
Achieving the IA2030 Coverage and Equity Goals through a Renewed Focus on Urban Immunization

 , ,
, ,
Abstract
:1. Background
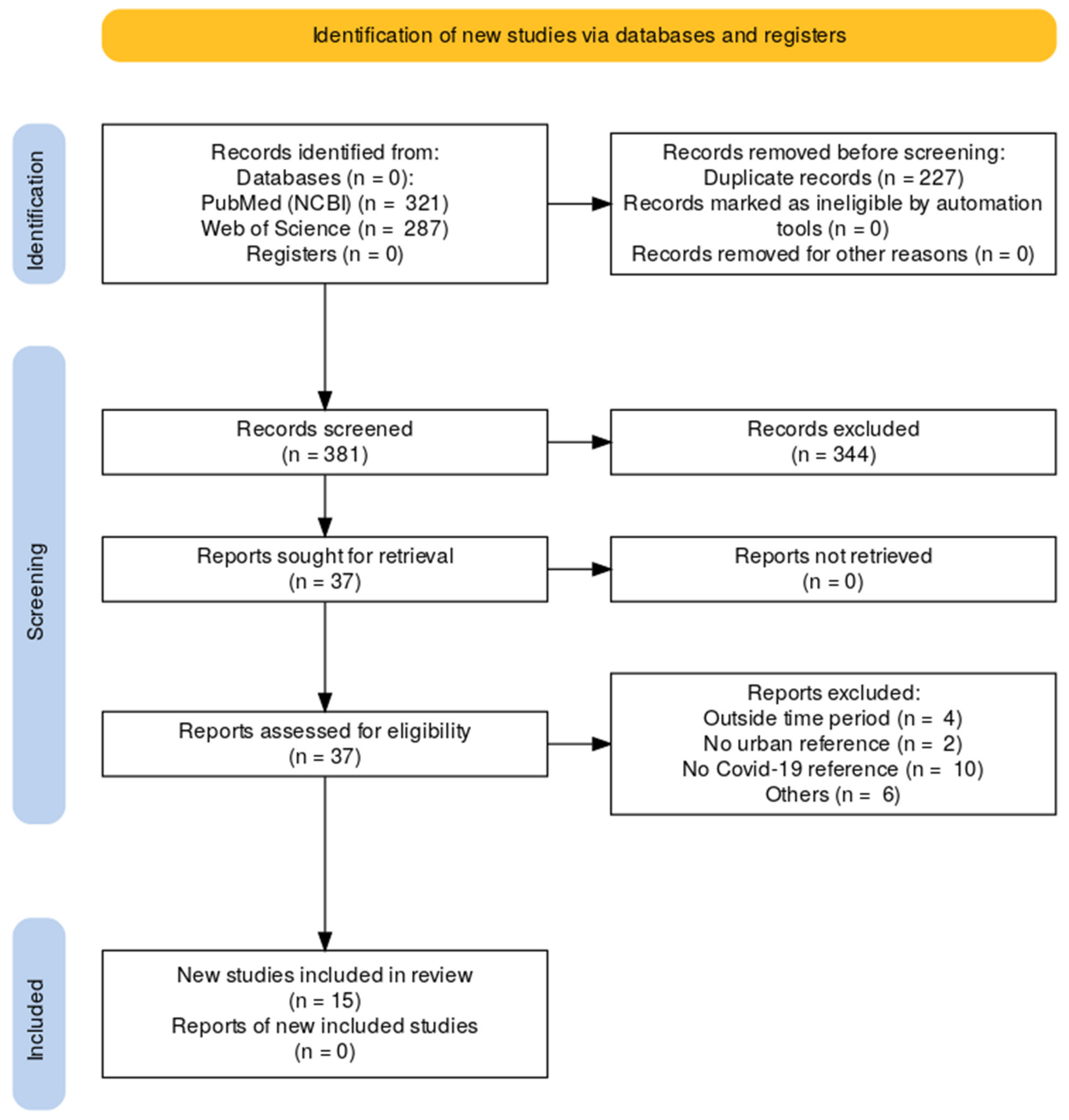
2. Methods
- To what extent did COVID-19 pandemic interrupt routine immunization performance and other related services in urban and peri-urban settings in focus countries?
