
Assessing Geographic Overlap between Zero-Dose Diphtheria–Tetanus–Pertussis Vaccination Prevalence and Other Health Indicators

Abstract
:1. Introduction
2. Materials and Methods
2.1. Geospatial Estimation of Vaccination Coverage
2.2. Spatial Estimates of Other Health Indicators
2.3. Analyses of Spatial Overlap
2.4. Ethical Approval and Reporting Guidelines
3. Results
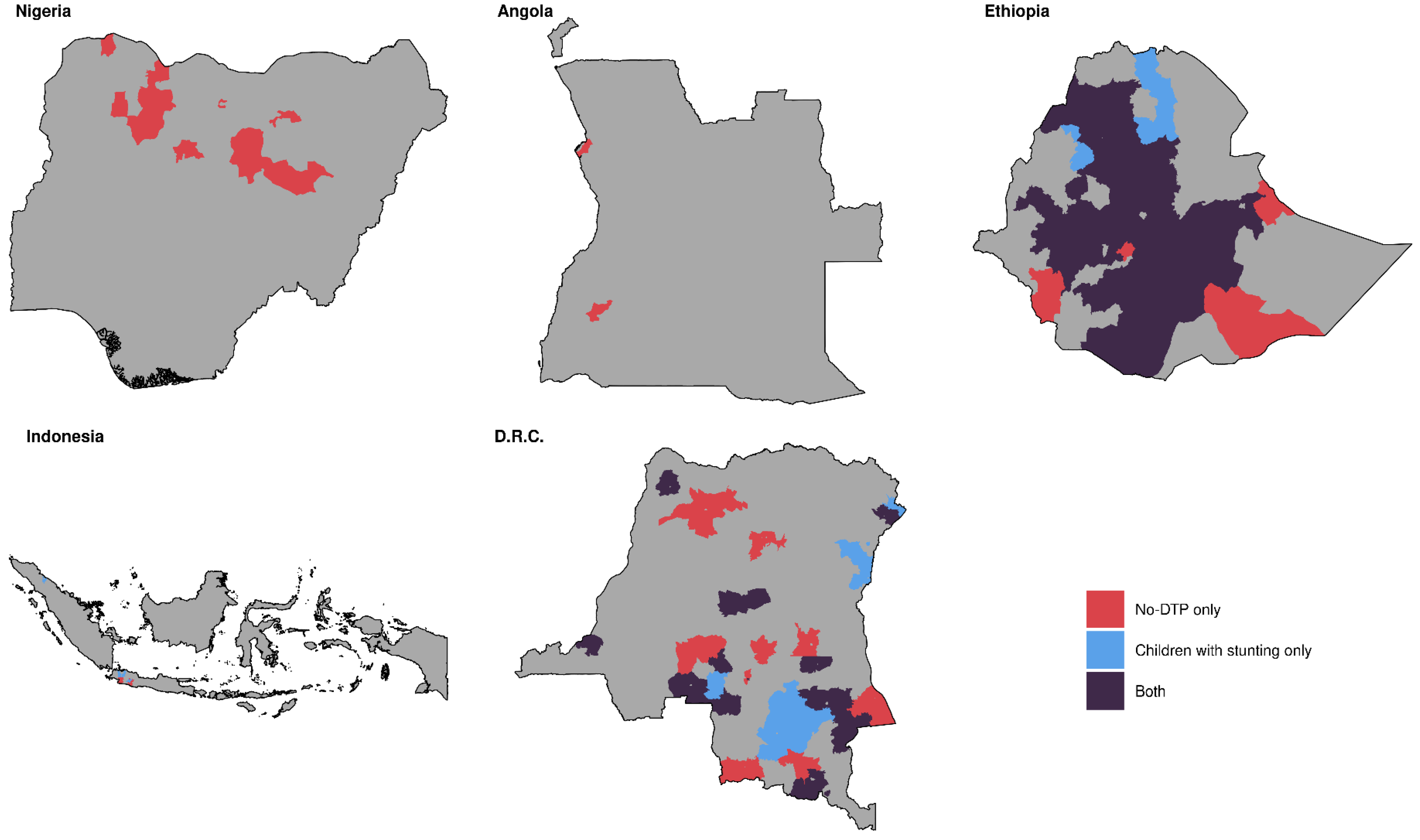
3.1. Mapping Overlap
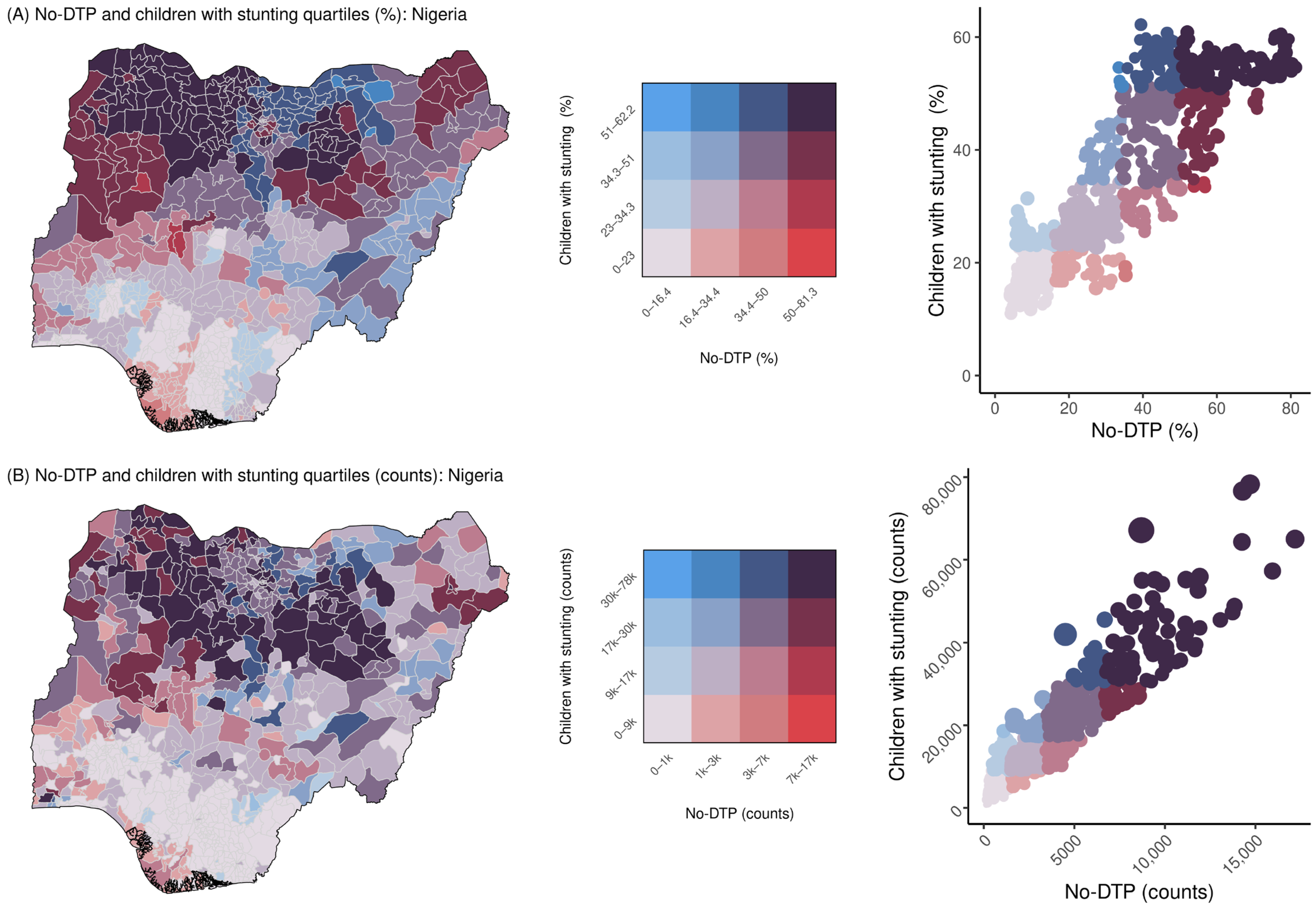
3.1.1. Country-Specific Overlap by Prevalence
3.1.2. Country-Specific Overlap by Counts
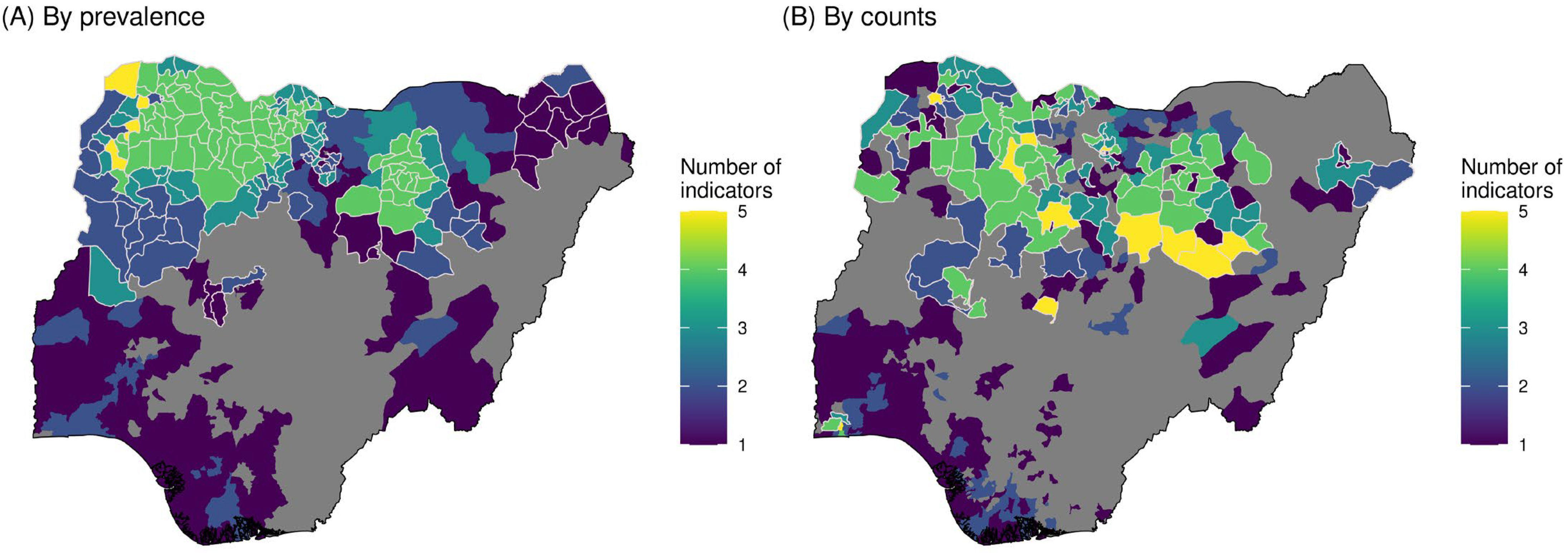
