

Longitudinal Changes in IgG-Type SARS-CoV-2 Antibody Titers after COVID-19 Vaccination and a Prominent Increase in Antibody Titers When Infected after Vaccination
Abstract
:1. Introduction
2. Materials and Methods
3. Serology Assays
4. Statistical Analysis
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Uwamino, Y.; Kurafuji, T.; Sato, Y.; Tomita, Y.; Shibata, A.; Tanabe, A.; Yatabe, Y.; Noguchi, M.; Arai, T.; Ohno, A.; et al. Young age, female sex, and presence of systemic adverse reactions are associated with high post-vaccination antibody titer after two doses of BNT162b2 mRNA SARS-CoV-2 vaccination: An observational study of 646 Japanese healthcare workers and university staff. Vaccine 2022, 40, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Sawahata, M.; Nakamura, Y.; Kurihara, M.; Koike, R.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; et al. Age and Smoking Predict Antibody Titres at 3 Months after the Second Dose of the BNT162b2 COVID-19 Vaccine. Vaccines 2021, 9, 1042. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent Immune Response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Terpos, E.; Trougakos, I.P.; Apostolakou, F.; Charitaki, I.; Sklirou, A.D.; Mavrianou, N.; Papanagnou, E.-D.; Liacos, C.-I.; Gumeni, S.; Rentziou, G.; et al. Age-dependent and gender-dependent antibody responses against SARS-CoV-2 in health workers and octogenarians after vaccination with the BNT162b2 mRNA vaccine. Am. J. Hematol. 2021, 96, E257–E259. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Iyer, A.S.; Jones, F.K.; Nodoushani, A.; Kelly, M.; Becker, M.; Slater, D.; Mills, R.; Teng, E.; Kamruzzaman, M.; Garcia-Beltran, W.F.; et al. Persistence and decay of human antibody responses to the receptor binding domain of SARS-CoV-2 spike protein in COVID-19 patients. Sci. Immunol. 2020, 5, eabe0367. [Google Scholar] [CrossRef]
- Fujigaki, H.; Yamamoto, Y.; Koseki, T.; Banno, S.; Ando, T.; Ito, H.; Fujita, T.; Naruse, H.; Hata, T.; Moriyama, S.; et al. Antibody Responses to BNT162b2 Vaccination in Japan: Monitoring Vaccine Efficacy by Measuring IgG Antibodies against the Receptor-Binding Domain of SARS-CoV-2. Microbiol. Spectr. 2022, 10, e0118121. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Sughayer, M.A.; Souan, L.; Abu Alhowr, M.M.; Al Rimawi, D.; Siag, M.; Albadr, S.; Owdeh, S.A.M.; Al Atrash, T. Comparison of the effectiveness and duration of anti-RBD SARS-CoV-2 IgG antibody response between different types of vaccines: Implications for vaccine strategies. Vaccine 2022, 40, 2841–2847. [Google Scholar] [CrossRef]
- Tamura, M.; Fujita, R.; Sato, T.; Sato, R.; Kato, Y.; Nagasawa, M.; Matsumoto, T. Immunological responses following the third dose of the BNT162b2 SARS-CoV-2 vaccine among Japanese healthcare workers. J. Infect. Chemother. 2022, 28, 1478–1482. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of COVID-19 mRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.R.; Painter, M.M.; Lundgreen, K.A.; Apostolidis, S.A.; Baxter, A.E.; Giles, J.R.; Mathew, D.; Pattekar, A.; Reynaldi, A.; Khoury, D.S.; et al. Efficient recall of Omicron-reactive B cell memory after a third dose of SARS-CoV-2 mRNA vaccine. Cell 2022, 185, 1875–1887.e8. [Google Scholar] [CrossRef] [PubMed]
- Manisty, C.; Otter, A.D.; Treibel, T.A.; McKnight, Á.; Altmann, D.M.; Brooks, T.; Noursadeghi, M.; Boyton, R.J.; Semper, A.; Moon, J.C. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet 2021, 397, 1057–1058. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Bielak, D.A.; Carreño, J.M.; Chernet, R.L.; et al. Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef]
- Nah, E.H.; Cho, S.; Park, H.; Kim, S.; Noh, D.; Kwon, E.; Cho, H. Antibody response after two doses of homologous or heterologous SARS-CoV-2 vaccines in healthcare workers at health promotion centers: A prospective observational study. J. Med. Virol. 2022, 94, 4719–4726. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.K.; Burke, P.C.; Nowacki, A.S.; Terpeluk, P.; Gordon, S.M. Necessity of Coronavirus Disease 2019 (COVID-19) Vaccination in Persons Who Have Already Had COVID-19. Clin. Infect. Dis. 2022, 75, e662–e671. [Google Scholar] [CrossRef]
- Desmecht, S.; Tashkeev, A.; El Moussaoui, M.; Marechal, N.; Perée, H.; Tokunaga, Y.; Fombellida-Lopez, C.; Polese, B.; Legrand, C.; Wéry, M.; et al. Kinetics and Persistence of the Cellular and Humoral Immune Responses to BNT162b2 mRNA Vaccine in SARS-CoV-2-Naive and -Experienced Subjects: Impact of Booster Dose and Breakthrough Infections. Front. Immunol. 2022, 13, 863554. [Google Scholar] [CrossRef]
