
A Systematic Review of Interventions to Improve HPV Vaccination Coverage

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Studies for This Review
2.2. Search Methods for Identification of Studies
2.3. Selection of Studies
2.4. Data Extraction and Management
2.5. Assessment of Risk of Bias in Included Studies
3. Results
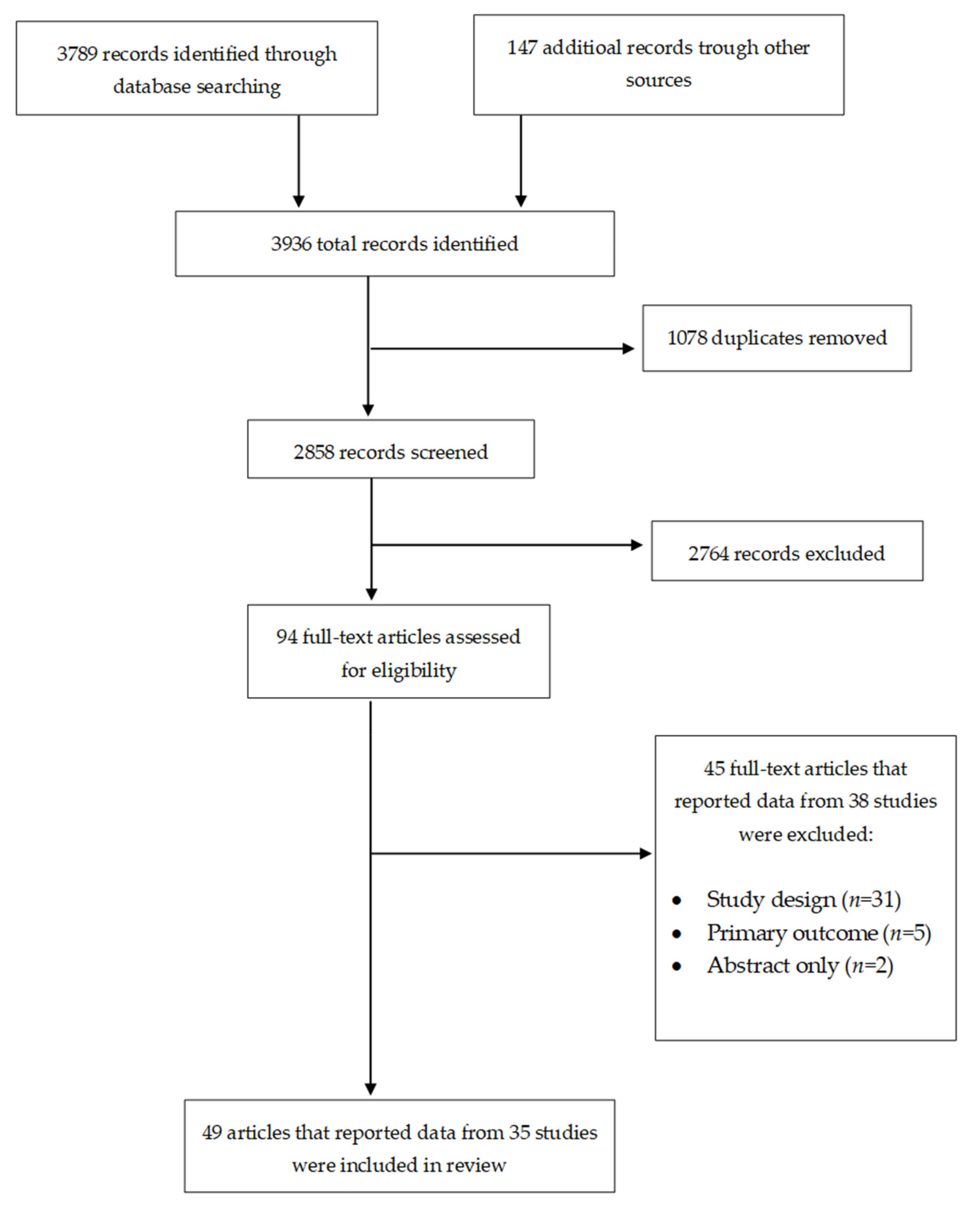
3.1. Results of the Search
3.2. Description of Studies
3.2.1. Study Design and Setting
3.2.2. Participants
3.2.3. Interventions and Comparators
3.2.4. Outcome Measures
3.2.5. Excluded Studies
3.2.6. Risk of Bias in Included Studies
3.3. Effects of Interventions
3.3.1. Recipient-Oriented Interventions
Comparison 1: Tailored Education Compared to Standard of Care
Comparison 2: Tailored Education Compared to Untailored Education
Comparison 3: Narrative Education Compared to Non-Narrative Education
Comparison 4: Multicomponent Education Compared to Standard of Care
Comparison 5: Outreach Plus Reminders Compared to Standard of Care
Comparison 6: Outreach Plus Education Compared to Standard of Care
Comparison 7: Education Plus Reminders Compared to Standard of Care
Comparison 8: Reminders vs. Standard of Care
Comparison 9: Educational Reminders Compared to Plain Reminders
Comparison 10: Financial Incentives Plus Reminders Compared to Standard of Care
Comparison 11: Brief Motivational Behavioral Intervention Compared to Standard of Care
Comparison 12: Brief Health Messaging Using Different Formats
3.3.2. Provider-Oriented Intervention
Comparison 13: Prompts Compared to Standard of Car
Comparison 14: Provider Training Compared to Standard of Care
Comparison 15: Provider Training Plus Assessment and Feedback Compared to Wait List Control
Comparison 16: Assessment and Feedback Compared to Standard of Care Series
Comparison 17: Provider Consultation Compared to Standard of Care
Comparison 18: Funding Compared to Training and Technical Assistance
Comparison 19: Multicomponent Intervention Compared Standard of Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Search | Query | Results |
|---|---|---|
| PubMed | ||
| #1 | Search (“papillomavirus vaccines”(MeSH Terms) OR (“papillomavirus”[All Fields] AND “vaccines”[All Fields]) OR “papillomavirus vaccines”(All Fields) OR (“hpv”[All Fields] AND “vaccine”[All Fields]) OR “hpv vaccine”(All Fields)) AND (VACCINATE[All Fields] OR [“vaccination”[MeSH Terms] OR “vaccination”[All Fields])) | 6876 |
| #2 | Search (randomized controlled trial(pt) OR controlled clinical trial(pt) OR randomized(tiab) OR placebo(tiab) OR “drug therapy”(Subheading) OR randomly(tiab) OR trial(tiab) OR groups(tiab)) NOT (“animals”(MeSH Terms) NOT “humans”(MeSH Terms)) | 3,933,624 |
| #3 | Search (“case-control studies”(MeSH Terms) OR (“case-control”[All Fields] AND “studies”[All Fields]) OR “case-control studies”(All Fields) OR (“case”[All Fields] AND “control”[All Fields] AND “studies”[All Fields]) OR “case control studies”(All Fields)) OR (“cohort studies”[MeSH Terms] OR [“cohort”[All Fields] AND “studies”[All Fields]] OR “cohort studies”(All Fields)) | 2,188,056 |
| #4 | Search (#2 OR #3) | 5,407,771 |
| #5 | Search (#1 AND #4) | 1815 |
| Web of Science | ||
| #1 | Search ((“papillomavirus vaccines” OR [“papillomavirus” AND “vaccines”] OR “papillomavirus vaccines” OR [“hpv” AND “vaccine”] OR “hpv vaccine”) AND (VACCINATE OR [“vaccination” OR “vaccination”])) | 5810 |
| #2 | Search (([randomized controlled trial] OR [controlled clinical trial]) OR ([“case-control studies” OR [“case-control” AND “studies”] OR [“case”AND “control” AND “studies”] OR “case control studies”] OR [“cohort studies” OR [“cohort” AND “studies”]])) | 652,297 |
| #3 | Search (#2 AND #1) | 669 |
| Scopus | ||
| #1 | Search (“papillomavirus vaccines” OR “papillomavirus vaccine” OR “hpv vaccine” OR “HPV vaccines”) | 9447 |
| #2 | Search (“Randomized controlled trial” OR “controlled clinical trial” OR “Randomized Controlled trials” OR “Controlled Clinical trials” OR “case-control studies” OR “Case control studies”) | 1,175,572 |
| #3 | Search (#1 AND #2) | 738 |
| No. | Study Id | Country | Study Type | Sample Size | Participants | Intervention | Comparator | Outcome Measure |
|---|---|---|---|---|---|---|---|---|
| 1 | Bennett (2015) [22] Bennett (2014) [58] NCT01769560 [59] | USA | RCT | 661 | Female students aged 18–26 years | 330 participants were randomized to individually tailored educational website. | 331 participants were randomized to the website of the standard CDC information factsheet on the HPV vaccine. | Initiation and completion of HPV vaccine series |
| 2 | Brewer (2017) [23] NCT02377843 [60] | USA | RCT | 30 | Providers | 10 clinics were randomized to announcement training. Participating clinicians received 1 h of training on announcement to recommend HPV vaccination. 10 clinics were randomized to conservation training. Participating clinicians received 1 h of training on conservation to recommend HPV vaccination. | 10 clinics were randomized to the waitlist control condition. Participating clinics received a video recording of the announcement training, which was sent 1 month after the 6-month assessment of vaccination outcomes. | Initiation of HPV vaccine series |
| 3 | Chao (2015) [24] | USA | RCT | 12,225 | Females aged 9–26 years | 9804 participants were randomized to reminder letter. Participants received a letter reminding them of the HPV vaccination. | 2451 participants were randomized to the standard of care. Participants received no reminder letters. | Completion of HPV vaccine series |
| 4 | Coley (2018) [25] | USA | RCT | 303,965 | Parents of adolescents aged 11–13 years | 151,982 participants were randomized to reminder letter. Parents received letters reminding them to vaccinate their adolescents. | 151,983 participants were randomized to control letters. Participants received letters six months after the observation period was completed. | Initiation and completion of HPV vaccine series Cost of intervention |
| 5 | Dempsey (2019) [26] NCT02145156 [61] | USA | RCT | 1294 | Young adults aged 18–26 years and their parents | 430 participants were randomized to web-based tailored messaging called CHICOs (Combatting HPV Infections and Cancers). Participants received an iPad with the CHICOS intervention programmed onto it. 425 participants were randomized to web-based untailored messaging. Participants received an iPad-based version of the Vaccine Information Sheet from the Centers for Disease Control and Prevention. | 439 participants were randomized to usual care. Participants received care routinely provided by the clinician and did not interact with or have access to the iPad | Receipt of any HPV vaccine dose |
| 6 | DiClemente (2015) [27] NCT00813319 [62] | USA | RCT | 216 | Female adolescents aged 14–18 years | 108 participants were randomized to theory-based, multi-component computer-delivered media-based intervention called Girls OnGuard. Participants viewed a 12-min interactive computer-delivered media presentation on HPV vaccination. | 108 participants were randomized to placebo. Participants viewed a time-equivalent health promotion media presentation on physical activity and nutrition. | Initiation and completion of HPV vaccine series |
| 7 | Fisher-Borne (2018) [30] | USA | RCT | 30 | Providers | 10 participants were randomized to $90,000 2-year grant. 10 participants were randomized to $10,000 3-month grant. | 10 participants were randomized to no funding. Participants received training and technical assistance. | Initiation and completion of HPV vaccine series |
| 8 | Gilkey (2014) [28] | USA | RCT | 91 | Providers Primary care clinics (pediatric and family practice clinics) serving adolescents 11–18 years old. | 30 clinics were randomized to in-person delivered Assessment, Feedback, Incentives, and eXchange (AFIX) consultation. 30 clinics were randomized to webinar-delivered AFIX consultation. | 30 clinics were randomized to no consultation | Initiation of HPV vaccine series |
| 9 | Gilkey (2019) [29] | USA | RCT | 78 | Pediatricians | 43 participants were randomized to quality improvement plus assessment and feedback. | 35 participants were randomized to wait-list control arm. Participants received QI program after 6 months of follow-up. | Initiation of the HPV vaccine series |
