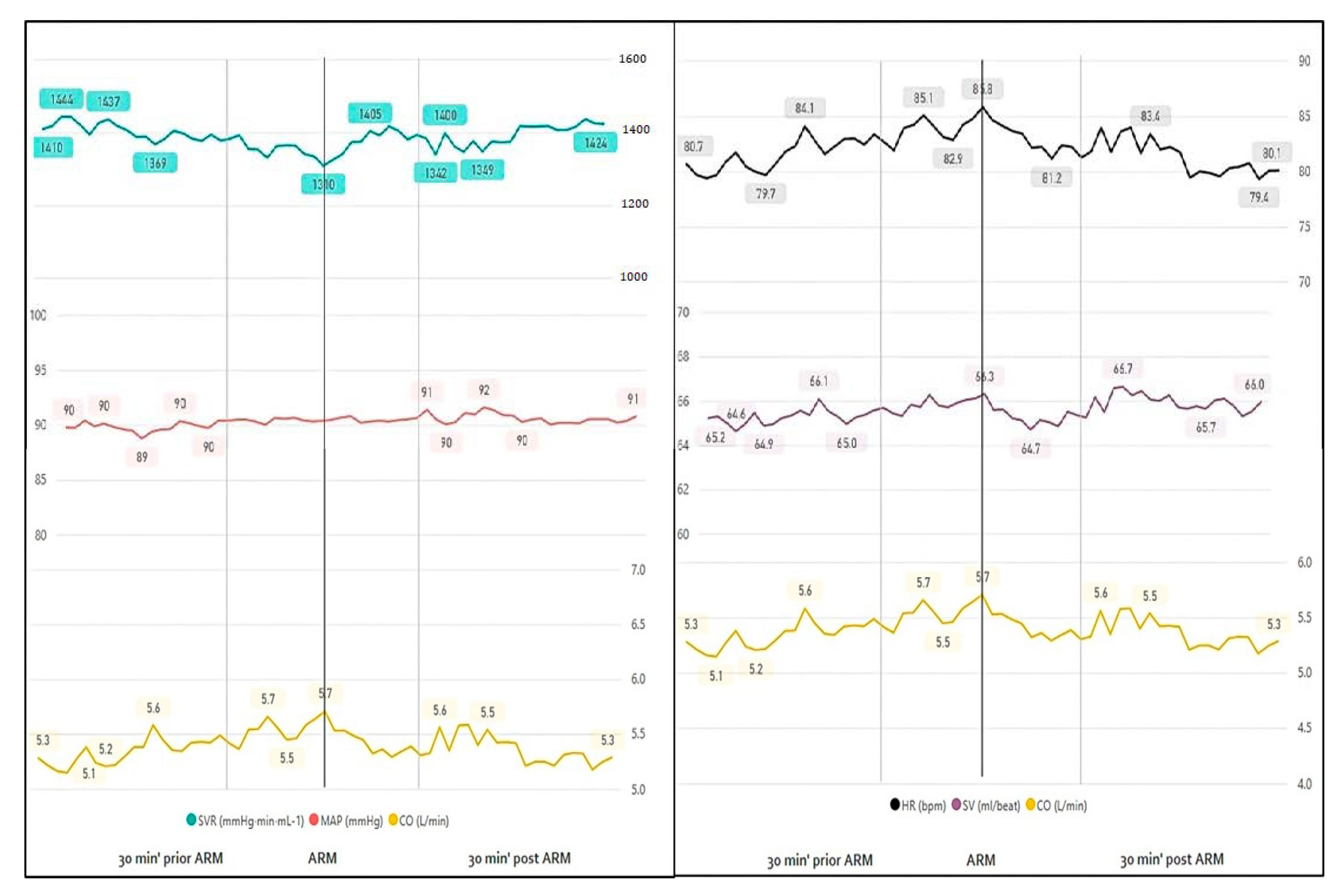
3.1. Epidural Anesthesia
3.1.1. Rupture of Membranes
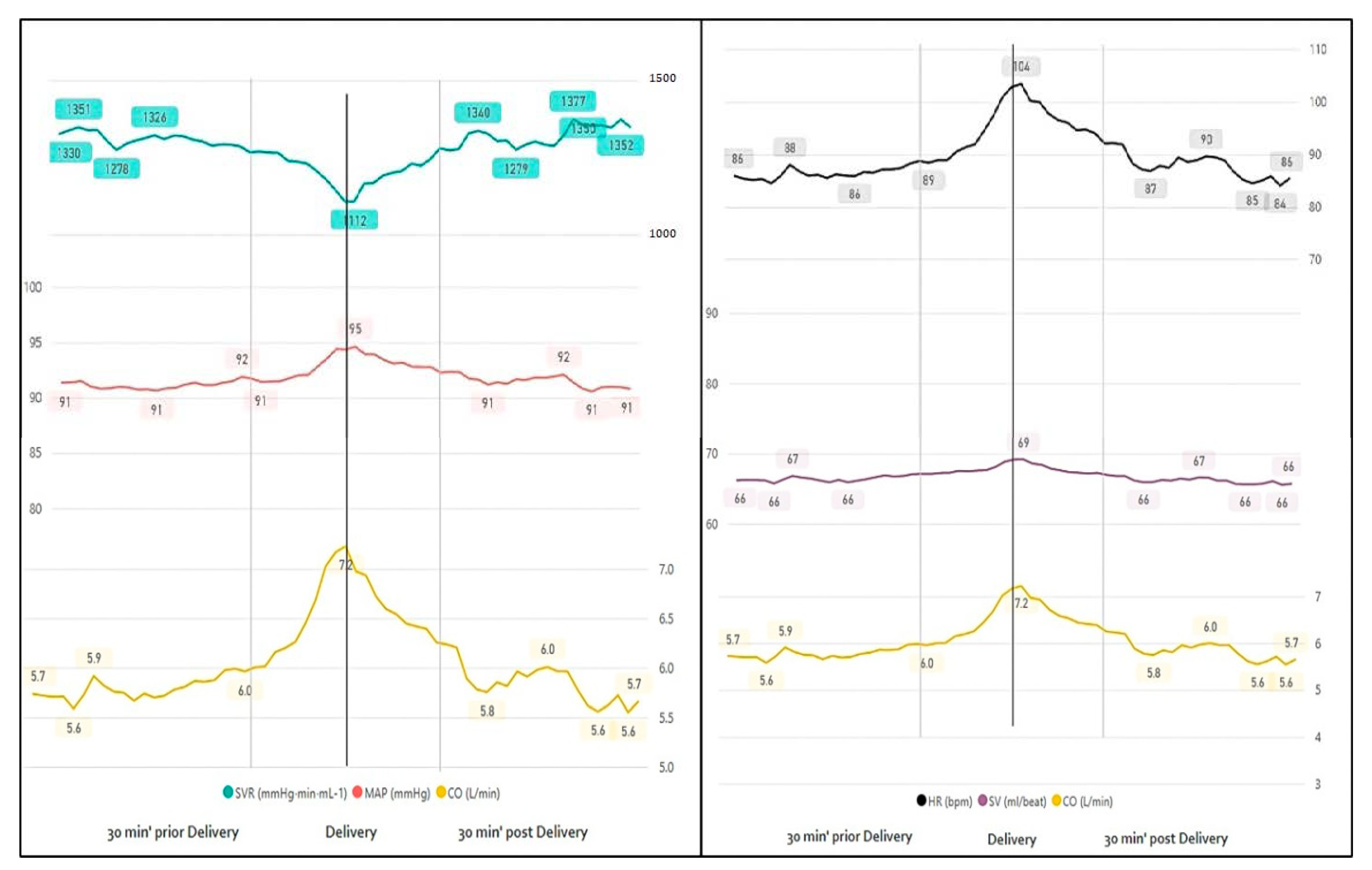
3.1.2. Delivery
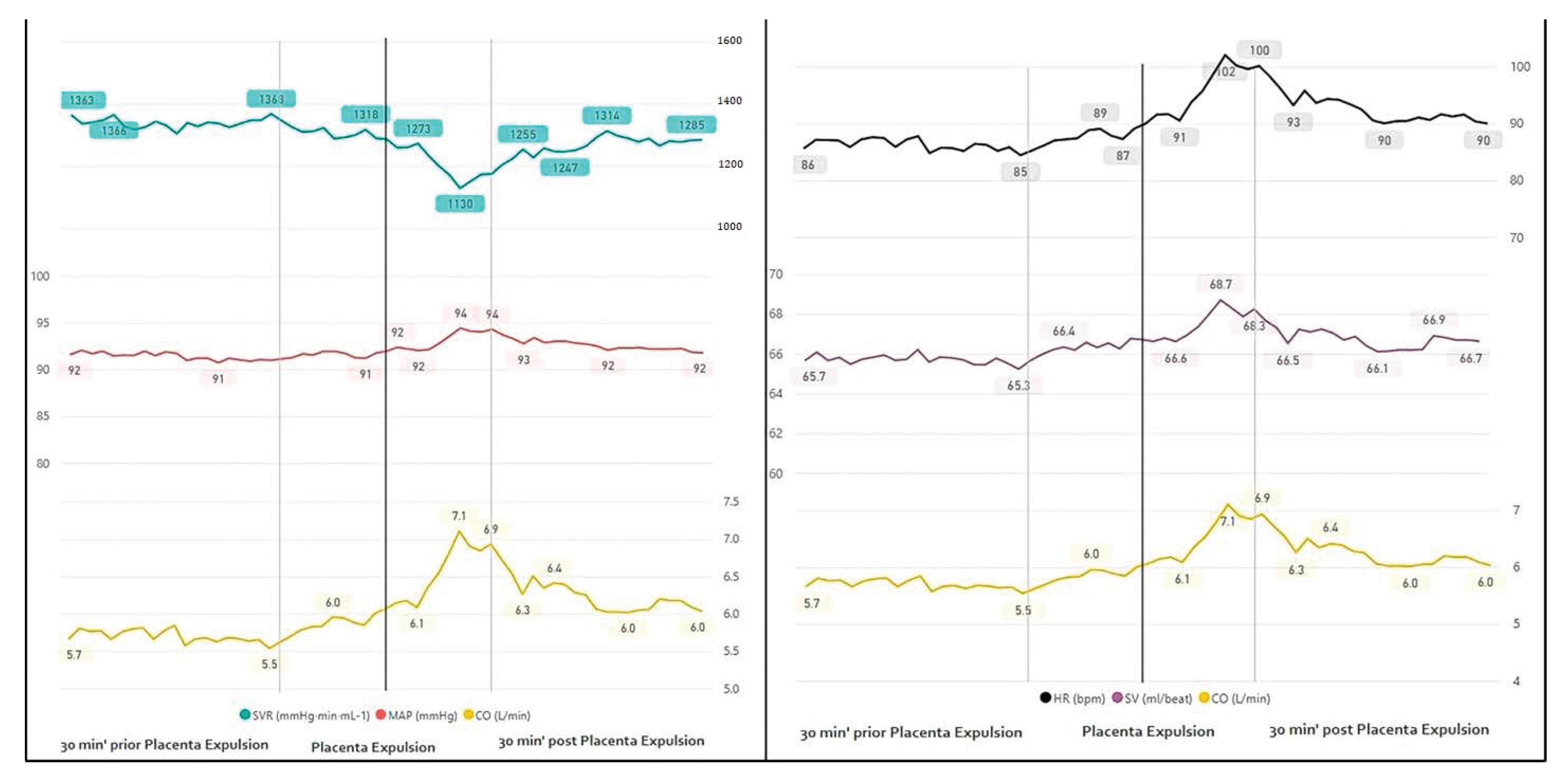
3.1.3. Placental Expulsion
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ouzounian, J.G.; Elkayam, U. Physiologic changes during normal pregnancy and delivery. Cardiol. Clin. 2012, 30, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Hunter, S.; Robson, S.C. Adaptation of the maternal heart in pregnancy. Br. Heart J. 1992, 68, 540–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, A.B.; Abraham, W.T.; Zamudio, S.; Coffin, C.; Merouani, A.; Young, D.; Johnson, A.; Osorio, F.; Goldberg, C.; Moore, L.G.; et al. Temporal relationships between hormonal and hemodynamic changes in early human pregnancy. Kidney Int. 1998, 54, 2056. [Google Scholar] [CrossRef] [Green Version]
- Meah, V.L.; Cockcroft, J.R.; Backx, K.; Shave, R.; Stöhr, E.J. Cardiac output and related haemodynamics during pregnancy: A series of meta-analyses. Heart 2016, 102, 518. [Google Scholar] [CrossRef] [PubMed]
- Duvekot, J.J.; Cheriex, E.C.; Pieters, F.A.; Menheere, P.P.; Peeters, L.H. Early pregnancy changes in hemodynamics and volume homeostasis are consecutive adjustments triggered by a primary fall in systemic vascular tone. Am. J. Obstet. Gynecol. 1993, 169, 1382. [Google Scholar] [CrossRef]
- Maruta, S. The observation of thematernal hemodynamics during labor and cesarean section. Nippon Sanka Fujinka Gakkai Zasshi 1982, 34, 776–784. [Google Scholar]
- Mahendru, A.A.; Everett, T.R.; Wilkinson, I.B.; Lees, C.C.; McEniery, C.M. A longitudinal study of maternal cardiovascular function from preconception to the postpartum period. J. Hypertens. 2014, 32, 849–856. [Google Scholar] [CrossRef]
