

Views and Perceptions of People Aged 55+ on the Vaccination Programme for Older Adults in the UK: A Qualitative Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodological Approach
2.2. Participant Recruitment
2.3. Data Collection
2.4. Data Analysis
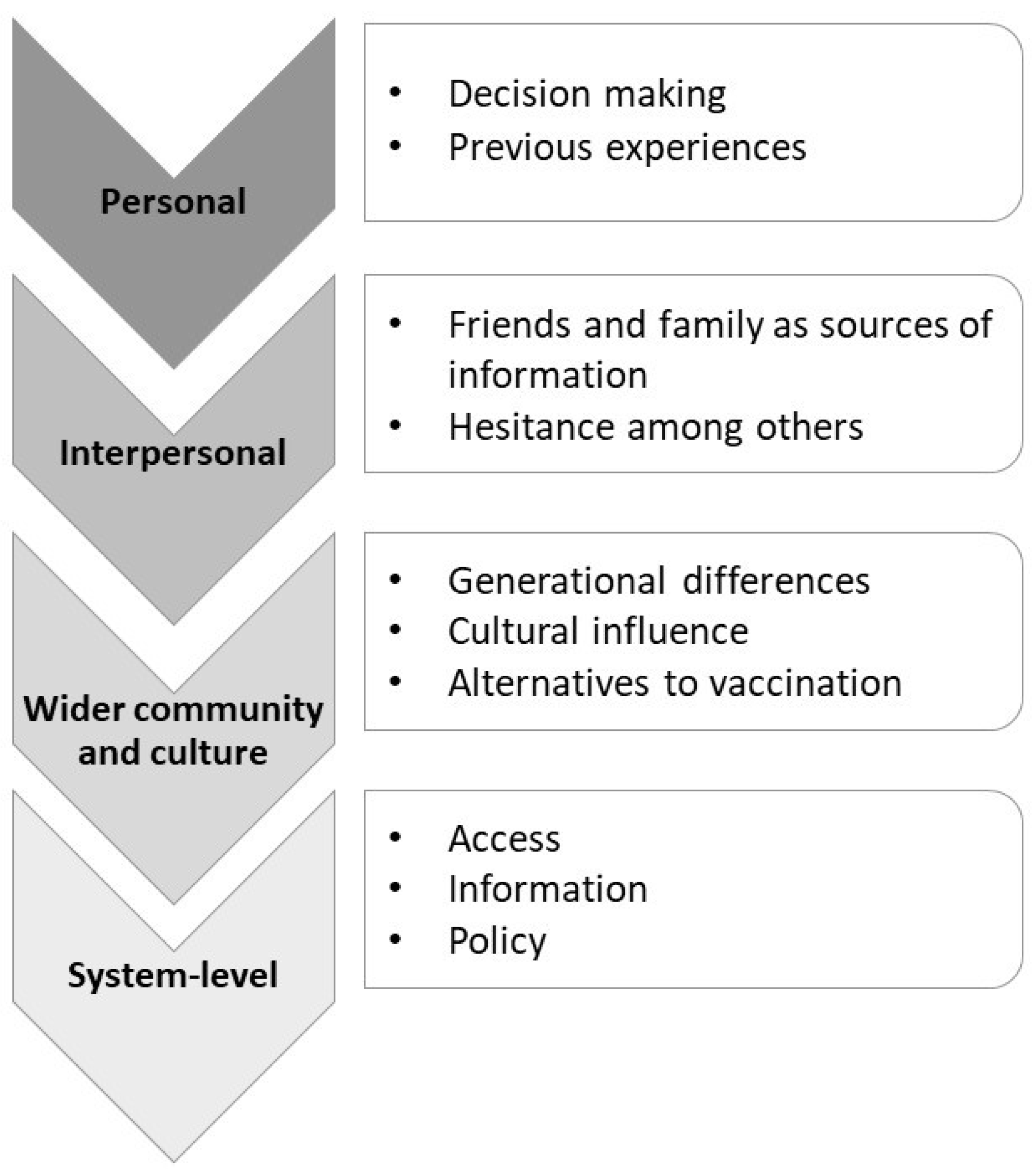
3. Results
3.1. Personal Factors Affecting Views on Vaccination
3.1.1. Decision Making
3.1.2. Previous Experiences
3.2. Interpersonal Interactions and Views on Vaccination
3.2.1. Friends and Family as Sources of Information
3.2.2. Influencing Others
3.3. Wider Community and Cultural Aspects
3.3.1. Generational Differences
3.3.2. Cultural Aspects
3.3.3. Alternatives to Vaccination
3.4. System-Level Aspects
3.4.1. Access
3.4.2. Lack of Information and Sources of Information
3.4.3. Policy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kan, T.; Zhang, J. Factors influencing seasonal influenza vaccination behaviour among elderly people: A systematic review. Public Health 2018, 156, 67–78. [Google Scholar] [CrossRef]
- Pereira, J.A.; Gilca, V.; Waite, N.; Andrew, M.K. Canadian older adults’ perceptions of effectiveness and value of regular and high-dose influenza vaccines. Hum. Vaccines Immunother. 2018, 15, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Mak, F.-Y.; Wong, Y.-Y.; Ko, S.; Chong, M.K.C.; Wang, Z.; Hon, K.-L.; Wong, E.L.Y.; Yeoh, E.-K.; Wong, M.C.S. Enabling Factors, Barriers, and Perceptions of Pneumococcal Vaccination Strategy Implementation: A Qualitative Study. Vaccines 2022, 10, 1164. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, L.A.B.; Gallant, A.J.; Cogan, N.; Rasmussen, S.; Young, D.; Williams, L. Older adults’ vaccine hesitancy: Psychosocial factors associated with influenza, pneumococcal, and shingles vaccine uptake. Vaccine 2021, 39, 3520–3527. [Google Scholar] [CrossRef] [PubMed]
- Shin, G.; Kang, D.; Cheong, H.J.; Choi, S.E. Cost-Effectiveness of Extending the National Influenza Vaccination Program in South Korea: Does Vaccination of Older Adults Provide Health Benefits to the Entire Population? Vaccines 2022, 10, 932. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, M.; Aoki, T.; Goto, R.; Ozone, S.; Haruta, J. Better Patient Experience is Associated with Better Vaccine Uptake in Older Adults: Multicentered Cross-sectional Study. J. Gen. Intern. Med. 2020, 35, 3485–3491. [Google Scholar] [CrossRef]
- Breeze, E.; Mangtani, P.; E Fletcher, A.; Price, G.M.; Kovats, S.; Roberts, J. Trends in influenza vaccination uptake among people aged over 74 years, 1997–2000: Survey of 73 general practices in Britain. BMC Fam. Pract. 2004, 5, 8. [Google Scholar] [CrossRef]
- Kajikawa, N.; Kataoka, Y.; Goto, R.; Maeno, T.; Yokoya, S.; Umeyama, S.; Takahashi, S.; Maeno, T. Factors associated with influenza vaccination in Japanese elderly outpatients. Infect. Dis. Heal. 2019, 24, 212–221. [Google Scholar] [CrossRef]