| 10 | Henrikson (2018) [31] Henrikson (2017) [63] | USA | RCT | 1805 | Parents of adolescents aged 10–12 years | 1354 participants were randomized to outreach letter, brochure, and reminder. Participants received outreach letter and brochure recommending HPV vaccination followed by automated HPV vaccine reminder call for dose 1. | 451 participants were randomized to usual care. Participants received no outreach letter or reminder call. | Initiation of the HPV vaccine series |
| 11 | Hofstetter (2017) [32] | USA | RCT | 295 | Parents of adolescents with chronic medical conditions | 154 participants were randomized to educational text message reminders. Participants received educational text message reminders on receipt of HPV. | 141 participants were randomized to plaint text message reminders. | Initiation of the HPV vaccine series |
| 12 | Hopfer (2012) [33] | USA | RCT | 404 | College women aged 18–26 years | 252 participants were randomized to narrative messages Participants viewed one of three videos: (1) a video of vaccine decision narratives delivered by peers (101), (2) a video of narratives delivered by medical experts (50), or (3) a video of narratives delivered by a combination of peers and experts (101) | 152 participants were randomized to no narrative messages Participants viewed one of three controls: (1) an informational video without narratives, (2) the campus website providing information about HPV and the vaccine, or (3) no message. | Initiation of the HPV vaccine series |
| 13 | Irving (2018) [54] | USA | BA | 12 | Providers (clinics) | 9 clinics were enrolled in the provider-focused assessment and feedback intervention. | 3 clinics were enrolled in the standard of care. | Initiation and completion of HPV vaccine series |
| 14 | Joseph (2016) [34] NCT01254669 [64] | USA | RCT | 200 | Mothers of daughters aged 11–15 years | 100 participants were randomized to brief negotiated interviewing (BNI).Participants received the BNI intervention, which addressed mothers’ beliefs, values, and concerns about HPV prevention and accounting for their priorities for health and well-being. | 100 participants were randomized to no BNI. Participants received the low literacy, standard-practice HPV vaccine information sheet given to all patients prior to vaccination | Initiation and completion of HPV vaccine series |
| 15 | Lee (2018) [35] | USA | RC | 19 | Mothers and daughters aged 14–17 years dyads | 10 participants were randomized to storytelling narrative videos. The participants watched a 26-min storytelling narrative DVD on HPV vaccine, entitled “Save My Daughter from Cervical Cancer.” | 9 participants were randomized to written non-narrative education materials. Participants received CDC flyers on the HPV vaccine. | Initiation of the HPV vaccine series |
| 16 | Mantzari (2015) [36] | UK | RCT | 1000 | Girls aged 16–18 years | 500 participants were randomized to financial incentives. Participants received the offer of “Love2Shop” vouchers worth £45 for receiving the three vaccinations. | 500 participants were randomized to no financial incentives. Participants received no incentives. | Initiation and completion of HPV vaccine series |
| 17 | Mclean (2017) [55] | USA | BA | 43 | Providers (clinics) | 9 participants were enrolled in the multi-component interventions. Participants received education on HPV vaccination, assessment and feedback, and patient reminder and recall notifications. | 34 participants were enrolled in the standard of care. | Initiation and completion of HPV vaccine series |
| 18 | Parra Medina (2015) [56] | USA | N-RCT | 372 | Hispanic mothers with a daughter aged 11–17 years | 257 participants were enrolled in the outreach and education program called Entre Madre e Hija (EMH), a culturally relevant cervical cancer prevention program. Participants received health education, referral, and navigation support for HPV vaccination. They also received an HPV vaccine educational brochure. | 115 participants were enrolled in the HPV vaccine educational brochure only. | Initiation and completion of HPV vaccine series |
| 19 | Patel (2012) [37] | USA | RCT | 256 | Female college students aged 18-26 years | 128 were randomized to HPV-specific patient education and reminder letter. Participants received HPV and Vaccination” fact sheet plus reminder letter for HPV vaccination. | 128 were randomized to standard of care. Participants did not receive “HPV and Vaccination” fact sheet and reminder letter. | Initiation of the HPV vaccine series |
| 20 | Pot (2017) [38] | The Netherlands | RCT | 806 | Mothers of girls aged 12 years | 3995 participants were randomized to web-based tailored intervention with virtual assistants. Participants received tailored information on HPV and HPV vaccination. | 4067 participants were randomized to standard of care. Participants received universal information about the HPV vaccination | Receipt of any HPV vaccine dose |
| 21 | Rand (2015) [39] | USA | RCT | 3812 | Parents of adolescents aged 11–16 years | 1893 participants were randomized to text message reminders. Parents received text message reminding them that their adolescents were due for HPV vaccine doses. | 1919 participants were randomized to general adolescent health text message. Parents received general adolescent health text message each time their adolescents were due for HPV vaccine dose. | Initiation of the HPV vaccine series |
| 22 | Rand (2017) [40] NCT01731496 [65] | USA | RCT | 749 | Parents of adolescents aged 11–17 years | 178 participants were randomized to telephone message reminder. Parents received telephone call reminding them that their adolescents were due for an HPV vaccine dose.191 participants were randomized to text message reminders. Parents received text message reminding them that their adolescents were due for HPV vaccine dose. | 180 participants were randomized to standard of care (telephone reminder control). 200 participants were randomized to standard of care (text reminder control). | Completion of HPV vaccine series |
| 23 | Reiter (2018) [41] Mcree (2018) [66], NCT01769560 [59] | USA | RCT | 150 | Young gay and bisexual men aged 18–25 years | 76 participants were randomized to outsmart HPV intervention. Participants received population-targeted, individually tailored content about HPV and the HPV vaccine, and monthly HPV vaccination reminders sent via email and/or text message. | 74 participants were randomized to standard HPV information. Participants received standard information about HPV and the HPV vaccine. | Completion of HPV vaccine series |
| 24 | Richman (2019) [42] | USA | RCT | 257 | Parents of adolescences aged 9–17 years. | 129 participants were randomized to electronic messaging (text or email).Participants received appointment reminders and education messages about HPV and the HPV vaccine. | 128 participants were randomized to standard of care. Participants received a paper card with the date of their next appointment written on it. | Completion of HPV vaccine series |
| 25 | Richman (2016) [43] | US | RCT | 264 | College students aged 18–26 years | 130 participants were randomized to electronic messaging (text or email). Participants received appointment reminders and education messages about HPV and the HPV vaccine. In addition, participants received a paper card with the date of their nextappointment written on it. | 134 participants were randomized to standard of care. Participants received a paper card with the date of their next appointment written on it. | Completion of HPV vaccine series |
| 26 | Rickert (2015) [44] | USA | RCT | 445 | Parents of male and female adolescents aged 11–15 years | 109 participants were randomized to rhetorical questions (RQ) plus one-sided message. 114 participants were randomized to RQ plus two-sided message. | 116 participants were randomized to no RQ plus one-sided message. 106 participants were randomized to no RQ plus two-sided message. | Initiation and completion of HPV vaccine series |