- Kusunoki, H.; Ekawa, K.; Ekawa, M.; Kato, N.; Yamasaki, K.; Motone, M.; Shimizu, H. Trends in Antibody Titers after SARS-CoV-2 Vaccination—Insights from Self-Paid Tests at a General Internal Medicine Clinic. Available online: https://www.medrxiv.org/content/10.1101/2023.03.03.23286284v1.full (accessed on 8 March 2023).
- Goel, R.R.; Painter, M.M.; Apostolidis, S.A.; Mathew, D.; Meng, W.; Rosenfeld, A.M.; Lundgreen, K.A.; Reynaldi, A.; Khoury, D.S.; Pattekar, A.; et al. mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science 2021, 374, abm0829. [Google Scholar] [CrossRef]
- Diseases, T.L.I. Why hybrid immunity is so triggering. Lancet Infect. Dis. 2022, 22, 1649. [Google Scholar] [CrossRef]
- Hall, V.; Foulkes, S.; Insalata, F.; Kirwan, P.; Saei, A.; Atti, A.; Wellington, E.; Khawam, J.; Munro, K.; Cole, M.; et al. Protection against SARS-CoV-2 after COVID-19 Vaccination and Previous Infection. N. Engl. J. Med. 2022, 386, 1207–1220. [Google Scholar] [CrossRef]
- Sidik, S.M. COVID vaccine plus infection can lead to months of immunity. Nature 2022. [Google Scholar] [CrossRef] [PubMed]
- Bobrovitz, N.; Ware, H.; Ma, X.; Li, Z.; Hosseini, R.; Cao, C.; Selemon, A.; Whelan, M.; Premji, Z.; Issa, H.; et al. Protective effectiveness of previous SARS-CoV-2 infection and hybrid immunity against the omicron variant and