
Humoral Response to SARS-CoV-2-Vaccination with BNT162b2 (Pfizer-BioNTech) in Patients on Hemodialysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Razzaghi, H.; Wang, Y.; Lu, H.; Marshall, K.E.; Dowling, N.F.; Paz-Bailey, G.; Twentyman, E.R.; Peacock, G.; Greenlund, K.J. Estimated county-level prevalence of selected underlying medical conditions associated with increased risk for severe COVID-19 illness—United States, 2018. Morb. Mortal. Wkly. Rep. 2020, 69, 945. [Google Scholar] [CrossRef]
- Hoxha, E.; Suling, A.; Turner, J.E.; Haubitz, M.; Floege, J.; Huber, T.B.; Galle, J. COVID-19 Prevalence and Mortality in Chronic Dialysis Patients. Dtsch. Arztebl. Int. 2021, 118, 195–196. [Google Scholar]
- Taji, L.; Thomas, D.; Oliver, M.J.; Ip, J.; Tang, Y.; Yeung, A.; Cooper, R.; House, A.A.; McFarlane, P.; Blake, P.G. COVID-19 in patients undergoing long-term dialysis in Ontario. CMAJ 2021, 193, E278–E284. [Google Scholar] [CrossRef]
- ERA-EDTA Council; ERACODA Working Group. Chronic kidney disease is a key risk factor for severe COVID-19: A call to action by the ERA-EDTA. Nephrol. Dial. Transplant. 2021, 36, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Windpessl, M.; Bruchfeld, A.; Anders, H.