
Internal and External Validity of Social Media and Mobile Technology-Driven HPV Vaccination Interventions: Systematic Review Using the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) Framework

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. RE-AIM Criteria
2.2.1. Reach Dimension
2.2.2. Effectiveness Dimension
2.2.3. Adoption Dimension
2.2.4. Implementation Dimension
2.2.5. Maintenance Dimension
2.3. Coding and Analysis
3. Results
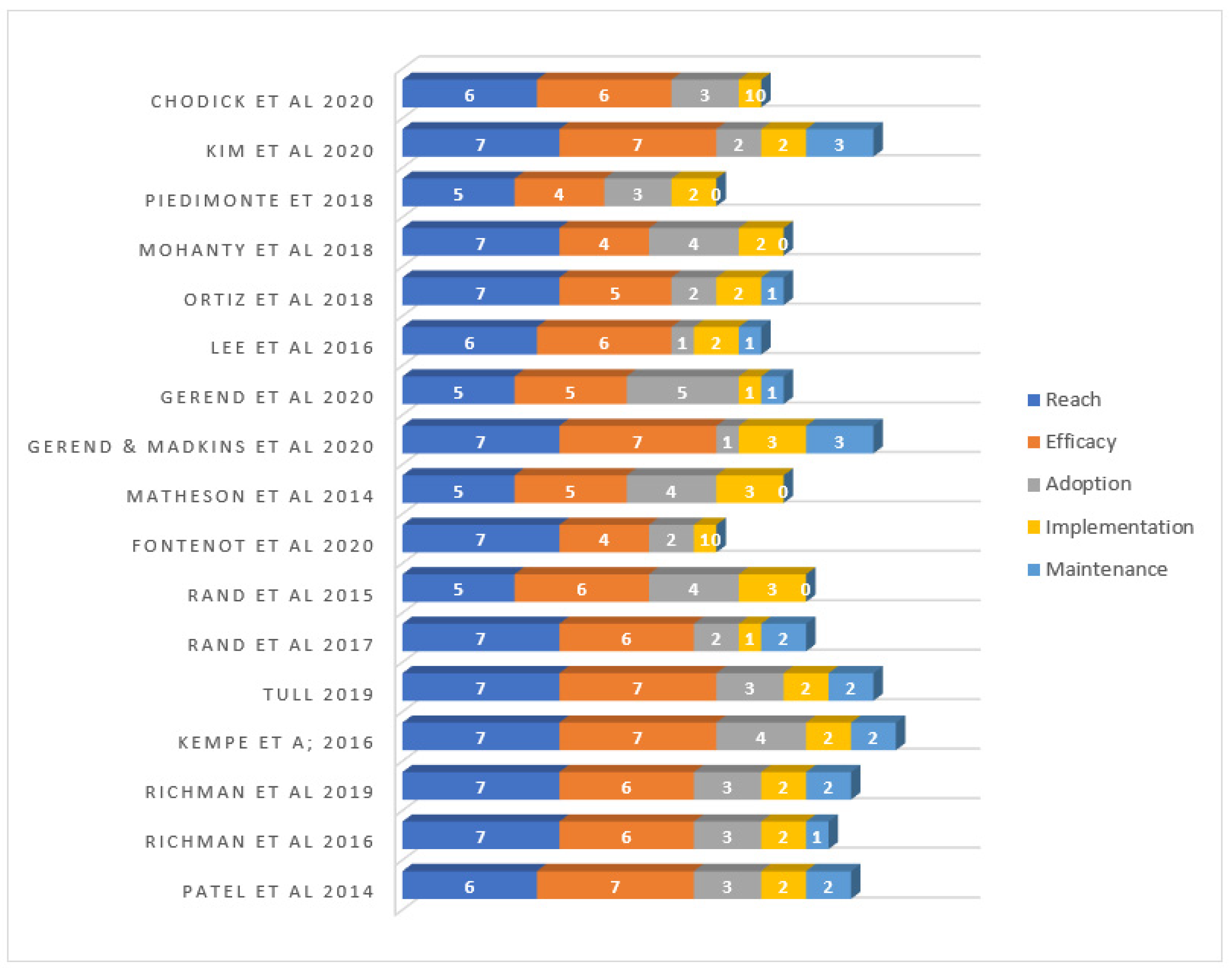
3.1. RE-AIM Reporting Scores
3.1.1. Reach Dimension
3.1.2. Efficacy/Effectiveness Dimension
3.1.3. Adoption Dimension
3.1.4. Implementation
3.1.5. Maintenance
4. Discussion
4.1. Summary
4.1.1. Reach Dimension
4.1.2. Efficacy/Effectiveness
4.1.3. Adoption Dimension
4.1.4. Implementation
4.1.5. Maintenance
4.2. Limitations
4.3. Strengths
4.4. Implications and Recommendations
4.4.1. Implication for Future Publication
4.4.2. Implications for Future HPV Vaccine Intervention
- While a few reviewed studies included parents of adolescents [15,45,46,50], there is a need to consider social media strategies as a potential method to reach parents. Parents either make decisions to vaccinate their teenagers or influence their children’s decisions so not including them in the target population is a missed opportunity to influence behavior [68].
