
Inequalities in Immunization against Maternal and Neonatal Tetanus: A Cross-Sectional Analysis of Protection at Birth Coverage Using Household Health Survey Data from 76 Countries
 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Outcome
2.3. Dimensions of Inequality
2.4. Statistical Analyses
- Median coverage by subgroup of each inequality dimension, overall;
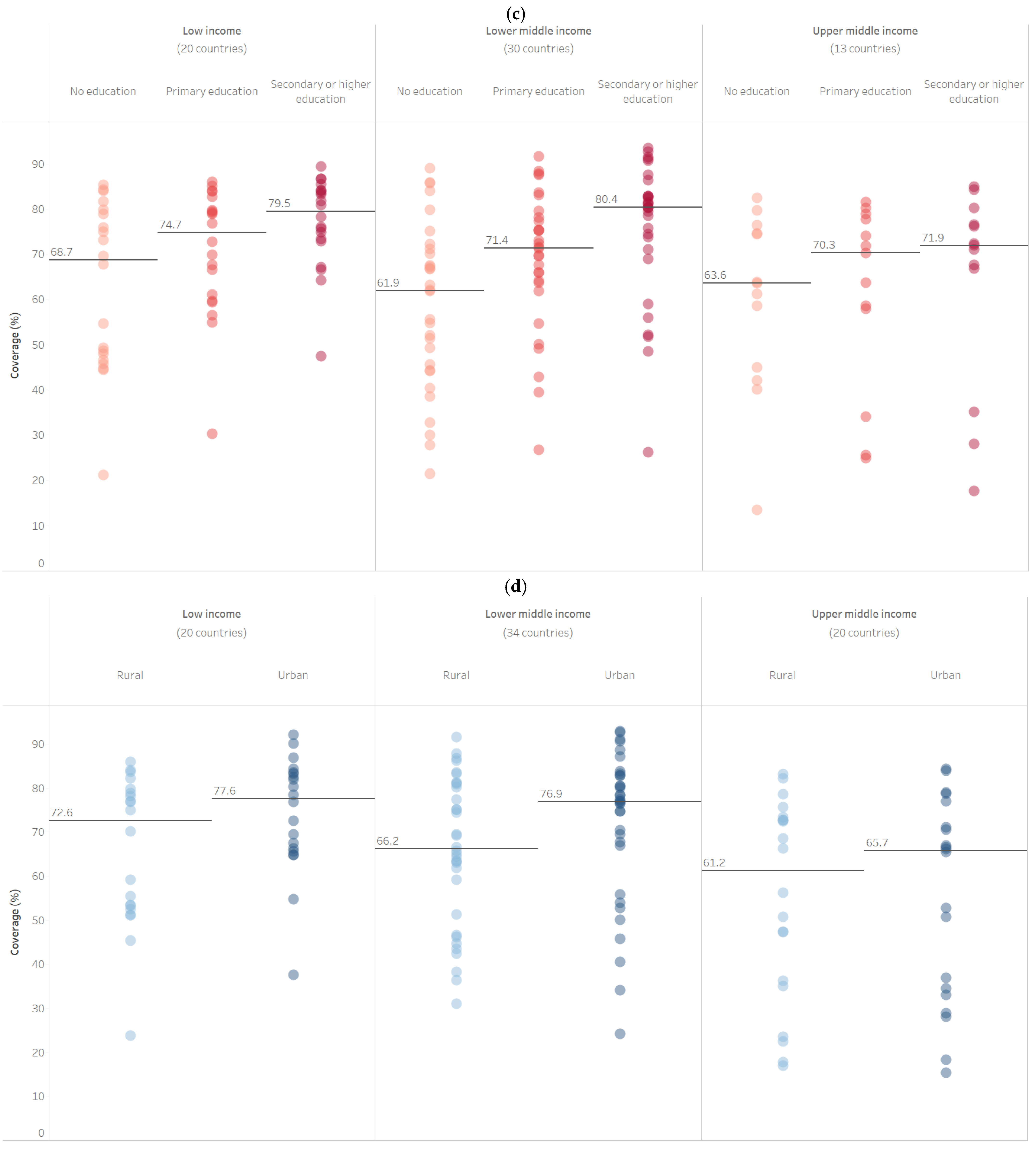
- Median coverage by subgroup of each inequality dimension, by country income group;
- Absolute inequality in coverage between the most and least advantaged subgroups of each inequality dimension, calculated using difference (e.g., highest wealth quintile coverage minus lowest wealth quintile coverage) and the slope index of inequality (SII), overall and by country income group;
- Relative inequality in coverage between the most and least advantaged subgroups of each inequality dimensions, calculated using ratio (e.g., highest wealth quintile coverage divided by lowest wealth quintile coverage) and the relative index of inequality (RII), overall and by country income group.