-J.; Kramer, H.; Waldman, M.; Renia, L.; Lisa, F.P.; Zhou, X.; Kronbichler, A. COVID-19 Vaccines and Kidney Disease. Nat. Rev. Nephrol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; Stein, G.E.; Bhupalam, S.; Havlichek, D.H. Immunogenicity of 13-valent conjugate pneumococcal vaccine in patients 50 years and older with end-stage renal disease and on dialysis. Clin. Vaccine Immunol. 2016, 23, 884–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastalerz-Migas, A.; Steciwko, A.; Brydak, L.B. Immune response to influenza vaccine in hemodialysis patients with chronic renal failure. Adv. Exp. Med. Biol. 2013, 756, 285–290. [Google Scholar] [PubMed]
- Ott, U.; Sauerbrei, A.; Lange, J.; Schäfler, A.; Walther, M.; Wolf, G.; Wutzler, P.; Zell, R.; Krumbholz, A. Serological response to influenza A H1N1 vaccine (Pandemrix®) and seasonal influenza vaccine 2009/2010 in renal transplant recipients and in hemodialysis patients. Med. Microbiol. Immunol. 2012, 201, 297–302. [Google Scholar] [CrossRef]
- Kong, N.; Beran, J.; Kee, S.; Miguel, J.; Sánchez, C.; Bayas, J.-M.; Vilella, A.; Calbo-Torrecillas, F.; de Novales, E.L.; Srinivasa, K. A new adjuvant improves the immune response to hepatitis B vaccine in hemodialysis patients. Kidney Int. 2008, 73, 856–862. [Google Scholar] [CrossRef] [Green Version]