- Morris, E.A.; Hale, S.A.; Badger, G.J.; Magness, R.R.; Bernstein, I.M. Pregnancy induces persistent changes in vascular compliance in primiparous women. Am. J. Obstet. Gynecol. 2015, 212, 633.e1–633.e6. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, M.B.; Bille-Brahe, N.E.; Engell, H.C. Cardiac output measurement by thermal dilution: Reproducibility and comparison with the dye-dilution technique. Ann. Surg. 1976, 183, 67–72. [Google Scholar] [CrossRef]
- Fegler, G. The reliability of the thermodilution method for determination of the cardiac output and the blood flow in central veins. Q. J. Exp. Physiol. Cogn. Med. Sci. 1957, 42, 254–266. [Google Scholar] [CrossRef] [Green Version]
- Driul, L.; Meroi, F.; Sala, A.; Delrio, S.; Pavoni, D.; Barbariol, F.; Londero, A.; Dogareschi, T.; Spasiano, A.; Vetrugno, L.; et al. Vaginal delivery in a patient with severe aortic stenosis under epidural analgesia, a case report. Cardiovasc. Ultrasound 2020, 18, 43. [Google Scholar] [CrossRef] [PubMed]
- Swan, H.J.; Ganz, W.; Forrester, J.; Marcus, H.; Diamond, G.; Chonette, D. Catheterization of the heart in man with use of a flow-directed balloontipped catheter. N. Engl. J. Med. 1970, 283, 447–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ventura, H.O.; Taler, S.J.; Strobeck, J.E. Hypertension as a hemodynamic disease: The role of impedance cardiography in diagnostic, prognostic, and therapeutic decision making. Am. J. Hypertens. 2005, 18, 26S–43S. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S.; Harrison, D.A.; Singer, M.; Ashcroft, J.; Jones, C.M.; Elbourne, D.; Brampton, W.; Williams, D.; Young, D.; Rowan, K. PAC-Man study collaboration. Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-man): A randomized controlled trial. Lancet 2005, 366, 472–477. [Google Scholar] [CrossRef]
- Peters, S.G.; Afessa, B.; Decker, P.A.; Schroeder, D.R.; Offord, K.P.; Scott, J.P. Increased risk associated with pulmonary artery catheterization in the medical intensive care unit. J. Crit. Care 2003, 18, 166–171. [Google Scholar] [CrossRef]
- Vetrugno, L.; Dogareschi, T.; Sassanelli, R.; Orso, D.; Seremet, L.; Mattuzzi, L.; Scapol, S.; Spasiano, A.; Cagnacci, A.; Bove, T. Thoracic ultrasound evaluation and B-type natriuretic peptide value in elective cesarean section under spinal anesthesia. Ultrasound J. 2020, 12, 10. [Google Scholar] [CrossRef] [Green Version]
- Arbeid, E.; Demi, A.; Brogi, E.; Gori, E.; Giusto, T.; Soldati, G.; Vetrugno, L.; Giunta, F.; Forfori, F. Lung Ultrasound Pattern Is Normal during the Last Gestational Weeks: An Observational Pilot Study. Gynecol. Obstet. Investig. 2017, 82, 398–403. [Google Scholar] [CrossRef]
- Easterling, T.F.; Benedetti, T.J.; Schmucker, B.C.; Millard, S.P. Maternal hemodynamics in normal and preeclamptic pregnancies; a longitudinal study. Obstet. Gynecol. 1990, 76, 1061–1069. [Google Scholar]
- Ashwal, E.; Shinar, S.; Orbach-Zinger, S.; Lev, S.; Gat, R.; Kedar, L.; Pauzner, Y.; Aviram, A.; Yogev, Y.; Hiersch, L. The Hemodynamics of Labor in Women Undergoing Vaginal and Cesarean Deliveries as Determined by Whole Body Bioimpedance. Am. J. Perinatol. 2018, 35, 177–183. [Google Scholar] [CrossRef]
