
Using Electronic Reminders to Improve Human Papillomavirus (HPV) Vaccinations among Primary Care Patients
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Ethics Approval and Consent
2.2. Study Population
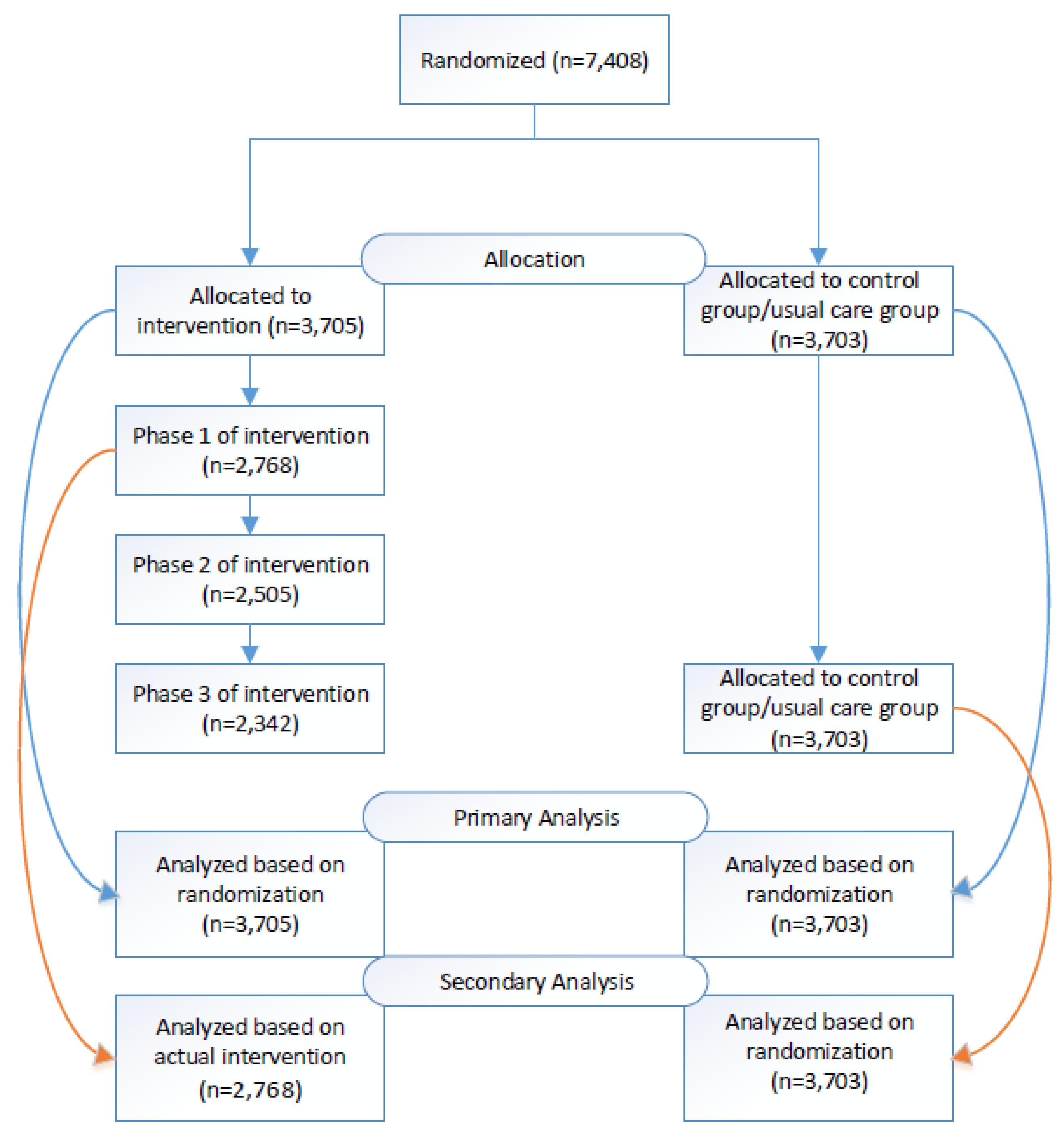
2.3. Randomization
2.4. Study Intervention and Usual Care Group
2.5. Intervention Period
2.6. Study Measures and Data collection
2.7. Analysis
3. Results
3.1. Patient Demographics
3.2. Appointment Scheduling and Clinic Visit
3.3. HPV Vaccination Rates
Secondary Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Senkomago, V.; Henley, S.J.; Thomas, C.C.; Mix, J.M.; Markowitz, L.E.; Saraiya, M. Human Papillomavirus–Attributable Cancers—United States, 2012–2016. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 724–728. [Google Scholar] [CrossRef]
- Drolet, M.; Bénard, É.; Pérez, N.; Brisson, M.; Ali, H.; Boily, M.-C.; Baldo, V.; Brassard, P.; Brotherton, J.M.L.; Callander, D.; et al. Population-Level Impact and Herd Effects Following the Introduction of Human Papillomavirus Vaccination Programmes: Updated Systematic Review and Meta-Analysis. Lancet 2019, 394, 497–509. [Google Scholar] [CrossRef] [PubMed]
- CDC. HPV Vaccine Safety and Effectiveness. Available online: https://www.cdc.gov/vaccines/vpd/hpv/hcp/safety-effectiveness.html (accessed on 17 March 2023).
- CDC. HPV Vaccination: What Everyone Should Know. Available online: https://www.cdc.gov/vaccines/vpd/hpv/public/index.html (accessed on 17 March 2023).
- O’Leary, S.T. Why the American Academy of Pediatrics Recommends Initiating HPV Vaccine at Age 9. Hum. Vaccines Immunother. 2022, 18, 2146434. [Google Scholar] [CrossRef] [PubMed]
- Saslow, D.; Andrews, K.S.; Manassaram-Baptiste, D.; Smith, R.A.; Fontham, E.T.H.; The American Cancer Society Guideline Development Group. Human Papillomavirus Vaccination 2020 Guideline Update: American Cancer Society Guideline Adaptation. CA Cancer J. Clin. 2020, 70, 274–280. [Google Scholar] [CrossRef] [PubMed]
- CDC. HPV Vaccination Recommendations. Available online: https://www.cdc.gov/vaccines/vpd/hpv/hcp/recommendations.html (accessed on 5 January 2023).
- Czeisler, M.É. Delay or Avoidance of Medical Care Because of COVID-19–Related Concerns—United States, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef]
