
Factors Influencing the Intention and Uptake of COVID-19 Vaccines on the African Continent: A Scoping Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Searching for Relevant Studies
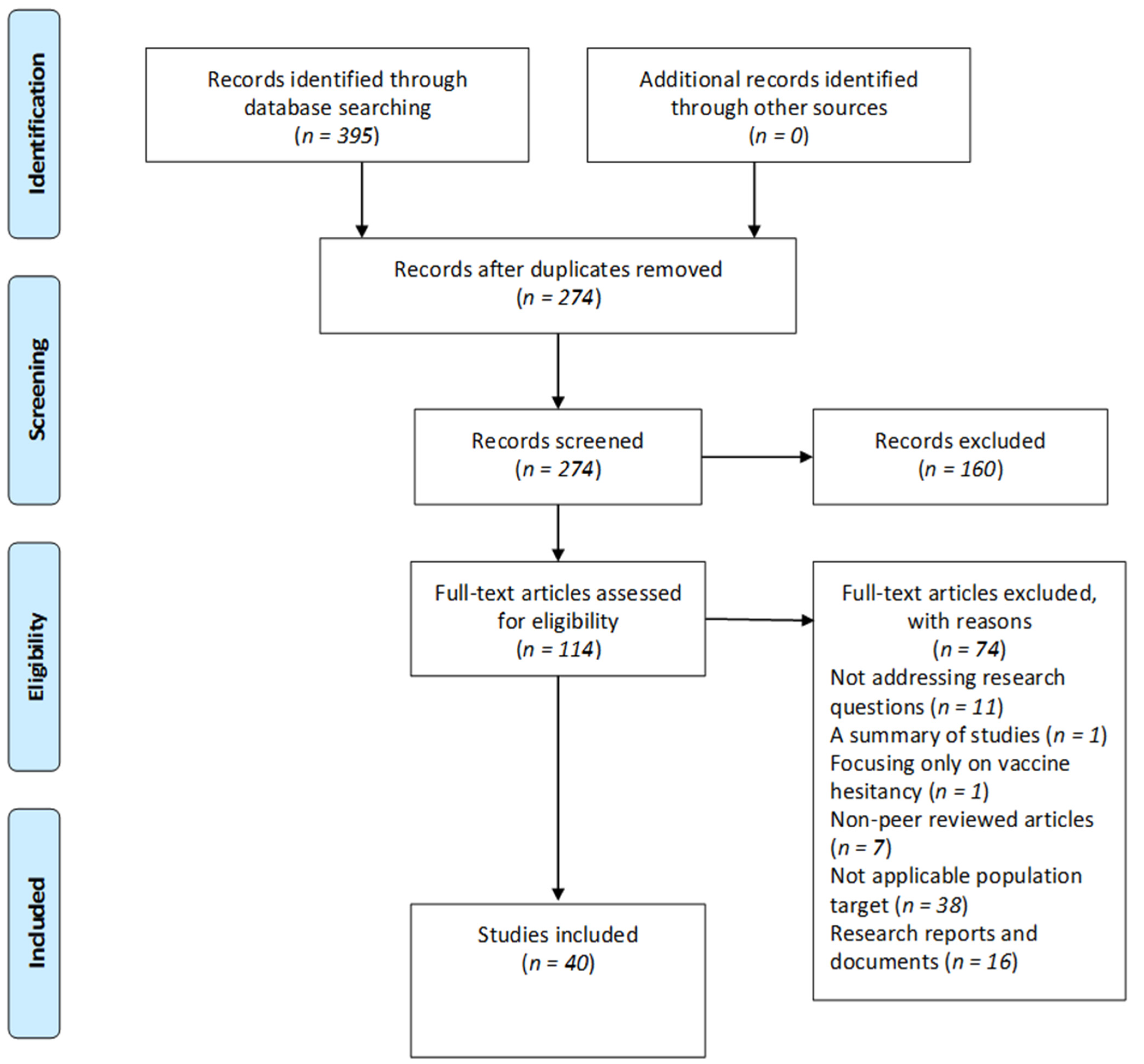
2.2. Study Selection
2.3. Charting Data
3. Reporting the Results
3.1. Study Design of Included Studies
3.2. Country of Focus
3.3. Participant Characteristics
4. Results Pertaining to the Research Questions
4.1. Attitudes and Perceptions Regarding COVID-19 Vaccines among People in Africa
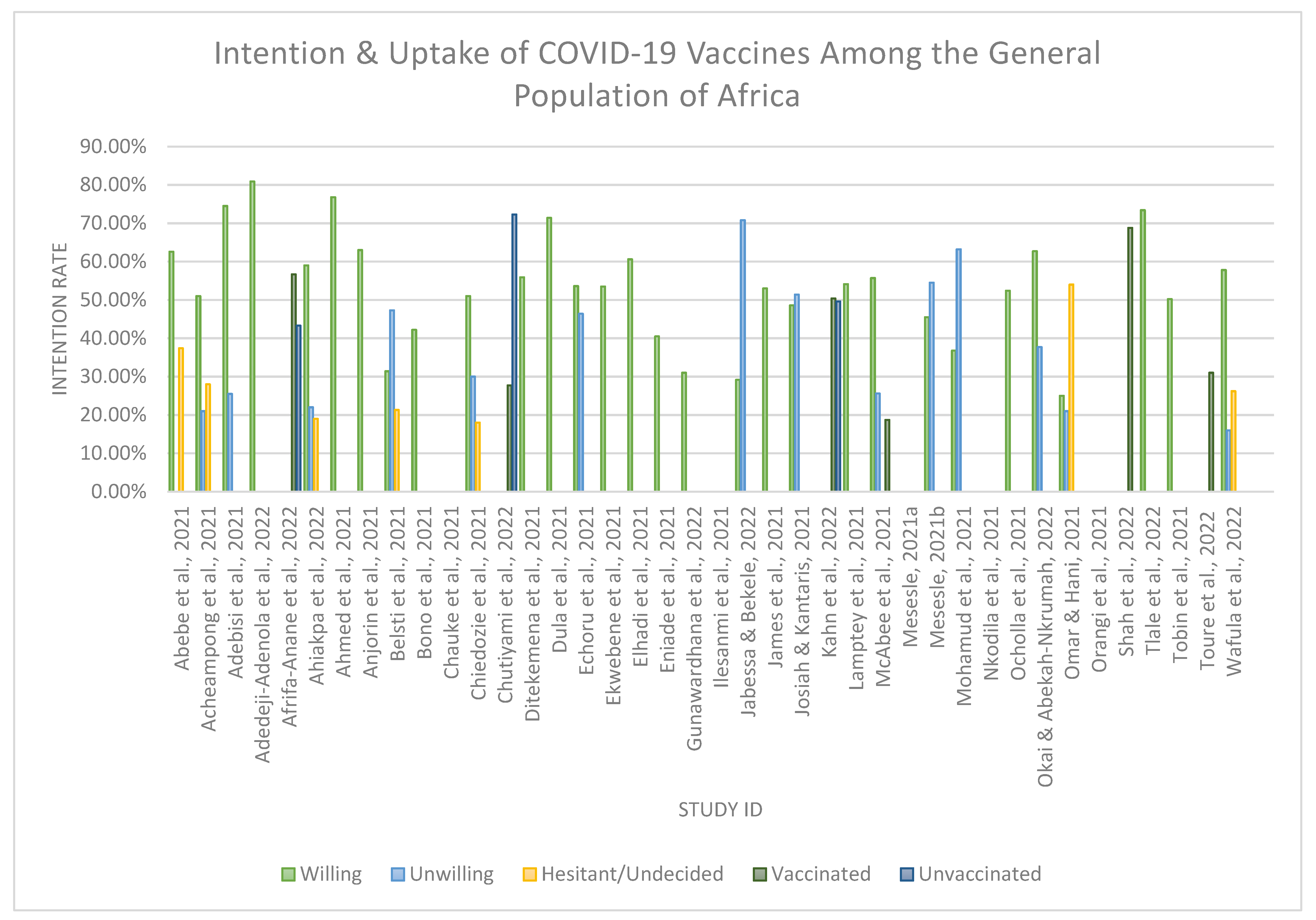
4.2. Intention to Uptake COVID-19 Vaccines
4.3. Factors Associated with COVID-19 Vaccine Uptake
4.4. Barriers to the Uptake of the COVID-19 Vaccine
4.5. Socio-Demographic Determinants Affecting the Intention and Uptake of COVID-19 Vaccines
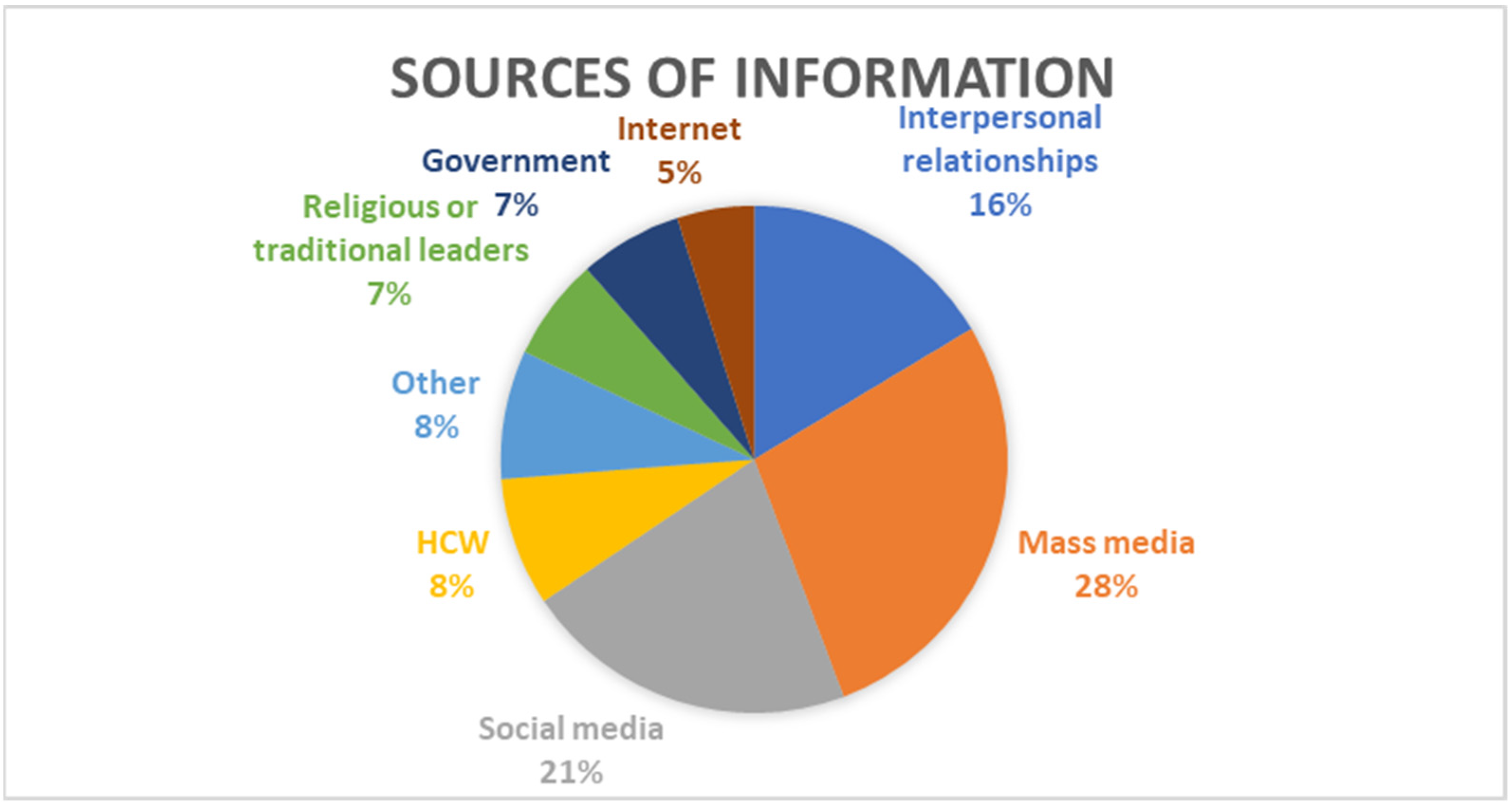
4.6. Information Sources for COVID-19 Vaccines
5. Discussion
Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CDC | Centers for Disease Control and Prevention |
| CHW | Community Healthcare Worker |
| COVID-19 | Coronavirus disease 2019 |
| DRC | Democratic Republic of the Congo |
| GP | General Population |
| HCW | Healthcare Worker |
| HIV/AIDS | Human immunodeficiency virus/acquired immunodeficiency syndrome |
| HPP | Health Promotion Practitioner |
| IDVI | Infectious Disease Vulnerability Index |
| MERS-Cov | Middle East respiratory syndrome coronavirus |
| PRISMA-ScR | Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews |
| SARS-CoV | Severe acute respiratory syndrome |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| TB | Tuberculosis |
| VH | Vaccine Hesitancy |
| VPD | Vaccine-preventable diseases |
| WHO AFRO | World Health Organization African Region |
| WHO | World Health Organization |
Appendix A. Search Strategy

{kind=link}
{kind=link}
{kind=link}
| Search ID# | Search Terms | Search Options | Actions |
|---|---|---|---|
| S5 | (Attitude and perception towards the COVID-19 vaccine) AND SU Africa OR TI (vaccine hesitancy or vaccine refusal or vaccine acceptance or vaccine uptake) | Limiters—Full Text; Published Date: 20200101–20211231; Hidden NetLibrary Holdings Expanders—Apply equivalent subjects Search modes—Boolean/Phrase | (247) |