| 27 | Suh (2012) [45] | USA | RCT | 1600 | Parents of adolescents aged 11 to 18 years | 800 participants were randomized to letter and telephone reminders. Parents received letter and autodialed telephone call informing them that their adolescents were due for an HPV vaccination. | 800 participants were randomized to usual care. Parents received no reminder/recall | Initiation and completion of HPV vaccine series Cost of intervention |
| 28 | Szilagyi (2015) [46] | USA | RCT | 22 | Providers / Primary care practices attendant by adolescents aged 11–17 years | 11 practices were randomized to provider prompts on HPV vaccination (electronic health record (EHR) or nurse- or staff-initiated prompts).Participants received prompts indicating the specific HPV vaccine doses that the adolescents were due for during their practice visits. | 11 practices were randomized to standard of care. Participants did not receive any prompts. | Completion of HPV vaccine series |
| 29 | Szilagyi (2013) [47] | USA | RCT | 7404 | Parents of adolescents aged 11–17 years | 2494 participants were randomized to letter reminder. Parents received reminder letters advising them to call their adolescent’s primary care practice to schedule an appointment for HPV vaccination. 2504 participants were randomized to telephone reminder. Parents received autodialed reminder calls advising them to call their adolescent’s primary care practice to schedule an appointment for HPV vaccination. | 2406 participants were randomized to standard of care. Parents received no reminder. | Initiation and completion of HPV vaccine series Costs of the intervention |
| 30 | Tiro (2015) [48] | USA | RCT | 814 | Parents and girls/daughters aged 11–18 years dyads | 410 participants were randomized to HPV-vaccine-specific brochure and recalls. Participants received HPV-vaccine-specific brochures and telephone recalls for vaccination. | 404 participants were randomized to general adolescent vaccine brochure. Participants received a CDC brochure about all Advisory Committee on Immunization Practices’ recommended vaccines. | Initiation and completion of HPV vaccine series |
| 31 | Tull (2019) [49] | Australia | RCT | 4386 | Parents of Year 7 students | 1442 participants were randomized to motivational short message service (SMS) Reminders. Participants received a motivational SMS: “Vaccine preventable diseases are still a problem in the community and children most at risk are those that have not been immunized.” 1418 participants were randomized to self-regulatory SMS reminders. Participants received an SMS: “make a plan now for how your child will get to school on-time on immunization day.” | 1526 participants were randomized to no SMS reminders. Participants received no SMS reminders. | Receipt of any HPV vaccine dose |
| 32 | Underwood (2019) [50] Herbert (2014) [67] | USA | RCT | 2135 | Parents and adolescents | 668 participants (parents only) were randomized to educational intervention. Participants received an educational brochure about adolescent vaccines. 690 participants (parents and adolescents) were randomized to multicomponent educational intervention. Participants (parents) received educational brochures about vaccines recommended during adolescence. Participants (adolescents) received a vaccine-focused curriculum delivered by science teachers. | 777 participants were randomized to no intervention. Parents received no information. | Receipt of any HPV vaccine dose |
| 33 | Vanderpool (2013) [51] | USA | RCT | 344 | Young women aged 18–26 years | 178 participants were randomized to an educational DVD, entitled “1-2-3 Pap.” Participants watched a 13-min educational DVD on HPV, HPV vaccines, and pap tests | 166 participants were randomized to Standard of care. | Completion of HPV vaccine series |
| 34 | Wilkinson (2019) [52] Zimet (2016) [68] NCT02558803 [69] | USA | RCT | 29 | Providers (pediatric clinicians) | 15 participants were randomized to automated reminder. Participants received automated reminders via Child Health Improvement through Computer Automation (CHICA) to recommend the 2nd and 3rd doses of HPV vaccine to adolescents aged 11–17 years who had already initiated the vaccine series. | 14 participants were randomized usual practice. Participants received reminders to recommend the 2nd and 3rd doses of HPV vaccine manually from the nurses who looked them up in the Children and Hoosier Immunization Registry Program (CHIRP). | Completion of HPV vaccine series |
| 35 | Zimet (2018) [53] | USA | RCT | 29 | Providers (health care providers) | 8 participants were randomized to simple reminder prompt. Participants received computer-generated messages reminding them of HPV vaccination eligibility. 11 participants were randomized to elaborated reminder prompt. Participants received computer-generated reminders with a suggested script for recommending the three adolescent platform vaccines. | 10 participants were randomized to usual practice. Participants did not receive any reminder prompt. They made HPV vaccination recommendations their existing methods for determining eligibility. | Initiation of the HPV vaccine series |
| Study No. | Study Id. | Reason |
|---|---|---|
| 1 | Chigbu (2017) [70] | A before–after study evaluating the impact of trained community health educators on the uptake of cervical and breast cancer screening and HPV vaccination. The study was excluded because it had one intervention and control group. |
| 2 | Cory (2019) [71] | A randomized study assessing the effects of educational interventions on human papillomavirus vaccine acceptability. Reported outcome was intention to vaccinate. |
| 3 | Daley (2014) [72] | A cluster-randomized controlled study assessing the program costs, the proportion of costs reimbursed, and the likelihood of vaccination in a school-located adolescent vaccination program that billed health insurance. One intervention and control cluster. |
| 4 | Davies (2017) [73] Skinner (2015) [74] | A cluster-randomized controlled study evaluating the effect of educational intervention on HPV vaccination uptake. One intervention and control cluster. |
| 5 | Dempsey (2018) [75] O’Leary (2017) [76] NCT02456077 [77] | A cluster-randomized controlled study evaluating the effect of a health care professional communication training intervention on adolescent human papillomavirus vaccination. One intervention and control cluster. |
| 6 | Deshmukh (2018) [78] | A before–after study evaluating the impact of a clinical intervention bundle on the rate of missed opportunities and uptake of the vaccine among young adult women. One intervention and control group. |
| 7 | Dixon (2019) [79] Dixon (2016) [80] NCT02546752 [81] | A cluster-randomized controlled study assessing the effects an educational intervention in improving HPV vaccination. One intervention and control cluster. |
| 8 | Fiks (2013) [82] | A cluster-randomized controlled study evaluating the effectiveness of decision support for families, clinicians, or both on HPV vaccine receipt. One intervention and control cluster. |
| 9 | Fiks (2016) [83] | A before–after study evaluating the impact of Maintenance-of-Certification program on improving HPV vaccination rates. One intervention and control group. |
| 10 | Forster (2017) [84] | A cluster-randomized controlled study evaluating the effect of an adolescent incentive intervention on improving HPV vaccination uptake. One intervention and control cluster. |
| 11 | Grandahl (2016) [85] | A cluster-randomized controlled study assessing the effect of the educational intervention on increasing HPV vaccination among adolescents. One intervention and control cluster. |
| 12 | Jacobs-Wingo (2017) [86] | A cross-sectional study assessing the impact of multi-component interventions on increasing HPV vaccine coverage. |
| 13 | Jiménez-Quiñones (2017) [87] | A descriptive study assessing the impact of a pharmacist administered educational program on the vaccination rates of HPV. A descriptive study. |
| 14 | Keeshin (2017) [88] | A prospective cohort study evaluating the impact of text message reminder recall on increasing HPV vaccination in young HIV-1-infected patients. A prospective study. |