- Domínguez, A.; Soldevila, N.; Toledo, D.; Godoy, P.; Torner, N.; Force, L.; Castilla, J.; Mayoral, J.M.; Tamames, S.; Martín, V.; et al. Factors associated with pneumococcal polysaccharide vaccination of the elderly in Spain: A cross-sectional study. Hum. Vaccines Immunother. 2016, 12, 1891–1899. [Google Scholar]
- Marcu, A.; Rubinstein, H.; Michie, S.; Yardley, L. Accounting for personal and professional choices for pandemic influenza vaccination amongst English healthcare workers. Vaccine 2015, 33, 2267–2272. [Google Scholar] [CrossRef]
- Sakamoto, A.; Chanyasanha, C.; Sujirarat, D.; Matsumoto, N.; Nakazato, M. Factors associated with pneumococcal vaccination in elderly people: A cross-sectional study among elderly club members in Miyakonojo City, Japan. BMC Public Health 2018, 18, 1172. [Google Scholar] [CrossRef] [PubMed]
- Guo, N.; Wang, J.; Nicholas, S.; Maitland, E.; Zhu, D. Behavioral Differences in the Preference for Hepatitis B Virus Vaccination: A Discrete Choice Experiment. Vaccines 2020, 8, 527. [Google Scholar] [CrossRef] [PubMed]
- Luz, P.M.; Brown, H.E.; Struchiner, C.J. Disgust as an emotional driver of vaccine attitudes and uptake? A mediation analysis. Epidemiol. Infect. 2019, 147, e182. [Google Scholar] [CrossRef]
- Mangtani, P.; Breeze, E.; Kovats, S.; Ng, E.S.; Roberts, J.A.; Fletcher, A. Inequalities in influenza vaccine uptake among people aged over 74 years in Britain. Prev. Med. 2005, 41, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 52, 3127–3141. [Google Scholar] [CrossRef]
- Tan, H.Y.; Lai, E.; Kunasekaran, M.; Chughtai, A.A.; Trent, M.; Poulos, C.J.; MacIntyre, C.R. Prevalence and predictors of influenza vaccination among residents of long-term care facilities. Vaccine 2019, 37, 6329–6335. [Google Scholar] [CrossRef]
- Lin, C.; Parker, T.; Pejavara, K.; Smith, D.; Tu, R.; Tu, P. “I Would Never Push a Vaccine on You”: A Qualitative Study of Social Norms and Pressure in Vaccine Behavior in the U.S. Vaccines 2022, 10, 1402. [Google Scholar] [CrossRef]
- Cornford, C.S.; Morgan, M. Elderly people’s beliefs about influenza vaccination. Br. J. Gen. Pract. 1999, 49, 281–284. [Google Scholar]
- Walzer, P.; Estève, C.; Barben, J.; Menu, D.; Cuenot, C.; Manckoundia, P.; Putot, A. Impact of Influenza Vaccination on Mortality in the Oldest Old: A Propensity Score-Matched Cohort Study. Vaccines 2020, 8, 356. [Google Scholar] [CrossRef]
- Denford, S.; Mowbray, F.; Towler, L.; Wehling, H.; Lasseter, G.; Amlôt, R.; Oliver, I.; Yardley, L.; Hickman, M. Exploration of attitudes regarding uptake of COVID-19 vaccines among vaccine hesitant adults in the UK: A qualitative analysis. BMC Infect. Dis. 2022, 22, 407. [Google Scholar] [CrossRef]
- Williams, S.N. Public attitudes to COVID-19 booster vaccinations and influenza vaccines: A qualitative focus group study. PsyArXiv 2021. preprint. [Google Scholar]
- NHS. NHS Vaccinations and When to Have Them. 2022. Available online: https://www.nhs.uk/conditions/vaccinations/nhs-vaccinations-and-when-to-have-them/ (accessed on 20 January 2023).