References
- Al-Jayyousi, G.F.; Sherbash, M.A.; Ali, L.A.; El-Heneidy, A.; Alhussaini, N.W.; Elhassan, M.E.; Nazzal, M.A. Factors Influencing Public Attitudes towards COVID-19 Vaccination: A Scoping Review Informed by the Socio-Ecological Model. Vaccines 2021, 9, 548. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-COV-2 and COVID-19. Nat. Rev. Microbiol. 2020, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Dellino, M.; Cascardi, E.; Vinciguerra, M.; Lamanna, B.; Malvasi, A.; Scacco, S.; Acquaviva, S.; Pinto, V.; Di Vagno, G.; Cormio, G.; et al. Nutrition as Personalized Medicine against SARS-COV-2 Infections: Clinical and Oncological Options with a Specific Female Groups Overview. Int. J. Mol. Sci. 2022, 23, 9136. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; He, Q.; Qian, H.; Liu, J. Overview of the Pathogenesis of COVID-19 (Review). Exp. Ther. Med. 2021, 22, 1011. [Google Scholar] [CrossRef]
- Borczuk, A.C.; Yantiss, R.K. The Pathogenesis of Coronavirus-19 Disease. J. Biomed. Sci. 2022, 29, 87. [Google Scholar] [CrossRef]
- Allagoa, D.O.; Oriji, P.C.; Tekenah, E.S.; Obagah, L.; Njoku, C.; Afolabi, A.S.; Atemie, G. Predictors of Acceptance of COVID-19 Vaccine among Patients at a Tertiary Hospital in South-South Nigeria. Int. J. Community Med. Public Health 2021, 8, 2165. [Google Scholar] [CrossRef]
- Li, Q.; Lu, H. Latest Updates on COVID-19 Vaccines. Biosci. Trends 2020, 14, 463–466. [Google Scholar] [CrossRef]
- Ndwandwe, D.; Wiysonge, C.S. COVID-19 Vaccines. Curr. Opin. Immunol. 2021, 71, 111–116. [Google Scholar] [CrossRef]
- Islam, M.S.; Siddique, A.B.; Akter, R.; Tasnim, R.; Sujan, M.S.; Ward, P.R.; Sikder, M.T. Knowledge, Attitudes and Perceptions towards COVID-19 Vaccinations: A Cross-Sectional Community Survey in Bangladesh. BMC Public Health 2021, 21, 1851. [Google Scholar] [CrossRef]
- World Health Organization AFRO. Omicron-Fuelled COVID-19 Surge in Africa Plateaus. Available online: http://www.afro.who.int/news/omicron-fuelled-covid-19-surge-africa-plateaus (accessed on 28 March 2022).