- Lavie, A.; Ram, M.; Lev, S.; Blecher, Y.; Amikam, U.; Shulman, Y.; Avnon, T.; Weiner, E.; Many, A. Maternal cardiovascular hemodynamics in normotensive versus preeclamptic pregnancies: A prospective longitudinal study using a noninvasive cardiac system (NICaS™). BMC Pregnancy Childbirth 2018, 18, 229. [Google Scholar] [CrossRef]
- Young, J.D.; McQuillan, P. Comparison of thoracic electrical bioimpedance and thermodilution for the measurement of cardiac index in patients with severe sepsis. Br. J. Anaesth. 1993, 70, 58–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotshall, R.W.; Wood, V.C.; Miles, D.S. Comparison of two impedance cardiographic techniques for measuring cardiac output in critically ill patients. Crit. Care Med. 1989, 17, 806–811. [Google Scholar] [CrossRef] [PubMed]
- Nachman, D.; Gepner, Y.; Goldstein, N.; Kabakov, E.; Ishay, A.B.; Littman, R.; Azmon, Y.; Jaffe, E.; Eisenkraft, A. Comparing Blood Pressure Measurements Between a Photoplethysmography-Based and a Standard Cuff-Based Manometry Device. Sci. Rep. 2020, 10, 16116. [Google Scholar] [CrossRef] [PubMed]
- Grant, G.J.; Susser, L.; Cascio, M.; Zakowski, M.I. Hemodynamic effects of intrathecal fentanyl in nonlaboring term parturients. J. Clin. Anesth. 1996, 8, 99. [Google Scholar] [CrossRef]
- Palmer, C.M.; Van Maren, G.; Nogami, W.M.; Alves, D. Bupivacaine augments intrathecal fentanyl for labor analgesia. Anesthesiology 1999, 91, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simmons, S.W.; Taghizadeh, N.; Dennis, A.T.; Hughes, D.; Cyna, A.M. Combined spinal-epidural versus epidural analgesia in labour. Cochrane DatabaseSyst. Rev. 2012, 10, CD003401. [Google Scholar] [CrossRef] [PubMed]