3. Results
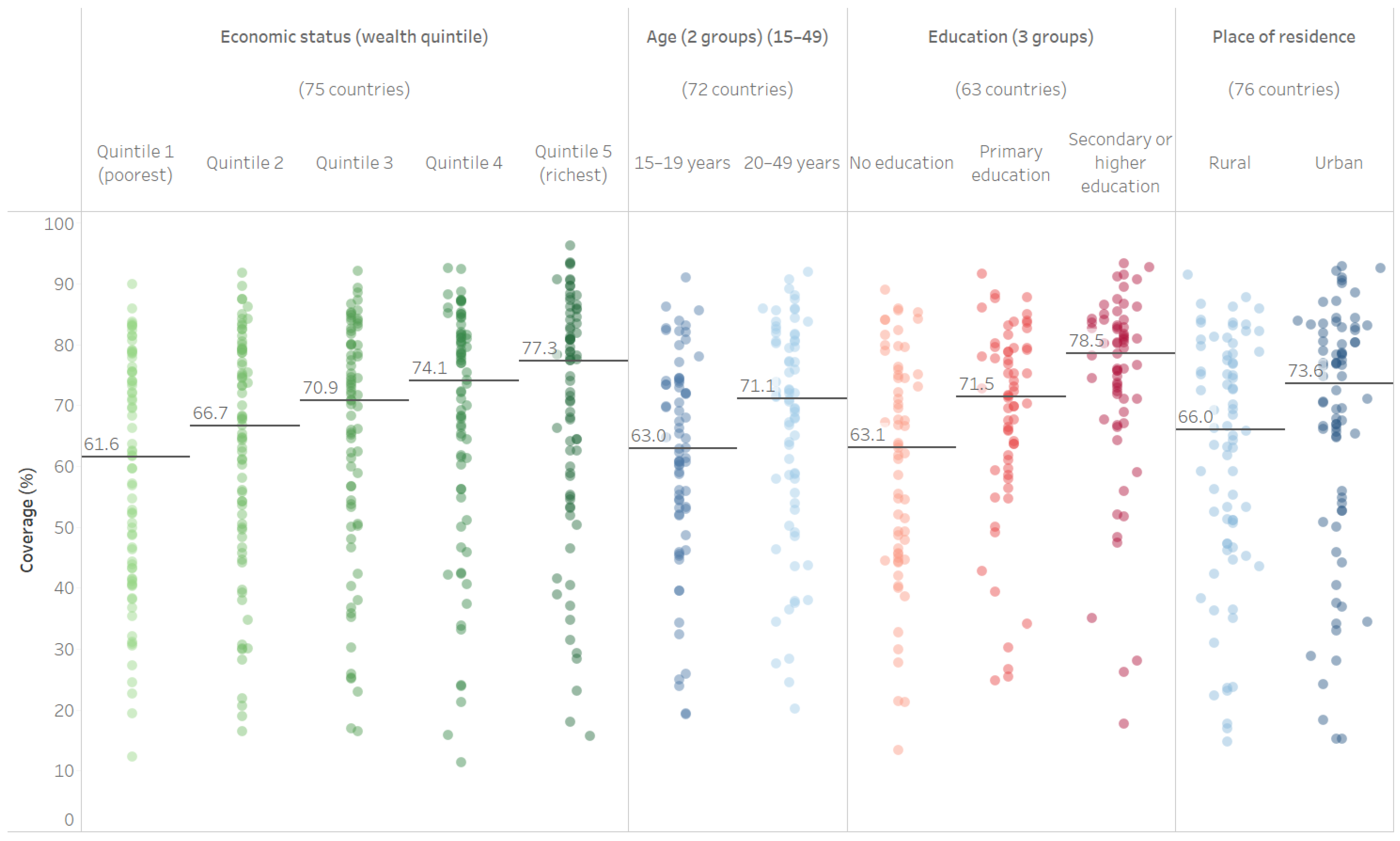
3.1. PAB Coverage Medians
3.2. Absolute and Relative Inequality in PAB Coverage
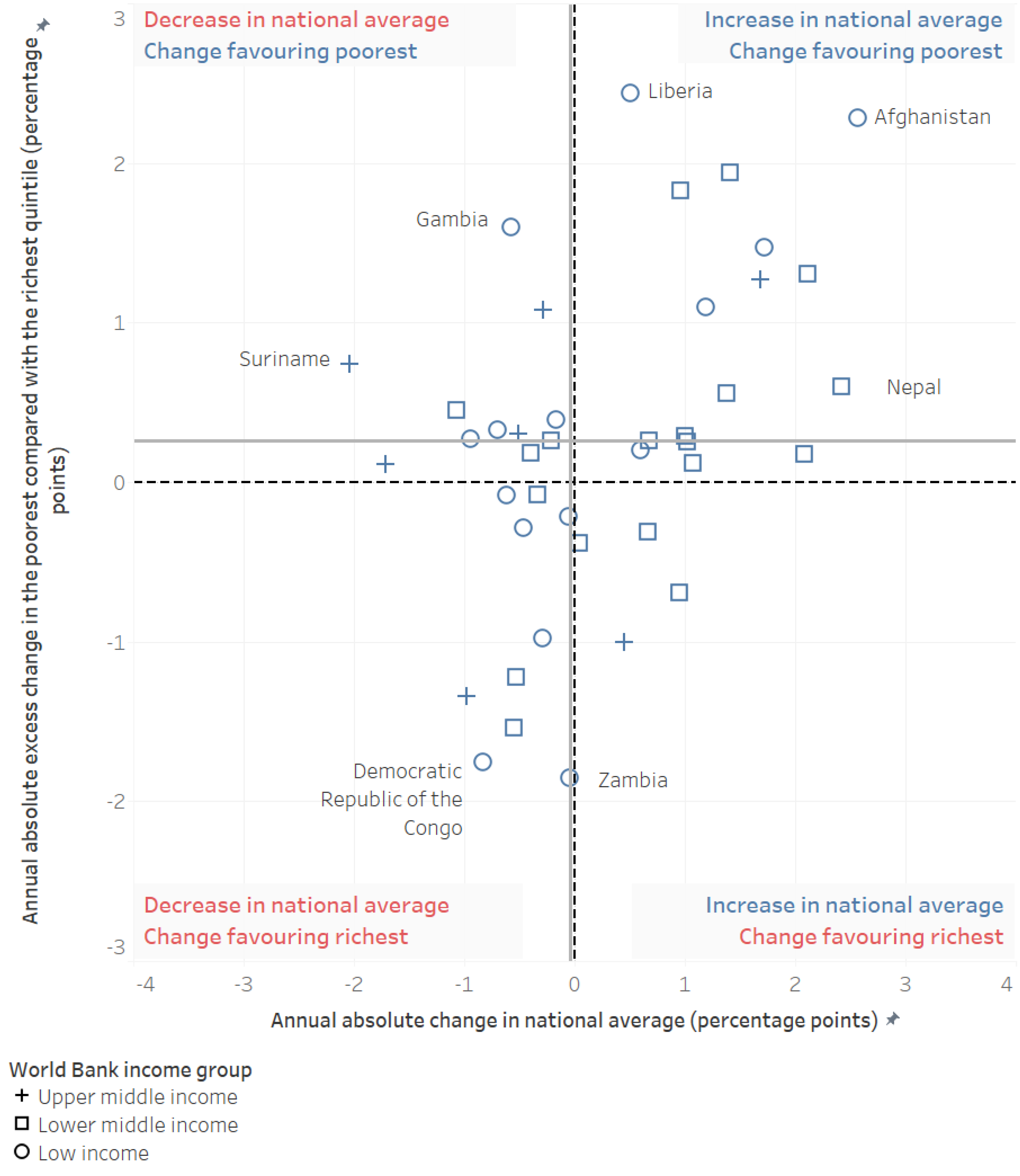
3.3. Change in Inequality in PAB Coverage over Time
3.4. PAB Coverage in Countries by MNTE Achievement Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roper, M.H.; Vandelaer, J.H.; Gasse, F.L. Maternal and neonatal tetanus. Lancet 2007, 370, 1947–1959. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tetanus vaccines: WHO position paper—February 2017. Wkly. Epidemiol. Rec. 2017, 92, 53–76. [Google Scholar]
- World Health Organization. Protecting All against Tetanus: Guide to Sustaining Maternal and Neonatal Tetanus Elimination (MNTE) and Broadening Tetanus Protection for All Populations; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Maternal and Neonatal Tetanus Elimination. Available online: https://www.who.int/initiatives/maternal-and-neonatal-tetanus-elimination-(mnte) (accessed on 22 September 2022).
- Kanu, F.A.; Yusuf, N.; Kassogue, M.; Ahmed, B.; Tohme, R.A. Progress toward Achieving and Sustaining Maternal and Neonatal Tetanus Elimination—Worldwide, 2000–2020. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Bergen, N.; Cata-Preta, B.O.; Schlotheuber, A.; Santos, T.M.; Danovaro-Holliday, M.C.; Mengistu, T.; Sodha, S.V.; Hogan, D.R.; Barros, A.J.D.; Hosseinpoor, A.R. Economic-Related Inequalities in Zero-Dose Children: A Study of Non-Receipt of Diphtheria-Tetanus-Pertussis Immunization Using Household Health Survey Data from 89 Low- and Middle-Income Countries. Vaccines 2022, 10, 633. [Google Scholar] [CrossRef]