- The overall penetration or reach of the studies was high, especially in studies that used Facebook to reach a large population [41,50]. However, the impact of social media on the vaccine uptake was rarely measured in the reviewed studies. Future studies should compare the effectiveness of different social media platforms (e.g., Facebook vs. text messaging) on HPV vaccine uptake.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Cervical Cancer. Available online: https://www.who.int/cancer/prevention/diagnosis-screening/cervical-cancer/en/ (accessed on 16 November 2020).
- Deshmukh, A.A.; Suk, R.; Shiels, M.S.; Sonawane, K.; Nyitray, A.G.; Liu, Y.; Gaisa, M.M.; Palefsky, J.M.; Sigel, K. Recent Trends in Squamous Cell Carcinoma of the Anus Incidence and Mortality in the United States, 2001–2015. J. Natl. Cancer Inst. 2020, 112, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Ellington, T.D.; Henley, S.J.; Senkomago, V.; O’Neil, M.E.; Wilson, R.J.; Singh, S.; Richardson, L.C. Trends in Incidence of Cancers of the Oral Cavity and Pharynx—United States 2007–2016. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 433. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Approves Expanded Use of Gardasil 9 to Include Individuals 27 through 45 Years Old. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-expanded-use-gardasil-9-include-individuals-27-through-45-years-old (accessed on 14 November 2020).
- Healthy People 2030. Increase the Proportion of Adolescents Who Get Recommended Doses of the HPV Vaccine—IID 08. Available online: https://health.gov/healthypeople/objectives-and-data/browse-objectives/vaccination/increase-proportion-adolescents-who-get-recommended-doses-hpv-vaccine-iid-08 (accessed on 2 December 2020).
- Peterson, C.E.; Dykens, J.A.; Brewer, N.T.; Buscemi, J.; Watson, K.; Comer-Hagans, D.; Ramamonjiarivelo, Z.; Fitzgibbon, M. Society of Behavioral Medicine Supports Increasing HPV Vaccination Uptake: An Urgent Opportunity for Cancer Prevention. Transl. Behav. Med. 2016, 6, 672–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elam-Evans, L.D.; Yankey, D.; Singleton, J.A.; Sterrett, N.; Markowitz, L.E.; Williams, C.L.; Stokley, S. National, Regional, State, and Selected Local Area Vaccination Coverage among Adolescents Aged 13–17 Years—United States, 2019. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 1109. [Google Scholar] [CrossRef] [PubMed]
- Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 6 November 2020).