3.1.3. Overlap for Multiple Indicators
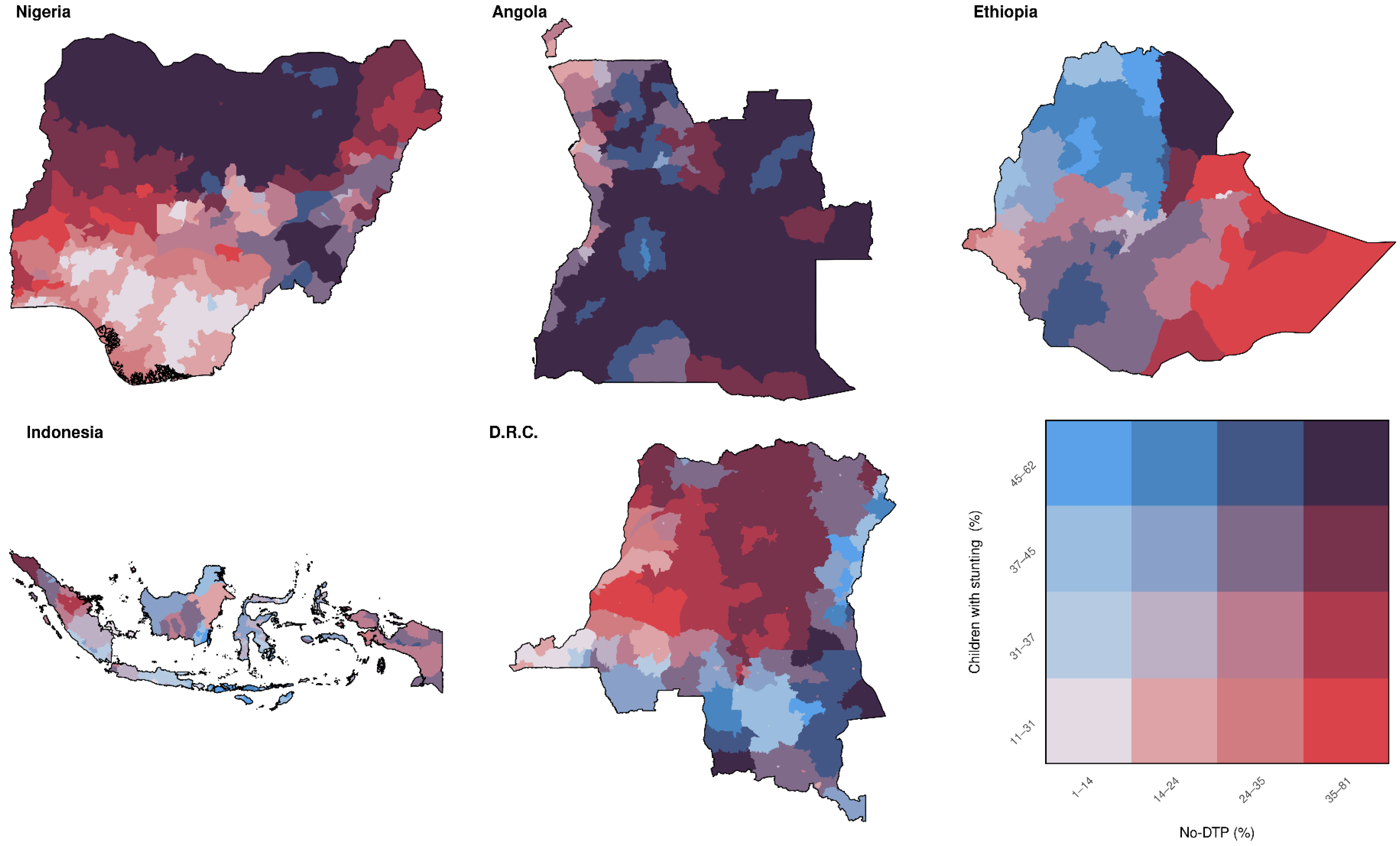
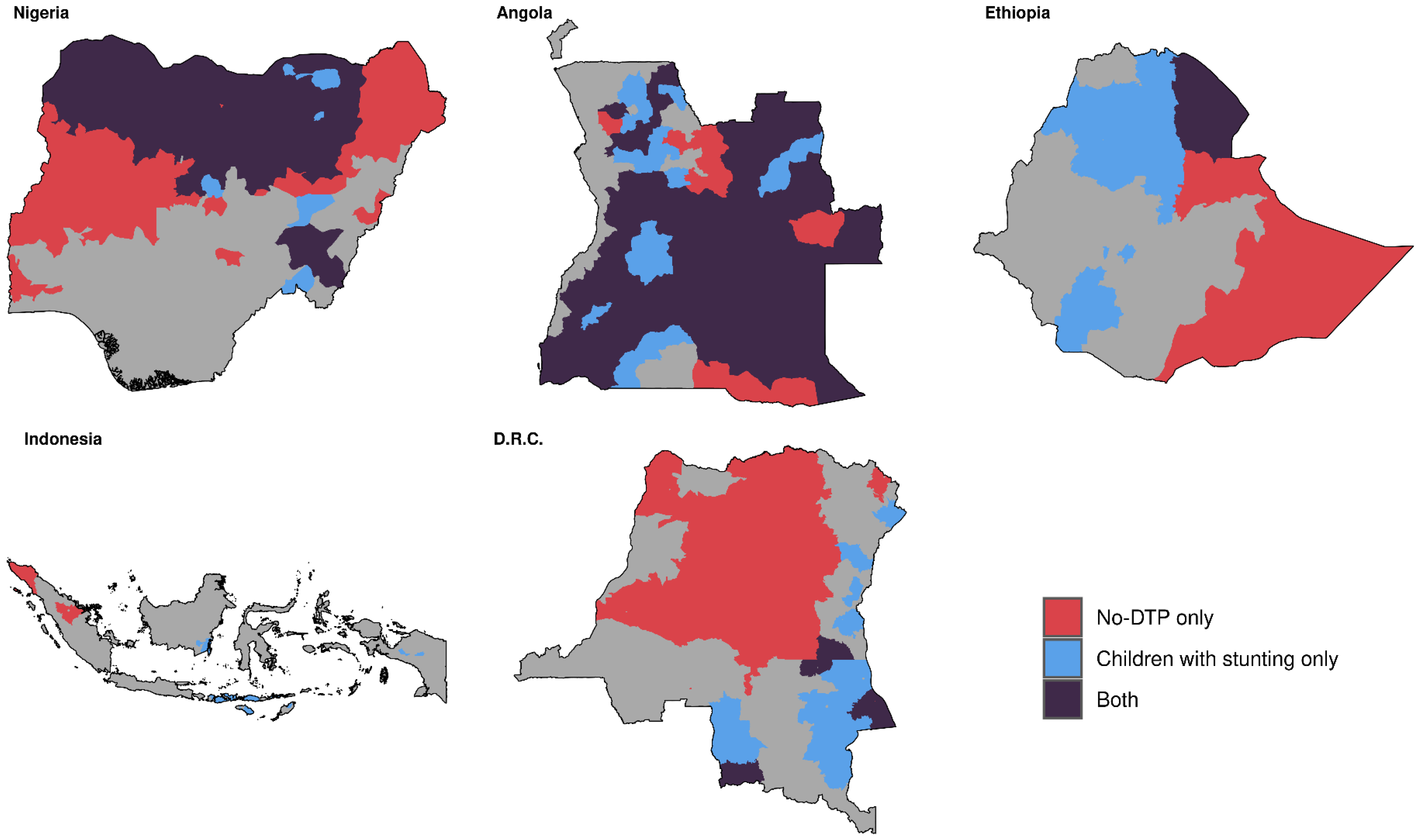
3.1.4. Multinational Overlap by Prevalence
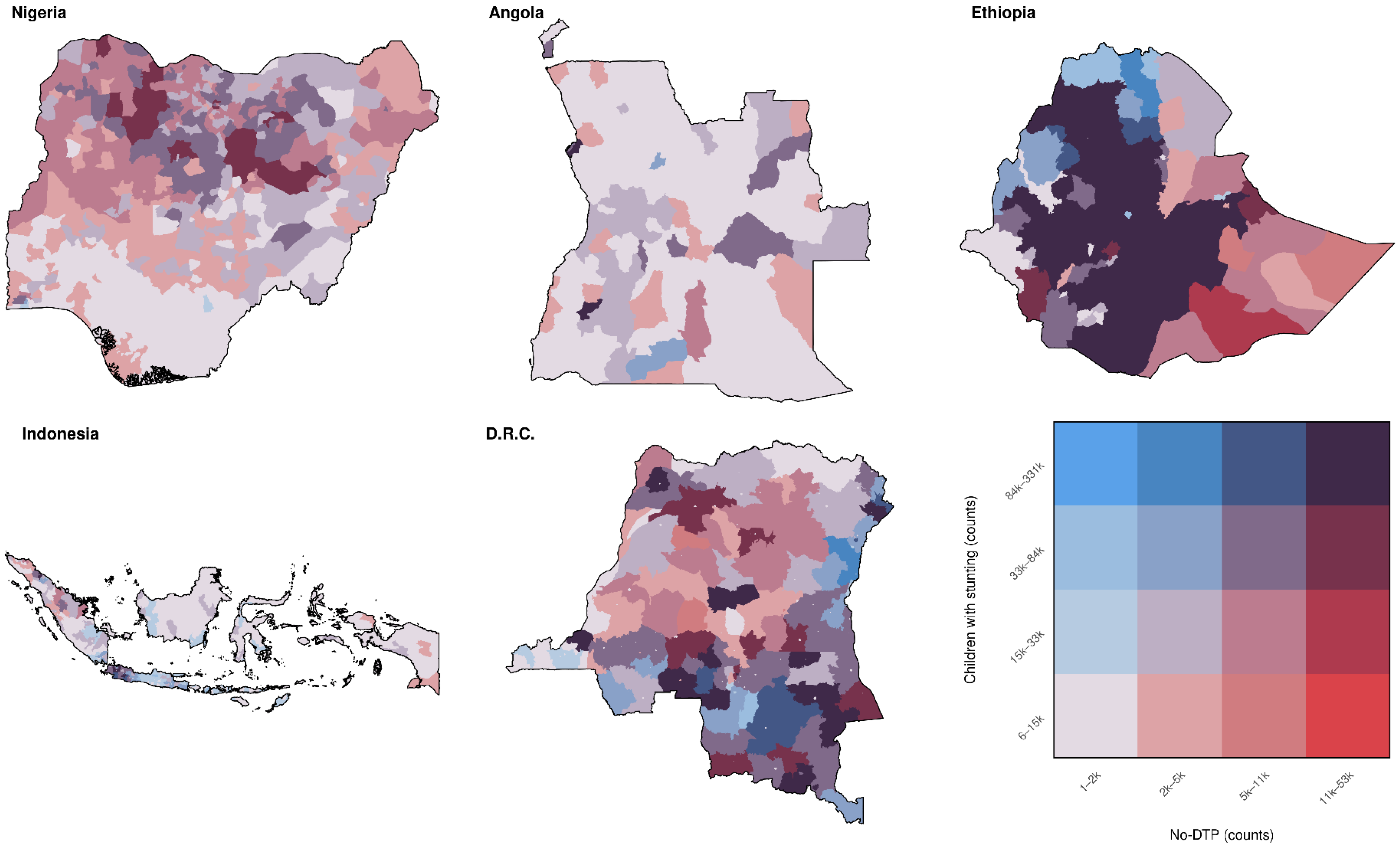
3.1.5. Multinational Overlap by Counts
3.2. Quantifying Spatial Overlap
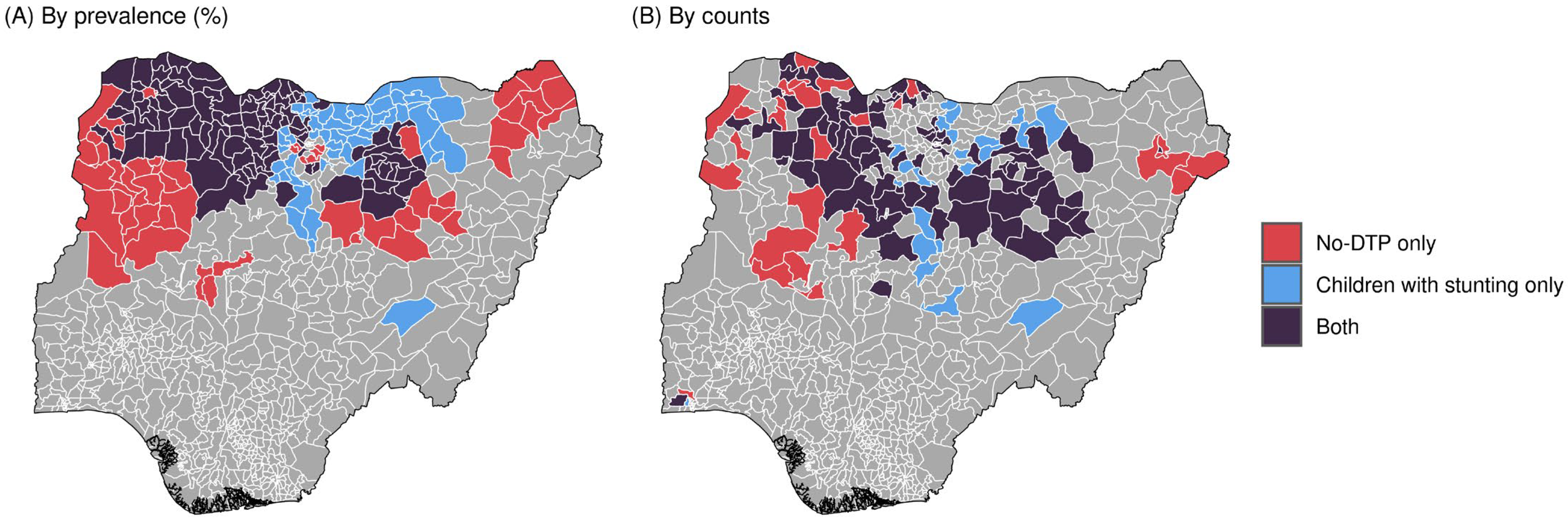
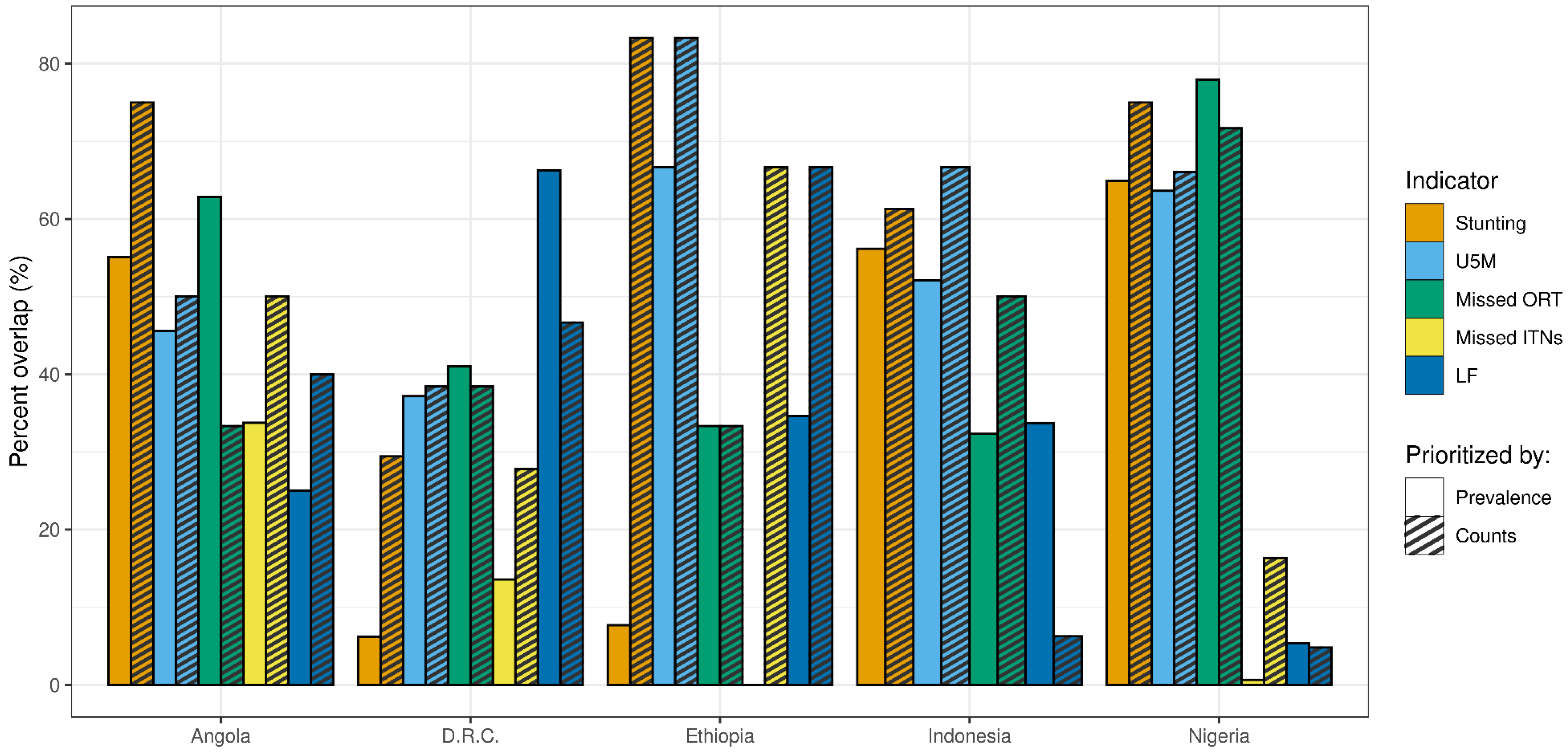
3.2.1. Percent Overlap of High-Quartile Districts
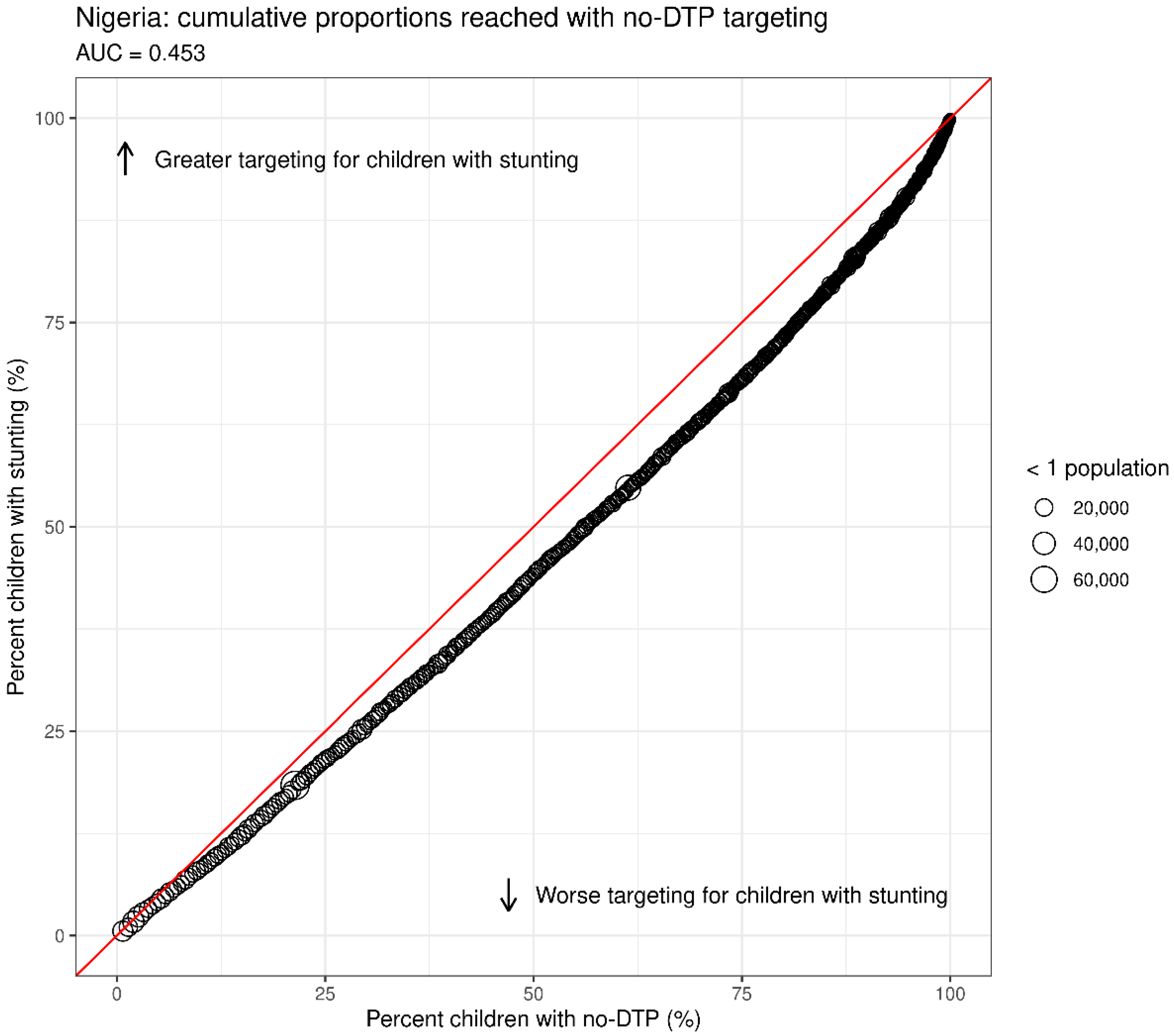
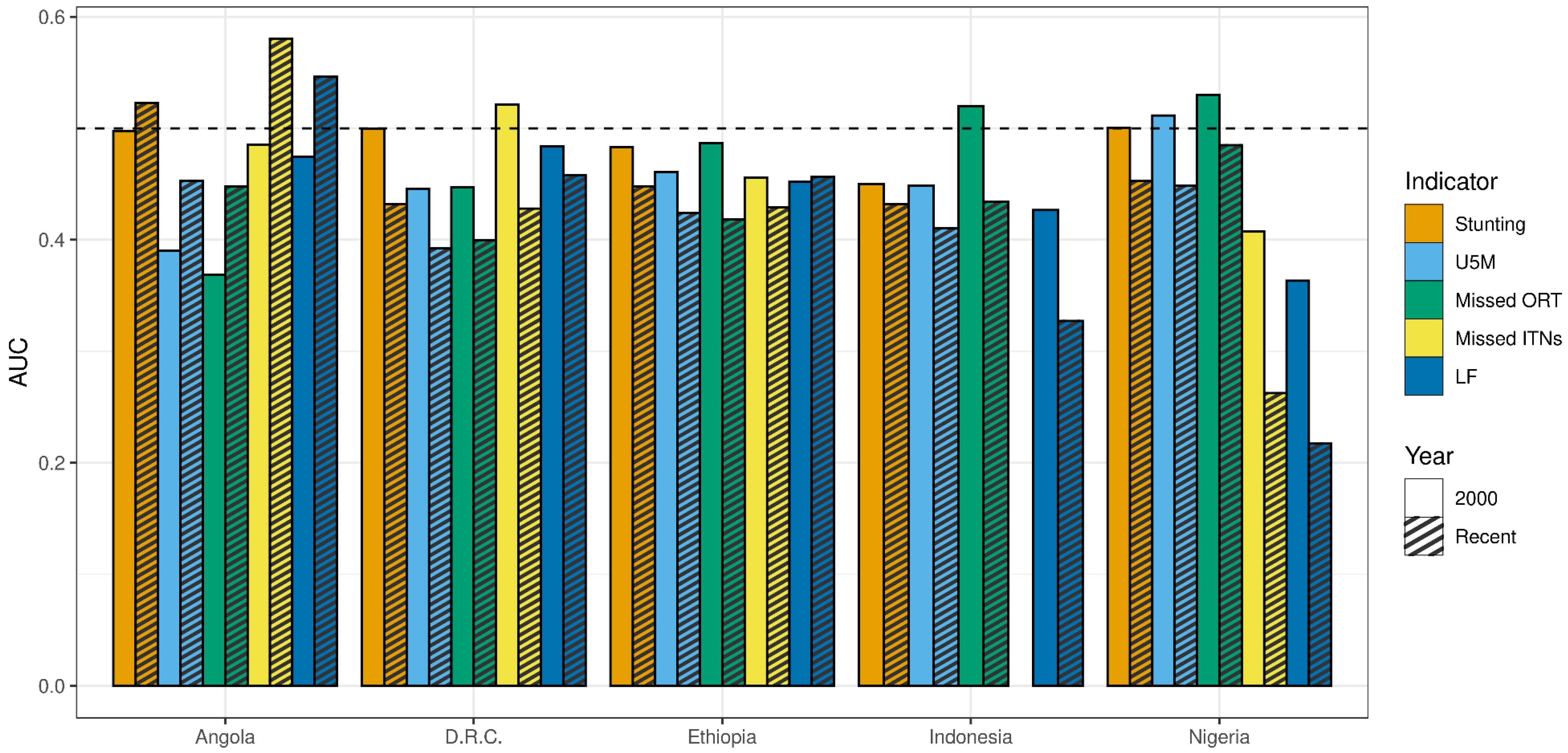
3.2.2. AUC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Essential Programme on Immunization. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization (accessed on 2 February 2023).