- What were the predictors of decline or backsliding in immunization coverage in these settings?
- What was done to recover immunization coverage?
3. Results
3.1. Backsliding of Immunization in Urban
3.2. Immunization Challenges and Predictors in Urban and Peri-Urban
3.3. Identified Pro-Equity Strategies
4. Discussion
4.1. Policy Suggestions
- (a)
- Multisectoral innovations: many of the drivers of immunization performance highlighted from this and other reviews transcend ‘traditional’ determinants of immunization performance (such as vaccine supply or trained community health worker availability). Addressing other social issues such as maternal education, access to water, sanitation, and hygiene (WASH) services, and (maternal and child) education is pivotal in improving immunization performance in urban settings [32], especially governance in the immunization space around urban and should be inclusive of these sectors for more robust programming.
- (b)
- Strengthen partnerships: leveraging the comparative strengths and expertise of partners across immunization, health, and other sectors such as planning and sanitation will be valuable. For instance, the Mission Indradhanush (MI) in India, which worked across sectors, recorded significant gains in immunization coverage in both urban and rural settings [36]. Considering the diversity of non-government actors in urban areas, a purposeful policy shift to further incorporate private service providers and non-governmental organizations into immunization service delivery is needed.
- (c)
- Monitoring and Data: The typical immunization data built upon traditional subnational administrative boundaries may not suffice to effectively monitor, measure, and track children in urban settings [13,35]. The urban population is fast growing and in motion most of the time. Modern innovations in digital registries and data tracking systems could provide answers on how to effectively track these inherently transient and migratory populations or populations that may not have access to the traditional identifications used in accessing government health services. Periodic routine micro census and the use of geographic information system (GIS) enable data to have shown great promise [8,37]. More enhanced disaggregation of immunization data by urban in routine data systems, such as the WHO and UNICEF joint reporting form (JRF), as well as in coverage surveys will support monitoring and tracking of immunization services in urban areas.
4.2. Future Studies
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Immunization Coverage Performance for the 20 Highest Burden Zero-Dose Countries
| Rank | Country | DTP1 (%) | DTP3 (%) | MCV1 (%) | Number Zero-Dose Children |
| 1 | India | 88 | 85 | 89 | 2,711,000 |
| 2 | Nigeria | 70 | 56 | 59 | 2,247,000 |
| 3 | Indonesia | 74 | 67 | 72 | 1,150,000 |
| 4 | Ethiopia | 70 | 65 | 54 | 1,134,000 |
| 5 | Philippines | 57 | 57 | 57 | 1,048,000 |
| 6 | Democratic Republic of the Congo | 81 | 65 | 55 | 734,000 |
| 7 | Brazil | 74 | 68 | 73 | 710,000 |
| 8 | Pakistan | 90 | 83 | 81 | 611,000 |
| 9 | Angola | 57 | 45 | 36 | 553,000 |
| 10 | Myanmar | 45 | 37 | 44 | 492,000 |
| 11 | United Republic of Tanzania | 82 | 81 | 76 | 402,000 |
| 12 | Mozambique | 67 | 61 | 84 | 372,000 |
| 13 | Afghanistan | 74 | 66 | 63 | 361,000 |
| 14 | Somalia | 52 | 42 | 46 | 338,000 |
| 15 | Mexico | 83 | 78 | 99 | 317,000 |
| 16 | Madagascar | 65 | 55 | 39 | 304,000 |
| 17 | Cameroon | 76 | 69 | 219,000 | |
| 18 | Democratic People’s Republic of Korea | 42 | 41 | 42 | 197,000 |
| 19 | Chad | 73 | 58 | 55 | 191,000 |
| 20 | Viet Nam | 87 | 83 | 89 | 187,000 |
Appendix A.2. Full Search Strategy
Appendix A.3. Summary Table for Search Results
| Title | Year | Type of Study | Location | Summary |