- Hosseinpoor, A.R.; Bergen, N.; Schlotheuber, A.; Gacic-Dobo, M.; Hansen, P.M.; Senouci, K.; Boerma, T.; Barros, A.J. State of inequality in diphtheria-tetanus-pertussis immunisation coverage in low-income and middle-income countries: A multicountry study of household health surveys. Lancet Glob. Health 2016, 4, e617–e626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acharya, K.; Dharel, D.; Subedi, R.K.; Bhattarai, A.; Paudel, Y.R. Inequalities in full vaccination coverage based on maternal education and wealth quintiles among children aged 12–23 months: Further analysis of national cross-sectional surveys of six South Asian countries. BMJ Open 2022, 12, e046971. [Google Scholar] [CrossRef]
- Mutua, M.K.; Mohamed, S.F.; Porth, J.M.; Faye, C.M. Inequities in On-Time Childhood Vaccination: Evidence from Sub-Saharan Africa. Am. J. Prev. Med. 2021, 60, S11–S23. [Google Scholar] [CrossRef]
- World Health Organization. Explorations of Inequality: Childhood Immunization; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. State of Inequality: Childhood Immunization; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Levine, O.; Lemango, E.; Befson, J.; Gurley, N.; Rowley, E.; McIlvaine, B. ERG Discussion Paper 08: Tackling Inequities in Immunization Outcomes in Remote Rural Contexts; Equity Reference Group for Immunisation: New York, NY, USA, 2018. [Google Scholar]
- Adamu, A.A.; Uthman, O.A.; Sambala, E.Z.; Ndwandwe, D.; Wiyeh, A.B.; Olukade, T.; Bishwajit, G.; Yaya, S.; Okwo-Bele, J.M.; Wiysonge, C.S. Rural-urban disparities in missed opportunities for vaccination in sub-Saharan Africa: A multi-country decomposition analyses. Hum. Vaccines Immunother. 2019, 15, 1191–1198. [Google Scholar] [CrossRef]