- European Consensus Group on Hepatitis B Immunity. Are booster immunisations needed for lifelong hepatitis B immunity? Lancet 2000, 355, 561–565. [Google Scholar] [CrossRef]
- Krueger, K.M.; Ison, M.G.; Ghossein, C. Practical guide to vaccination in all stages of CKD, including patients treated by dialysis or kidney transplantation. Am. J. Kidney Dis. 2020, 75, 417–425. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Pahl, M.V.; Crum, A.; Norris, K. Effect of uremia on structure and function of immune system. J. Ren. Nutr. 2012, 22, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Kato, S.; Chmielewski, M.; Honda, H.; Pecoits-Filho, R.; Matsuo, S.; Yuzawa, Y.; Tranaeus, A.; Stenvinkel, P.; Lindholm, B. Aspects of immune dysfunction in end-stage renal disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1526–1533. [Google Scholar] [CrossRef] [Green Version]
- Fabrizi, F.; Dixit, V.; Martin, P.; Messa, P. Meta-analysis: The impact of diabetes mellitus on the immunological response to hepatitis B virus vaccine in dialysis patients. Aliment. Pharmacol. Ther. 2011, 33, 815–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabrizi, F.; Dixit, V.; Martin, P.; Jadoul, M.; Messa, P. Meta-analysis: The impact of nutritional status on the immune response to hepatitis B virus vaccine in chronic kidney disease. Dig. Dis. Sci. 2012, 57, 1366–1372. [Google Scholar] [CrossRef]