- Toor, J.; Echeverria-Londono, S.; Li, X.; Abbas, K.; Carter, E.D.; Clapham, H.E.; Clark, A.; De Villiers, M.J.; Eilertson, K.; Ferrari, M.; et al. Lives Saved with Vaccination for 10 Pathogens across 112 Countries in a Pre-COVID-19 World. ELife 2021, 10, e67635. [Google Scholar] [CrossRef]
- Galles, N.C.; Liu, P.Y.; Updike, R.L.; Fullman, N.; Nguyen, J.; Rolfe, S.; Sbarra, A.N.; Schipp, M.F.; Marks, A.; Abady, G.G.; et al. Measuring Routine Childhood Vaccination Coverage in 204 Countries and Territories, 1980–2019: A Systematic Analysis for the Global Burden of Disease Study 2020, Release 1. Lancet 2021, 398, 503–521. [Google Scholar] [CrossRef]
- WHO & UNICEF. WHO/UNICEF Estimates of National Immunization Coverage. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/who-unicef-estimates-of-national-immunization-coverage (accessed on 2 February 2023).
- Causey, K.; Fullman, N.; Sorensen, R.J.D.; Galles, N.C.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, M.C.; Martinez-Piedra, R.; Sodha, S.V.; Velandia-González, M.P.; et al. Estimating Global and Regional Disruptions to Routine Childhood Vaccine Coverage during the COVID-19 Pandemic in 2020: A Modelling Study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef] [PubMed]