- CMS. Issues Urgent Call to Action Following Drastic Decline in Care for Children in Medicaid and Children’s Health Insurance Program Due to COVID-19 Pandemic | CMS. Available online: https://www.cms.gov/newsroom/press-releases/cms-issues-urgent-call-action-following-drastic-decline-care-children-medicaid-and-childrens-health (accessed on 23 December 2022).
- Santoli, J.M. Effects of the COVID-19 Pandemic on Routine Pediatric Vaccine Ordering and Administration—United States, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Patel Murthy, B.; Zell, E.; Kirtland, K.; Jones-Jack, N.; Harris, L.; Sprague, C.; Schultz, J.; Le, Q.; Bramer, C.A.; Kuramoto, S.; et al. Impact of the COVID-19 Pandemic on Administration of Selected Routine Childhood and Adolescent Vaccinations—10 U.S. Jurisdictions, March–September 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Ryan, G.; Gilbert, P.A.; Ashida, S.; Charlton, M.E.; Scherer, A.; Askelson, N.M. Challenges to Adolescent HPV Vaccination and Implementation of Evidence-Based Interventions to Promote Vaccine Uptake During the COVID-19 Pandemic: “HPV Is Probably Not at the Top of Our List”. Prev. Chronic Dis. 2022, 19, 210378. [Google Scholar] [CrossRef]
- Tsui, J.; Martinez, B.; Shin, M.B.; Allee-Munoz, A.; Rodriguez, I.; Navarro, J.; Thomas-Barrios, K.R.; Kast, W.M.; Baezconde-Garbanati, L. Understanding Medical Mistrust and HPV Vaccine Hesitancy among Multiethnic Parents in Los Angeles. J. Behav. Med. 2023, 46, 100–115. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Albertin, C.S.; Gurfinkel, D.; Saville, A.W.; Vangala, S.; Rice, J.D.; Helmkamp, L.; Zimet, G.D.; Valderrama, R.; Breck, A.; et al. Prevalence and Characteristics of HPV Vaccine Hesitancy among Parents of Adolescents across the US. Vaccine 2020, 38, 6027–6037. [Google Scholar] [CrossRef] [PubMed]
- Office of Disease Prevention and Health Promotion, Office of the Assistant Secretary for Health, Office of the Secretary, U.S. Department of Health and Human Services. Increase the Proportion of Adolescents Who Get Recommended Doses of the HPV Vaccine—IID-08—Healthy People 2030 | Health.Gov. Available online: https://health.gov/healthypeople/objectives-and-data/browse-objectives/vaccination/increase-proportion-adolescents-who-get-recommended-doses-hpv-vaccine-iid-08 (accessed on 5 January 2023).