| 15 | Kempe (2012) [89] | A demonstration study assessing the effectiveness and cost of immunization recall at school-based health centers. A demonstration study. |
| 16 | Kim (2018) [90] | Conference abstract only |
| 17 | Lee (2016) [91] | A before–after study evaluating the effect of the text messaging intervention on HPV vaccination among Korean-American women. One intervention group. |
| 18 | Mayne (2014) [92] | A cluster-randomized controlled study evaluating the effect of decision support on HPV vaccination. One intervention and control cluster |
| 19 | Mehta (2013) [93] | A randomized-controlled study evaluating a health-belief-model-based intervention to increase vaccination rates in college men. The reported outcome was intention to vaccinate. |
| 10 | O’Leary (2019) [94] | A cluster-randomized controlled study assessing the effectiveness of a multimodal intervention in obstetrics/gynecology clinics in increasing vaccination uptake. One intervention and control cluster. |
| 21 | Patel (2014) [95] NCT01343485 [96] | A cluster-randomized control study evaluating the impact of an automated reminders in increasing on-time completion of the three-dose HPV vaccine series. One intervention and control cluster. |
| 22 | Perez (2016) [2] | A randomized controlled study evaluating the effect of an information–motivation–behavioral skills (IMB) intervention in increasing HPV vaccination knowledge, motivation, and intentions among college-aged women. Reported outcome was intentions to vaccinate |
| 23 | Perkins (2015) [97] | A before–after study assessing the effectiveness of a provider-focused intervention in improving HPV vaccination rates in boys and girls. One intervention group and control group. |
| 24 | Rahman (2013) [98] | A cross-sectional study evaluating the impact of attending a well-woman clinic on HPV vaccine intent and uptake among both their sons and daughters. A cross-sectional study. |
| 25 | Rickert (2014) [99] | A before–after study assessing the impact of health beliefs on intent and first dose uptake of HPV vaccine among young adolescent males. One intervention and control cluster. |
| 26 | Roblin (2014) [100] | An observational study evaluating the influence of deductible health plans on receipt of the human papillomavirus vaccine series. An observational study. |
| 27 | Ruffin (2015) [101] | A retrospective study assessing the impact of electronic health record reminder on HPV vaccine initiation and timely completion among female patients. A retrospective study. |
| 28 | Russel (2012) [102] | A randomized controlled study assessing the effectiveness of text message reminders in improving vaccination appointment attendance and series completion among adolescents and adults. Abstract only. |
| 29 | Sanderson (2017) [103] NCT02808832 [104] | A cluster-randomized controlled study evaluating the effectiveness of provider-focused and patient-focused intervention strategies in increasing HPV vaccination. One intervention and control cluster. |
| 30 | Spleen (2012) [105] | A before–after study evaluating the impact of theory and community-based educational intervention on increasing parents’ HPV-related knowledge and parental intent to vaccinate their daughters against HPV. One intervention and control group. |
| 31 | Valdez (2015) [106] | A randomized controlled trial evaluating the effects of HPV vaccine education intervention on promoting informed decision-making about HPV vaccination among parents. Reported outcome were intentions to vaccinate |
| 32 | Whadera (2015) [107] | A prospective study assessing the effect of HPV educational intervention on HPV knowledge, vaccine acceptance, and vaccine series completion among female entertainment and sex workers. A prospective study. |
| 33 | Wedel (2016) [108] | A before–after study evaluating the effect of HPV educational intervention on increasing HPV vaccinations among military women. Not a controlled before and after study. |
| 34 | Wegwart (2014) [109] | A before–after study evaluating the effect of evidence-based HPV vaccination leaflets on understanding, intention, and actual vaccination decision. One intervention and control group |
| 35 | Whelan (2014) [110] | A retrospective study examining the relationship between school-based strategies and uptake of HPV vaccine. A retrospective study. |
| 36 | Winer (2016) [111] | A cluster-randomized controlled study evaluating the impact of an educational intervention on increasing HPV vaccination coverage in American Indian girls. One intervention and control cluster. |
| 37 | Zimmerman (2017) [112] | A before–after study evaluating the effect of the 4 Pillars™ Practice Transformation Program on improving adolescent HPV vaccination. One intervention and control group. |
| 38 | Zimmerman (2017) [113] | A cluster-randomized controlled study evaluating the effect of the 4 Pillars™ Practice Transformation Program on improving adolescent HPV vaccination. One intervention and control cluster. |
| Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | |
|---|---|---|---|---|---|---|---|
| Bennett (2015) [22] |  | | |  |  | | |
| Brewer (2017) [23] | | | | | | | |
| Chao (2015) [24] | | | | | | | |
| Coley (2018) [25] | | | | | | | |
| Dempsey (2019b) [26] | | | | | | | |
| DiClemente (2015) [27] | | | | | | | |
| Fisher-Borne (2018) [30] | | | | | | | |
| Gilkey (2014) [28] | | | | | | | |
| Gilkey (2019) [29] | | | | | | | |
| Henrikson (2018) [31] | | | | | | | |
| Hofstetter (2017) [32] | | | | | | | |
| Hopfer (2012) [33] | | | | | | | |
| Irving (2018) [54] | | | | | | | |
| Joseph (2016) [34] | | | | | | | |
| Lee (2018) [35] | | | | | | | |
| Mantzari (2015) [36] | | | | | | | |
| Mclean (2017) [55] | | | | | | | |
| Parra-Medina (2015) [56] | | | | | | | |
| Patel (2012) [37] | | | | | | | |
| Pot (2017) [38] | | | | | | | |
| Rand (2015) [39] | | | | | | | |
| Rand (2017) [40] | | | | | | | |
| Reiter (2018) [41] | | | | | | | |
| Richman (2019) [42] | | | | | | | |
| Richman (2016) [43] | | | | | | | |
| Rickert (2015) [44] | | | | | | | |
| Suh (2012) [45] | | | | | | | |
| Szilagyi (2015) [46] | | | | | | | |
| Szilagyi (2013) [47] | | | | | | | |
| Tiro (2015) [48] | | | | | | | |
| Tull (2019) [49] | | | | | | | |
| Underwood (2019) [50] | | | | | | | |
| Vanderpool (2013) [51] | | | | | | | |
| Wilkinson (2019) [52] | | | | | | | |
| Zimet (2018) [53] | | | | | | | |
References
- Loke, A.Y.; Kwan, M.L.; Wong, Y.-T.; Wong, A.K.Y. The Uptake of Human Papillomavirus Vaccination and Its Associated Factors Among Adolescents: A Systematic Review. J. Prim. Care Community Health 2017, 8, 349–362. [Google Scholar] [CrossRef]
- Perez, G.K.; Cruess, D.G.; Strauss, N.M. A brief information–motivation–behavioral skills intervention to promote human papillomavirus vaccination among college-aged women. Psychol. Res. Behav. Manag. 2016, 9, 285–296. [Google Scholar] [CrossRef] [Green Version]
- Fontes, A.; Andreoli, M.A.; Villa, L.L.; Assone, T.; Gaester, K.; Fonseca, L.A.; Duarte, A.J.; Casseb, J. High specific immune response to a bivalent anti-HPV vaccine in HIV-1-infected men in São Paulo, Brazil. Papillomavirus Res. 2016, 2, 17–20. [Google Scholar] [CrossRef] [Green Version]
- Holman, D.M.; Benard, V.; Roland, K.; Watson, M.; Liddon, N.; Stockley, S. Barriers to human papillomavirus vaccination among US adolescents: A systematic review of the literature. JAMA Pediatr. 2014, 168, 76–82. [Google Scholar] [CrossRef] [Green Version]
- Lu, P.-J.; Yankey, D.; Jeyarajah, J.; O’Halloran, A.; Elam-Evans, L.D.; Smith, P.J.; Stokley, S.; Singleton, J.A.; Dunne, E.F. HPV Vaccination Coverage of Male Adolescents in the United States. Pediatrics 2015, 136, 839–849. [Google Scholar] [CrossRef] [Green Version]
- Niccolai, M.L.; Hansen, C.E. Practice- and Community-Based Interventions to Increase Human Papillomavirus Vaccine Coverage: A Systematic Review. JAMA Pediatr. 2015, 169, 686–692. [Google Scholar] [CrossRef] [Green Version]
- Egawa, N.; Doorbar, J. The low-risk papillomaviruses. Virus Res. 2017, 231, 119–127. [Google Scholar] [CrossRef]
- Globocan. Available online: https://gco.iarc.fr (accessed on 30 March 2021).