- Africa Centres for Disease Control and Prevention. Talking Points, Weekly Press Briefing on COVID-19 in Africa. 6 January 2022. Available online: https://africacdc.org/speech/talking-points-weekly-press-briefing-on-covid-19-in-africa-06-january-2022/ (accessed on 22 March 2022).
- Niankara, I.; Muqattash, R.; Niankara, A.; Traoret, R.I. COVID-19 Vaccine Development in a Quadruple Helix Innovation System: Uncovering the Preferences of the Fourth Helix in the UAE. J. Open Innov. Technol. Mark. Complex. 2020, 6, 132. [Google Scholar] [CrossRef]
- Toll, M.; Li, A. Vaccine Sentiments and under-Vaccination: Attitudes and Behaviour around Measles, Mumps, and Rubella Vaccine (MMR) in an Australian Cohort. Vaccine 2021, 39, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Thomson, A.; Vallée-Tourangeau, G.; Suggs, L.S. Strategies to Increase Vaccine Acceptance and Uptake: From Behavioral Insights to Context-Specific, Culturally-Appropriate, Evidence-Based Communications and Interventions. Vaccine 2018, 36, 6457–6458. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Bergen, N.; Kirkby, K.; Fuertes, C.V.; Schlotheuber, A.; Menning, L.; Mac Feely, S.; O’Brien, K.; Hosseinpoor, A.R. Global State of Education-Related Inequality in COVID-19 Vaccine Coverage, Structural Barriers, Vaccine Hesitancy, and Vaccine Refusal: Findings from the Global COVID-19 Trends and Impact Survey. Lancet Glob. Health 2023, 11, e207–e217. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Patwary, M.M.; Alam, M.A.; Bardhan, M.; Disha, A.S.; Haque, M.Z.; Billah, S.M.; Kabir, M.P.; Browning, M.H.; Rahman, M.M.; Parsa, A.D.; et al. COVID-19 Vaccine Acceptance among Low- and Lower-Middle-Income Countries: A Rapid Systematic Review and Meta-Analysis. Vaccines 2022, 10, 427. [Google Scholar] [CrossRef]
- Abu El Kheir-Mataria, W.; Saleh, B.M.; El-Fawal, H.; Chun, S. COVID-19 Vaccine Hesitancy among Parents in Low- and Middle-Income Countries: A Meta-Analysis. Front. Public Health 2023, 11, 1078009. [Google Scholar] [CrossRef]
- Westphaln, K.K.; Regoeczi, W.; Masotya, M.; Vazquez-Westphaln, B.; Lounsbury, K.; McDavid, L.; Lee, H.N.; Johnson, J.; Ronis, S.D. From Arksey and o’Malley and beyond: Customizations to Enhance a Team-Based, Mixed Approach to Scoping Review Methodology. MethodsX 2021, 8, 101375. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Lisy, K.; Porritt, K. Narrative Synthesis. Int. J. Evid.-Based Healthc. 2016, 14, 201. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Bono, S.A.; Faria de Moura Villela, E.; Siau, C.S.; Chen, W.S.; Pengpid, S.; Hasan, M.T.; Sessou, P.; Ditekemena, J.D.; Amodan, B.O.; Hosseinipour, M.C.; et al. Factors Affecting COVID-19 Vaccine Acceptance: An International Survey among Low- and Middle-Income Countries. Vaccines 2021, 9, 515. [Google Scholar] [CrossRef] [PubMed]
- Ahiakpa, J.K.; Cosmas, N.T.; Anyiam, F.E.; Enalume, K.O.; Lawan, I.; Gabriel, I.B.; Oforka, C.L.; Dahir, H.G.; Fausat, S.T.; Nwobodo, M.A.; et al. COVID-19 Vaccines Uptake: Public Knowledge, Awareness, Perception and Acceptance among Adult Africans. PLoS ONE 2022, 17, e0268230. [Google Scholar] [CrossRef] [PubMed]
- Anjorin, A.A.A.; Odetokun, I.A.; Abioye, A.I.; Elnadi, H.; Umoren, M.V.; Damaris, B.F.; Eyedo, J.; Umar, H.I.; Nyandwi, J.B.; Abdalla, M.M.; et al. Will Africans Take COVID-19 Vaccination? PLoS ONE 2021, 16, e0260575. [Google Scholar] [CrossRef]
- Elhadi, M.; Alsoufi, A.; Alhadi, A.; Hmeida, A.; Alshareea, E.; Dokali, M.; Abodabos, S.; Alsadiq, O.; Abdelkabir, M.; Ashini, A.; et al. Knowledge, Attitude, and Acceptance of Healthcare Workers and the Public Regarding the COVID-19 Vaccine: A Cross-Sectional Study. BMC Public Health 2021, 21, 955. [Google Scholar] [CrossRef]
- Gunawardhana, N.; Baecher, K.; Boutwell, A.; Pekwarake, S.; Kifem, M.; Ngong, M.G.; Fondzeyuf, A.; Halle-Ekane, G.; Mbah, R.; Tih, P.; et al. COVID-19 Vaccine Acceptance and Perceived Risk among Pregnant and Non-Pregnant Adults in Cameroon, Africa. PLoS ONE 2022, 17, e0274541. [Google Scholar] [CrossRef] [PubMed]
- Toure, A.A.; Traore, F.A.; Camara, G.; Magassouba, A.S.; Barry, I.; Kourouma, M.L.; Sylla, Y.; Conte, N.Y.; Cisse, D.; Dioubaté, N.; et al. Facilitators and Barriers to COVID-19 Vaccination among Healthcare Workers and the General Population in Guinea. BMC Infect. Dis. 2022, 22, 752. [Google Scholar] [CrossRef] [PubMed]
- Abebe, H.; Shitu, S.; Mose, A. Understanding of COVID-19 Vaccine Knowledge, Attitude, Acceptance, and Determinates of COVID-19 Vaccine Acceptance among Adult Population in Ethiopia. Infect. Drug Resist. 2021, 14, 2015–2025. [Google Scholar] [CrossRef]
- Acheampong, T.; Akorsikumah, E.A.; Osae-Kwapong, J.; Khalid, M.; Appiah, A.; Amuasi, J.H. Examining Vaccine Hesitancy in Sub-Saharan Africa: A Survey of the Knowledge and Attitudes among Adults to Receive COVID-19 Vaccines in Ghana. Vaccines 2021, 9, 814. [Google Scholar] [CrossRef]