| Yellow fever vaccination before and during the COVID-19 pandemic in Brazil [14]. | 2022 | Ecological, time series study | Brazil (Nationwide) | A 48.55% reduction in the median number of yellow fever vaccine doses administered in Brazil and in its regions 1 year before the pandemic as compared to 1 year during the pandemic: North (−34.71%), Midwest (−21.72%), South (−63.50%), and Southeast (−34.42%) |
| Child Vaccination Coverage, Trends and Predictors in Eastern Ethiopia: Implication for Sustainable Development Goals [21]. | 2021 | A population-based longitudinal study | Kersa, Eastern Ethiopia (incl. Harar town) | A little more than a third (39%) of children were fully vaccinated; with highest proportion (45%) seen in 2020 and the lowest (32%) in 2019. Other towns classified as semi-urban had the lowest fully vaccinated proportion even as Harar city saw 45% full vaccination for its children. |
| Experiences of Urban Slum-Dwelling Women with Maternal and Child Health Services During COVID-19 Pandemic: A Multi-City Qualitative Study From India [15]. | 2022 | A phenomenological study to document MCH experience during COVID-19 pandemic | India: Four states Odisha, Uttarakhand, Chhattisgarh, and Assam. One slum city per state | All participants in this study mentioned that their children were vaccinated during the pandemic with little or no issues. Fear that the child may get infected with COVID-19 was highlighted by caregivers. A few choose a private hospital for child immunization due to fear of COVID-19. |
| Strategies to revitalize immunization service provision in urban settings of Ethiopia [26]. | 2021 | A qualitative study with a phenomenological study design | Ethiopia: Addis Ababa, Dire Dawa and Mekele | The highlight of the study is that existing immunization service delivery strategies within urban contexts which are mostly fixed sites are not adequate to effectively reach children with vaccines in these settings. |
| Impact of COVID-19 pandemic on routine immunization of children [16]. | 2022 | Cross-sectional study | Pakistan: Mirpur, Azad Kashmir, | The fear of COVID-19 infection was highlighted as an important factor for delayed vaccination in 65% of respondents. |
| Disparities in full immunization coverage among urban and rural children aged 12–23 months in southwest Ethiopia: A comparative cross-sectional study [17]. | 2022 | A comparative cross-sectional | Ethiopia: Wolaita zone | Children in urban areas had a higher prevalence of full vaccination than their rural counterparts with a 15.10% (95% CI; 0.102–0.192) point estimate for the difference but still below WHO recommendation. Knowledge and place of delivery were predictor variables. |
| Effect of intensive training in improving older women’s knowledge and support for infant vaccination in Nigerian urban slums: a before-and-after intervention study [27]. | 2021 | Pre- and post-study | Nigeria: Seven urban slums communities in Ibadan | Participatory learning improved the knowledge about and support for infant vaccination among older women supervising childcare in these urban slum communities. |
| Assessment of vaccination timeliness and associated factors among children in Toke Kutaye district, central Ethiopia: A Mixed study [22]. | 2022 | A community-based cross-sectional mixed-method study | Ethiopia: Toke Kutaye district, central Ethiopia. | Timeliness of childhood vaccination was 23.9 percent among children aged 12 to 23 months. Urban residence (AOR: 3.15, 95% CI: 1.56–6.4), participation of pregnant women in conferences (AOR: 2.35, 95% CI: 1.2–4.57), institutional delivery (AOR: 2.5) |