- Chabeda, A.; Yanez, R.J.; Lamprecht, R.; Meyers, A.E.; Rybicki, E.P.; Hitzeroth, I.I. Therapeutic vaccines for high-risk HPV-associated diseases. Papillomavirus Res. 2018, 5, 46–58. [Google Scholar] [CrossRef]
- Gallagher, K.E.; Howard, N.; Kabakama, S.; Mounier-Jack, S.; Burchett, H.E.D.; Lamontagne, D.S.; Watson-Jones, D. Human papillomavirus (HPV) vaccine coverage achievements in low and middle-income countries 2007–2016. Papillomavirus Res. 2017, 4, 72–78. [Google Scholar] [CrossRef]
- Carney, P.A.; Hatch, B.; Stock, I.; Dickinson, C.; Davis, M.; Larsen, R.; Valenzuela, S.; Marino, M.; Darden, P.M.; Gunn, R.; et al. A stepped-wedge cluster randomized trial designed to improve completion of HPV vaccine series and reduce missed opportunities to vaccinate in rural primary care practices. Implement. Sci. 2019, 14, 30. [Google Scholar] [CrossRef]
- Brandt, H.M.; Pierce, J.Y.; Crary, A. Increasing HPV vaccination through policy for public health benefit. Hum. Vaccines Immunother. 2015, 12, 1623–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acampora, A.; Grossi, A.; Barbara, A.; Colamesta, V.; Causio, F.A.; Calabrò, G.E.; Boccia, S.; De Waure, C. Increasing HPV Vaccination Uptake among Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 7997. [Google Scholar] [CrossRef] [PubMed]
- Barnard, M.; Cole, A.C.; Ward, L.; Gravlee, E.; Cole, M.L.; Compretta, C. Interventions to increase uptake of the human papillomavirus vaccine in unvaccinated college students: A systematic literature review. Prev. Med. Rep. 2019, 14, 100884. [Google Scholar] [CrossRef] [PubMed]
- Walling, E.B.; Benzoni, N.; Dornfeld, J.; Bhandari, R.; Sisk, B.A.; Garbutt, J.; Colditz, G. Interventions to Improve HPV Vaccine Uptake: A Systematic Review. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francis, D.B.; Cates, J.R.; Wagner, K.P.G.; Zola, T.; Fitter, J.E.; Coyne-Beasley, T. Communication technologies to improve HPV vaccination initiation and completion: A systematic review. Patient Educ. Couns. 2017, 100, 1280–1286. [Google Scholar] [CrossRef]
- Smulian, E.A.; Mitchell, K.R.; Stokley, S. Interventions to increase HPV vaccination coverage: A systematic review. Hum. Vaccines Immunother. 2016, 12, 1566–1588. [Google Scholar] [CrossRef]
- PROSPERO. Available online: https://www.crd.york.ac.uk/prospero/ (accessed on 30 March 2021).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Cochrane Effective Practice and Organisation of Care. EPOC Resources for Review Authors. Available online: https://epoc.cochrane.org/resources/epoc-resources-review-authors/ (accessed on 20 March 2021).
- Higgins, J.; Altman, D.; Sterne, J. Assessing Risk of Bias in Included Studies. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 Updated March, 2011; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Bennett, A.T.; Patel, D.A.; Carlos, R.C.; Zochowski, M.K.; Pennewell, S.M.; Chi, A.M.; Dalton, V.K. Human Papillomavirus Vaccine Uptake after a Tailored, Online Educational Intervention for Female University Students: A Randomized Controlled Trial. J. Women Health 2015, 24, 950–957. [Google Scholar] [CrossRef] [Green Version]
- Brewer, N.T.; Hall, M.E.; Malo, T.L.; Gilkey, M.B.; Quinn, B.; Lathren, C. Announcements Versus Conversations to Improve HPV Vaccination Coverage: A Randomized Trial. Pediatrics 2016, 139, e20161764. [Google Scholar] [CrossRef] [Green Version]
- Chao, C.; Preciado, M.; Slezak, J.; Xu, L. A Randomized Intervention of Reminder Letter for Human Papillomavirus Vaccine Series Completion. J. Adolesc. Health 2015, 56, 85–90. [Google Scholar] [CrossRef]
- Coley, S.; Hoefer, D.; Rausch-Phung, E. A population-based reminder intervention to improve human papillomavirus vaccination rates among adolescents at routine vaccination age. Vaccine 2018, 36, 4904–4909. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, A.F.; Maertens, J.; Sevick, C.; Jimenez-Zambrano, A.; Juarez-Colunga, E. A randomized, controlled, pragmatic trial of an iPad-based, tailored messaging intervention to increase human papillomavirus vaccination among Latinos. Hum. Vaccines Immunother. 2019, 15, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- DiClemente, R.J.; Murray, C.C.; Graham, T.; Still, J. Overcoming barriers to HPV vaccination: A randomized clinical trial of a culturally-tailored, media intervention among African American girls. Hum. Vaccines Immunother. 2015, 11, 2883–2894. [Google Scholar] [CrossRef]
- Gilkey, M.B.; Dayton, A.M.; Moss, J.L.; Sparks, A.C.; Grimshaw, A.H.; Bowling, J.M.; Brewer, N.T. Increasing Provision of Adolescent Vaccines in Primary Care: A Randomized Controlled Trial. Pediatrics 2014, 134, e346–e353. [Google Scholar] [CrossRef] [Green Version]
- Gilkey, M.B.; Parks, M.J.; Margolis, M.A.; McRee, A.-L.; Terk, J.V. Implementing Evidence-Based Strategies to Improve HPV Vaccine Delivery. Pediatrics 2019, 144, e20182500. [Google Scholar] [CrossRef] [PubMed]
- Fisher-Borne, M.; Preiss, A.J.; Black, M.; Roberts, K.; Saslow, D. Early Outcomes of a Multilevel Human Papillomavirus Vaccination Pilot Intervention in Federally Qualified Health Centers. Acad. Pediatr. 2018, 18, S79–S84. [Google Scholar] [CrossRef] [Green Version]
- Henrikson, N.B.; Zhu, W.; Baba, L.; Nguyen, M.; Berthoud, H.; Gundersen, G.; Hofstetter, A.M. Outreach and Reminders to Improve Human Papillomavirus Vaccination in an Integrated Primary Care System. Clin. Pediatr. 2018, 57, 1523–1531. [Google Scholar] [CrossRef]
- Hofstetter, A.M.; Barrett, A.; Camargo, S.; Rosenthal, S.L.; Stockwell, M.S. Text message reminders for vaccination of adolescents with chronic medical conditions: A randomized clinical trial. Vaccine 2017, 35, 4554–4560. [Google Scholar] [CrossRef]
- Hopfer, S. Effects of a Narrative HPV Vaccination Intervention Aimed at Reaching College Women: A Randomized Controlled Trial. Prev. Sci. 2011, 13, 173–182. [Google Scholar] [CrossRef]
- Joseph, N.P.; Bernstein, J.; Pelton, S.; Goff, G.; Horanieh, N.; Freund, K.M. Brief Client-Centered Motivational and Behavioral Intervention to Promote HPV Vaccination in a Hard-to-Reach Population: A Pilot Randomized Controlled Trial. Clin. Pediatr. 2016, 55, 851–859. [Google Scholar] [CrossRef]
- Lee, H.; Kim, M.; Cooley, M.E.; Kiang, P.N.-C.; Kim, D.; Tang, S.; Shi, L.; Thiem, L.; Kan, P.; Peou, S.; et al. Using narrative intervention for HPV vaccine behavior change among Khmer mothers and daughters: A pilot RCT to examine feasibility, acceptability, and preliminary effectiveness. Appl. Nurs. Res. 2018, 40, 51–60. [Google Scholar] [CrossRef]
- Mantzari, E.; Vogt, F.; Marteau, T.M. Financial incentives for increasing uptake of HPV vaccinations: A randomized controlled trial. Health Psychol. 2015, 34, 160–171. [Google Scholar] [CrossRef]