- Adebisi, Y.A.; Alaran, A.J.; Bolarinwa, O.A.; Akande-Sholabi, W.; Lucero-Prisno, D.E., III. When It Is Available, Will We Take It? Social Media Users’ Perception of Hypothetical COVID-19 Vaccine in Nigeria. Pan Afr. Med. J. 2021, 38, 230. [Google Scholar] [CrossRef] [PubMed]
- Adedeji-Adenola, H.; Olugbake, O.A.; Adeosun, S.A. Factors Influencing COVID-19 Vaccine Uptake among Adults in Nigeria. PLoS ONE 2022, 17, e0264371. [Google Scholar] [CrossRef] [PubMed]
- Afrifa-Anane, G.F.; Larbi, R.T.; Addo, B.; Agyekum, M.W.; Kyei-Arthur, F.; Appiah, M.; Agyemang, C.O.; Sakada, I.G. Facilitators and Barriers to COVID-19 Vaccine Uptake among Women in Two Regions of Ghana: A Qualitative Study. PLoS ONE 2022, 17, e0272876. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Colebunders, R.; Gele, A.A.; Farah, A.A.; Osman, S.; Guled, I.A.; Abdullahi, A.A.; Hussein, A.M.; Ali, A.M.; Siewe Fodjo, J.N. COVID-19 Vaccine Acceptability and Adherence to Preventive Measures in Somalia: Results of an Online Survey. Vaccines 2021, 9, 543. [Google Scholar] [CrossRef]
- Belsti, Y.; Gela, Y.Y.; Akalu, Y.; Dagnew, B.; Getnet, M.; Abdu Seid, M.; Diress, M.; Yeshaw, Y.; Fekadu, S.A. Willingness of Ethiopian Population to Receive COVID-19 Vaccine. J. Multidiscip. Healthc. 2021, 14, 1233–1243. [Google Scholar] [CrossRef] [PubMed]
- Chauke, T.A.; Obadire, O.S.; Malatji, K.S. Exploring the Perceptions of Youth about COVID-19 and the Use of Vaccine in South Africa. Gend. Behav. 2021, 19, 17099–17115. [Google Scholar]
- Chiedozie, A.P.; Chukwuebuka, O.J.; Chidimma, C.F.; Onyinyechi, O.V.; ChidimChijioke, A.K.; Chibuzor, O.S.; Gabriel, O.C.; Chioma, U.B. Willingness to Accept a Potential COVID-19 Vaccine in Nigeria. Am. J. Med. Sci. Med. 2021, 9, 1–5. [Google Scholar]
- Chutiyami, M.; Salihu, D.; Bello, U.M.; Winser, S.J.; Gambo, A.A.; Sabo, H.; Kolo, A.M.; Jalo, H.A.; Muhammad, A.S.; Mahmud, F.A.; et al. Are Fear of COVID-19 and Vaccine Hesitancy Associated with COVID-19 Vaccine Uptake? A Population-Based Online Survey in Nigeria. Vaccines 2022, 10, 1271. [Google Scholar] [CrossRef] [PubMed]
- Ditekemena, J.D.; Nkamba, D.M.; Mutwadi, A.; Mavoko, H.M.; Siewe Fodjo, J.N.; Luhata, C.; Obimpeh, M.; Van Hees, S.; Nachega, J.B.; Colebunders, R. COVID-19 Vaccine Acceptance in the Democratic Republic of Congo: A Cross-Sectional Survey. Vaccines 2021, 9, 153. [Google Scholar] [CrossRef]
- Dula, J.; Mulhanga, A.; Nhanombe, A.; Cumbi, L.; Júnior, A.; Gwatsvaira, J.; Fodjo, J.N.; Faria de Moura Villela, E.; Chicumbe, S.; Colebunders, R. COVID-19 Vaccine Acceptability and Its Determinants in Mozambique: An Online Survey. Vaccines 2021, 9, 828. [Google Scholar] [CrossRef]
- Echoru, I.; Ajambo, P.D.; Keirania, E.; Bukenya, E.E. Sociodemographic Factors Associated with Acceptance of COVID-19 Vaccine and Clinical Trials in Uganda: A Cross-Sectional Study in Western Uganda. BMC Public Health 2021, 21, 1106. [Google Scholar] [CrossRef]
- Ekwebene, O.C.; Obidile, V.C.; Azubuike, P.C.; Nnamani, C.P.; Dankano, N.E.; Egbuniwe, M.C. COVID-19 Vaccine Knowledge and Acceptability among Healthcare Providers in Nigeria. Int. J. Trop. Dis. Health 2021, 42, 51–60. [Google Scholar] [CrossRef]
- Eniade, O.D.; Olarinmoye, A.; Otovwe, A.; Akintunde, F.E.; Okedare, O.O.; Aniyeloye, A.O. Willingness to Accept COVID-19 Vaccine and Its Determinants among Nigeria Citizens: A Web-Based Cross-Sectional Study. J. Adv. Med. Med. Res. 2021, 33, 13–22. [Google Scholar] [CrossRef]
- Ilesanmi, O.; Afolabi, A.; Uchendu, O. The Prospective COVID-19 Vaccine: Willingness to Pay and Perception of Community Members in Ibadan, Nigeria. PeerJ 2021, 9, e11153. [Google Scholar] [CrossRef] [PubMed]
- Jabessa, D.; Bekele, F. Willingness to Receive the COVID-19 Vaccine and Associated Factors among Residents of Southwestern Ethiopia: A Cross-Sectional Study. Patient Prefer. Adherence 2022, 16, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- James, B.C.; Ede, S.S.; Aroh, C.M.; Kanokwan, C.K.; Rasip, M.L.; Enbeyle, W. Attitudes and Perceptions of Nigerians Regarding Receiving COVID-19 Vaccines: An Online Cross-Sectional Study. Pan Afr. Med. J. 2022, 41, 247. [Google Scholar] [PubMed]
- Josiah, B.O.; Kantaris, M. Perception of COVID-19 and Acceptance of Vaccination in Delta State Nigeria. Niger. Health J. 2021, 21, 60–68. [Google Scholar]
- Kahn, K.; Pettifor, A.; Mataboge, P.; Kelly, N.K.; Mashinini, D.P.; Nair, H.; Campbell, H.; Cohen, C.; Gómez-Olivé, F.X.; Tollman, S. COVID-19 Vaccine Hesitancy in Rural South Africa: Deepening Understanding to Increase Uptake and Access. J. Glob. Health 2022, 12, 05013. [Google Scholar] [CrossRef]
- Lamptey, E.; Serwaa, D.; Appiah, A.B. A Nationwide Survey of the Potential Acceptance and Determinants of COVID-19 Vaccines in Ghana. Clin. Exp. Vaccine Res. 2021, 10, 183. [Google Scholar] [CrossRef]
- McAbee, L.; Tapera, O.; Kanyangarara, M. Factors Associated with COVID-19 Vaccine Intentions in Eastern Zimbabwe: A Cross-Sectional Study. Vaccines 2021, 9, 1109. [Google Scholar] [CrossRef]
- Mesesle, M. Awareness and Attitude towards COVID-19 Vaccination and Associated Factors in Ethiopia: Cross-Sectional Study. Infect. Drug Resist. 2021, 14, 2193–2199. [Google Scholar] [CrossRef]