- Holman, D.M.; Benard, V.; Roland, K.B.; Watson, M.; Liddon, N.; Stokley, S. Barriers to Human Papillomavirus Vaccination among US Adolescents: A Systematic Review of the Literature. JAMA Pediatr. 2014, 168, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, S.O.A.; Akinwunmi, B.; Elias, K.M.; Feldman, S. Educating Healthcare Providers to Increase Human Papillomavirus (HPV) Vaccination Rates: A Qualitative Systematic Review. Vaccine X 2019, 3, 100037. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.; Carrico, C.; Costanzo, C. Identifying and Overcoming Perceived Barriers of Providers towards HPV Vaccination: A Literature Review. J. Vaccines 2015, 2015, 869468. [Google Scholar] [CrossRef] [Green Version]
- Wilson, A.R.; Hashibe, M.; Bodson, J.; Gren, L.H.; Taylor, B.A.; Greenwood, J.; Jackson, B.R.; She, R.; Egger, M.J.; Kepka, D. Factors Related to HPV Vaccine Uptake and 3-Dose Completion among Women in a Low Vaccination Region of the USA: An Observational Study. BMC Womens Health 2016, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fishman, J.; Taylor, L.; Frank, I. Awareness of HPV and Uptake of Vaccination in a High-Risk Population. Pediatrics 2016, 138, e20152048. [Google Scholar] [CrossRef] [Green Version]
- Chao, C.; Preciado, M.; Slezak, J.; Xu, L. A Randomized Intervention of Reminder Letter for Human Papillomavirus Vaccine Series Completion. J. Adolesc. Health 2015, 56, 85–90. [Google Scholar] [CrossRef]
- Kempe, A.; O’Leary, S.T.; Shoup, J.A.; Stokley, S.; Lockhart, S.; Furniss, A.; Dickinson, L.M.; Barnard, J.; Daley, M.F. Parental Choice of Recall Method for HPV Vaccination: A Pragmatic Trial. Pediatrics 2016, 137, e20152857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, K.; Zoellner, J.; Motley, M.; Estabrooks, P.A. Understanding the Internal and External Validity of Health Literacy Interventions: A Systematic Literature Review Using the RE-AIM Framework. J. Health Commun. 2011, 16, 55–72. [Google Scholar] [CrossRef] [Green Version]
- Steckler, A.; McLeroy, K.R. The Importance of External Validity. Am. J. Public Health 2008, 98, 9–10. [Google Scholar] [CrossRef]
- Akers, J.D.; Estabrooks, P.A.; Davy, B.M. Translational Research: Bridging the Gap between Long-Term Weight Loss Maintenance Research and Practice. J. Am. Diet. Assoc. 2010, 110, 1511–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glasgow, R.E.; Klesges, L.M.; Dzewaltowski, D.A.; Bull, S.S.; Estabrooks, P. The Future of Health Behavior Change Research: What Is Needed to Improve Translation of Research into Health Promotion Practice? Ann. Behav. Med. 2004, 27, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Dzewaltowski, D.A.; Estabrooks, P.A.; Klesges, L.M.; Bull, S.; Glasgow, R.E. Behavior Change Intervention Research in Community Settings: How Generalizable Are the Results? Health Promot. Int. 2004, 19, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the Public Health Impact of Health Promotion Interventions: The RE-AIM Framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [Green Version]
- McGoey, T.; Root, Z.; Bruner, M.W.; Law, B. Evaluation of Physical Activity Interventions in Children via the Reach, Efficacy/Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) Framework: A Systematic Review of Randomized and Non-Randomized Trials. Prev. Med. 2016, 82, 8–19. [Google Scholar] [CrossRef]
- Craike, M.; Hill, B.; Gaskin, C.J.; Skouteris, H. Interventions to Improve Physical Activity during Pregnancy: A Systematic Review on Issues of Internal and External Validity Using the RE-AIM Framework. BJOG 2017, 124, 573–583. [Google Scholar] [CrossRef]