- Sherley, J.; Newton, S. The association between area of residence and sufficient antenatal tetanus vaccination in women ages 15–49 in Afghanistan: An analysis of the 2015 DHS dataset. Glob. Health Res. Policy 2020, 5, 51. [Google Scholar] [CrossRef]
- Amin, M.B.; Roy, N.; Meem, A.E.; Hossain, E.; Aktarujjaman, M. Trends and determinants of taking tetanus toxoid vaccine among women during last pregnancy in Bangladesh: Country representative survey from 2006 to 2019. PLoS ONE 2022, 17, e0276417. [Google Scholar] [CrossRef]
- Rahman, M.; Obaida-Nasrin, S. Factors affecting acceptance of complete immunization coverage of children under five years in rural Bangladesh. Salud Publica Mex. 2010, 52, 134–140. [Google Scholar] [CrossRef]
- Thind, A. Determinants of tetanus toxoid immunization in pregnancy in rural Bihar. Trop. Dr. 2005, 35, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Liyew, A.M.; Ayalew, H.G. Individual and community-level determinants of poor tetanus toxoid immunization among pregnant women in Ethiopia using data from 2016 Ethiopian demographic and health survey; multilevel analysis. Arch. Public Health 2021, 79, 92. [Google Scholar] [CrossRef] [PubMed]
- Barrow, A.; Barrow, S.; Jobe, A. Differentials in prevalence and correlates on uptake of tetanus toxoid and intermittent preventive treatment with sulfadoxine-pyrimethamine during pregnancy: A community-based cross-sectional study in The Gambia. SAGE Open Med. 2022, 10, 20503121211065908. [Google Scholar] [CrossRef] [PubMed]
- Haile, Z.T.; Chertok, I.R.; Teweldeberhan, A.K. Determinants of utilization of sufficient tetanus toxoid immunization during pregnancy: Evidence from the Kenya Demographic and Health Survey, 2008-2009. J. Community Health 2013, 38, 492–499. [Google Scholar] [CrossRef]