- Patel, D.A.; Zochowski, M.; Peterman, S.; Dempsey, A.F.; Ernst, S.; Dalton, V.K. Human Papillomavirus Vaccine Intent and Uptake Among Female College Students. J. Am. Coll. Health 2012, 60, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Pot, M.; Paulussen, T.G.; Ruiter, R.A.; Eekhout, I.; De Melker, H.E.; Spoelstra, M.E.; Van Keulen, H.M.; Grandahl, M.; Glanz, J.; Bragazzi, N. Effectiveness of a Web-Based Tailored Intervention With Virtual Assistants Promoting the Acceptability of HPV Vaccination Among Mothers of Invited Girls: Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, e312. [Google Scholar] [CrossRef] [Green Version]
- Rand, C.M.; Brill, H.; Albertin, C.; Humiston, S.G.; Schaffer, S.; Shone, L.P.; Blumkin, A.K.; Szilagyi, P.G. Effectiveness of Centralized Text Message Reminders on Human Papillomavirus Immunization Coverage for Publicly Insured Adolescents. J. Adolesc. Health 2015, 56, S17–S20. [Google Scholar] [CrossRef] [PubMed]
- Rand, C.M.; Vincelli, P.; Goldstein, N.P.; Blumkin, A.; Szilagyi, P.G. Effects of Phone and Text Message Reminders on Completion of the Human Papillomavirus Vaccine Series. J. Adolesc. Health 2017, 60, 113–119. [Google Scholar] [CrossRef]
- Reiter, P.L.; Katz, M.L.; Bauermeister, J.A.; Shoben, A.B.; Paskett, E.D.; McRee, A.-L. Increasing Human Papillomavirus Vaccination Among Young Gay and Bisexual Men: A Randomized Pilot Trial of the Outsmart HPV Intervention. LGBT Health 2018, 5, 325–329. [Google Scholar] [CrossRef]
- Richman, A.R.; Torres, E.; Wu, Q.; Carlston, L.; O’Rorke, S.; Moreno, C.; Olsson, J. Text and Email Messaging for Increasing Human Papillomavirus Vaccine Completion among Uninsured or Medicaid-insured Adolescents in Rural Eastern North Carolina. J. Health Care Poor Underserved 2019, 30, 1499–1517. [Google Scholar] [CrossRef] [PubMed]
- Richman, A.R.; Maddy, L.; Torres, E.; Goldberg, E.J. A randomized intervention study to evaluate whether electronic messaging can increase human papillomavirus vaccine completion and knowledge among college students. J. Am. Coll. Health 2016, 64, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Rickert, V.I.; Auslander, B.; Cox, D.S.; Rosenthal, S.L.; Rupp, R.E.; Zimet, G.D. School-based HPV immunization of young adolescents: Effects of two brief health interventions. Hum. Vaccines Immunother. 2015, 11, 315–321. [Google Scholar] [CrossRef] [Green Version]
- Suh, C.A.; Saville, A.; Daley, M.F.; Glazner, J.E.; Barrow, J.; Stokley, S.; Dong, F.; Beaty, B.; Dickinson, L.M.; Kempe, A. Effectiveness and Net Cost of Reminder/Recall for Adolescent Immunizations. Pediatrics 2012, 129, e1437–e1445. [Google Scholar] [CrossRef] [Green Version]
- Szilagyi, P.G.; Serwint, J.R.; Humiston, S.G.; Rand, C.M.; Schaffer, S.; Vincelli, P.; Dhepyasuwan, N.; Blumkin, A.; Albertin, C.; Curtis, C.R. Effect of Provider Prompts on Adolescent Immunization Rates: A Randomized Trial. Acad. Pediatr. 2015, 15, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Szilagyi, P.G.; Albertin, C.; Humiston, S.G.; Rand, C.M.; Schaffer, S.; Brill, H.; Stankaitis, J.; Yoo, B.-K.; Blumkin, A.; Stokley, S. A Randomized Trial of the Effect of Centralized Reminder/Recall on Immunizations and Preventive Care Visits for Adolescents. Acad. Pediatr. 2013, 13, 204–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiro, J.A.; Sanders, J.M.; Pruitt, S.L.; Stevens, C.F.; Skinner, C.S.; Bishop, W.P.; Fuller, S.; Persaud, D. Promoting HPV Vaccination in Safety-Net Clinics: A Randomized Trial. Pediatrics 2015, 136, 850–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tull, F.; Borg, K.; Knott, C.; Beasley, M.; Halliday, J.; Faulkner, N.; Sutton, K.; Bragge, P. Short Message Service Reminders to Parents for Increasing Adolescent Human Papillomavirus Vaccination Rates in a Secondary School Vaccine Program: A Randomized Control Trial. J. Adolesc. Health 2019, 65, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Underwood, N.L.; Gargano, L.M.; Sales, J.; Vogt, T.M.; Seib, K.; Hughes, J.M. Evaluation of Educational Interventions to Enhance Adolescent Specific Vaccination Coverage. J. Sch. Health 2019, 89, 603–611. [Google Scholar] [CrossRef]
- Vanderpool, R.C.; Cohen, E.L.; Crosby, R.A.; Jones, M.G.; Bates, W.; Casey, B.R.; Collins, T. “1-2-3 Pap” Intervention Improves HPV Vaccine Series Completion Among Appalachian Women. J. Commun. 2013, 63, 95–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, T.A.; Dixon, B.E.; Xiao, S.; Tu, W.; Lindsay, B.; Sheley, M.; Dugan, T.; Church, A.; Downs, S.M.; Zimet, G. Physician clinical decision support system prompts and administration of subsequent doses of HPV vaccine: A randomized clinical trial. Vaccine 2019, 37, 4414–4418. [Google Scholar] [CrossRef]
- Zimet, G.; Dixon, B.E.; Xiao, S.; Tu, W.; Kulkarni, A.; Dugan, T.; Sheley, M.; Downs, S.M. Simple and Elaborated Clinician Reminder Prompts for Human Papillomavirus Vaccination: A Randomized Clinical Trial. Acad. Pediatr. 2018, 18, S66–S71. [Google Scholar] [CrossRef] [Green Version]
- Irving, S.A.; Groom, H.C.; Stokley, S.; McNeil, M.M.; Gee, J.; Smith, N.; Naleway, A.L. Human Papillomavirus Vaccine Coverage and Prevalence of Missed Opportunities for Vaccination in an Integrated Healthcare System. Acad. Pediatr. 2018, 18, S85–S92. [Google Scholar] [CrossRef] [Green Version]
- McLean, H.Q.; VanWormer, J.J.; Chow, B.D.W.; Birchmeier, B.; Vickers, E.; Devries, E.; Meyer, J.; Moore, J.; McNeil, M.M.; Stokley, S.; et al. Improving Human Papillomavirus Vaccine Use in an Integrated Health System: Impact of a Provider and Staff Intervention. J. Adolesc. Health 2017, 61, 252–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parra-Medina, D.; Morales-Campos, D.Y.; Mojica, C.; Ramirez, A.G. Promotora Outreach, Education and Navigation Support for HPV Vaccination to Hispanic Women with Unvaccinated Daughters. J. Cancer Educ. 2015, 30, 353–359. [Google Scholar] [CrossRef]
- Odone, A.; Ferrari, A.; Spagnoli, F.; Visciarelli, S.; Shefer, A.; Pasquarella, C.; Signorelli, C. Effectiveness of interventions that apply new media to improve vaccine uptake and vaccine coverage: A systematic review. Hum. Vaccines Immunother. 2015, 11, 72–82. [Google Scholar] [CrossRef] [Green Version]
- Bennett, A. Use of “mefirst,” a tailored, online educational intervention to promote HPV vaccination among female university students. J. Women Health 2014, 23, 22. [Google Scholar]
- MeFirst: A Tailored Intervention to HPV Vaccine Decision Making. Available online: https://clinicaltrials.gov/ct2/show/NCT01769560/ (accessed on 30 March 2021).
- Making Effective Human Papillomavirus (HPV) Vaccine Recommendations. Available online: https://clinicaltrials.gov/ct2/show/NCT02377843/ (accessed on 30 March 2021).
- Educational Intervention to Minimize Disparities in Humanpapillomavirus Vaccination (HPV). Available online: https://clinicaltrials.gov/ct2/show/NCT02145156/ (accessed on 30 March 2021).
- Girls OnGuard: HPV Vaccination Uptake Among African American Adolescent Females (Girls OnGuard). Available online: https://www.clinicaltrials.gov/ct2/show/study/NCT00813319/ (accessed on 30 March 2021).