- ACS. HPV Vaccination Project Texas HPV Vaccination Landscape Dashboard. Available online: https://public.tableau.com/app/profile/acs.hpv.vaccination/viz/TexasHPVVaccinationLandscapeDashboard/Dashboard1 (accessed on 5 January 2023).
- ACS. HPV Vaccination Project HPV Landscape Dashboard. Available online: https://public.tableau.com/app/profile/acs.hpv.vaccination/viz/HPVLandscapeDashboard-November2019/Dashboard (accessed on 5 January 2023).
- Gilkey, M.B.; McRee, A.-L. Provider Communication about HPV Vaccination: A Systematic Review. Hum. Vaccines Immunother. 2016, 12, 1454–1468. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, A.C.; Madden, C.A.; Thompson, D.M.; Garbe, M.C.; Roberts, J.R.; Jacobson, R.M.; Darden, P.M. The Impact of Provider Recommendation on Human Papillomavirus Vaccine and Other Adolescent Vaccines. Hum. Vaccines Immunother. 2021, 17, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, S.L.; Weiss, T.W.; Zimet, G.D.; Ma, L.; Good, M.B.; Vichnin, M.D. Predictors of HPV Vaccine Uptake among Women Aged 19–26: Importance of a Physician’s Recommendation. Vaccine 2011, 29, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Kester, L.M.; Zimet, G.D.; Fortenberry, J.D.; Kahn, J.A.; Shew, M.L. A National Study of HPV Vaccination of Adolescent Girls: Rates, Predictors, and Reasons for Non-Vaccination. Matern. Child Health J. 2013, 17, 879–885. [Google Scholar] [CrossRef]
- Gargano, L.M.; Herbert, N.L.; Painter, J.E.; Sales, J.M.; Morfaw, C.; Rask, K.; Murray, D.; DiClemente, R.J.; Hughes, J.M. Impact of a Physician Recommendation and Parental Immunization Attitudes on Receipt or Intention to Receive Adolescent Vaccines. Vaccines 2013, 9, 2627–2633. [Google Scholar] [CrossRef]
- Fisher, L.; Loiacono, M.M.; Payne, N.; Kelley, T.; Greenberg, M.; Charpentier, M.; Leblanc, C.; Sundaresan, D.; Bancroft, T.; Steffens, A.; et al. A Novel Household-based Patient Outreach Pilot Program to Boost Late-season Influenza Vaccination Rates during the COVID-19 Pandemic. Influenza Respir. Viruses 2022, 16, 1141–1150. [Google Scholar] [CrossRef]
- CDC. The Top 10 Tips for HPV Vaccination Success. Available online: https://www.cdc.gov/hpv/downloads/Top10-improving-practice.pdf (accessed on 3 February 2023).