- WHO. COVID-19 Pandemic Fuels Largest Continued Backslide in Vaccinations in Three Decades. Available online: https://www.who.int/news/item/15-07-2022-covid-19-pandemic-fuels-largest-continued-backslide-in-vaccinations-in-three-decades (accessed on 2 February 2023).
- WHO. Immunization Agenda 2030: A Global Strategy to Leave No One Behind. Available online: http://www.who.int/immunization/immunization_agenda_2030/en/ (accessed on 2 February 2023).
- Joint SDG Fund Sustainable Development Goals. Available online: https://jointsdgfund.org/sustainable-development-goals/goal-3-good-health-and-well-being (accessed on 2 February 2023).
- Wallace, A.S.; Ryman, T.K.; Privor-Dumm, L.; Morgan, C.; Fields, R.; Garcia, C.; Sodha, S.V.; Lindstrand, A.; Nic Lochlainn, L.M. Leaving No One behind: Defining and Implementing an Integrated Life Course Approach to Vaccination across the next Decade as Part of the Immunization Agenda 2030. Vaccine 2022, S0264410X22014529. [Google Scholar] [CrossRef]
- WHO. Implementing the Immunization Agenda. 2023. Available online: https://www.who.int/publications/m/item/implementing-the-immunization-agenda-2030 (accessed on 2 February 2023).