| Parental acceptance of human papillomavirus vaccination for adolescent girls in Lagos, Nigeria [23]. | 2020 | A descriptive cross-sectional survey of adolescent girls’ parents | India: 2 urban and 2 rural schools in Lagos | Tertiary level of education in the mother (cOR = 67.41; 95% CI = 15.25–297.97; p = 0.0000), skilled occupation in the mother (cOR = 11.55; 95% CI = 5.55–24.04; p = 0.0000), skilled occupation in the father (cOR = 4.10; 95% CI = 2.31–7.28; p = 0.0000), are predictors of HPV vaccination. |
| Second-dose measles vaccination and associated factors among under-five children in urban areas of North Shoa Zone, Central Ethiopia, 2022 [24]. | 2022 | A community-based cross-sectional study | Ethiopia: urban areas of North Shewa Zone, Oromia | With a 90.1% response rate in 372 participants, the coverage of measles second-dose vaccination (MCV2) among children in urban areas was low (42.5%). |
| Impact of COVID-19 pandemic response on uptake of routine immunizations in Sindh, Pakistan: An analysis of provincial electronic immunization registry data [6]. | 2020 | Quantitative: Secondary data analysis of daily immunization coverage | Pakistan: Sindh urban and rural | The average daily vaccination rate during the COVID-19 lockdown saw a 52.5% decline. Bacille Calmette Guérin (BCG) vaccines saw the highest decline of 40.6% (958/2360). An estimated 8438 children per day missed their vaccines during the lockdown. Areas mostly affected included rural districts, urban sub-districts with large slums, and polio-endemic super high-risk sub-districts. |
| Impact of the Early Stages of the COVID-19 Pandemic on Coverage of Reproductive, Maternal, and Newborn Health Interventions in Ethiopia: A Natural Experiment [18]. | 2022 | A nationally representative cross-sectional survey | Ethiopia: Addis Ababa | Significant reductions in coverage of BCG vaccination and chlorohexidine use in urban areas were observed in the COVID-19-affected cohort. |
| Impact and projections of the COVID-19 epidemic on attendance and routine vaccinations at a pediatric referral hospital in Cameroon [19]. | 2021 | A descriptive and retrospective cross-sectional study | Cameroon: Yaoundé | There was a decline in vaccination demand including BCG vaccines, DPT, polio, and MMR in children as well as tetanus vaccines in women of childbearing age, all dropped significantly. |
| Scared, powerless, insulted and embarrassed: hesitancy towards vaccines among caregivers in Cavite Province, the Philippines [25]. | 2021 | Qualitative: In-depth interviews (IDIs) | Philippines: Cavite Province | Among the reasons for delay or refusal of childhood vaccinations, fear of side effects emerged as the most salient concern, exacerbated by previous negative experiences (including trauma) from a dengue vaccine controversy in 2017. |
| Missed childhood immunizations during the COVID-19 pandemic in Brazil: Analyses of routine statistics and a national household survey [20]. | 2021 | Qualitative: Ecological, time series study | Brazil: National with subnational statistics | About 20% decline in vaccination rates was seen in children 2 years or older during the months of March and April 2020 during the lockdown in comparison with January and February 2020. The least developed regions of the country were the most affected by missed immunization |
References
- Equity Reference Group. Who We Are/What We Do. Zero-Dose Community of Practice. Available online: https://www.zero-dose.org/services (accessed on 4 April 2023).
- UN-Habitat. World Cities Report 2022. Available online: https://unhabitat.org/sites/default/files/2022/06/wcr_2022.pdf (accessed on 4 April 2023).
- Equity Reference Group. Tackling Inequities in Immunization Outcomes in Urban Contexts. Available online: https://drive.google.com/file/d/1qB__5YAhyQiponTlL50a8y7h5LiTG_Kb/view (accessed on 4 April 2023).
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 4 April 2023).