- Pich, J. Patient Reminder and Recall Interventions to Improve Immunization Rates: A Cochrane Review Summary. Int. J. Nurs. Stud. 2019, 91, 144–145. [Google Scholar] [CrossRef]
- Jacobson Vann, J.C.; Jacobson, R.M.; Coyne-Beasley, T.; Asafu-Adjei, J.K.; Szilagyi, P.G. Patient Reminder and Recall Interventions to Improve Immunization Rates. Cochrane Database Syst. Rev. 2018, 2018, CD003941. [Google Scholar] [CrossRef]
- Rand, C.M.; Vincelli, P.; Goldstein, N.P.N.; Blumkin, A.; Szilagyi, P.G. Effects of Phone and Text Message Reminders on Completion of the Human Papillomavirus Vaccine Series. J. Adolesc. Health 2017, 60, 113–119. [Google Scholar] [CrossRef]
- Kharbanda, E.O.; Stockwell, M.S.; Fox, H.W.; Andres, R.; Lara, M.; Rickert, V.I. Text Message Reminders to Promote Human Papillomavirus Vaccination. Vaccine 2011, 29, 2537–2541. [Google Scholar] [CrossRef]
- Rand, C.M.; Brill, H.; Albertin, C.; Humiston, S.G.; Schaffer, S.; Shone, L.P.; Blumkin, A.K.; Szilagyi, P.G. Effectiveness of Centralized Text Message Reminders on Human Papillomavirus Immunization Coverage for Publicly Insured Adolescents. J. Adolesc. Health 2015, 56, S17–S20. [Google Scholar] [CrossRef] [PubMed]
- Tull, F.; Borg, K.; Knott, C.; Beasley, M.; Halliday, J.; Faulkner, N.; Sutton, K.; Bragge, P. Short Message Service Reminders to Parents for Increasing Adolescent Human Papillomavirus Vaccination Rates in a Secondary School Vaccine Program: A Randomized Control Trial. J. Adolesc. Health 2019, 65, 116–123. [Google Scholar] [CrossRef] [PubMed]
- McGlone, M.S.; Stephens, K.K.; Rodriguez, S.A.; Fernandez, M.E. Persuasive Texts for Prompting Action: Agency Assignment in HPV Vaccination Reminders. Vaccine 2017, 35, 4295–4297. [Google Scholar] [CrossRef] [PubMed]
- Matheson, E.C.; Derouin, A.; Gagliano, M.; Thompson, J.A.; Blood-Siegfried, J. Increasing HPV Vaccination Series Completion Rates via Text Message Reminders. J. Pediatr. Health Care 2014, 28, e35–e39. [Google Scholar] [CrossRef] [PubMed]
- Ueberroth, B.E.; Labonte, H.R.; Wallace, M.R. Impact of Patient Portal Messaging Reminders with Self-Scheduling Option on Influenza Vaccination Rates: A Prospective, Randomized Trial. J. Gen. Intern. Med. 2022, 37, 1394–1399. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Albertin, C.S.; Casillas, A.; Valderrama, R.; Duru, O.K.; Ong, M.K.; Vangala, S.; Tseng, C.-H.; Humiston, S.G.; Evans, S.; et al. Effect of Personalized Messages Sent by a Health System’s Patient Portal on Influenza Vaccination Rates: A Randomized Clinical Trial. J. Gen. Intern. Med. 2022, 37, 615–623. [Google Scholar] [CrossRef]
- Shah, S.F.A.; Ginossar, T.; Bentley, J.M.; Zimet, G.; McGrail, J.P. Using the Theory of Planned Behavior to Identify Correlates of HPV Vaccination Uptake among College Students Attending a Rural University in Alabama. Vaccine 2021, 39, 7421–7428. [Google Scholar] [CrossRef]