- Grangier, L.; de Tejada, B.M.; Savoldelli, G.L.; Irion, O.; Haller, G. Adverse side effects and route of administration of opioids in combined spinal-epidural analgesia for labour: A meta-analysis of randomised trials. Int. J. Obstet. Anesth. 2020, 41, 83. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal age, years | 30 (21–42) |
| Advanced maternal age (>35 years) | 16 (19.7) |
| BMI, Kg/m2 | 29.2 (20.7–48.1) |
| Class II–III BMI (>35 Kg/m2) | 36 (44.4) |
| Nulliparity | 24 (29.6) |
| Gestational diabetes | 14 (17.3) |
| Induction of labor | 33 (40.7) |
| Epidural anesthesia | 69 (85.2) |
| Artificial rupture of membranes | 50 (61.7) |
| Gestational age at delivery in weeks | 39.4 (37–41.9) |
| Birth weight in grams | 3265 (2615–4494) |
| Epidural Anesthesia | |||
| 10 min prior | 10 min after | p-Value | |
| HR | 81.9 | 84.0 | 0.0727 |
| SVR | 1361 | 1319 | 0.0177 |
| CO | 5.5 | 5.6 | 0.0079 |
| SV | 66.6 | 66.9 | 0.0733 |
| MAP | 89.4 | 89.8 | 0.2464 |
| SBP | 123.5 | 123.9 | 0.4724 |
| DBP | 72.2 | 72.7 | 0.1822 |
| Rupture of MEMBRANES | |||
| 10 min prior | 10 min after | p-Value | |
| HR | 88 | 85 | 0.3502 |
| SVR | 1233 | 1282 | 0.2601 |
| CO | 5.8 | 5.5 | 0.3113 |
| SV | 65.9 | 64.4 | 0.1309 |
| MAP | 87.9 | 86.6 | 0.0614 |
| SBP | 120 | 119.7 | 0.0832 |
| DBP | 71.6 | 70 | 0.0526 |
| Delivery | |||
| 30 min prior | 30 min after | p-Value | |
| HR | 88.8 | 90.5 | 0.0002 |
| SVR | 1284 | 1280 | 0.0000 |
| CO | 6.0 | 6.1 | 0.0003 |
| SV | 67.0 | 67.1 | 0.0001 |
| MAP | 92.0 | 92.1 | 0.0059 |
| SBP | 125.5 | 126.1 | 0.0071 |
| DBP | 75.2 | 75.1 | 0.0061 |
| Placental Expulsion | |||
| 10 min prior | 10 min after | p-Value | |