- Ota, M.O.C.; Badur, S.; Romano-Mazzotti, L.; Friedland, L.R. Impact of COVID-19 pandemic on routine immunization. Ann. Med. 2021, 53, 2286–2297. [Google Scholar] [CrossRef] [PubMed]
- Chandir, S.; Siddiqi, D.A.; Mehmood, M.; Setayesh, H.; Siddique, M.; Mirza, A.; Soundardjee, R.; Dharma, V.K.; Shah, M.T.; Abdullah, S.; et al. Impact of COVID-19 pandemic response on uptake of routine immunizations in Sindh, Pakistan: An analysis of provincial electronic immunization registry data. Vaccine 2020, 38, 7146–7155. [Google Scholar] [CrossRef] [PubMed]
- Causey, K.; Fullman, N.; Sorensen, R.J.D.; Galles, N.C.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, M.C.; Martinez-Piedra, R.; Sodha, S.V.; Velandia-González, M.P.; et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: A modelling study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef] [PubMed]
- Wigley, A.; Lorin, J.; Hogan, D.; Utazi, C.E.; Hagedorn, B.; Dansereau, E.; Tatem, A.J.; Tejedor-Garavito, N. Estimates of the number and distribution of zero-dose and under-immunised children across remote-rural, urban, and conflict-affected settings in low and middle-income countries. PLOS Glob. Public Health 2022, 2, e0001126. [Google Scholar] [CrossRef]
- Immunization Agenda. (IA2030). Scorecard. Available online: http://scorecard.immunizationagenda2030.org/ (accessed on 4 April 2023).
- World Health Organization. Implementing the Immunization Agenda 2030. 2021. Available online: https://www.who.int/publications/m/item/implementing-the-immunization-agenda-2030 (accessed on 7 January 2021).
- UNICEF. Catch-Up|Restore|Strengthen: Immunization Recovery Plan 2023–2025. 2022. Available online: https://apps.who.int/gb/MSPI/pdf_files/2023/03/Item1_24-03.pdf (accessed on 4 April 2023).
- World Bank. Urban Population (% of Total Population). Available online: https://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS (accessed on 4 April 2023).
- UIWG. Urban Immunization Working Group Terms of Reference. Available online: https://www3.paho.org/hq/index.php?option=com_content&view=article&id=14086:tag-onvpd-tor&Itemid=0&lang=en#gsc.tab=0 (accessed on 4 April 2023).
- Silva, T.M.R.D.; Sá, A.C.M.G.N.D.; Prates, E.J.S.; Rodrigues, D.E.; Silva, T.P.R.D.; Matozinhos, F.P.; Vieira, E.W.R. Yellow fever vaccination before and during the COVID-19 pandemic in Brazil. Rev. Saude Publica 2022, 56, 45. [Google Scholar] [CrossRef]
- Sahoo, K.C.; Doley, C.; Negi, S.; Das, S.; Verma, P.; Kanungo, S.; Pati, S. Experiences of Urban Slum-Dwelling Women with Maternal and Child Health Services During COVID-19 Pandemic: A Multi-City Qualitative Study From India. Int. J. Public Health 2022, 67, 1604348. [Google Scholar] [CrossRef]
- Manzoor, A.; Abbasi, N.B.; Khizar, N.; Khalil, M.; Anjum, S.; Iqbal, A. Impact of COVID-19 pandemic on routine immunization of children. Rawal Med. J. 2022, 47, 45–48. [Google Scholar]
- Asmare, G.; Madalicho, M.; Sorsa, A. Disparities in full immunization coverage among urban and rural children aged 12–23 months in southwest Ethiopia: A comparative cross-sectional study. Hum. Vaccines Immunother. 2022, 18, 2101316. [Google Scholar] [CrossRef]
- Carter, E.D.; Zimmerman, L.; Qian, J.; Roberton, T.; Seme, A.; Shiferaw, S. Impact of the Early Stages of the COVID-19 Pandemic on Coverage of Reproductive, Maternal, and Newborn Health Interventions in Ethiopia: A Natural Experiment. Front. Public Health 2022, 10, 778413. [Google Scholar] [CrossRef]