severe disease: A systematic review and meta-regression. Lancet Infect. Dis. 2023, in press. [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifon, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- Crotty, S. Hybrid immunity: COVID-19 vaccine responses provide insights into how the immune system perceives threats. Science 2021, 372, 1392–1393. [Google Scholar] [CrossRef]
- Arunachalam, P.S.; Wimmers, F.; Mok, C.K.P.; Perera, R.A.P.M.; Scott, M.; Hagan, T.; Sigal, N.; Feng, Y.; Bristow, L.; Tsang, O.T.-Y.; et al. Systems biological assessment of immunity to mild versus severe COVID-19 infection in humans. Science 2020, 369, 1210–1220. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
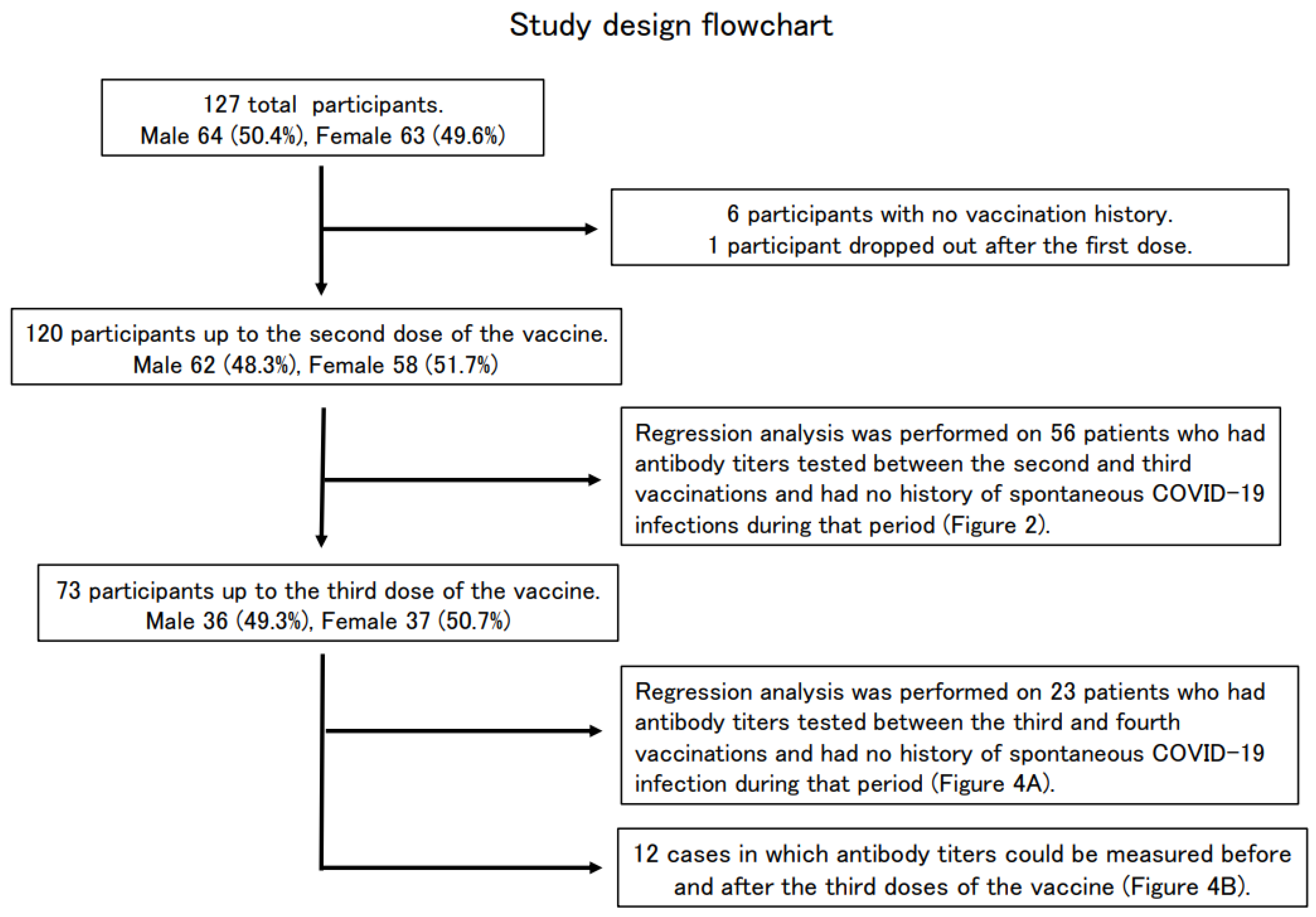
| Total Participants | Participants up to the Second Dose | Participants up to the Third Dose | |
|---|---|---|---|
| Total | 127 | 120 | 73 |
| Male, n (%) | 64 (50.4) | 62 (48.3) | 36 (49.3) |
| Female, n (%) | 63 (49.6) | 58 (51.7) | 37 (50.7) |
| Mean age | 52.3 ± 19.0 | 52.7 ± 19.0 | 54.6 ± 17.8 |
| Median age | 57 | 57.5 | 59 |
| Type of vaccine | BNT162b2 (BioNTech and Pfizer), n (%) | 64 (53.3) | 56 (76.7) |
| mRNA-1273 (Moderna and Takeda), n (%) | 12 (10.0) | 8 (11.0) | |
| Unknown, n (%) | 44 (36.7) | 9 (12.3) | |
| No vaccination history, n (%) | 6 (4.7) | ||
| Participants up to the first dose | 1 (0.8) | ||
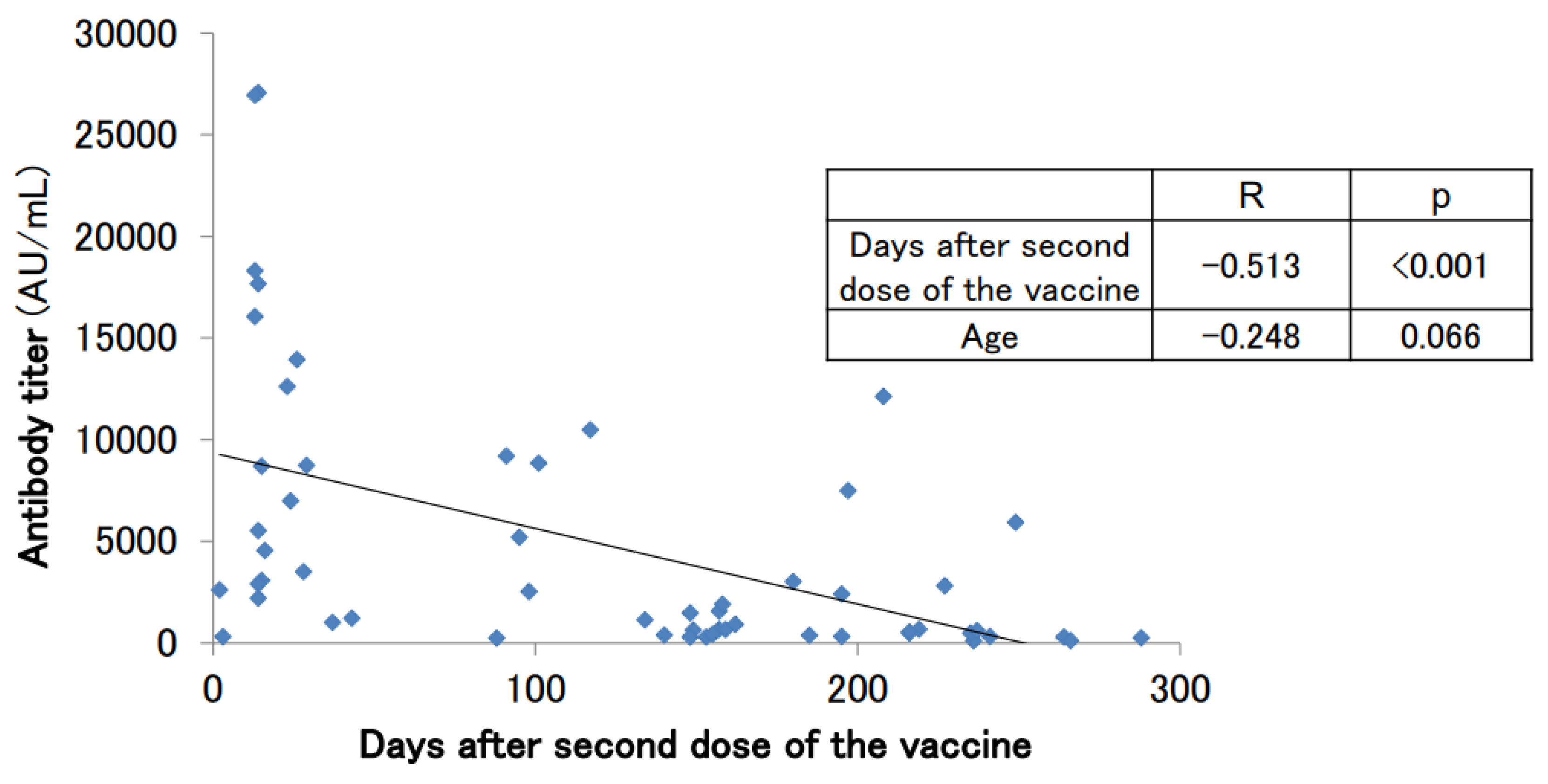
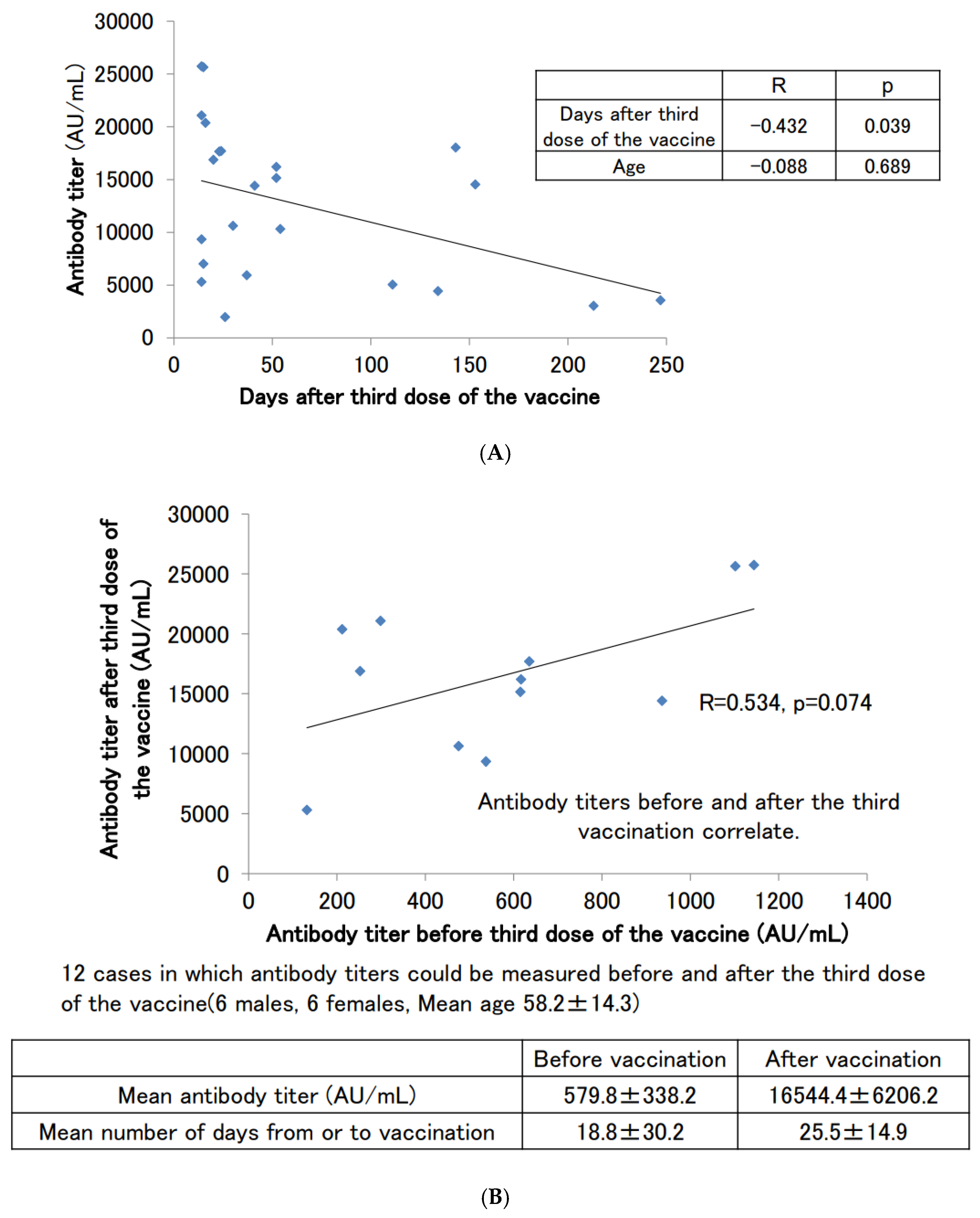