- Mesele, M. COVID-19 Vaccination Acceptance and Its Associated Factors in Sodo Town, Wolaita Zone, Southern Ethiopia: Cross-Sectional Study. Infect. Drug Resist. 2021, 14, 2361–2367. [Google Scholar] [CrossRef] [PubMed]
- Mohamud, A.I.; Mohamed, S.A.; Jimale, K.A. Assessments of a COVID-19 Vaccine Acceptance Rate in Population of Benadir Region, Somalia. IOSR J. Dent. Med. Sci. (IOSR-JDMS) 2021, 20, 1–4. [Google Scholar]
- Natuhoyila Nkodila, A.; Ngwala Lukanu, P.; Nlombi Mbendi, C.; Marie Tebeu, P.; Saint Antaon Saba, J.; Alex Kabangi Tukadila, H.; Muhala, B.; Lelo Mananga, G.; Cecile Djuikoue, I.; Mokondjimabe, E.; et al. Perception of the Congolese Population on COVID-19 Vaccination: Cross-Sectional Survey of Online. Int. J. Vaccines Vaccin. 2021, 6, 12–19. [Google Scholar] [CrossRef]
- Ocholla, B.A.; Nyangena, O.; Murayi, H.K.; Mwangi, J.W.; Belle, S.K.; Ondeko, P.; Kendagor, R. Association of Demographic and Occupational Factors with SARS-CoV-2 Vaccine Uptake in Kenya. OALib 2021, 8, e7424. [Google Scholar] [CrossRef]
- Okai, G.A.; Abekah-Nkrumah, G. The Level and Determinants of COVID-19 Vaccine Acceptance in Ghana. PLoS ONE 2022, 17, e0270768. [Google Scholar] [CrossRef]
- Omar, D.I.; Hani, B.M. Attitudes and Intentions towards COVID-19 Vaccines and Associated Factors among Egyptian Adults. J. Infect. Public Health 2021, 14, 1481–1488. [Google Scholar] [CrossRef]
- Orangi, S.; Pinchoff, J.; Mwanga, D.; Abuya, T.; Hamaluba, M.; Warimwe, G.; Austrian, K.; Barasa, E. Assessing the Level and Determinants of COVID-19 Vaccine Confidence in Kenya. Vaccines 2021, 9, 936. [Google Scholar] [CrossRef]
- Shah, J.; Abeid, A.; Sharma, K.; Manji, S.; Nambafu, J.; Korom, R.; Patel, K.; Said, M.; Mohamed, M.A.; Sood, M.; et al. Perceptions and Knowledge towards COVID-19 Vaccine Hesitancy among a Subpopulation of Adults in Kenya: An English Survey at Six Healthcare Facilities. Vaccines 2022, 10, 705. [Google Scholar] [CrossRef]
- Tlale, L.B.; Gabaitiri, L.; Totolo, L.K.; Smith, G.; Puswane-Katse, O.; Ramonna, E.; Mothowaeng, B.; Tlhakanelo, J.; Masupe, T.; Rankgoane-Pono, G.; et al. Acceptance Rate and Risk Perception towards the COVID-19 Vaccine in Botswana. PLoS ONE 2022, 17, e0263375. [Google Scholar] [CrossRef]
- Tobin, E.A.; Okonofua, M.; Adeke, A.; Obi, A. Willingness to Accept a COVID-19 Vaccine in Nigeria: A Population-Based Cross-Sectional Study. Cent. Afr. J. Public Health 2021, 7, 53. [Google Scholar] [CrossRef]
- Wafula, S.T.; Mugume, I.B.; Sensasi, B.; Okware, S.; Chimbaru, A.; Nanyunja, M.; Talisuna, A.; Kabanda, R.; Bakyaita, T.; Wanyenze, R.K.; et al. Intention to Vaccinate against COVID-19 and Adherence to Non-Pharmaceutical Interventions against COVID-19 Prior to the Second Wave of the Pandemic in Uganda: A Cross-Sectional Study. BMJ Open 2022, 12, e057322. [Google Scholar] [CrossRef] [PubMed]
- Sekiguchi, T.; Nakamaru, M. How Inconsistency between Attitude and Behavior Persists through Cultural Transmission. J. Theor. Biol. 2011, 271, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Stangor, C.; Jhangiani, R.; Tarry, H. Principles of Social Psychology; BCcampus Open Publishing: Victoria, BC, Canada, 2022. [Google Scholar]
- Frymier, A.B.; Nadler, M.K. Persuasion: Integrating Theory, Research, and Practice; Kendall Hunt Publishing: Dubuque, IA, USA, 2007; pp. 42–58. [Google Scholar]
- Ajzen, I.; Fishbein, M. The Handbook of Attitudes; Albarracín, D., Johnson, B.T., Zanna, M.P., Eds.; Psychology Press: Mahwah, NJ, USA, 2018; pp. 173–221. [Google Scholar]
- World Health Organization AFRO. African Vaccination Week 2021-‘Vaccines Bring Us Closer’. Available online: https://www.afro.who.int/media-centre/events/african-vaccination-week-2021-vaccines-bring-us-closer (accessed on 28 March 2022).
- Bai, L.; Zhao, Y.; Dong, J.; Liang, S.; Guo, M.; Liu, X.; Wang, X.; Huang, Z.; Sun, X.; Zhang, Z.; et al. Coinfection with Influenza A Virus Enhances SARS-CoV-2 Infectivity. Cell Res. 2021, 31, 395–403. [Google Scholar] [CrossRef]
- Petravić, L.; Arh, R.; Gabrovec, T.; Jazbec, L.; Rupčić, N.; Starešinič, N.; Zorman, L.; Pretnar, A.; Srakar, A.; Zwitter, M.; et al. Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia. Vaccines 2021, 9, 247. [Google Scholar] [CrossRef]
- Nzaji, M.K.; Ngombe, L.K.; Mwamba, G.N.; Ndala, D.B.; Miema, J.M.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.; Musenga, E.M. Acceptability of Vaccination against COVID-19 among Healthcare Workers in the Democratic Republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Fares, S.; Elmnyer, M.M.; Mohamed, S.S.; Elsayed, R. COVID-19 Vaccination Perception and Attitude among Healthcare Workers in Egypt. J. Prim. Care Community Health 2021, 12, 215013272110133. [Google Scholar] [CrossRef]
- Eniola, K.; Sykes, J. Four Reasons for COVID-19 Vaccine Hesitancy among Health Care Workers, and Ways to Counter Them. Available online: https://www.aafp.org/journals/fpm/blogs/inpractice/entry/countering_vaccine_hesitancy.html (accessed on 5 May 2022).