- Kidane, T. Factors influencing TT immunization coverage and protection at birth coverage in Tselemti District, Ethiopia. Ethiop. J. Health Dev. 2004, 18, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Tun, Z.M.; Ring, Z.; Tam, C.C. Factors associated with maternal tetanus vaccination in Myanmar: An analysis of demographic and health survey data. Vaccine 2022, 40, 1135–1142. [Google Scholar] [CrossRef]
- Yaya, S.; Kota, K.; Buh, A.; Bishwajit, G. Prevalence and predictors of taking tetanus toxoid vaccine in pregnancy: A cross-sectional study of 8722 women in Sierra Leone. BMC Public Health 2020, 20, 855. [Google Scholar] [CrossRef]
- Mohamed, S.O.O.; Ahmed, E.M. Prevalence and determinants of antenatal tetanus vaccination in Sudan: A cross-sectional analysis of the Multiple Indicator Cluster Survey. Trop. Med. Health 2022, 50, 7. [Google Scholar] [CrossRef]
- Belay, A.T.; Fenta, S.M.; Agegn, S.B.; Muluneh, M.W. Prevalence and risk factors associated with rural women’s protected against tetanus in East Africa: Evidence from demographic and health surveys of ten East African countries. PLoS ONE 2022, 17, e0265906. [Google Scholar] [CrossRef]
- Yeshaw, Y.; Jemere, T.; Dagne, H.; Andualem, Z.; Akalu, Y.; Dewau, R.; Teshale, A.B.; Tesema, G.A.; Dagnew, B. Factors associated with births protected against neonatal tetanus in Africa: Evidences from Demographic and health surveys of five African countries. PLoS ONE 2021, 16, e0253126. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization Agenda 2030: A Global Strategy to Leave No One Behind; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- The DHS Program. The Demographic and Health Surveys Program. Available online: https://dhsprogram.com/ (accessed on 18 January 2023).