- Cata-Preta, B.O.; Santos, T.M.; Mengistu, T.; Hogan, D.R.; Barros, A.J.D.; Victora, C.G. Zero-Dose Children and the Immunisation Cascade: Understanding Immunisation Pathways in Low and Middle-Income Countries. Vaccine 2021, 39, 4564–4570. [Google Scholar] [CrossRef]
- Wendt, A.; Santos, T.M.; Cata-Preta, B.O.; Arroyave, L.; Hogan, D.R.; Mengistu, T.; Barros, A.J.D.; Victora, C.G. Exposure of Zero-Dose Children to Multiple Deprivation: Analyses of Data from 80 Low- and Middle-Income Countries. Vaccines 2022, 10, 1568. [Google Scholar] [CrossRef]
- Wigley, A.; Lorin, J.; Hogan, D.; Utazi, C.E.; Hagedorn, B.; Dansereau, E.; Tatem, A.J.; Tejedor-Garavito, N. Estimates of the Number and Distribution of Zero-Dose and under-Immunised Children across Remote-Rural, Urban, and Conflict-Affected Settings in Low and Middle-Income Countries. PLoS Glob. Public Health 2022, 2, e0001126. [Google Scholar] [CrossRef]
- Santos, T.M.; Cata-Preta, B.O.; Mengistu, T.; Victora, C.G.; Hogan, D.R.; Barros, A.J.D. Assessing the Overlap between Immunisation and Other Essential Health Interventions in 92 Low- and Middle-Income Countries Using Household Surveys: Opportunities for Expanding Immunisation and Primary Health Care. eClinicalMedicine 2021, 42, 101196. [Google Scholar] [CrossRef] [PubMed]
- Johri, M.; Rajpal, S.; Subramanian, S.V. Progress in Reaching Unvaccinated (Zero-Dose) Children in India, 1992–2016: A Multilevel, Geospatial Analysis of Repeated Cross-Sectional Surveys. Lancet Glob. Health 2021, 9, e1697–e1706. [Google Scholar] [CrossRef]
- Restrepo-Méndez, M.C.; Barros, A.J.D.; Wong, K.L.M.; Johnson, H.L.; Pariyo, G.; Wehrmeister, F.C.; Victora, C.G. Missed Opportunities in Full Immunization Coverage: Findings from Low- and Lower-Middle-Income Countries. Glob. Health Action 2016, 9, 30963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosser, J.F.; Gagne-Maynard, W.; Rao, P.C.; Osgood-Zimmerman, A.; Fullman, N.; Graetz, N.; Burstein, R.; Updike, R.L.; Liu, P.Y.; Ray, S.E. Mapping Diphtheria-Pertussis-Tetanus Vaccine Coverage in Africa, 2000–2016: A Spatial and Temporal Modelling Study. Lancet 2019, 393, 1843–1855. [Google Scholar] [PubMed] [Green Version]
- Sbarra, A.N.; Rolfe, S.; Nguyen, J.Q.; Earl, L.; Galles, N.C.; Marks, A.; Abbas, K.M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; et al. Mapping Routine Measles Vaccination in Low- and Middle-Income Countries. Nature 2021, 589, 415–419. [Google Scholar] [CrossRef]
- Takahashi, S.; Metcalf, C.J.E.; Ferrari, M.J.; Tatem, A.J.; Lessler, J. The Geography of Measles Vaccination in the African Great Lakes Region. Nat. Commun. 2017, 8, 15585. [Google Scholar] [CrossRef] [Green Version]
- Utazi, C.E.; Aheto, J.M.K.; Wigley, A.; Tejedor-Garavito, N.; Bonnie, A.; Nnanatu, C.C.; Wagai, J.; Williams, C.; Setayesh, H.; Tatem, A.J.; et al. Mapping the Distribution of Zero-Dose Children to Assess the Performance of Vaccine Delivery Strategies and Their Relationships with Measles Incidence in Nigeria. Vaccine 2023, 41, 170–181. [Google Scholar] [CrossRef]
- Utazi, C.E.; Aheto, J.M.K.; Chan, H.M.T.; Tatem, A.J.; Sahu, S.K. Conditional Probability and Ratio-Based Approaches for Mapping the Coverage of Multi-Dose Vaccines. Stat. Med. 2022, 41, 5662–5678. [Google Scholar] [CrossRef]
- Burgert-Brucker, C.R.; Dontamsetti, T.; Gething, P.W. The DHS Program’s Modeled Surfaces Spatial Datasets. Stud. Fam. Plan. 2018, 49, 87–92. [Google Scholar] [CrossRef]
- Dimitrova, A.; Carrasco-Escobar, G.; Richardson, R.; Benmarhnia, T. Essential Childhood Immunization in 43 Low- and Middle-Income Countries: Analysis of Spatial Trends and Socioeconomic Inequalities in Vaccine Coverage. PLoS Med. 2023, 20, e1004166. [Google Scholar] [CrossRef]
- Burstein, R.; Henry, N.J.; Collison, M.L.; Marczak, L.B.; Sligar, A.; Watson, S.; Marquez, N.; Abbasalizad-Farhangi, M.; Abbasi, M.; Abd-Allah, F.; et al. Mapping 123 Million Neonatal, Infant and Child Deaths between 2000 and 2017. Nature 2019, 574, 353–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinyoki, D.K.; Osgood-Zimmerman, A.E.; Pickering, B.V.; Schaeffer, L.E.; Marczak, L.B.; Lazzar-Atwood, A.; Collison, M.L.; Henry, N.J.; Abebe, Z.; Adamu, A.A.; et al. Mapping Child Growth Failure across Low- and Middle-Income Countries. Nature 2020, 577, 231–234. [Google Scholar] [CrossRef] [Green Version]
- Haeuser, E.; Serfes, A.L.; Cork, M.A.; Yang, M.; Abbastabar, H.; Abhilash, E.S.; Adabi, M.; Adebayo, O.M.; Adekanmbi, V.; Adeyinka, D.A.; et al. Mapping Age- and Sex-Specific HIV Prevalence in Adults in Sub-Saharan Africa, 2000–2018. BMC Med. 2022, 20, 488. [Google Scholar] [CrossRef]
- Deshpande, A.; Miller-Petrie, M.K.; Lindstedt, P.A.; Baumann, M.M.; Johnson, K.B.; Blacker, B.F.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; Abdollahpour, I.; et al. Mapping Geographical Inequalities in Access to Drinking Water and Sanitation Facilities in Low-Income and Middle-Income Countries, 2000–2017. Lancet Glob. Health 2020, 8, e1162–e1185. [Google Scholar] [CrossRef]
- Graetz, N.; Friedman, J.; Osgood-Zimmerman, A.; Burstein, R.; Biehl, M.H.; Shields, C.; Mosser, J.F.; Casey, D.C.; Deshpande, A.; Earl, L.; et al. Mapping Local Variation in Educational Attainment across Africa. Nature 2018, 555, 48–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrasco-Escobar, G.; Manrique, E.; Tello-Lizarraga, K.; Miranda, J.J. Travel Time to Health Facilities as a Marker of Geographical Accessibility Across Heterogeneous Land Coverage in Peru. Front. Public Health 2020, 8, 498. [Google Scholar] [CrossRef]
- Chamberlain, H.R.; Lazar, A.N.; Tatem, A.J. High-Resolution Estimates of Social Distancing Feasibility, Mapped for Urban Areas in Sub-Saharan Africa. Sci. Data 2022, 9, 711. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi-Villa, A.; Bever, C.A.; Koenker, H.; Weiss, D.J.; Vargas-Ruiz, C.; Nandi, A.K.; Gibson, H.S.; Harris, J.; Battle, K.E.; Rumisha, S.F.; et al. Maps and Metrics of Insecticide-Treated Net Access, Use, and Nets-per-Capita in Africa from 2000–2020. Nat. Commun. 2021, 12, 3589. [Google Scholar] [CrossRef] [PubMed]
- Unwin, H.J.T.; Mwandigha, L.; Winskill, P.; Ghani, A.C.; Hogan, A.B. Analysis of the Potential for a Malaria Vaccine to Reduce Gaps in Malaria Intervention Coverage. Malar. J. 2021, 20, 438. [Google Scholar] [CrossRef]
- World Health Organization. Health Equity Assessment Toolkit. Available online: https://www.who.int/data/health-equity/assessment_toolkit (accessed on 12 February 2023).