- Rimer, B.K.; Brewer, N. Chapter 4: Introduction to Health Behavior Theories That Focus on Individuals. In Health Behavior: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass Public Health; Jossey-Bass & Pfeiffer Imprints, Wiley: San Francisco, CA, USA, 2015; ISBN 978-1-118-62905-5. [Google Scholar]
- Francis, D.B.; Cates, J.R.; Wagner, K.P.G.; Zola, T.; Fitter, J.E.; Coyne-Beasley, T. Communication Technologies to Improve HPV Vaccination Initiation and Completion: A Systematic Review. Patient Educ. Couns. 2017, 100, 1280–1286. [Google Scholar] [CrossRef]
- Acampora, A.; Grossi, A.; Barbara, A.; Colamesta, V.; Causio, F.A.; Calabrò, G.E.; Boccia, S.; de Waure, C. Increasing HPV Vaccination Uptake among Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 7997. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Albertin, C.; Humiston, S.G.; Rand, C.M.; Schaffer, S.; Brill, H.; Stankaitis, J.; Yoo, B.-K.; Blumkin, A.; Stokley, S. A Randomized Trial of the Effect of Centralized Reminder/Recall on Immunizations and Preventive Care Visits for Adolescents. Acad. Pediatr. 2013, 13, 204–213. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size—Or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Szilagyi, P.G.; Humiston, S.G.; Gallivan, S.; Albertin, C.; Sandler, M.; Blumkin, A. Effectiveness of a Citywide Patient Immunization Navigator Program on Improving Adolescent Immunizations and Preventive Care Visit Rates. Arch. Pediatr. Adolesc. Med. 2011, 165, 547–553. [Google Scholar] [CrossRef]
- Petrosky, E.; Bocchini, J.A.; Hariri, S.; Chesson, H.; Curtis, C.R.; Saraiya, M.; Unger, E.R.; Markowitz, L.E.; Centers for Disease Control and Prevention (CDC). Use of 9-Valent Human Papillomavirus (HPV) Vaccine: Updated HPV Vaccination Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 300–304. [Google Scholar] [PubMed]
- Chido-Amajuoyi, O.G.; Talluri, R.; Wonodi, C.; Shete, S. Trends in HPV Vaccination Initiation and Completion Within Ages 9–12 Years: 2008–2018. Pediatrics 2021, 147, e2020012765. [Google Scholar] [CrossRef] [PubMed]
- Boersma, P.; Black, L. Human Papillomavirus Vaccination among Adults, Aged 18−26, 2013−2018; NCHS: Hyattsville, MD, USA, 2020. [Google Scholar]
- TeenVaxView | Adolescent Vaccine Coverage Interactive Data | NIS | CDC. Available online: https://www.cdc.gov/vaccines/imz-managers/coverage/teenvaxview/data-reports/index.html (accessed on 9 February 2023).
- Health and Economic Benefits of Cervical Cancer Interventions | Power of Prevention. Available online: https://www.cdc.gov/chronicdisease/programs-impact/pop/cervical-cancer.htm (accessed on 17 March 2023).
- CDC. HPV Vaccine Safety. Available online: https://www.cdc.gov/hpv/hcp/vaccine-safety-data.html (accessed on 10 February 2023).
- CDC. VFC: Current CDC Vaccine Price List. Available online: https://www.cdc.gov/vaccines/programs/vfc/awardees/vaccine-management/price-list/index.html (accessed on 17 March 2023).