- UNICEF. Multiple Indicator Cluster Surveys. Available online: https://mics.unicef.org/ (accessed on 18 January 2023).
- The DHS Program. Methodology. Available online: https://dhsprogram.com/Methodology/ (accessed on 18 March 2022).
- UNICEF. MICS Publications—Reports and Methodological Papers. Available online: https://mics.unicef.org/publications/reports-and-methodological-papers (accessed on 18 January 2023).
- World Health Organization. Neonates Protected at Birth against Neonatal Tetanus (%). Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3207 (accessed on 18 January 2023).
- DHS Program. Tetanus Toxoid Injections. Available online: https://dhsprogram.com/data/Guide-to-DHS-Statistics/Tetanus_Toxoid_Injections.htm (accessed on 18 January 2023).
- The World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 18 January 2023).
- Conover, W.J. Practical Nonparametric Statistics, 3rd ed.; Wiley: New York, NY, USA, 1999. [Google Scholar]
- Mood, A.M.; Graybill, F.A. Introduction to the Theory of Statistics, 2nd ed.; McGraw-Hill: New York, NY, USA, 1963. [Google Scholar]
- World Health Organization; International Center for Equity in Health Pelotas. State of Inequality: Reproductive, Maternal, Newborn and Child Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Feletto, M.; Sharkey, A.; Rowley, E.; Gurley, N.; Sinha, A.; Champions, E.; Gupta, A.; Tolhurst, R. A Gender Lens to Advance Equity in Immunization; Equity Reference Group for Immunisation: New York, NY, USA, 2018. [Google Scholar]
- World Health Organization. Why Gender Matters: Immunization Agenda 2030; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Gavi the Vaccine Alliance. Phase V (2021–2025). Available online: https://www.gavi.org/our-alliance/strategy/phase-5-2021-2025 (accessed on 18 March 2022).
- Johns, N.E.; Santos, T.M.; Arroyave, L.; Cata-Preta, B.O.; Heidari, S.; Kirkby, K.; Munro, J.; Schlotheuber, A.; Wendt, A.; O’Brien, K.; et al. Gender-Related Inequality in Childhood Immunization Coverage: A Cross-Sectional Analysis of DTP3 Coverage and Zero-Dose DTP Prevalence in 52 Countries Using the SWPER Global Index. Vaccines 2022, 10, 988. [Google Scholar] [CrossRef] [PubMed]
- Vidal Fuertes, C.; Johns, N.E.; Goodman, T.S.; Heidari, S.; Munro, J.; Hosseinpoor, A.R. The Association between Childhood Immunization and Gender Inequality: A Multi-Country Ecological Analysis of Zero-Dose DTP Prevalence and DTP3 Immunization Coverage. Vaccines 2022, 10, 1032. [Google Scholar] [CrossRef]
- Yusuf, N.; Steinglass, R.; Gasse, F.; Raza, A.; Ahmed, B.; Blanc, D.C.; Yakubu, A.; Gregory, C.; Tohme, R.A. Sustaining Maternal and Neonatal Tetanus Elimination (MNTE) in countries that have been validated for elimination—Progress and challenges. BMC Public Health 2022, 22, 691. [Google Scholar] [CrossRef] [PubMed]
- Dhir, S.K.; Dewan, P.; Gupta, P. Maternal and Neonatal Tetanus Elimination: Where are We Now? Res. Rep. Trop. Med. 2021, 12, 247–261. [Google Scholar] [CrossRef] [PubMed]