- Agyekum, M.W.; Afrifa-Anane, G.F.; Kyei-Arthur, F.; Addo, B. Acceptability of COVID-19 Vaccination among Health Care Workers in Ghana. Adv. Public Health 2021, 2021, 9998176. [Google Scholar] [CrossRef]
- Hernandez, R.G.; Hagen, L.; Walker, K.; O’Leary, H.; Lengacher, C. The COVID-19 vaccine social media infodemic: Healthcare providers’ missed dose in addressing misinformation and vaccine hesitancy. Hum. Vaccines Immunother. 2021, 17, 2962–2964. [Google Scholar] [CrossRef]
- Magadmi, R.M.; Kamel, F.O. Beliefs and Barriers Associated with COVID-19 Vaccination among the General Population in Saudi Arabia. BMC Public Health 2021, 21, 1438. [Google Scholar] [CrossRef]
- Aroh, A.; Asaolu, B.; Okafor, C.T. Myths and Models: What’s Driving Vaccine Hesitancy in Africa and How Can We Overcome It? Available online: https://www.africaportal.org/features/myths-and-models-whats-driving-vaccine-hesitancy-in-africa-and-how-can-we-overcome-it/ (accessed on 31 March 2022).
- Akwataghibe, N.N.; Ogunsola, E.A.; Broerse, J.E.; Popoola, O.A.; Agbo, A.I.; Dieleman, M.A. Exploring factors influencing immunization utilization in Nigeria—A mixed methods study. Front. Public Health 2019, 7, 392. [Google Scholar] [CrossRef] [PubMed]
- Carson, S.L.; Casillas, A.; Castellon-Lopez, Y.; Mansfield, L.N.; Morris, D.A.; Barron, J.; Ntekume, E.; Landovitz, R.; Vassar, S.D.; Norris, K.C.; et al. COVID-19 vaccine decision-making factors in racial and ethnic minority communities in Los Angeles, California. JAMA Netw. Open 2021, 4, e2127582. [Google Scholar] [CrossRef] [PubMed]
- Massinga Loembé, M.; Nkengasong, J.N. COVID-19 vaccine access in Africa: Global distribution, vaccine platforms, and challenges ahead. Immunity 2021, 54, 1353–1362. [Google Scholar] [CrossRef] [PubMed]
- Sturgis, P.; Brunton-Smith, I.; Jackson, J. Trust in science, social consensus and Vaccine Confidence. Nat. Hum. Behav. 2021, 5, 1528–1534. [Google Scholar] [CrossRef] [PubMed]
- Milošević Đorđević, J.; Mari, S.; Vdović, M.; Milošević, A. Links between conspiracy beliefs, vaccine knowledge, and trust: Anti-vaccine behavior of Serbian adults. Soc. Sci. Med. 2021, 277, 113930. [Google Scholar] [CrossRef] [PubMed]
- Hausenkamph, D.S. Vaccine Hesitancy, Institutional Mistrust and Corruption in Sub-Saharan Africa: Everything Is Connected. Available online: https://www.u4.no/blog/vaccine-hesitancy-institutional-mistrust-sub-saharan-africa (accessed on 31 March 2022).
- Mills, M.; Rahal, C.; Brazel, D.; Yan, J.; Gieysztor, S. COVID-19 Vaccine Deployment: Behaviour, Ethics, Misinformation and Policy Strategies; The Royal Society & The British Academy: London, UK, 2020; pp. 1–35. Available online: https://royalsociety.org/-/media/policy/projects/set-c/set-c-vaccine-deployment.pdf (accessed on 5 May 2021).
- Hogg, M.A.; Cooper, J. The SAGE Handbook of Social Psychology: Concise Student Edition; SAGE Publications Ltd.: London, UK, 2007. [Google Scholar] [CrossRef]
- Enea, V.; Eisenbeck, N.; Carreno, D.F.; Douglas, K.M.; Sutton, R.M.; Agostini, M.; Bélanger, J.J.; Gützkow, B.; Kreienkamp, J.; Abakoumkin, G.; et al. Intentions to be vaccinated against COVID-19: The role of prosociality and conspiracy beliefs across 20 countries. Health Commun. 2022, 1–10. [Google Scholar] [CrossRef]



| Country of Focus | Number of Studies |
|---|---|
| Ethiopia | 5 |
| Ghana | 4 |
| Nigeria | 10 |
| Multiple African Countries | 3 |
| Somalia | 2 |
| South Africa | 2 |
| DRC | 2 |
| Mozambique | 1 |
| Uganda | 2 |
| Libya | 1 |
| Cameroon | 1 |
| Zimbabwe | 1 |
| Kenya | 3 |
| Egypt | 1 |
| Botswana | 1 |
| Guinea | 1 |
| Author(s) and Publication Year | Country and Data Collection Period | Methodology | Willing | Refusal | Hesitant/Undecided | Vaccinated | Unvaccinated |
|---|---|---|---|---|---|---|---|
| Abebe et al., 2021 [31] | Ethiopia March 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 492 | 62.6% | 37.4% | |||
| Acheampong et al., 2021 [32] | Ghana February 2021 | Study design: A quantitative cross-sectional study Population target: General population Sample size: 2345 | 51% | 21% | 28% | ||
| Adebisi et al., 2021 [33] | Nigeria August 2020 | Study design: A quantitative cross-sectional study Population target: General population Sample size: 517 | 74.5% | 25.5% | |||
| Adedeji-Adenola et al., 2022 [34] | Nigeria April to June 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 1058 | 80.9% | ||||
| Afrifa-Anane et al., 2022 [35] | Ghana October to November 2021 | Study design: A cross-sectional descriptive qualitative design Population target: General Population–Women Sample size: 30 | 56.7% | 43.3% | |||
| Ahiakpa et al., 2022 [26] | 17 African countries December 2020 to March 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 365 | 59% | 22% | 19% | ||
| Ahmed et al., 2021 [36] | Somalia December 2020 to January 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 4543 | 76.8% | ||||
| Anjorin et al., 2021 [27] | Multiple African countries February to March 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 5416 | 63% | ||||
| Belsti et al., 2021 [37] | Ethiopia February to March 2021 | Study design: A quantitative study Population target: General adult population (aged ≥ 18 years) Sample size: 1184 | 31.4% | 47.3% | 21.3% | ||
| Bono et al., 2021 [25] | Multiple African countries December 2020 to February 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 621 | 42.2% | ||||
| Chauke et al., 2021 [38] | South Africa | Study design: A qualitative study Population target: General population-Youth (18–35 years) Sample size: 14 | |||||
| Chiedozie et al., 2021 [39] | Nigeria | Study design: A quantitative study Population target: General adult population (aged ≥ 18 years) Sample size: 499 | 51% | 30% | 18% | ||
| Chutiyami et al., 2022 [40] | Nigeria October to December 2021 | Study design: A quantitative population-based study Population target: General population Sample size: 577 | 27.7% | 72.3% | |||
| Ditekemena et al., 2021 [41] | The Democratic Republic of Congo August 2020 to September 2020 | Study design: A quantitative cross-sectional study Population target: General population Sample size: 4160 | 55.9% | ||||
| Dula et al., 2021 [42] | Mozambique March 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 1878 | 71.4% | ||||
| Echoru et al., 2021 [43] | Uganda July to September 2020 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 1067 | 53.6% | 46.4% | |||
| Ekwebene et al., 2021 [44] | Nigeria | Study design: A quantitative study Population target: General adult population (aged ≥ 18 years) Sample size: 445 | 53.5% | ||||
| Elhadi et al., 2021 [28] | Libya December 2020 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) (including medical students and HCW) Sample size: GP-11120 | 60.6% | ||||