- Patel, N.; Assimon, M.M.; Bruni, E.; McNutt, L.-A.; Mason, D.L. Incidence and clinical predictors of nonresponse to hepatitis B vaccination among patients receiving hemodialysis: Importance of obesity. South. Med. J. 2015, 108, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Asan, A.; Demirhan, H.; Sorkun, H.Ç.; Özkan, S.; Aydın, M.; Akın, D.; Tatar, B.; Çatak, B.; Şener, A.; Köse, Ş. Factors affecting responsiveness to hepatitis B immunization in dialysis patients. Int. Urol. Nephrol. 2017, 49, 1845–1850. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck Jr, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J. Safety and immunogenicity of SARS-CoV-2 mRNA-1273 vaccine in older adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Bradley, T.; Grundberg, E.; Selvarangan, R.; LeMaster, C.; Fraley, E.; Banerjee, D.; Belden, B.; Louiselle, D.; Nolte, N.; Biswell, R.; et al. Antibody Responses after a Single Dose of SARS-CoV-2 mRNA Vaccine. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Geisen, U.M.; Berner, D.K.; Tran, F.; Sümbül, M.; Vullriede, L.; Ciripoi, M.; Reid, H.M.; Schaffarzyk, A.; Longardt, A.C.; Franzenburg, J.; et al. Immunogenicity and safety of anti-SARS-CoV-2 mRNA vaccines in patients with chronic inflammatory conditions and immunosuppressive therapy in a monocentric cohort. Ann. Rheum. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, B. Vaccines for the elderly: Current use and future challenges. Immun. Ageing 2018, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Gandjour, A.; Armsen, W.; Wehmeyer, W.; Multmeier, J.; Tschulena, U. Costs of patients with chronic kidney disease in Germany. PLoS ONE 2020, 15, e0231375. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subgroups of HDP | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HCW 39–65 years | All HDP 37–90 years | HDP 37–59 years | HDP 60–69 years | HDP 70–79 years | HDP 80–90 years | |||||||
| MD (Q1; Q3), (range: min–max); or n (%) | MD (Q1; Q3), (range: min–max); or n (%) | MD (Q1; Q3), (range: min–max); or n (%) | MD (Q1; Q3), (range: min–max); or n (%) | MD (Q1; Q3), (range: min–max); or n (%) | MD (Q1; Q3), (range: min–max); or n (%) | |||||||
| Subjects | 16 | 72 | 17 | 22 | 22 | 11 | ||||||
| Sex | ♀ | 9 (56.2%) | ♀ | 31 (43.1%) | ♀ | 8 (47.0%) | ♀ | 10 (45.5%) | ♀ | 8 (36.4%) | ♀ | 4 (36.4%) |
| ♂ | 7 (43.8%) | ♂ | 41 (56.9%) | ♂ | 9 (53.0%) | ♂ | 12 (54.5%) | ♂ | 14 (63.6%) | ♂ | 7 (63.6%) | |
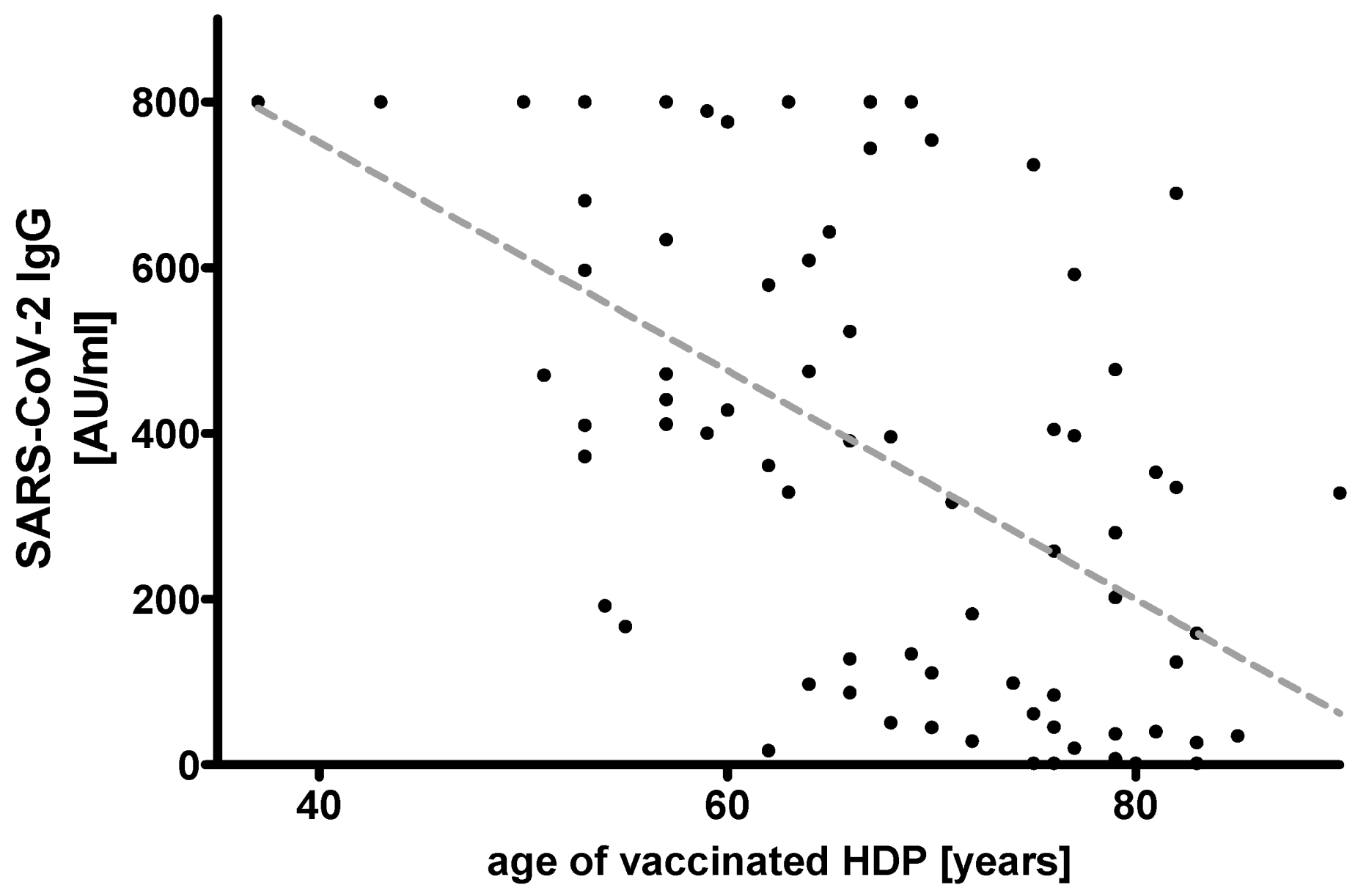