- Bull, S.S.; Gillette, C.; Glasgow, R.E.; Estabrooks, P. Work Site Health Promotion Research: To What Extent Can We Generalize the Results and What Is Needed to Translate Research to Practice? Health Educ. Behav. 2003, 30, 537–549. [Google Scholar] [CrossRef]
- Estabrooks, P.; Dzewaltowski, D.A.; Glasgow, R.E.; Klesges, L.M. School-Based Health Promotion: Issues Related to Translating Research into Practice. J. Sch. Health 2002, 73, 21–28. [Google Scholar] [CrossRef]
- Bastos, P.d.O.; Cavalcante, A.S.P.; Pereira, W.M.G.; de Castro, V.H.S.; Ferreira Júnior, A.R.; Guerra, P.H.; da Silva, K.S.; da Silva, M.R.F.; Barbosa Filho, V.C. Health Promoting School Interventions in Latin America: A Systematic Review Protocol on the Dimensions of the RE-AIM Framework. Int. J. Environ. Res. Public Health 2020, 17, 5558. [Google Scholar] [CrossRef]
- Klesges, L.M.; Dzewaltowski, D.A.; Glasgow, R.E. Review of External Validity Reporting in Childhood Obesity Prevention Research. Am. J. Prev. Med. 2008, 34, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Economos, C.D.; Anzman-Frasca, S.; Koomas, A.H.; Bakun, P.J.; Brown, C.M.; Brown, D.; Folta, S.C.; Fullerton, K.J.; Sacheck, J.M.; Sharma, S.; et al. Dissemination of Healthy Kids out of School Principles for Obesity Prevention: A RE-AIM Analysis. Prev. Med. 2019, 119, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Flack, J.C.; Herman, A.; Buscemi, J.; Kong, A.; Bains, A.; Fitzgibbon, M.L. A Systematic Review of the Implementation of Obesity Prevention Interventions in Early Childcare and Education Settings Using the RE-AIM Framework. Transl. Behav. Med. 2020, 10, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Schlechter, C.R.; Rosenkranz, R.R.; Guagliano, J.M.; Dzewaltowski, D.A. A Systematic Review of Children’s Dietary Interventions with Parents as Change Agents: Application of the RE-AIM Framework. Prev. Med. 2016, 91, 233–243. [Google Scholar] [CrossRef]
- Barden, C.; Bekker, S.; Brown, J.C.; Stokes, K.A.; McKay, C.D. Evaluating the Implementation of Injury Prevention Strategies in Rugby Union and League: A Systematic Review Using the RE-AIM Framework. Int. J. Sports Med. 2021, 42, 112–121. [Google Scholar]
- Isaacs, S.A.; Roman, N.V.; Savahl, S.; Sui, X.-C. Using the RE-AIM Framework to Identify and Describe Best Practice Models in Family-Based Intervention Development: A Systematic Review. Child Fam. Soc. Work 2018, 23, 122–136. [Google Scholar] [CrossRef]
- Yoshida, Y.; Patil, S.J.; Brownson, R.C.; Boren, S.A.; Kim, M.; Dobson, R.; Waki, K.; Greenwood, D.A.; Torbjørnsen, A.; Ramachandran, A.; et al. Using the RE-AIM Framework to Evaluate Internal and External Validity of Mobile Phone-Based Interventions in Diabetes Self-Management Education and Support. J. Am. Med. Inform. Assoc. 2020, 27, 946–956. [Google Scholar] [CrossRef] [PubMed]
- Iwelunmor, J.; Nwaozuru, U.; Obiezu-Umeh, C.; Uzoaru, F.; Ehiri, J.; Curley, J.; Ezechi, O.; Airhihenbuwa, C.; Ssewamala, F. Is It Time to RE-AIM? A Systematic Review of Economic Empowerment as HIV Prevention Intervention for Adolescent Girls and Young Women in Sub-Saharan Africa Using the RE-AIM Framework. Implement Sci. Commun. 2020, 1, 53. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.S.; De Gagne, J.C.; Son, Y.D.; Chae, S.-M. Completeness of Human Papilloma Virus Vaccination: A Systematic Review. J. Pediatr. Nurs. 2018, 39, 7–14. [Google Scholar] [CrossRef]
- Francis, D.B.; Cates, J.R.; Wagner, K.P.G.; Zola, T.; Fitter, J.E.; Coyne-Beasley, T. Communication Technologies to Improve HPV Vaccination Initiation and Completion: A Systematic Review. Patient Educ. Couns. 2017, 100, 1280–1286. [Google Scholar] [CrossRef]