- Okwo-Bele, J.-M.; Conner, R.; McIlvaine, B.; Rowley, E.; Bernson, J. ERG Discussion Paper 06: Tackling Inequities in Immunization Outcomes in Conflict Contexts; Equity Reference Group for Immunisation: New York, NY, USA, 2018. [Google Scholar]
- Rahman, M. Tetanus toxoid vaccination coverage and differential between urban and rural areas of Bangladesh. East Afr. J. Public Health 2009, 6, 26–31. [Google Scholar] [CrossRef]
- Nandy, R.; Reese, H.; Bernson, J.; Digre, P.; Rowley, E.; McIlvaine, B. ERG Discussion Paper 07: Tackling Inequities in Immunization Outcomes in Urban Contexts; Equity Reference Group for Immunisation: New York, NY, USA, 2018. [Google Scholar]
- Pathirana, J.; Nkambule, J.; Black, S. Determinants of maternal immunization in developing countries. Vaccine 2015, 33, 2971–2977. [Google Scholar] [CrossRef]
- Khan, A.A.; Zahidie, A.; Rabbani, F. Interventions to reduce neonatal mortality from neonatal tetanus in low and middle income countries—A systematic review. BMC Public Health 2013, 13, 322. [Google Scholar] [CrossRef] [Green Version]
- Vouking, M.Z.; Tadenfok, C.N.; Ekani, J.M.E. Strategies to increase immunization coverage of tetanus vaccine among women in Sub Saharan Africa: A systematic review. Pan Afr. Med. J. 2017, 27, 25. [Google Scholar] [CrossRef]
- World Health Organization. Reaching Every District (RED), 2017 Revision; WHO Regional Office for Africa: Brazzaville, Congo, 2017. [Google Scholar]
- De Francisco, A.; Chakraborty, J. Maternal recall of tetanus toxoid vaccination. Ann. Trop. Paediatr. 1996, 16, 49–54. [Google Scholar] [CrossRef]
- Dansereau, E.; Brown, D.; Stashko, L.; Danovaro-Holliday, M.C. A systematic review of the agreement of recall, home-based records, facility records, BCG scar, and serology for ascertaining vaccination status in low and middle-income countries. Gates Open Res. 2019, 3, 923. [Google Scholar] [CrossRef] [PubMed]
- Deming, M.S.; Roungou, J.B.; Kristiansen, M.; Heron, I.; Yango, A.; Guenengafo, A.; Ndamobissi, R. Tetanus toxoid coverage as an indicator of serological protection against neonatal tetanus. Bull. World Health Organ. 2002, 80, 696–703. [Google Scholar] [PubMed]
- Brown, D.W.; Bosch-Capblanch, X.; Shimp, L. Where Do We Go from Here? Defining an Agenda for Home-Based Records Research and Action Considering the 2018 WHO Guidelines. Glob. Health Sci. Pract. 2019, 7, 6–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Household Wealth Highest vs. Lowest Quintile | Maternal Age Age 20–49 vs. Age 15–19 | Maternal Education Secondary or More vs. No Schooling | Place of Residence Urban vs. Rural | |||||
|---|---|---|---|---|---|---|---|---|
| Difference (95% CI) | Ratio (95% CI) | Difference (95% CI) | Ratio (95% CI) | Difference (95% CI) | Ratio (95% CI) | Difference (95% CI) | Ratio (95% CI) | |
| All Countries | 7.9 (5.0–11.8) | 1.12 (1.08–1.19) | 4.5 (2.9–6.1) | 1.07 (1.04–1.10) | 11.6 (8.4–15.7) | 1.18 (1.12–1.25) | 3.7 (1.9–6.4) | 1.05 (1.03–1.10) |
| Low-Income Countries | 15.2 (5.7–24.7) | 1.21 (1.09–1.66) | 4.8 (1.9–8.4) | 1.09 (1.03–1.18) | 15.6 (4.3–25.2) | 1.23 (1.05–1.53) | 7.3 (3.8–11.3) | 1.10 (1.05–1.21) |