- Henrikson, N.; Zhu, W.; Nguyen, M.; Baba, L.; Berthoud, H.; Hofstetter, A. Health System-Based HPV Vaccine Reminders: Randomized Trial Results. Cancer Epidemiol. Biomark. Prev. 2017, 26, 435. [Google Scholar] [CrossRef] [Green Version]
- An Intervention Study To Improve Human PapillomaVirus ( HPV) Immunization in Haitian and African American Girls (HPV). Available online: https://clinicaltrials.gov/ct2/show/NCT01254669/ (accessed on 30 March 2021).
- The Efficacy of Reminders to Complete HPV Series (ICHAT). Available online: https://clinicaltrials.gov/ct2/show/NCT01731496/ (accessed on 30 March 2021).
- McRee, A.-L.; Shoben, A.; Bauermeister, J.A.; Katz, M.L.; Paskett, E.D.; Reiter, P.L. Outsmart HPV: Acceptability and short-term effects of a web-based HPV vaccination intervention for young adult gay and bisexual men. Vaccine 2018, 36, 8158–8164. [Google Scholar] [CrossRef]
- Herbert, N. Parental Attitudes and Beliefs About Human Papillomavirus (HPV) Vaccination and Vaccine Receipt Among Adolescents in Richmond County, Georgia. J. Adolesc. Health 2014, 54, S82. [Google Scholar] [CrossRef]
- Zimet, G.; Dixon, B.; Xiao, S.; Tu, W.; Lindsay, B.; Sheley, M.; Downs, S.; Dugan, T.; Church, A. Can automated physician reminders increase 2nd and 3rd dose administration of HPV vaccine? Sex. Transm. Dis. 2016, 43, S158. [Google Scholar]
- HPV Vaccination: Evaluation of Reminder Prompts for Doses 2 & 3. Available online: https://clinicaltrials.gov/ct2/show/NCT02558803/ (accessed on 30 March 2021).
- Chigbu, C.O.; Onyebuchi, A.K.; Onyeka, T.C.; Odugu, B.U.; Dim, C.C. The impact of community health educators on uptake of cervical and breast cancer prevention services in Nigeria. Int. J. Gynecol. Obstet. 2017, 137, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Cory, L.; Cha, B.; Ellenberg, S.; Borger, H.; Hwuang, W.-T.; Smith, J.; Haggerty, A.; Morgan, M.; Burger, R.; Chu, C.; et al. Effects of Educational Interventions on Human Papillomavirus Vaccine Acceptability: A Randomized Controlled Trial. Obstet. Gynecol. 2019, 134, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Daley, M.F.; Kempe, A.; Pyrzanowski, J.; Vogt, T.M.; Dickinson, L.M.; Kile, D.; Fang, H.; Rinehart, D.J.; Shlay, J.C. School-Located Vaccination of Adolescents With Insurance Billing: Cost, Reimbursement, and Vaccination Outcomes. J. Adolesc. Health 2014, 54, 282–288. [Google Scholar] [CrossRef]
- Davies, C.; Skinner, S.R.; Stoney, T.; Marshall, H.S.; Collins, J.; Jones, J.; Hutton, H.; Parrella, A.; Cooper, S.; McGeechan, K.; et al. ‘Is it like one of those infectious kind of things?’ The importance of educating young people about HPV and HPV vaccination at school. Sex Educ. 2017, 17, 256–275. [Google Scholar] [CrossRef]
- Skinner, S.R.; Davies, C.; Cooper, S.; Stoney, T.; Marshall, H.; Jones, J.; Collins, J.; Hutton, H.; Parrella, A.; Zimet, G.; et al. HPV.edu study protocol: A cluster randomised controlled evaluation of education, decisional support and logistical strategies in school-based human papillomavirus (HPV) vaccination of adolescents. BMC Public Health 2015, 15, 896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dempsey, A.F.; Pyrznawoski, J.; Lockhart, S.; Barnard, J.; Campagna, E.J.; Garret, K.; Fisher, A.; Dickinson, L.M.; O’Leary, S.T. Effect of a Health Care Professional Communication Training Intervention on Adolescent Human Papillomavirus Vaccination: A Cluster Randomized Clinical Trial. JAMA Pediatr. 2018, 172, e180016. [Google Scholar] [CrossRef]
- O’Leary, S.; Pyrzanowski, M.J.; Lockhart, B.S.; Barnard, M.J.; Campagna, M.E.; Garrett, M.K.; Fisher, M.A.; Dickinson, M.; Dempsey, A. Impact of a Provider Communication Training Intervention on Adolescent Human Papillomavirus Vaccination: A Cluster Randomized, Clinical Trial. Open Forum Infect. Dis. 2017, 4, S61. [Google Scholar] [CrossRef] [Green Version]
- Strengthening Physician Communication About HPV Vaccines. Available online: https://clinicaltrials.gov/ct2/show/NCT02456077/ (accessed on 30 March 2021).
- Deshmukh, U.; Oliveira, C.R.; Griggs, S.; Coleman, E.; Avni-Singer, L.; Pathy, S.; Shapiro, E.D.; Sheth, S.S. Impact of a clinical interventions bundle on uptake of HPV vaccine at an OB/GYN clinic. Vaccine 2018, 36, 3599–3605. [Google Scholar] [CrossRef]
- Dixon, B.E.; Zimet, G.D.; Xiao, S.; Tu, W.; Lindsay, B.; Church, A.; Downs, S.M. An Educational Intervention to Improve HPV Vaccination: A Cluster Randomized Trial. Pediatrics 2019, 143, e20181457. [Google Scholar] [CrossRef] [Green Version]
- Dixon, B.; Downs, S.; Zhang, Z.; Tu, W.; Lindsay, B.; Dugan, T.; Zimet, G. A mhealth intervention trial to improve HPV vaccination rates in urban primary care clinics. Sex. Transm. Dis. 2016, 43, S199. [Google Scholar]
- Use of a Patient Education/Messaging Platform to Increase Uptake and Series Completion of the HPV Vaccine. Available online: https://clinicaltrials.gov/ct2/show/NCT02546752/ (accessed on 30 March 2021).
- Fiks, A.G.; Grundmeier, R.W.; Mayne, S.; Song, L.; Feemster, K.; Karavite, D.; Hughes, C.C.; Massey, J.; Keren, R.; Bell, L.M.; et al. Effectiveness of Decision Support for Families, Clinicians, or Both on HPV Vaccine Receipt. Pediatrics 2013, 131, 1114–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiks, A.G.; Luan, X.; Mayne, S.L. Improving HPV Vaccination Rates Using Maintenance-of-Certification Requirements. Pediatrics 2016, 137, e20150675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forster, A.S.; Cornelius, V.; Rockliffe, L.; Marlow, L.A.; Bedford, H.; Waller, J. A cluster randomised feasibility study of an adolescent incentive intervention to increase uptake of HPV vaccination. Br. J. Cancer 2017, 117, 1121–1127. [Google Scholar] [CrossRef] [Green Version]
- Grandahl, M.; Rosenblad, A.; Stenhammar, C.; Tydén, T.; Westerling, R.; Larsson, M.; Oscarsson, M.; Andrae, B.; Dalianis, T.; Nevéus, T. School-based intervention for the prevention of HPV among adolescents: A cluster randomised controlled study. BMJ Open 2016, 6, e009875. [Google Scholar] [CrossRef]
- Jacobs-Wingo, J.L.; Jim, C.C.; Groom, A.V. Human Papillomavirus Vaccine Uptake: Increase for American Indian Adolescents, 2013–2015. Am. J. Prev. Med. 2017. [Google Scholar] [CrossRef]
- Jiménez-Quiñones, E.M.; Melin, K.; Jiménez-Ramírez, F.J. Impact of a Pharmacist Conducted Educational Program on Human Papilloma Virus Vaccination Rates in a Low Socioeconomic Population in the City of Lares, PR. P. R. Health Sci. J. 2017, 36, 67–70. [Google Scholar] [PubMed]
- Keeshin, S.W.; Feinberg, J. Text Message Reminder–Recall to Increase HPV Immunization in Young HIV-1-Infected Patients. J. Int. Assoc. Provid. AIDS Care 2017, 16, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Kempe, A.; Barrow, J.; Stokley, S.; Saville, A.; Glazner, J.E.; Suh, C.; Federico, S.; Abrams, L.; Seewald, L.; Beaty, B.; et al. Effectiveness and Cost of Immunization Recall at School-Based Health Centers. Pediatrics 2012, 129, e1446–e1452. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.; Lee, H.; Aronowitz, T.; Sheldon, L.K.; Kiang, P.; Allison, J.; Shi, L. Abstract C56: An online-based storytelling video intervention on promoting Korean American female college students’ HPV vaccine uptake. Cancer Epidemiol. Biomark. Prev. 2018, 27, C56. [Google Scholar] [CrossRef]
- Lee, H.Y.; Koopmeiners, J.S.; McHugh, J.; Raveis, V.H.; Ahluwalia, J.S. mHealth Pilot Study: Text Messaging Intervention to Promote HPV Vaccination. Am. J. Health Behav. 2016, 40, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Mayne, S.L.; Durivage, N.E.; Feemster, K.A.; Localio, A.R.; Grundmeier, R.W.; Fiks, A.G. Effect of Decision Support on Missed Opportunities for Human Papillomavirus Vaccination. Am. J. Prev. Med. 2014, 47, 734–744. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; Lee, R.C.; Sharma, M. Designing and Evaluating a Health Belief Model-Based Intervention to Increase Intent of HPV Vaccination among College Males. Int. Q. Community Health Educ. 2013, 34, 101–117. [Google Scholar] [CrossRef]
- O’Leary, S.T.; Pyrzanowski, J.; Brewer, S.E.; Sevick, C.; Dickinson, L.M.; Dempsey, A.F. Effectiveness of a multimodal intervention to increase vaccination in obstetrics/gynecology settings. Vaccine 2019, 37, 3409–3418. [Google Scholar] [CrossRef]
- Patel, A.; Stern, L.; Unger, Z.; Debevec, E.; Roston, A.; Hanover, R.; Morfesis, J. Staying on track: A cluster randomized controlled trial of automated reminders aimed at increasing human papillomavirus vaccine completion. Vaccine 2014, 32, 2428–2433. [Google Scholar] [CrossRef]
- Innovative Tool to Increase Completion of Human Papillomavirus (HPV) Vaccine Series. Available online: https://clinicaltrials.gov/ct2/show/NCT01343485 (accessed on 18 May 2021).