- Gerend, M.A.; Murdock, C.; Grove, K. An Intervention for Increasing HPV Vaccination on a University Campus. Vaccine 2020, 38, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Lee, H.; Kiang, P.; Aronowitz, T.; Sheldon, L.K.; Shi, L.; Allison, J.J. A Storytelling Intervention in a Mobile, Web-Based Platform: A Pilot Randomized Controlled Trial to Evaluate the Preliminary Effectiveness to Promote Human Papillomavirus Vaccination in Korean American College Women. Health Educ. Behav. 2020, 47, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Koopmeiners, J.S.; McHugh, J.; Raveis, V.H.; Ahluwalia, J.S. mHealth Pilot Study: Text Messaging Intervention to Promote HPV Vaccination. Am. J. Health Behav. 2016, 40, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matheson, E.C.; Derouin, A.; Gagliano, M.; Thompson, J.A.; Blood-Siegfried, J. Increasing HPV Vaccination Series Completion Rates via Text Message Reminders. J. Pediatr. Health Care 2014, 28, e35–e39. [Google Scholar] [CrossRef]
- Mohanty, S.; Leader, A.E.; Gibeau, E.; Johnson, C. Using Facebook to Reach Adolescents for Human Papillomavirus (HPV) Vaccination. Vaccine 2018, 36, 5955–5961. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, R.R.; Shafer, A.; Cates, J.; Coyne-Beasley, T. Development and Evaluation of a Social Media Health Intervention to Improve Adolescents’ Knowledge about and Vaccination against the Human Papillomavirus. Glob. Pediatr. Health 2018, 5, 2333794X18777918. [Google Scholar] [CrossRef]
- Patel, A.; Stern, L.; Unger, Z.; Debevec, E.; Roston, A.; Hanover, R.; Morfesis, J. Staying on Track: A Cluster Randomized Controlled Trial of Automated Reminders Aimed at Increasing Human Papillomavirus Vaccine Completion. Vaccine 2014, 32, 2428–2433. [Google Scholar] [CrossRef] [PubMed]
- Piedimonte, S.; Leung, A.; Zakhari, A.; Giordano, C.; Tellier, P.-P.; Lau, S. Impact of an HPV Education and Vaccination Campaign among Canadian University Students. J. Obstet. Gynaecol. Can. 2018, 40, 440–446. [Google Scholar] [CrossRef]
- Rand, C.M.; Brill, H.; Albertin, C.; Humiston, S.G.; Schaffer, S.; Shone, L.P.; Blumkin, A.K.; Szilagyi, P.G. Effectiveness of Centralized Text Message Reminders on Human Papillomavirus Immunization Coverage for Publicly Insured Adolescents. J. Adolesc. Health 2015, 56, S17–S20. [Google Scholar] [CrossRef]
- Rand, C.M.; Vincelli, P.; Goldstein, N.P.N.; Blumkin, A.; Szilagyi, P.G. Effects of Phone and Text Message Reminders on Completion of the Human Papillomavirus Vaccine Series. J. Adolesc. Health 2017, 60, 113–119. [Google Scholar] [CrossRef]
- Richman, A.R.; Torres, E.; Wu, Q.; Carlston, L.; O’Rorke, S.; Moreno, C.; Olsson, J. Text and Email Messaging for Increasing Human Papillomavirus Vaccine Completion among Uninsured or Medicaid-Insured Adolescents in Rural Eastern North Carolina. J. Health Care Poor Underserved 2019, 30, 1499–1517. [Google Scholar] [CrossRef]
- Richman, A.R.; Maddy, L.; Torres, E.; Goldberg, E.J. A Randomized Intervention Study to Evaluate Whether Electronic Messaging Can Increase Human Papillomavirus Vaccine Completion and Knowledge among College Students. J Am. Coll. Health 2016, 64, 269–278. [Google Scholar] [CrossRef]
- Tull, F.; Borg, K.; Knott, C.; Beasley, M.; Halliday, J.; Faulkner, N.; Sutton, K.; Bragge, P. Short Message Service Reminders to Parents for Increasing Adolescent Human Papillomavirus Vaccination Rates in a Secondary School Vaccine Program: A Randomized Control Trial. J. Adolesc. Health 2019, 65, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Chodick, G.; Teper, G.R.; Levi, S.; Kopel, H.; Kleinbort, A.; Khen, E.; Schejter, E.; Shalev, V.; Stein, M.; Lewis, N. The Impact of a Facebook Campaign among Mothers on HPV Vaccine Uptake among Their Daughters: A Randomized Field Study. Gynecol. Oncol. 2021, 160, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Fontenot, H.B.; White, B.P.; Rosenberger, J.G.; Lacasse, H.; Rutirasiri, C.; Mayer, K.H.; Zimet, G. Mobile App Strategy to Facilitate Human Papillomavirus Vaccination among Young Men Who Have Sex with Men: Pilot Intervention Study. J. Med. Internet Res. 2020, 22, e22878. [Google Scholar] [CrossRef]