- Liamputtong, P. Focus Group Methodology: Principles and Practice; SAGE Publications: London, UK, 2011. [Google Scholar]
- Fabiani, M.; Volpe, E.; Faraone, M.; Bella, A.; Rizzo, C.; Marchetti, S.; Chini, F. Influenza vaccine uptake in the elderly population: Individual and general practitioner’s determinants in Central Italy, Lazio region, 2016–2017 season. Vaccine 2019, 37, 5314–5322. [Google Scholar] [CrossRef]
- Bell, S.; Edelstein, M.; Zatoński, M.; Ramsay, M.E.; Mounier-Jack, S. ‘I don’t think anybody explained to me how it works’: Qualitative study exploring vaccination and primary health service access and uptake amongst Polish and Romanian communities in England. BMJ Open 2019, 9, e028228. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; SAGE Publications Ltd.: London, UK, 2021. [Google Scholar]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.; Mehrotra, A.; Knights, F.; Deal, A.; Crawshaw, A.F.; Farah, Y.; Goldsmith, L.P.; Wurie, F.; Ciftci, Y.; Majeed, A.; et al. “We don’t routinely check vaccination background in adults”: A national qualitative study of barriers and facilitators to vaccine delivery and uptake in adult migrants through UK primary care. BMJ Open. 2022, 12, e062894. [Google Scholar] [CrossRef] [PubMed]
- Kirkdale, C.; Nebout, G.; Megerlin, F.; Thornley, T. Benefits of pharmacist-led flu vaccination services in community pharmacy. Ann. Pharm. Françaises 2017, 75, 3–8. [Google Scholar] [CrossRef]
- Perman, S.; Kwiatkowska, R.M.; Gjini, A. Do community pharmacists add value to routine immunization programmes? A review of the evidence from the UK. J. Public Heal. 2018, 40, e510–e520. [Google Scholar] [CrossRef]


{kind=link}
| Local Authority | Country |
|---|---|
| Bedford | England |
| Birmingham * | England |
| Bradford * | England |
| Manchester * | England |
| Newcastle-Upon-Tyne * | England |
| Newham borough of London * | England |
| Tewkesbury | England |
| Wellingborough | England |
| Wycombe | England |
| Armagh City, Banbridge and Craigavon | Northern Ireland |
| Belfast * | Northern Ireland |
| Glasgow * | Scotland |
| Perth & Kinross | Scotland |
| Cardiff * | Wales |
| Pembrokeshire | Wales |
| Number (n) | |
|---|---|
| Age group | |
| 55–64 | 19 |
| 65–74 | 29 |
| 75–84 | 6 |
| 85+ | 2 |
| Gender | |
| Female | 33 |
| Male | 22 |
| Non-binary | 1 |
| Ethnic group | |
| White | 52 |
| Mixed ethnicity | 2 |
| Asian | 1 |
| Black | 1 |
| Health status | |
| In good general health | 28 |
| No serious underlying health condition | 18 |
| Underlying health condition | 1 |
| Serious underlying health condition | 7 |
| Other | 2 |
| Disability status | |
| Disability | 10 |
| No disability | 43 |
| Prefer not to say | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silvonen, T.; Kesten, J.; Cabral, C.; Coast, J.; Ben-Shlomo, Y.; Christensen, H. Views and Perceptions of People Aged 55+ on the Vaccination Programme for Older Adults in the UK: A Qualitative Study. Vaccines 2023, 11, 870. https://doi.org/10.3390/vaccines11040870
Silvonen T, Kesten J, Cabral C, Coast J, Ben-Shlomo Y, Christensen H. Views and Perceptions of People Aged 55+ on the Vaccination Programme for Older Adults in the UK: A Qualitative Study. Vaccines. 2023; 11(4):870. https://doi.org/10.3390/vaccines11040870
Chicago/Turabian StyleSilvonen, Taru, Jo Kesten, Christie Cabral, Jo Coast, Yoav Ben-Shlomo, and Hannah Christensen. 2023. "Views and Perceptions of People Aged 55+ on the Vaccination Programme for Older Adults in the UK: A Qualitative Study" Vaccines 11, no. 4: 870. https://doi.org/10.3390/vaccines11040870