- Chelo, D.; Nguefack, F.; Enyama, D.; Nansseu, R.; Tefoueyet, G.F.; Awa, H.M.; Nkwelle, I.M.; Nguefack-Tsague, G.; Ndenbe, P.; Ndombo, P.K. Impact and projections of the COVID-19 epidemic on attendance and routine vaccinations at a pediatric referral hospital in Cameroon. Arch. Pediatr. 2021, 28, 441–450. [Google Scholar] [CrossRef]
- Silveira, M.F.; Tonial, C.T.; Maranhão, A.G.K.; Teixeira, A.M.; Hallal, P.C.; Menezes, A.M.B.; Horta, B.L.; Hartwig, F.P.; Barros, A.J.; Victora, C.G. Missed childhood immunizations during the COVID-19 pandemic in Brazil: Analyses of routine statistics and of a national household survey. Vaccine 2021, 39, 3404–3409. [Google Scholar] [CrossRef]
- Dheresa, M.; Dessie, Y.; Negash, B.; Balis, B.; Getachew, T.; Mamo Ayana, G.; Merga, B.T.; Regassa, L.D. Child Vaccination Coverage, Trends and Predictors in Eastern Ethiopia: Implication for Sustainable Development Goals. J. Multidiscip. Healthc. 2021, 14, 2657–2667. [Google Scholar] [CrossRef]
- Dirirsa, K.; Makuria, M.; Mulu, E.; Deriba, B.S. Assessment of vaccination timeliness and associated factors among children in Toke Kutaye district, central Ethiopia: A Mixed study. PLoS ONE 2022, 17, e0262320. [Google Scholar] [CrossRef]
- Rabiu, K.A.; Alausa, T.G.; Akinlusi, F.M.; Davies, N.O.; Shittu, K.A.; Akinola, O.I. Parental acceptance of human papillomavirus vaccination for adolescent girls in Lagos, Nigeria. J. Fam. Med. Prim. Care 2020, 9, 2950–2957. [Google Scholar] [CrossRef]
- Tadesse, A.; Sahlu, D.; Benayew, M. Second-dose measles vaccination and associated factors among under-five children in urban areas of North Shoa Zone, Central Ethiopia, 2022. Front. Public Health 2022, 10, 1029740. [Google Scholar] [CrossRef]
- Landicho-Guevarra, J.; Reñosa, M.D.C.; Wachinger, J.; Endoma, V.; Aligato, M.F.; Bravo, T.A.; Landicho, J.; Bärnighausen, K.; A McMahon, S. Scared, powerless, insulted and embarrassed: Hesitancy towards vaccines among caregivers in Cavite Province, the Philippines. BMJ Glob. Health 2021, 6, e006529. [Google Scholar] [CrossRef]
- Mekonnen, Z.A.; Nigus, M.; Assefa, S.; Biru, A.; Teklu, A.; Feletto, M.; Gera, R.; Ba-Nguz, A.; Tilahun, B. Strategies to revitalize immunization service provision in urban settings of Ethiopia. Ethiop. J. Health Dev. 2021, 35, 98–110. [Google Scholar]
- Balogun, F.; Bamidele, O.; Bamgboye, E. Effect of intensive training in improving older women’s knowledge and support for infant vaccination in Nigerian urban slums: A before-and-after intervention study. BMC Public Health 2021, 21, 266. [Google Scholar] [CrossRef]
- Baroni, L.; Alves, R.F.S.; Boccolini, C.S.; Salles, R.; Gritz, R.; Paixão, B.; Boccolini, P.D.M.M. Database on the coverage of the “Bolsa-Familia” conditioning cash-transfer program: Brazil, 2005 to 2021. BMC Res. Notes 2021, 14, 435. [Google Scholar] [CrossRef]
- Larkin, H.D. Backslide in Global Childhood Vaccinations. JAMA 2022, 328, 1029. [Google Scholar] [CrossRef]
- Maina, L.C.; Karanja, S.; Kombich, J. Immunization coverage and its determinants among children aged 12–23 months in a peri-urban area of Kenya. Pan. Afr. Med. J. 2013, 14, 3. [Google Scholar] [CrossRef] [PubMed]