- Gerend, M.A.; Madkins, K.; Crosby, S.; Korpak, A.K.; Phillips, G.L.; Bass, M.; Houlberg, M.; Mustanski, B. Evaluation of a Text Messaging-Based Human Papillomavirus Vaccination Intervention for Young Sexual Minority Men: Results from a Pilot Randomized Controlled Trial. Ann. Behav. Med. 2020. [Google Scholar] [CrossRef]
- White, S.M.; McAuley, E.; Estabrooks, P.A.; Courneya, K.S. Translating Physical Activity Interventions for Breast Cancer Survivors into Practice: An Evaluation of Randomized Controlled Trials. Ann. Behav. Med. 2009, 37, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Gaglio, B.; Shoup, J.A.; Glasgow, R.E. The RE-AIM Framework: A Systematic Review of Use over Time. Am. J. Public Health 2013, 103, e38–e46. [Google Scholar] [CrossRef]
- Dixon, B.E.; Zimet, G.D.; Xiao, S.; Tu, W.; Lindsay, B.; Church, A.; Downs, S.M. An educational intervention to improve HPV vaccination: A cluster randomized trial. Pediatrics 2019, 143, e20181457. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, S.A.; Roncancio, A.M.; Savas, L.S.; Lopez, D.M.; Vernon, S.W.; Fernandez, M.E. Using Intervention Mapping to Develop and Adapt Two Educational Interventions for Parents to Increase HPV Vaccination Among Hispanic Adolescents. Front. Public Health 2018, 6, 164. [Google Scholar] [CrossRef] [Green Version]
- Watts, L.A.; Joseph, N.; Wallace, M.; Rauh-Hain, J.A.; Muzikansky, A.; Growdon, W.B.; Del Carmen, M.G. HPV vaccine: A comparison of attitudes and behavioral perspectives between Latino and non-Latino women. Gynecol. Oncol. 2009, 112, 577–582. [Google Scholar] [CrossRef]
- Dempsey, A.F.; Zimet, G.D.; Davis, R.L.; Koutsky, L. Factors that are associated with parental acceptance of human papillomavirus vaccines: A randomized intervention study of written information about HPV. Pediatrics 2006, 117, 1486–1493. [Google Scholar] [CrossRef]
- Friedman, L.M.; Furberg, C.D.; DeMets, D.L.; Reboussin, D.M.; Granger, C.B. Issues in Data Analysis. In Fundamentals of Clinical Trials; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- McCoy, C.E. Understanding the Intention-to-Treat Principle in Randomized Controlled Trials. West. J. Emerg. Med. 2017, 18, 1075–1078. [Google Scholar] [CrossRef] [PubMed]
- Hollis, S.; Campbell, F. What Is Meant by Intention to Treat Analysis? Survey of Published Randomised Controlled Trials. BMJ 1999, 319, 670–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumville, J.C.; Torgerson, D.J.; Hewitt, C.E. Reporting Attrition in Randomised Controlled Trials. BMJ 2006, 332, 969–971. [Google Scholar] [CrossRef] [Green Version]
- Shanks, C.B.; Harden, S. A Reach, Effectiveness, Adoption, Implementation, Maintenance Evaluation of Weekend Backpack Food Assistance Programs. Am. J. Health Promot. 2016, 30, 511–520. [Google Scholar] [CrossRef] [Green Version]
- Weiss, C.H. Evaluation: Methods for Studying Programs and Policies; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Lipsey, M.; Sechrest, P.; Perrin, E.; Bunker, J. Research Methodology: Strengthening Causal Interpretations of Non-Experimental Data. Cancer Causes Control 1990, 1, 196. [Google Scholar]
- Brazil, K.; Ozer, E.; Cloutier, M.M.; Levine, R.; Stryer, D. From Theory to Practice: Improving the Impact of Health Services Research. BMC Health Serv. Res. 2005, 5, 1. [Google Scholar] [CrossRef]