| HR | 88.5 | 96 | 0.0040 |
| SVR | 1294 | 1200 | 0.0464 |
| CO | 5.9 | 6.6 | 0.0049 |
| SV | 66.8 | 67.7 | 0.2182 |
| MAP | 92.2 | 93.4 | 0.6398 |
| SBP | 126 | 127 | 0.9658 |
| DBP | 75 | 76 | 0.6557 |
| Epidural Anesthesia | |||
|---|---|---|---|
| 10 min Prior | 10–20 min after | p-Value | |
| HR | 81.9 | 83.5 | 0.1648 |
| SVR | 1361 | 1317.8 | 0.0240 |
| CO | 5.5 | 5.5 | 0.0854 |
| SV | 66.6 | 66.4 | 0.4080 |
| MAP | 89.4 | 88.3 | 0.5243 |
| SBP | 123.5 | 122.2 | 0.3459 |
| DBP | 72.2 | 71.3 | 0.7622 |
| 10 min Prior | 20–30 min after | p-Value | |
| HR | 81.9 | 81.6 | 0.1913 |
| SVR | 1361 | 1348.2 | 0.4167 |
| CO | 5.5 | 5.3 | 0.1128 |
| SV | 66.6 | 65.7 | 0.8424 |
| MAP | 89.4 | 87.9 | 0.0929 |
| SBP | 123.5 | 121.7 | 0.2257 |
| DBP | 72.2 | 70.9 | 0.0709 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atzmon, Y.; Ben Ishay, E.; Hallak, M.; Littman, R.; Eisenkraft, A.; Gabbay-Benziv, R. Continuous Maternal Hemodynamics Monitoring at Delivery Using a Novel, Noninvasive, Wireless, PPG-Based Sensor. J. Clin. Med. 2021, 10, 8. https://doi.org/10.3390/jcm10010008
Atzmon Y, Ben Ishay E, Hallak M, Littman R, Eisenkraft A, Gabbay-Benziv R. Continuous Maternal Hemodynamics Monitoring at Delivery Using a Novel, Noninvasive, Wireless, PPG-Based Sensor. Journal of Clinical Medicine. 2021; 10(1):8. https://doi.org/10.3390/jcm10010008
Chicago/Turabian StyleAtzmon, Yuval, Efrat Ben Ishay, Mordechai Hallak, Romi Littman, Arik Eisenkraft, and Rinat Gabbay-Benziv. 2021. "Continuous Maternal Hemodynamics Monitoring at Delivery Using a Novel, Noninvasive, Wireless, PPG-Based Sensor" Journal of Clinical Medicine 10, no. 1: 8. https://doi.org/10.3390/jcm10010008