- Perkins, R.B.; Zisblatt, L.; Legler, A.; Trucks, E.; Hanchate, A.; Gorin, S.S. Effectiveness of a provider-focused intervention to improve HPV vaccination rates in boys and girls. Vaccine 2015, 33, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Elam, L.B.; Balat, M.I.; Berenson, A.B. Well-woman visit of mothers and human papillomavirus vaccine intent and uptake among their 9–17 year old children. Vaccine 2013, 31, 5544–5548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rickert, V.I.; Auslander, B.A.; Cox, D.S.; Rosenthal, S.L.; Rickert, J.A.; Rupp, R.; Zimet, G.D. School-based vaccination of young US males: Impact of health beliefs on intent and first dose acceptance. Vaccine 2014, 32, 1982–1987. [Google Scholar] [CrossRef] [PubMed]
- Roblin, D.W.; Ritzwoller, D.P.; Rees, D.I.; Carroll, N.M.; Chang, A.; Daley, M.F. The influence of deductible health plans on receipt of the human papillomavirus vaccine series. J. Adolesc. Health 2014, 54, 275–281. [Google Scholar] [CrossRef] [Green Version]
- Ruffin, M.T.; Plegue, M.A.; Rockwell, P.G.; Young, A.P.; Patel, D.A.; Yeazel, M.W. Impact of an Electronic Health Record (EHR) Reminder on Human Papillomavirus (HPV) Vaccine Initiation and Timely Completion. J. Am. Board Fam. Med. 2015, 28, 324–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, S. PIN62 Effectiveness of Text Message Reminders for Improving Vaccination Appointment Attendance and Series Completion Among Adolescents and Adults. Value Health 2012, 15, A248. [Google Scholar] [CrossRef]
- Sanderson, M.; Canedo, J.R.; Khabele, D.; Fadden, M.K.; Harris, C.; Beard, K.; Burress, M.; Pinkerton, H.; Jackson, C.; Mayo-Gamble, T.; et al. Pragmatic trial of an intervention to increase human papillomavirus vaccination in safety-net clinics. BMC Public Health 2017, 17, 158. [Google Scholar] [CrossRef] [Green Version]
- An HPV Vaccine Provider Intervention in Safety Net Clinics. Available online: https://clinicaltrials.gov/ct2/show/NCT02808832/ (accessed on 30 March 2021).
- Spleen, A.M.; Kluhsman, B.C.; Clark, A.D.; Dignan, M.B.; Lengerich, E.J.; The ACTION Health Cancer Task Force. An Increase in HPV-Related Knowledge and Vaccination Intent Among Parental and Non-parental Caregivers of Adolescent Girls, Age 9–17 Years, in Appalachian Pennsylvania. J. Cancer Educ. 2011, 27, 312–319. [Google Scholar] [CrossRef]
- Valdez, A.; Stewart, S.L.; Tanjasari, S.P.; Levy, V.; Garza, A. Design and efficacy of a multilingual, multicultural HPV vaccine education intervention. J. Commun. Health 2015, 8, 106–118. [Google Scholar] [CrossRef] [Green Version]
- Wadhera, P.; Evans, J.L.; Stein, E.; Gandhi, M.; Couture, M.-C.; Sansothy, N.; Sichan, K.; Maher, L.; Kaldor, J.; Page, K.; et al. Human papillomavirus knowledge, vaccine acceptance, and vaccine series completion among female entertainment and sex workers in Phnom Penh, Cambodia: The Young Women’s Health Study. Int. J. STD AIDS 2015, 26, 893–902. [Google Scholar] [CrossRef] [Green Version]
- Wedel, S.; Navarrete, C.R.; Burkard, C.J.F.; Clark, M.J. Improving Human Papillomavirus Vaccinations in Military Women. Mil. Med. 2016, 181, 1224–1227. [Google Scholar] [CrossRef] [Green Version]
- Wegwarth, O.; Kurzenhäuser-Carstens, S.; Gigerenzer, G. Overcoming the knowledge–behavior gap: The effect of evidence-based HPV vaccination leaflets on understanding, intention, and actual vaccination decision. Vaccine 2014, 32, 1388–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelan, N.W.; Steenbeek, A.; Martin-Misener, R.; Scott, J.; Smith, B.; D’Angelo-Scott, H. Engaging parents and schools improves uptake of the human papillomavirus (HPV) vaccine: Examining the role of the public health nurse. Vaccine 2014, 32, 4665–4671. [Google Scholar] [CrossRef] [PubMed]
- Winer, R.L.; Gonzales, A.A.; Noonan, C.J.; Buchwald, D.S. A Cluster-Randomized Trial to Evaluate a Mother–Daughter Dyadic Educational Intervention for Increasing HPV Vaccination Coverage in American Indian Girls. J. Community Health 2016, 41, 274–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, R.K.; Raviotta, J.M.; Nowalk, M.P.; Moehling, K.K.; Reis, E.C.; Humiston, S.G.; Lin, C.J. Using the 4 Pillars™ Practice Transformation Program to increase adolescent human papillomavirus, meningococcal, tetanus-diphtheria-pertussis and influenza vaccination. Vaccine 2017, 35, 6180–6186. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, R.K.; Moehling, K.K.; Lin, C.J.; Zhang, S.; Raviotta, J.M.; Reis, E.C.; Humiston, S.G.; Nowalk, M.P. Improving adolescent HPV vaccination in a randomized controlled cluster trial using the 4 Pillars™ practice Transformation Program. Vaccine 2017, 35, 109–117. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mavundza, E.J.; Iwu-Jaja, C.J.; Wiyeh, A.B.; Gausi, B.; Abdullahi, L.H.; Halle-Ekane, G.; Wiysonge, C.S. A Systematic Review of Interventions to Improve HPV Vaccination Coverage. Vaccines 2021, 9, 687. https://doi.org/10.3390/vaccines9070687
Mavundza EJ, Iwu-Jaja CJ, Wiyeh AB, Gausi B, Abdullahi LH, Halle-Ekane G, Wiysonge CS. A Systematic Review of Interventions to Improve HPV Vaccination Coverage. Vaccines. 2021; 9(7):687. https://doi.org/10.3390/vaccines9070687
Chicago/Turabian StyleMavundza, Edison J., Chinwe J. Iwu-Jaja, Alison B. Wiyeh, Blessings Gausi, Leila H. Abdullahi, Gregory Halle-Ekane, and Charles S. Wiysonge. 2021. "A Systematic Review of Interventions to Improve HPV Vaccination Coverage" Vaccines 9, no. 7: 687. https://doi.org/10.3390/vaccines9070687