- Global Health Data Exchange. GHDx. Available online: http://ghdx.healthdata.org/ (accessed on 16 June 2020).
- WorldPop. WorldPop Dataset. Available online: https://hub.worldpop.org/ (accessed on 20 March 2020).
- Tatem, A.J. WorldPop, Open Data for Spatial Demography. Available online: https://www.nature.com/articles/sdata20174 (accessed on 17 January 2018).
- Global Administrative Areas. GADM Maps and Data. v.3.6. Available online: https://gadm.org/ (accessed on 4 December 2018).
- Wiens, K.E.; Lindstedt, P.A.; Blacker, B.F.; Johnson, K.B.; Baumann, M.M.; Schaeffer, L.E.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; Abdollahpour, I.; et al. Mapping Geographical Inequalities in Oral Rehydration Therapy Coverage in Low-Income and Middle-Income Countries, 2000–2017. Lancet Glob. Health 2020, 8, e1038–e1060. [Google Scholar] [CrossRef]
- Cromwell, E.A.; Schmidt, C.A.; Kwong, K.T.; Pigott, D.M.; Mupfasoni, D.; Biswas, G.; Shirude, S.; Hill, E.; Donkers, K.M.; Abdoli, A.; et al. The Global Distribution of Lymphatic Filariasis, 2000–2018: A Geospatial Analysis. Lancet Glob. Health 2020, 8, e1186–e1194. [Google Scholar] [CrossRef]
- Wallace, A.; Dietz, V.; Cairns, K.L. Integration of Immunization Services with Other Health Interventions in the Developing World: What Works and Why? Systematic Literature Review. Trop. Med. Int. Health 2009, 14, 11–19. [Google Scholar] [CrossRef]
- World Health Organization; United Nations Children’s Fund (UNICEF). Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025: The Integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD); World Health Organization: Geneva, Switzerland, 2013; ISBN 978-92-4-150523-9. [Google Scholar]
- Olofin, I.; McDonald, C.M.; Ezzati, M.; Flaxman, S.; Black, R.E.; Fawzi, W.W.; Caulfield, L.E.; Danaei, G.; Membership for the Nutrition Impact Model Study (anthropometry cohort pooling). Associations of Suboptimal Growth with All-Cause and Cause-Specific Mortality in Children under Five Years: A Pooled Analysis of Ten Prospective Studies. PLoS ONE 2013, 8, e64636. [Google Scholar] [CrossRef] [Green Version]
- Prendergast, A.J. Malnutrition and Vaccination in Developing Countries. Phil. Trans. R. Soc. B 2015, 370, 20140141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mejía-Guevara, I.; Zuo, W.; Bendavid, E.; Li, N.; Tuljapurkar, S. Age Distribution, Trends, and Forecasts of under-5 Mortality in 31 Sub-Saharan African Countries: A Modeling Study. PLoS Med. 2019, 16, e1002757. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. GVIS: Global Immunization Vision and Strategy 2006–2015; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- World Health Organization. Global Vaccine Action Plan 2011–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Working Together: An Integration Resource Guide for Immunization Services throughout the Life Course; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-151473-6. [Google Scholar]
- Partapuri, T.; Steinglass, R.; Sequeira, J. Integrated Delivery of Health Services During Outreach Visits: A Literature Review of Program Experience Through a Routine Immunization Lens. J. Infect. Dis. 2012, 205, S20–S27. [Google Scholar] [CrossRef]
- Stevens, G.A.; Alkema, L.; Black, R.E.; Boerma, J.T.; Collins, G.S.; Ezzati, M.; Grove, J.T.; Hogan, D.R.; Hogan, M.C.; Horton, R.; et al. Guidelines for Accurate and Transparent Health Estimates Reporting: The GATHER Statement. The Lancet 2016, 388, e19–e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faraway, J.J. Linear Models with R; Chapman & Hall/CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar]
- R Core Team R. A Language and Environment for Statistical Computing. 2022. Available online: https://www.utstat.toronto.edu/~brunner/books/LinearModelsWithR.pdf (accessed on 2 February 2023).
- Rue, H.; Martino, S.; Chopin, N. Approximate Bayesian Inference for Latent Gaussian Models by Using Integrated Nested Laplace Approximations. J. R. Stat. Soc. Ser. B (Stat. Methodol.) 2009, 71, 319–392. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | Definition | Example Countries Available | Most Recent Year Available | Target Population Age Range | Citation |
|---|---|---|---|---|---|
| No-DTP | No-DTP prevalence rate | Angola, DRC, Ethiopia, Indonesia, Nigeria | 2019 | Under 1 year | Mosser, J.F. et al. [17] * |
| Stunting | Stunting prevalence rate | Angola, DRC, Ethiopia, Indonesia, Nigeria | 2019 | Under 5 years | Kinyoki, D.K. et al. [25] |
| U5M | Mortality probability and death counts | Angola, DRC, Ethiopia, Indonesia, Nigeria | 2017 | Under 5 years | Burstein, R. et al. [24] |
| Missed ORT | (1–ORT coverage) for children who had diarrhea | Angola, DRC, Ethiopia, Indonesia, Nigeria | 2017 | Under 5 years | Wiens, K.E. et al. [38] |
| Missed ITNs | (1–proportion of population that sleeps under an ITN) | Angola, DRC, Ethiopia, Nigeria | 2019 | All ages | Bertozzi-Villa, A. et al. [31] |
| LF | LF prevalence rate | Angola, DRC, Ethiopia, Indonesia, Nigeria | 2018 | All ages | Cromwell, E.A. et al. [39] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haeuser, E.; Nguyen, J.Q.; Rolfe, S.; Nesbit, O.; Fullman, N.; Mosser, J.F. Assessing Geographic Overlap between Zero-Dose Diphtheria–Tetanus–Pertussis Vaccination Prevalence and Other Health Indicators. Vaccines 2023, 11, 802. https://doi.org/10.3390/vaccines11040802
Haeuser E, Nguyen JQ, Rolfe S, Nesbit O, Fullman N, Mosser JF. Assessing Geographic Overlap between Zero-Dose Diphtheria–Tetanus–Pertussis Vaccination Prevalence and Other Health Indicators. Vaccines. 2023; 11(4):802. https://doi.org/10.3390/vaccines11040802
Chicago/Turabian StyleHaeuser, Emily, Jason Q. Nguyen, Sam Rolfe, Olivia Nesbit, Nancy Fullman, and Jonathan F. Mosser. 2023. "Assessing Geographic Overlap between Zero-Dose Diphtheria–Tetanus–Pertussis Vaccination Prevalence and Other Health Indicators" Vaccines 11, no. 4: 802. https://doi.org/10.3390/vaccines11040802