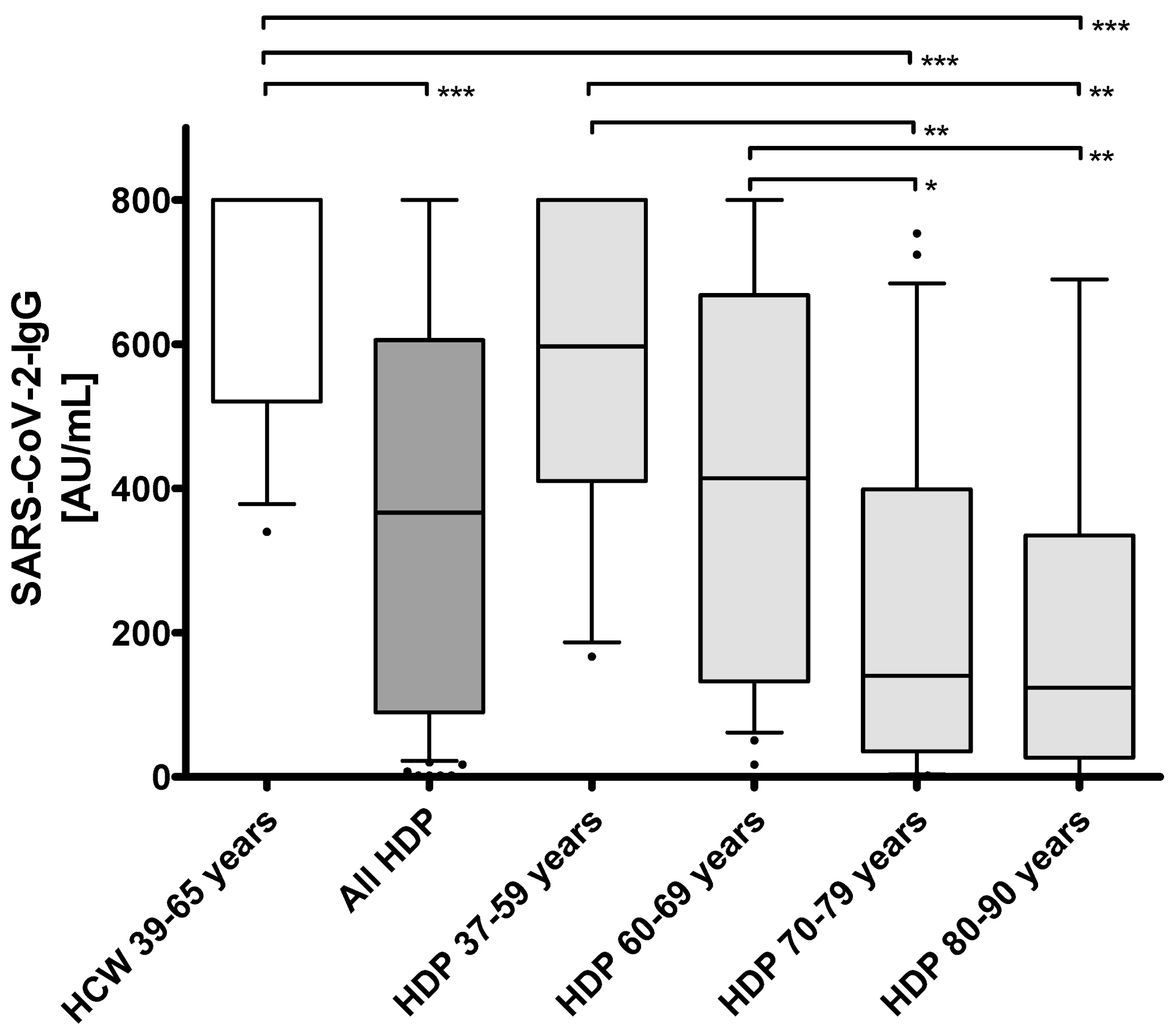
| Age (years) | 45.5 (41.2; 54.7), (range: 39.0–65.0) | 68.0 (60.0; 77.0), (range: 37.0–90.0) *** | 54.0 (53.0; −57.0), (range: 37.0–59.0) ns | 64.5 (62.0; 67.0), (range: 60.0–69.0) * | 76.0 (73.5; 77.5), (range: 70.0–79.0) *** | 82.0 (81.0; 83.0), (range: 80.0–90.0) *** | ||||||
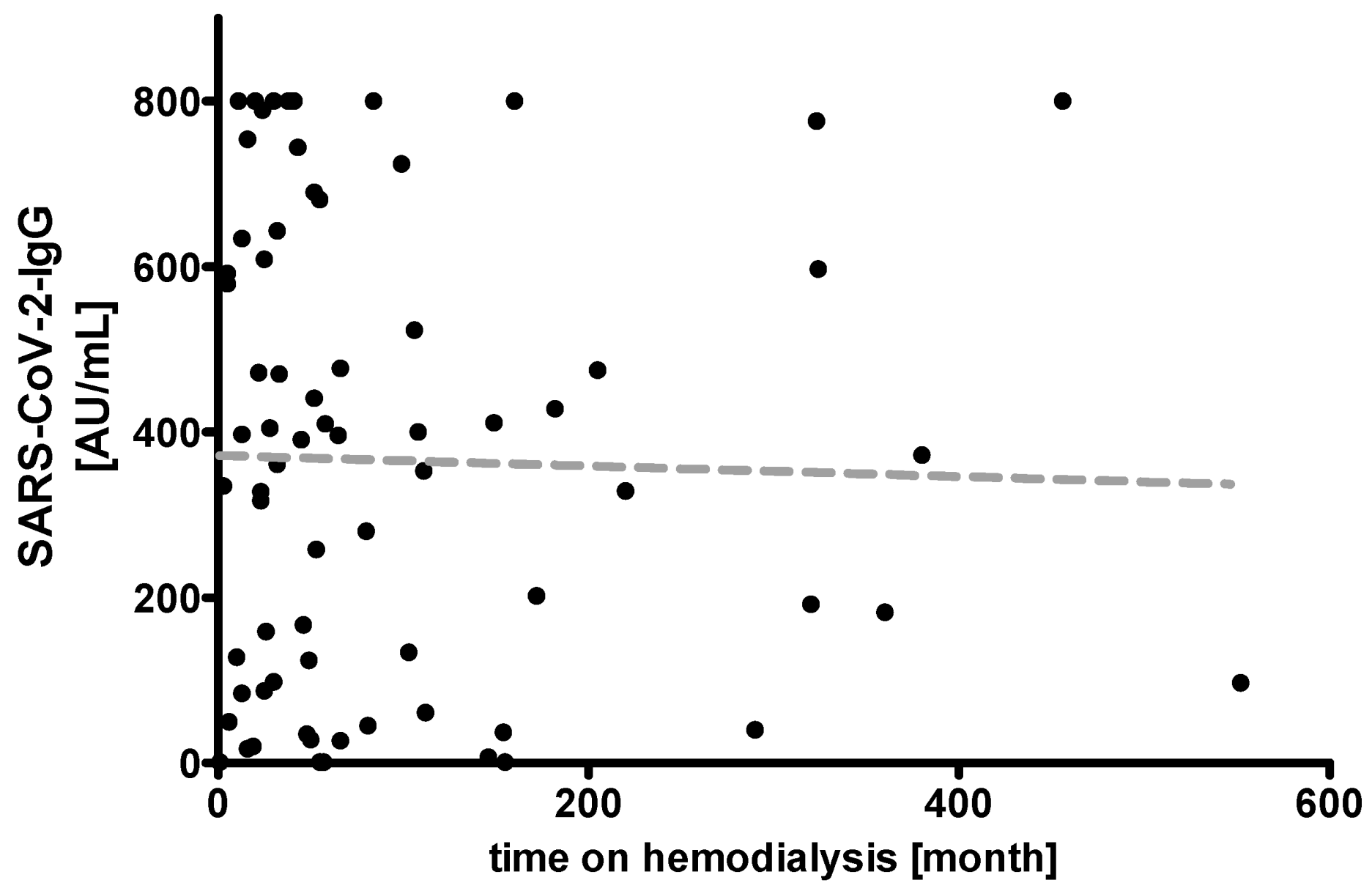
| Time on hemodialysis (months) | - | 52.0 (24.5; 111.7), (range: 1.0–552.0) | 52.0 (27.0; 240.0), (range: 11.0–456.0) | 44.0 (23.7; 126.5), (range: 5.0–552.0) | 56.0 (22.0; 102.2), (range: 5.0–360.0) | 49.0 (23.0; 111.0), (range: 1.0–290.0) | ||||||
| Time between 1st and 2nd vac (days) | 22.0 (22.0; 22.0), (range: 22.0–22.0) | 21.0 (21.0; 21.0), (range: 21.0–21.0) | 21.0 (21.0; 21.0), (range: 21.0–21.0) | 21.0 (21.0; 21.0), (range: 21.0–21.0) | 21.0 (21.0; 21.0), (range: 21.0–21.0) | 21.0 (21.0; 21.0), (range: 21.0–21.0) | ||||||
| Time between 2nd vac and sampling (days) | 13.0 (13.0; 13.0), (range: 13.0–19.0) | 17.0 (15.0; 18.0), (range: 15.0–26.0) | 17.0 (15.0; 18.0), (range: 15.0–18.0) | 17.5 (15.0; 18.0), (range: 15.0–26.0) | 17.0 (15.0; 18.0), (range: 15.0–20.0) | 15.0 (15.0; 18.0), (range: 15.0–18.0) | ||||||
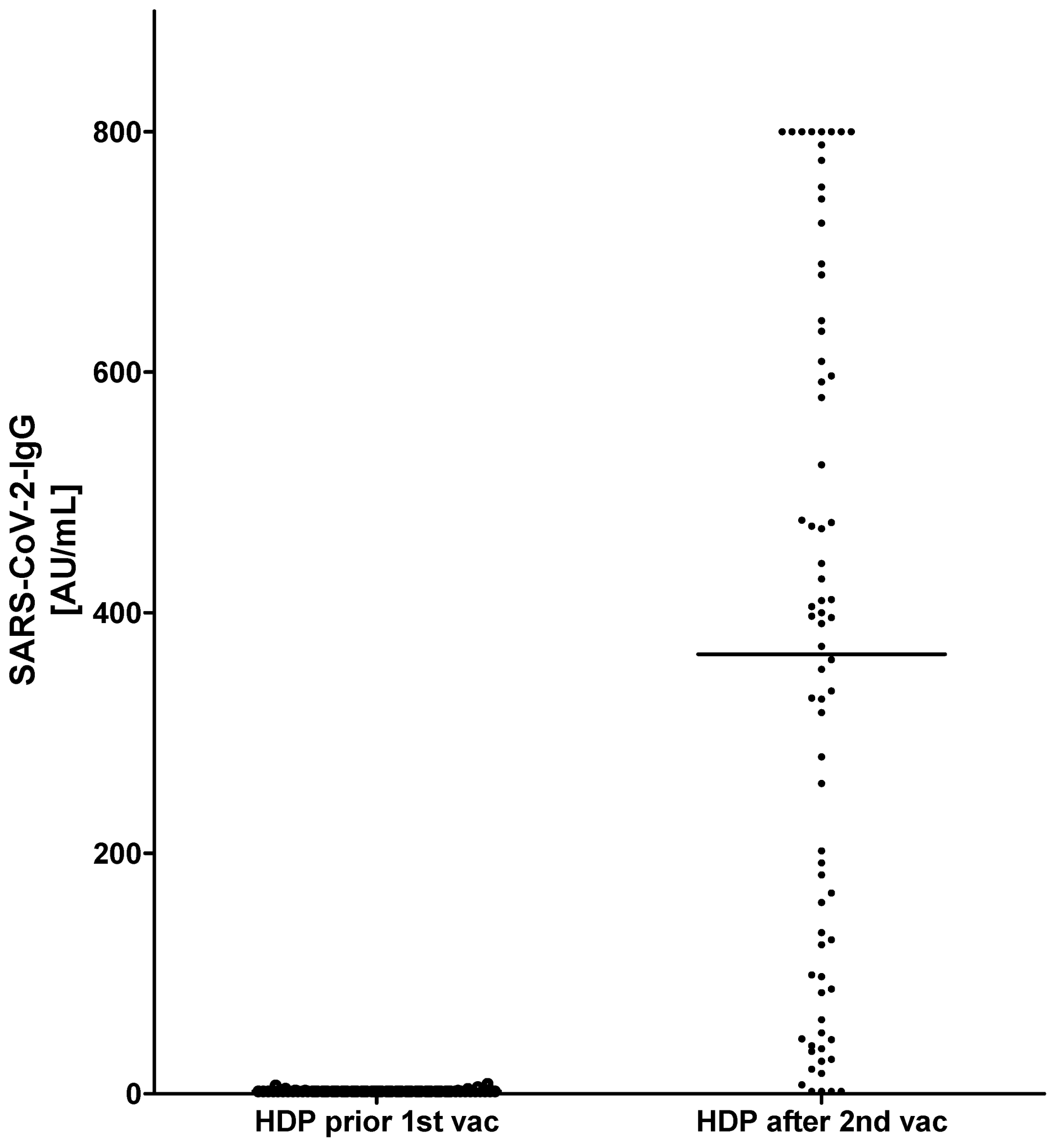