| Analyzed Participants up to the Second Dose | Analyzed Participants up to the Third Dose | ||
|---|---|---|---|
| Total | 56 | 23 | |
| Male, n (%) | 30 (53.6) | 12 (52.2) | |
| Female, n (%) | 26 (46.4) | 11 (47.8) | |
| Mean age | 55.6 ± 16.5 | 59.3 ± 14.8 | |
| Median age | 59.5 | 60.0 | |
| Type of vaccine | BNT162b2 (BioNTech and Pfizer), n (%) | 34 (60.7) | 16 (69.6) |
| mRNA-1273 (Moderna and Takeda), n (%) | 6 (10.7) | 4 (17.4) | |
| Unknown, n (%) | 16 (28.6) | 3 (13.0) | |
| Mean antibody titer (U/mL) (Mean ± standard deviation) | 4807.7 ± 6472.6 | 12,617.5 ± 7256.2 | |
| Median antibody titer (U/mL) | 2052.0 | 14,416.2 | |
| Mean number of days between the vaccination and the measurement day (Mean ± standard deviation) | 122.0 ± 89.3 | 63.6 ± 68.6 | |
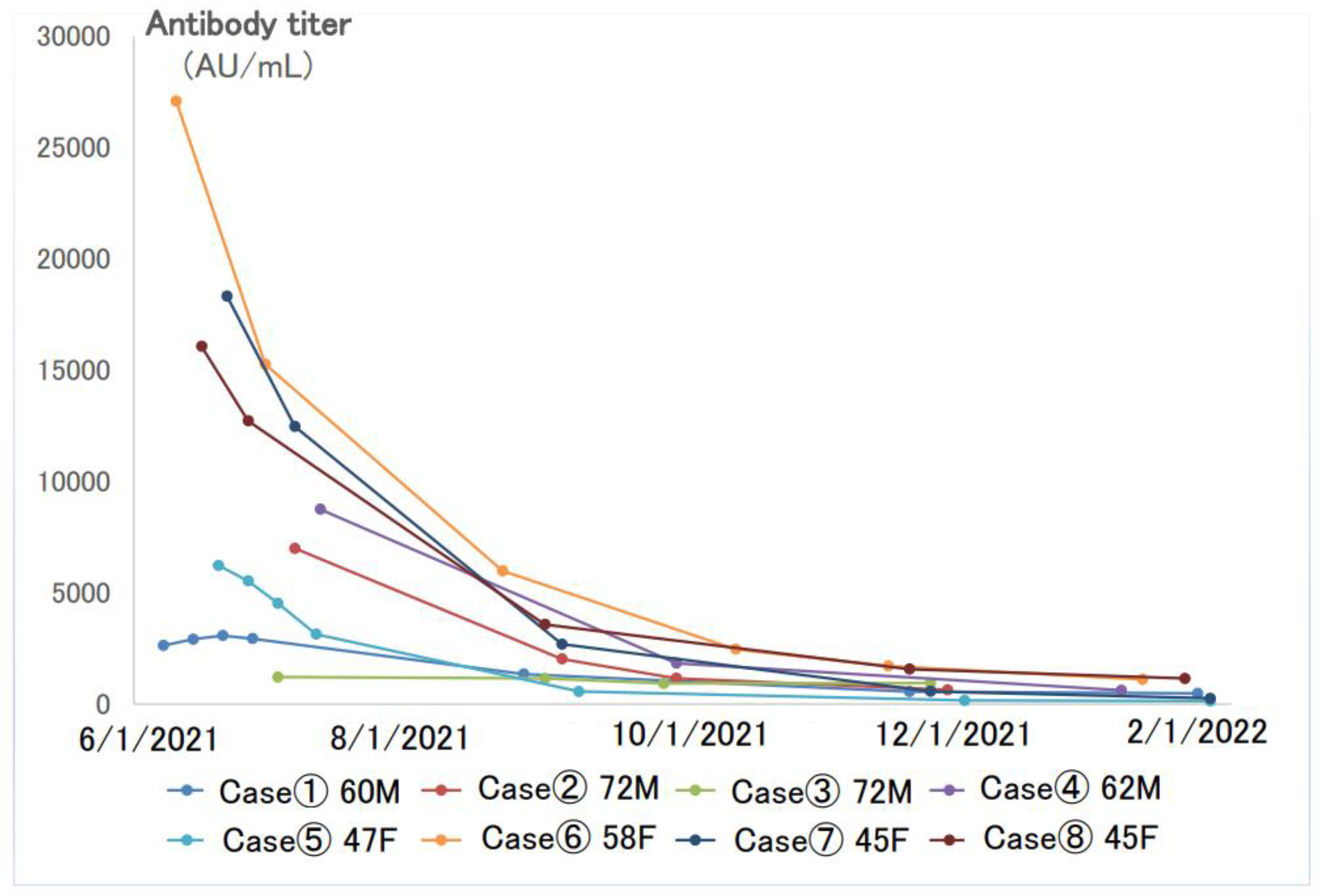
| Case | Days from the 2nd Dose of the Vaccine to the Maximum Antibody Titer | Maximum Antibody Titer (AU/mL) | Minimum Antibody Titer (AU/mL) | Follow-up (Number of Days) | Rate of Decrease in Antibody Titer (AU/mL/Day) |
|---|---|---|---|---|---|
| Case①60M | 21 | 3073.8 | 475.5 | 230 | 11.3 |
| Case②72M | 24 | 6988.8 | 635.4 | 154 | 41.3 |
| Case③83M | 65 | 1211.7 | 936.1 | 154 | 1.8 |
| Case④62M | 29 | 8745.5 | 616.8 | 189 | 43.0 |
| Case⑤47F | 7 | 6221.9 | 132.2 | 234 | 26.0 |
| Case⑥58F | 14 | 27,079.9 | 1101.9 | 228 | 113.9 |
| Case⑦45F | 13 | 18,316.8 | 252.3 | 166 | 108.8 |
| Case⑧45F | 13 | 16,064.3 | 1144 | 232 | 64.3 |