| Eniade et al., 2021 [45] | Nigeria December 2020 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 368 | 40.5% | ||||
| Gunawardhana et al., 2022 [29] | Cameroon 1 June 2021 to 14 July 2021 | Study design: A quantitative cross-sectional study Population target: Pregnant women and general population Sample size: GP-448 | 31% | ||||
| Ilesanmi et al., 2021 [46] | Nigeria September 2020 | Study design: A quantitative cross-sectional study Population target: General population Sample size: 440 | |||||
| Jabessa and Bekele, 2022 [47] | Ethiopia August 1st to September 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 350 | 29.2% | 70.8% | |||
| James et al., 2021 [48] | Nigeria July to August 2022 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 334 | 53% | ||||
| Josiah and Kantaris, 2021 [49] | Nigeria December 2020 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 410 | 48.6% | 51.4% | |||
| Kahn et al., 2022 [50] | South Africa 25 August 2021 to 29 October 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 1662 | 50.4% | 49.6% | |||
| Lamptey et al., 2021 [51] | Ghana October to December 2020 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 1000 | 54.1% | ||||
| McAbee et al., 2021 [52] | Zimbabwe May 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 551 | 55.7% | 25.6% | 18.7% | ||
| Mesesle, 2021a [53] | Ethiopia March to April 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 425 | |||||
| Mesesle, 2021b [54] | Ethiopia April 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 415 | 45.5% | 54.5% | |||
| Mohamud et al., 2021 [55] | Somalia October to December 2020 | Study design: A quantitative cross-sectional study Population target: General population Sample size: 500 | 36.8% | 63.2% | |||
| Natuhoyila et al., 2021 [56] | The Democratic Republic of Congo January to March 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 11,971 | |||||
| Ocholla et al., 2021 [57] | Kenya March 2021 | Study design: A quantitative cross-sectional study Population target: General population Sample size: 171 | 52.4% | ||||
| Okai and Abekah-Nkrumah, 2022 [58] | Ghana 18 May 2021 to 14 July 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 362 | 62.7% | 37.7% | |||
| Omar and Hani, 2021 [59] | Egypt January to March 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 1011 | 25% | 21% | 54% | ||
| Orangi et al., 2021 [60] | Kenya February 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 4136 | |||||
| Shah et al., 2022 [61] | Kenya November 2021 to January 2022 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 3996 | 68.8% | ||||
| Tlale et al., 2022 [62] | Botswana 1 February 2021 to 28 February 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 5300 | 73.4% | ||||
| Tobin et al., 2021 [63] | Nigeria July 2020 to August 2020 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 1228 | 50.2% | ||||
| Toure et al., 2022 [30] | Guinea 23 March 2021 to 25 August 2021 | Study design: A mixed method cross-sectional study Population target: General adult population (aged ≥ 18 years) and HCW Sample size: GP–3663 | 31% | ||||
| Wafula et al., 2022 [64] | Uganda March 2021 | Study design: A quantitative cross-sectional study Population target: General adult population (aged ≥ 18 years) Sample size: 1053 | 57.8% | 16% | 26.2% |
| Country and Study ID | Attitudes and Perceptions towards COVID-19 Vaccines | Reasons for Acceptance/ Non-Acceptance | Determinants Affecting the Vaccine-Related Outcome (Significantly Associated) | Information Sources for COVID-19 Vaccines |
|---|---|---|---|---|
| Ethiopia [31] | Negative attitude | Acceptance: Age (≥46 years) Education level (secondary and above) Presence of comorbidities Having a good knowledge of COVID-19 | Interpersonal relationships Mass media Social media Internet | |
| Ghana [32] | Hesitant attitude | Acceptance: Desire to protect people Confidence in the COVID-19 vaccines A public health responsibility Awareness of possible side effects Non-acceptance: Safety concerns Perceived lack of information Effectiveness concerns Vaccine inaccessibility | Acceptance: Gender (female) Age (older) | Mass media Social media Interpersonal relationships Other |
| Nigeria [33] | Non-acceptance: Perceived scientific uncertainty Belief in one’s immune system Safety concerns | Acceptance: Age Geographical region Non-acceptance: Age Education level | ||
| Nigeria [34] | Positive perception | Non-acceptance: Safety concerns | Acceptance: Education level (diploma and above) Prior diagnosis of COVID | Mass media Social media HCWs Interpersonal relationships Other |
| Ghana [35] | Acceptance: Desire to protect people Increased education about COVID-19 vaccines Observing others get the COVID-19 vaccine Vaccines are available free of charge Receiving a vaccination certificate Non-acceptance: Vaccine inaccessibility Safety concerns Subscribing to misinformation or conspiracies | |||
| 17 African countries [26] | Negative perception | Acceptance: Prior diagnosis of COVID Having a positive perception towards the COVID-19 vaccine Non-acceptance: Subscribing to misinformation or conspiracies | Social media Mass media Interpersonal relationships Religious or traditional leaders Other | |
| Somalia [36] | Non-acceptance: Effectiveness concerns Safety concerns Belief in one’s immune system Doubts about the seriousness of the pandemic | Non-acceptance: Gender (female) | ||
| Multiple African countries [27] | Non-acceptance: Safety concerns Preferred alternative treatment to the COVID-19 vaccine | Non-acceptance: Age (older) Gender (female) Employment status Income level Residence (urban area) Negative experience with vaccines | HCWs Mass media Government Religious or traditional leaders Other | |
| Ethiopia [37] | Hesitant attitude | Non-acceptance: Safety concerns | Acceptance: Gender (female) Age (<30) Marital status Residence Occupation Religion (Muslim) Education level (tertiary) | |
| Multiple African countries [25] | ||||
| South Africa [38] | Opposing attitudes | Acceptance: Desire to protect people To return to normality Non-acceptance: Lack of trust in stakeholders | ||
| Nigeria [39] | Hesitant attitude | Acceptance: Confidence in COVID-19 vaccines Non-acceptance Subscribing to misinformation or conspiracies | ||
| Nigeria [40] | Non-acceptance: Safety concerns Effectiveness concerns Negative experience with vaccines | Non-acceptance: Safety concerns Perceived scientific uncertainty Effectiveness concerns Negative experience with vaccines | ||
| The Democratic Republic of Congo [41] | Non-acceptance: Subscribing to misinformation or conspiracies Safety concerns Effectiveness concerns | Acceptance: Income level (middle-and high-level) Prior diagnosis of COVID | Interpersonal relationships Mass media Religious or traditional leaders Social media | |