| Lower-Middle Income Countries | 10.9 (7.2–16.7) | 1.16 (1.10–1.32) | 6.0 (3.7–8.3) | 1.09 (1.06–1.14) | 13.1 (10.0–25.9) | 1.20 (1.17–1.47) | 4.7 (1.3–8.1) | 1.07 (1.02–1.13) |
| Upper-Middle Income Countries | −1.5 (−6.5–5.5) | 0.98 (0.88–1.08) | 1.1 (−3.0–5.0) | 1.03 (0.96–1.14) | 7.3 (−3.3–9.5) | 1.11 (0.96–1.15) | 0.2 (−1.7–2.9) | 1.00 (0.94–1.05) |
| Household Wealth Highest vs. Lowest Quintile | Maternal Age Age 20–49 vs. Age 15–19 | Maternal Education Secondary or More vs. No Schooling | Place of Residence Urban vs. Rural | |||||
|---|---|---|---|---|---|---|---|---|
| Difference (95% CI) | Ratio (95% CI) | Difference (95% CI) | Ratio (95% CI) | Difference (95% CI) | Ratio (95% CI) | Difference (95% CI) | Ratio (95% CI) | |
| All Countries | 7.9 (5.0–11.8) | 1.12 (1.08–1.19) | 4.5 (2.9–6.1) | 1.07 (1.04–1.10) | 11.6 (8.4–15.7) | 1.18 (1.12–1.25) | 3.7 (1.9–6.4) | 1.05 (1.03–1.10) |
| Countries which have NOT achieved MNTE | 30.6 (23.1–46.1) | 1.89 (1.67–2.14) | 2.0 (−1.7–8.0) | 1.04 (0.97–1.17) | 28.4 (23.8–37.4) | 1.67 (1.52–2.17) | 18.0 (11.3–26.0) | 1.40 (1.21–1.56) |
| Countries which have achieved MNTE | 6.4 (3.5–9.8) | 1.10 (1.05–1.15) | 4.7 (3.0–6.2) | 1.07 (1.05–1.10) | 9.1 (5.6–12.0) | 1.15 (1.08–1.19) | 3.0 (1.4–5.0) | 1.04 (1.02–1.07) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© World Health Organization 2023. Licensee MDPI, Basel, Switzerland. This article is distributed under the terms of the Creative Commons Attribution IGO License. (https://creativecommons.org/licenses/by/3.0/igo/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organization or products. The use of the WHO logo is not permitted. This notice should be preserved along with the article’s original URL.
Share and Cite
Johns, N.E.; Cata-Preta, B.O.; Kirkby, K.; Arroyave, L.; Bergen, N.; Danovaro-Holliday, M.C.; Santos, T.M.; Yusuf, N.; Barros, A.J.D.; Hosseinpoor, A.R. Inequalities in Immunization against Maternal and Neonatal Tetanus: A Cross-Sectional Analysis of Protection at Birth Coverage Using Household Health Survey Data from 76 Countries. Vaccines 2023, 11, 752. https://doi.org/10.3390/vaccines11040752
Johns NE, Cata-Preta BO, Kirkby K, Arroyave L, Bergen N, Danovaro-Holliday MC, Santos TM, Yusuf N, Barros AJD, Hosseinpoor AR. Inequalities in Immunization against Maternal and Neonatal Tetanus: A Cross-Sectional Analysis of Protection at Birth Coverage Using Household Health Survey Data from 76 Countries. Vaccines. 2023; 11(4):752. https://doi.org/10.3390/vaccines11040752
Chicago/Turabian StyleJohns, Nicole E., Bianca O. Cata-Preta, Katherine Kirkby, Luisa Arroyave, Nicole Bergen, M. Carolina Danovaro-Holliday, Thiago M. Santos, Nasir Yusuf, Aluísio J. D. Barros, and Ahmad Reza Hosseinpoor. 2023. "Inequalities in Immunization against Maternal and Neonatal Tetanus: A Cross-Sectional Analysis of Protection at Birth Coverage Using Household Health Survey Data from 76 Countries" Vaccines 11, no. 4: 752. https://doi.org/10.3390/vaccines11040752