| Case | 1st Vaccination Date | 2nd Vaccination Date | 3rd Vaccination Date | Date of Infection | Post-Infection Antibody Test Date① | Post-Infection Antibody Titer① (AU/mL) | Post-Infection Antibody Test Date② | Post-Infection Antibody Titer② (AU/mL) | Post-Infection Antibody Test Date③ | Post-Infection Antibody Titer③ (AU/mL) |
|---|---|---|---|---|---|---|---|---|---|---|
| 36M | 4/30/2021 | 5/21/2021 | 1/17/2022 ※ | 2/7/2022 | >40,000.0 | 8/16/2022 | 31,409.9 | 11/15/2022 | 22,684.0 | |
| 65M | 4/27/2021 | 5/18/2021 | 2/7/2022 | 4/2/2022 | 4/20/2022 | >40,000.0 | 10/4/2022 | 15,769.9 | 12/27/2022 | 12,379.0 |
| 45M | 5/6/2021 | 5/27/2021 | 8/3/2022 | 9/20/2022 | >40,000.0 | 12/23/2022 | 19,533.0 | |||
| 68M | July 2021 | Aug 2021 | April 2022 | Aug 2022 # | 11/1/2022 | >40,000.0 | 12/20/2022 | 39,247.6 | ||
| 63M | 4/28/2021 | 5/19/2021 | 2/4/2022 | 8/20/2022 | 11/4/2022 | >40,000.0 | ||||
| 44M | 7/24/2021 | 8/21/2021 | 7/16/2022 | 8/9/2022 | 11/10/2022 | 17,451.4 | ||||
| 27F | 4/30/2021 | 5/21/2021 | 1/22/2022 | 2/7/2022 | >40,000.0 | |||||
| 23F | 5/26/2021 | 6/18/2021 | 3/11/2022 | Aug 2022 | 11/28/2022 | >40,000.0 | ||||
| 24F | April 2021 | 5/14/2021 | 1/15/2022 | Aug 2022 | 11/28/2022 | 36,446.4 | ||||
| 23F | 7/24/2021 | 8/21/2021 | 4/22/2022 | 8/12/2022 | 12/1/2022 | 36,292.0 | ||||
| 35F | April 2021 | May 2021 | 1/10/2022 | 1/24/2022 | 18,907.4 | |||||
| 28F | 8/27/2021 | 9/17/2021 | 4/9/2022 | 12/14/2022 | 1/6/2023 | 45,218.1 | ||||
| 25F | April 2021 | Aug 2021 | May 2022 | Aug 2022 | 11/29/2022 | 37,648.8 | ||||