| Mozambique [42] | Acceptance: Confidence in COVID-19 Vaccines Non-acceptance: Effectiveness concerns Safety concerns Subscribing to misinformation or conspiracies | |||
| Uganda [43] | Non-acceptance: Safety concerns | Acceptance Age (18–20 years) Education level (primary) Occupation Religion (Christian) Marital status (married) Residence (rural area) Income level | ||
| Nigeria [44] | Hesitant attitude | Non-acceptance: Safety concerns Religious beliefs Acceptance: Confidence in COVID-19 vaccines | ||
| Libya [28] | Positive attitude | Acceptance: Confidence in the COVID-19 vaccines Non-acceptance: Subscribing to misinformation or conspiracies | Acceptance: Age (31–50 years) Marital status (married) Geographical region Prior diagnosis of COVID Knowing someone who tested positive for COVID Efficacy of 70% and above Non-acceptance: Loss of someone to COVID-19 | Mass media Social media Internet |
| Nigeria [45] | Non-acceptance: Lack of trust in stakeholders Safety concerns | Acceptance: High perceived susceptibility to contracting COVID Age (≥40) | Social media Mass media Interpersonal relationships | |
| Cameroon [29] | Hesitant attitude | Non-acceptance: Safety concerns Effectiveness concerns Perceived lack of information Subscribing to misinformation or conspiracies Acceptance: Receiving COVID-19 vaccines from an African country | Acceptance: Being a parent Education level (secondary) | HCWs Social media Mass media Interpersonal relationships Government Religious or traditional leaders Other |
| Nigeria [46] | Positive perception | Mass media Social media | ||
| Ethiopia [47] | Acceptance: Age (≥50) Income level (low) Low perception level towards COVID-19 vaccines Employment status (unemployed) low level of acceptance of COVID-19 vaccines Unwilling to test for COVID Education level (low) | |||
| Nigeria [48] | Positive attitude and negative perception | Non-acceptance: Safety concerns | Acceptance: Age (older) Gender Education level Marital status | |
| Nigeria [49] | Non-acceptance: Doubts about the seriousness of the pandemic Receiving COVID-19 vaccines from a Western/European country Perceived scientific uncertainty Acceptance: Receiving COVID-19 vaccines from an African country Receiving COVID-19 vaccines from a Muslim country | Acceptance: Gender Education level Religious beliefs Employment status Income level High perceived susceptibility to contracting COVID Trust in stakeholders | ||
| South Africa [50] | Non-acceptance: Perceived lack of information Safety concerns Vaccine inaccessibility | Acceptance: Age (older) Confidence in the COVID-19 vaccines | ||
| Ghana [51] | Acceptance: Age Marital status Education level Occupation | |||
| Zimbabwe [52] | Acceptance: Practising COVID-19 prevention measures Confidence in the COVID-19 vaccines The COVID-19 vaccines are being recommended by the Ministry of Health and World Health Organisation Vaccines are available free of charge Vaccine accessibility Education level (secondary and tertiary) Gender (male) | |||
| Ethiopia [53] | Positive attitude and negative perception | Mass media | ||
| Ethiopia [54] | Non-acceptance: Perceived lack of information Safety concerns Acceptance: Access to the media | Acceptance: Gender Education level Use of mass media Received childhood vaccines Knowing someone who tested positive for COVID | Mass media | |
| Somalia [55] | Negative attitude | Non-acceptance: Safety concerns Effectiveness concerns Perceived scientific uncertainty | ||
| The Democratic Republic of Congo [56] | Negative perception | Non-acceptance: Effectiveness concerns Safety concerns Subscribing to misinformation or conspiracies | ||
| Kenya [57] | Non-acceptance: Safety concerns | Acceptance: Occupation | Mass media Social media HCWs Interpersonal relationships | |
| Ghana [58] | Non-acceptance: Safety concerns Perceived scientific uncertainty Low perceived susceptibility to contracting COVID | |||
| Egypt [59] | Negative attitude | Non-acceptance: Safety concerns | Non-acceptance: Gender (female) Residence (urban area) Education level (tertiary) Marital status (married) Rejected flu vaccines in the past Lack of trust in stakeholders | |
| Kenya [60] | Hesitant attitude | Acceptance: High perceived susceptibility to contracting COVID Non-acceptance: Safety concerns Effectiveness concerns Religious beliefs | Non-acceptance: Residence (rural area) Safety concerns Effectiveness concerns Vaccine inaccessibility Religious beliefs | |
| Kenya [61] | Non-acceptance: Safety concerns | |||
| Botswana [62] | Non-acceptance: Perceived scientific uncertainty Safety concerns | Acceptance: Gender (male) Age (55–64 years) Education level (primary) Willingness to wear a mask Employment status Presence of comorbidities | Mass media Social media Internet Government | |
| Nigeria [63] | Acceptance: Self-protection Desire to protect people COVID-19 vaccines are being recommended by HCWs Presence of chronic illness Non-acceptance: Safety concerns Effectiveness concerns Doubts about the seriousness of the pandemic Afraid of needles | Acceptance: Age (≥24 years) Religion (Muslim) Gender (male) Trust in stakeholders Willing to pay and travel for the COVID-19 vaccine Vaccinating during an outbreak | Social media Internet Mass media HCWs Interpersonal relationships | |
| Guinea [30] | Negative perception | Non-acceptance: Having a negative perception towards the COVID-19 vaccine Lack of trust in stakeholders Safety concerns | Acceptance: Marital status (single) Education level Non-pregnant women Confidence in the COVID-19 vaccines Age Vaccine eligibility Non-acceptance: Higher vaccine knowledge Having a negative attitude toward the COVID-19 vaccine | Mass media Social media Interpersonal relationships Government |
| Uganda [64] | Non-acceptance: Safety concerns Effectiveness concerns Perceived lack of information Low perceived susceptibility to contracting COVID Prior diagnosis of COVID Belief in one’s immune system | Acceptance: Geographical region Age (55–64 years) High perceived susceptibility to contracting COVID Developing severe disease and side effects | Mass media |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naidoo, D.; Meyer-Weitz, A.; Govender, K. Factors Influencing the Intention and Uptake of COVID-19 Vaccines on the African Continent: A Scoping Review. Vaccines 2023, 11, 873. https://doi.org/10.3390/vaccines11040873
Naidoo D, Meyer-Weitz A, Govender K. Factors Influencing the Intention and Uptake of COVID-19 Vaccines on the African Continent: A Scoping Review. Vaccines. 2023; 11(4):873. https://doi.org/10.3390/vaccines11040873
Chicago/Turabian StyleNaidoo, Damian, Anna Meyer-Weitz, and Kaymarlin Govender. 2023. "Factors Influencing the Intention and Uptake of COVID-19 Vaccines on the African Continent: A Scoping Review" Vaccines 11, no. 4: 873. https://doi.org/10.3390/vaccines11040873