- Tefera, Y.A.; Wagner, A.L.; Mekonen, E.B.; Carlson, B.F.; Boulton, M.L. Predictors and Barriers to Full Vaccination among Children in Ethiopia. Vaccines 2018, 6, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crocker-Buque, T.; Mindra, G.; Duncan, R.; Mounier-Jack, S. Immunization, urbanization and slums—A systematic review of factors and interventions. BMC Public Health 2017, 17, 556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadari, I.; Higgins-Steele, A.; Sharkey, A.; Charlet, D.; Shahabuddin, A.; Nandy, R.; Jackson, D. Pro-equity immunization and health systems strengthening strategies in select Gavi-supported countries. Vaccine 2021, 39, 2434–2444. [Google Scholar] [CrossRef]
- Siddiqui, F.A.; Padhani, Z.A.; Salam, R.A.; Aliani, R.; Lassi, Z.S.; Das, J.K.; Bhutta, Z.A. Interventions to Improve Immunization Coverage Among Children and Adolescents: A Meta-analysis. Pediatrics 2022, 149 (Suppl. 5), e2021053852D. [Google Scholar] [CrossRef]
- United Nations International Children’s Emergency Fund. Urban Immunization Toolkit; UNICEF: New York, NY, USA, 2018. [Google Scholar]
- Gurnani, V.; Haldar, P.; Aggarwal, M.K.; Das, M.K.; Chauhan, A.; Murray, J.; Arora, N.K.; Jhalani, M.; Sudan, P. Improving vaccination coverage in India: Lessons from Intensified Mission Indradhanush, a cross-sectoral systems strengthening strategy. BMJ 2018, 363, k4782. [Google Scholar] [CrossRef] [Green Version]
- WorldPop and National Population Commission of Nigeria. Bottom-Up Gridded Population Estimates for Nigeria; Version 2.0; WorldPop, University of Southampton: Southampton, UK, 2021. [Google Scholar]


{kind=link}
| Criteria | Inclusion | Exclusion |
|---|---|---|
| Language | English, Spanish, French | Other languages |
| Dates | March 2020–January 2023 | Before March 2020, unless analysis reviews general immunization trends pre-March 2020 to post-March 2020 |
| Database | PubMed (NCBI), Web of Science (Clarivate) | Other databases |
| Vaccines | All routine vaccines administered to children up to age of 18 years. | Exclude COVID vaccines and vaccines administered to adults >18 years. |
| Topic | COVID-19 impact on routine immunization and recovery | Articles which do not focus on the COVID-19 impact on routine immunization and recovery |
| Geographic Location (Countries) | India, Nigeria, Indonesia, Ethiopia, Philippines, Democratic Republic of the Congo, Brazil, Pakistan, Angola, Myanmar, United Republic of Tanzania, Mozambique, Afghanistan, Somalia, Mexico, Madagascar, Cameroon, Democratic People’s Republic of Korea, Chad, Vietnam | All other countries |
| Geographic Location (Urban) | Urban and peri-urban, cities, Urban vs. rural analysis | Rural |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dadari, I.; Belt, R.V.; Iyengar, A.; Ray, A.; Hossain, I.; Ali, D.; Danielsson, N.; Sodha, S.V.; The Global Urban Immunization Working Group. Achieving the IA2030 Coverage and Equity Goals through a Renewed Focus on Urban Immunization. Vaccines 2023, 11, 809. https://doi.org/10.3390/vaccines11040809
Dadari I, Belt RV, Iyengar A, Ray A, Hossain I, Ali D, Danielsson N, Sodha SV, The Global Urban Immunization Working Group. Achieving the IA2030 Coverage and Equity Goals through a Renewed Focus on Urban Immunization. Vaccines. 2023; 11(4):809. https://doi.org/10.3390/vaccines11040809
Chicago/Turabian StyleDadari, Ibrahim, Rachel V. Belt, Ananya Iyengar, Arindam Ray, Iqbal Hossain, Daniel Ali, Niklas Danielsson, Samir V. Sodha, and The Global Urban Immunization Working Group. 2023. "Achieving the IA2030 Coverage and Equity Goals through a Renewed Focus on Urban Immunization" Vaccines 11, no. 4: 809. https://doi.org/10.3390/vaccines11040809