{kind=link}
| Patient Less Than 18 Years Old | Patients 18 Years or Older | |
|---|---|---|
| Initial Message | Dr. Yetman [PCP name] recommends Jane [Patient name] complete their HPV vaccination to prevent cancers caused by HPV. To schedule go to [Scheduling link]. Reply OK to confirm receipt. | John [Patient Name]: Dr. Foxhall [PCP name] recommends you complete your HPV vaccination to prevent cancers caused by HPV. To schedule, go to [Scheduling link]. Reply OK to confirm receipt. |
| Second or Third Message | Reminder: Dr. Yetman [PCP name] recommends Jane [patient name] complete their HPV vaccination. To schedule go to [Scheduling link]. Reply OK to confirm receipt. | Reminder for John [Patient Name]: Dr. Foxhall [PCP name] recommends you complete your HPV vaccination. To schedule, go to [Scheduling link]. Reply OK to confirm receipt. |
| Baseline Characteristics | Electronic Reminder (N = 3705) N (%) | Usual Care (N = 3703) N (%) | p-Value |
|---|---|---|---|
| Age | 0.689 | ||
| 9–14 | 1511 (40.78) | 1535 (41.45) | |
| 15–18 | 721 (19.46) | 693 (18.71) | |
| 19–25 | 1473 (39.76) | 1475 (39.83) | |
| Sex | 0.942 | ||
| Male | 1676 (45.24) | 1672 (45.15) | |
| Female | 2029 (54.76) | 2031 (54.85) | |
| Vaccine Status | 0.834 | ||
| Not initiated | 2542 (68.61) | 2549 (68.84) | |
| Initiated | 1163 (31.39) | 1154 (31.16) | |
| Race/Ethnicity | 0.176 | ||
| Non-Hispanic White | 865 (23.35) | 939 (25.36) | |
| Non-Hispanic Black | 955 (25.78) | 962 (25.98) | |
| Hispanic | 911 (24.59) | 874 (23.60) | |
| Other/Unknown | 974 (26.29) | 928 (25.06) | |
| Insurance | 0.134 | ||
| Medicaid | 1317 (35.55) | 1337 (36.11) | |
| Private (Managed Care) | 2014 (54.36) | 2049 (55.33) | |
| Uninsured | 338 (9.12) | 291 (7.86) | |
| Other | 36 (0.97) | 26 (0.70) |
| Electronic Reminder | Usual Care | |||
|---|---|---|---|---|
| (N = 3705) | (N = 3703) | |||
| HPV Outcomes | N (%) | N (%) | Adjusted OR (95% CI *) | p-Value |
| Appointment Scheduling | 752 (20.3) | 700 (18.9) | 1.12 (1.00, 1.26) | 0.056 |
| Clinic Visit | 423 (11.42) | 419 (11.32) | 1.07 (0.94, 1.23) | 0.300 |
| All Additional HPV Vaccination(s) | 450 (12.15) | 402 (10.86) | 1.17 (1.01, 1.36) | 0.036 |
| Electronic Reminder | Usual Care | |||
|---|---|---|---|---|
| (N = 2529) | (N = 2538) | |||
| N (%) | N (%) | Adjusted OR (95% CI**) | p-Value | |
| HPV vaccine initiation rate | 206 (8.15) | 181 (7.13) | 1.22 (0.98, 1.51) | 0.076 |
| Electronic Reminder | Usual Care | |||
| (N = 3705) | (N = 3703) | |||
| N (%) | N (%) | Adjusted OR (95% CI**) | p-Value | |
| HPV vaccine completion rate | 225 (6.07) | 207 (5.59) | 1.12 (0.90, 1.38) | 0.302 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanley, K.; Chung, T.H.; Nguyen, L.K.; Amadi, T.; Stansberry, S.; Yetman, R.J.; Foxhall, L.E.; Bello, R.; Diallo, T.; Le, Y.-C.L. Using Electronic Reminders to Improve Human Papillomavirus (HPV) Vaccinations among Primary Care Patients. Vaccines 2023, 11, 872. https://doi.org/10.3390/vaccines11040872
Hanley K, Chung TH, Nguyen LK, Amadi T, Stansberry S, Yetman RJ, Foxhall LE, Bello R, Diallo T, Le Y-CL. Using Electronic Reminders to Improve Human Papillomavirus (HPV) Vaccinations among Primary Care Patients. Vaccines. 2023; 11(4):872. https://doi.org/10.3390/vaccines11040872
Chicago/Turabian StyleHanley, Kathleen, Tong Han Chung, Linh K. Nguyen, Tochi Amadi, Sandra Stansberry, Robert J. Yetman, Lewis E. Foxhall, Rosalind Bello, Talhatou Diallo, and Yen-Chi L. Le. 2023. "Using Electronic Reminders to Improve Human Papillomavirus (HPV) Vaccinations among Primary Care Patients" Vaccines 11, no. 4: 872. https://doi.org/10.3390/vaccines11040872