| 23F | 7/24/2021 | 8/21/2021 | 4/22/2022 | 8/12/2022 | 12/1/2022 | 27,238.4 | ||||
| 23F | July 2021 | 8/13/2021 | 3/19/2022 | Sep 2022 | 12/2/2022 | >80,000.0 | ||||
| 63F | 5/14/2021 | 6/4/2021 | 3/14/2022 | 11/9/2022 | 12/5/2022 | 31,879.8 | ||||
| 40F | 3/26/2021 | 4/16/2021 | 12/17/2021 | 1/1/2023 | 2/2/2023 | 27,849.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kusunoki, H.; Ohkusa, M.; Iida, R.; Saito, A.; Kawahara, M.; Ekawa, K.; Kato, N.; Yamasaki, K.; Motone, M.; Shimizu, H. Longitudinal Changes in IgG-Type SARS-CoV-2 Antibody Titers after COVID-19 Vaccination and a Prominent Increase in Antibody Titers When Infected after Vaccination. Vaccines 2023, 11, 860. https://doi.org/10.3390/vaccines11040860
Kusunoki H, Ohkusa M, Iida R, Saito A, Kawahara M, Ekawa K, Kato N, Yamasaki K, Motone M, Shimizu H. Longitudinal Changes in IgG-Type SARS-CoV-2 Antibody Titers after COVID-19 Vaccination and a Prominent Increase in Antibody Titers When Infected after Vaccination. Vaccines. 2023; 11(4):860. https://doi.org/10.3390/vaccines11040860
Chicago/Turabian StyleKusunoki, Hiroshi, Michiko Ohkusa, Rie Iida, Ayumi Saito, Mikio Kawahara, Kazumi Ekawa, Nozomi Kato, Keita Yamasaki, Masaharu Motone, and Hideo Shimizu. 2023. "Longitudinal Changes in IgG-Type SARS-CoV-2 Antibody Titers after COVID-19 Vaccination and a Prominent Increase in Antibody Titers When Infected after Vaccination" Vaccines 11, no. 4: 860. https://doi.org/10.3390/vaccines11040860