| Ab SARS-CoV-2 CLIA (AU/mL) | 800.0 (520.5; 800.0), (range: 340.0–800.0) | 366.5 (89.6; 606.0), (range: 1.8–800.0) *** | 597.0 (410.5; 800.0), (range: 167.0–800.0) ns | 414.0 (132.5; 668.3), (range: 17.0–800.0) ns | 140.0 (35.3; 399.0), (range: 1.8–754.0) *** | 124.0 (27.0; 335.0), (range: 1.8–690.0) *** | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jahn, M.; Korth, J.; Dorsch, O.; Anastasiou, O.E.; Sorge-Hädicke, B.; Tyczynski, B.; Gäckler, A.; Witzke, O.; Dittmer, U.; Dolff, S.; et al. Humoral Response to SARS-CoV-2-Vaccination with BNT162b2 (Pfizer-BioNTech) in Patients on Hemodialysis. Vaccines 2021, 9, 360. https://doi.org/10.3390/vaccines9040360
Jahn M, Korth J, Dorsch O, Anastasiou OE, Sorge-Hädicke B, Tyczynski B, Gäckler A, Witzke O, Dittmer U, Dolff S, et al. Humoral Response to SARS-CoV-2-Vaccination with BNT162b2 (Pfizer-BioNTech) in Patients on Hemodialysis. Vaccines. 2021; 9(4):360. https://doi.org/10.3390/vaccines9040360
Chicago/Turabian StyleJahn, Michael, Johannes Korth, Oliver Dorsch, Olympia Evdoxia Anastasiou, Burkhard Sorge-Hädicke, Bartosz Tyczynski, Anja Gäckler, Oliver Witzke, Ulf Dittmer, Sebastian Dolff, and et al. 2021. "Humoral Response to SARS-CoV-2-Vaccination with BNT162b2 (Pfizer-BioNTech) in Patients on Hemodialysis" Vaccines 9, no. 4: 360. https://doi.org/10.3390/vaccines9040360