- Dzewaltowski, D.A.; Estabrooks, P.A.; Glasgow, R.E. The Future of Physical Activity Behavior Change Research: What Is Needed to Improve Translation of Research into Health Promotion Practice? Exerc. Sport Sci. Rev. 2004, 32, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Duggan, M.; Lenhart, A.; Lampe, C.; Ellison, N.B. Parents and Social Media; Pew Research Center: Washington, DC, USA, 2015; p. 16. [Google Scholar]



{kind=link}
{kind=link}
| Dimension | Definition | Indicator | Percentage (%) |
|---|---|---|---|
| Reach (R) | The proportion and representativeness of individuals willing to participate in a given intervention. | 1. Described Target Population | 100 |
| 2. Demographic & behavioral information | 100 | ||
| 3. Recruitment Strategies | 94.1 | ||
| 4. Inclusion & exclusion criteria | 94.1 | ||
| 5. Method to identify the target population | 76.5 | ||
| 6. Sample size | 88.2 | ||
| 7. Participation rate | 82.4 | ||
| Average: 90.8 | |||
| Efficacy/Effectiveness (E) | The influence of an intervention on important outcomes, including potential negative effects, quality of life, and economic outcomes | 1. Design/Conditions | 100 |
| 2. Efficacy, Effectiveness, Translational? | 100 | ||
| 3. Measure of the primary outcome | 100 | ||
| 4. Results (shortest assessment) | 94.1 | ||
| 5. Intent-to-treat or present at FU | 35.3 | ||
| 6. Imputation procedure | 76.5 | ||
| 7. Measure of robustness across subgroups | 47.1 | ||
| 8. Measure of short-term attrition | 23.5 | ||
| Average: 72.1 | |||
| Adoption (A) | The proportion and representativeness of locations and intervention staff willing to initiate and adopt an intervention | 1. Description of intervention location | 88.2 |
| 2. Description of delivery staff | 64.7 | ||
| 3. Method to identify target delivery agent | 47.1 | ||
| 4. Level of expertise of delivery agent | 58.8 | ||
| 5. Delivery staff participation rate | 11.8 | ||
| 6. Organizational spread | 5.9 | ||
| 7. Measures of cost of adoption | 5.9 | ||
| Average: 40.3 | |||
| Implementation (I) | How consistently various elements of an intervention are delivered as intended by staff, and the time and cost of the intervention | 1. Intervention frequency | 88.2 |
| 2. Extent protocol delivered as intended (%) | 11.8 | ||
| 3. Participant attendance/completion rates | 82.4 | ||
| 4. Measures of cost | 0 | ||
| Average: 45.6 | |||
| Maintenance (M) | The extent to which participants make and maintain a behavior change and the sustainability of a program or policy in the setting in which it was intervened | 1. Follow-up assessment (3- or 6-months) | 70.6 |
| 2. Attrition | 35.3 | ||
| 3. Is the program still in place? | 0 | ||
| 4. Was the program institutionalized? | 0 | ||
| Average: 26.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asare, M.; Popelsky, B.; Akowuah, E.; Lanning, B.A.; Montealegre, J.R. Internal and External Validity of Social Media and Mobile Technology-Driven HPV Vaccination Interventions: Systematic Review Using the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) Framework. Vaccines 2021, 9, 197. https://doi.org/10.3390/vaccines9030197
Asare M, Popelsky B, Akowuah E, Lanning BA, Montealegre JR. Internal and External Validity of Social Media and Mobile Technology-Driven HPV Vaccination Interventions: Systematic Review Using the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) Framework. Vaccines. 2021; 9(3):197. https://doi.org/10.3390/vaccines9030197
Chicago/Turabian StyleAsare, Matthew, Braden Popelsky, Emmanuel Akowuah, Beth A. Lanning, and Jane R. Montealegre. 2021. "Internal and External Validity of Social Media and Mobile Technology-Driven HPV Vaccination Interventions: Systematic Review Using the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) Framework" Vaccines 9, no. 3: 197. https://doi.org/10.3390/vaccines9030197