

Immune Response Related to Lymphadenopathy Post COVID-19 Vaccination

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
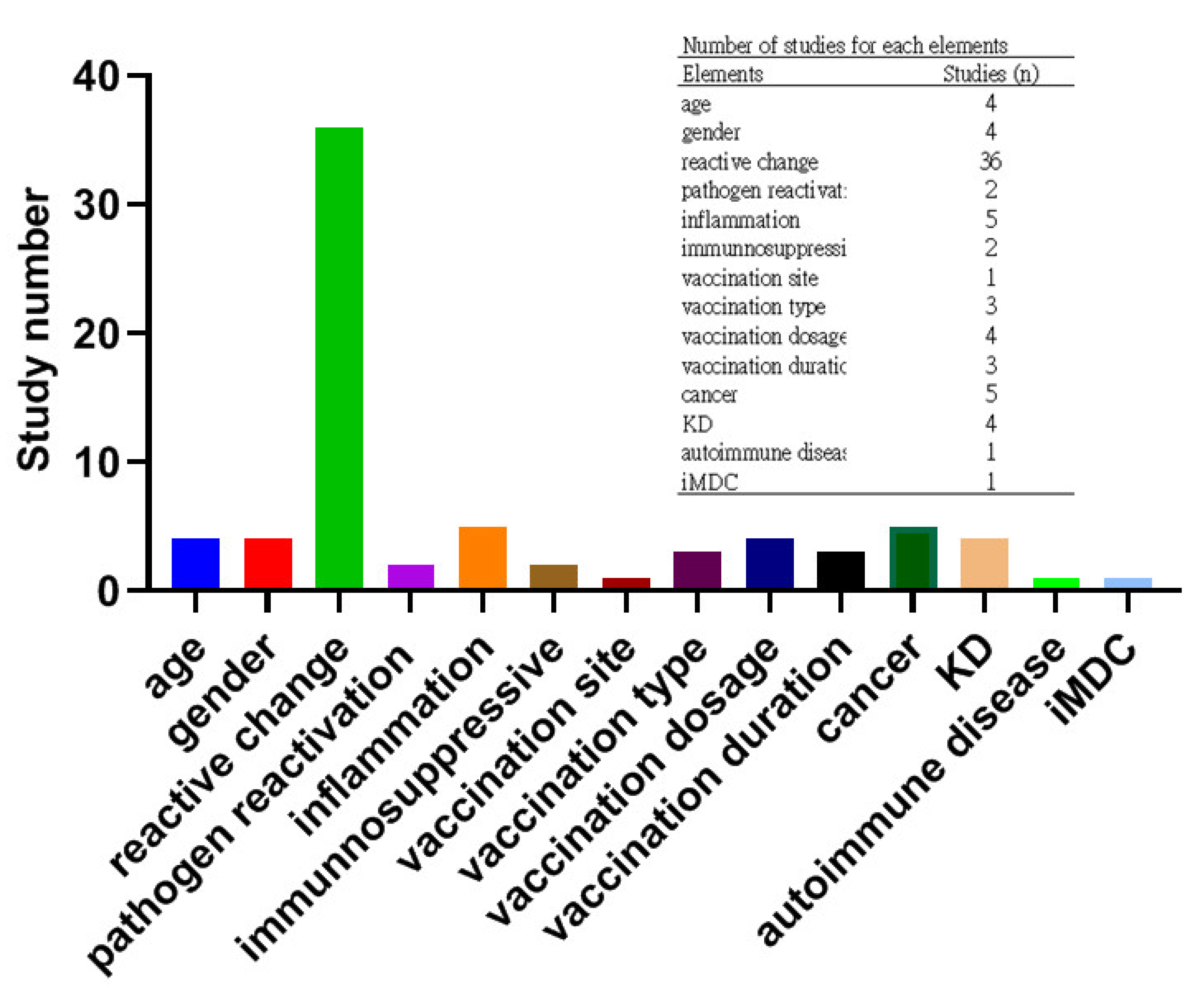
3.1. Studies including and Characterization
3.2. Negative Correlation between Days Post-Vaccination and C19-VAL Incidence
3.3. Reactive Change and B Cell Germinal Center Related to the C19-VAL Development

{kind=link}
{kind=link}
| Design | Study | Country | Participants | Age (Years) | Medical History | Male N (%) | Vaccine Type | Vaccine Dose | Last Vaccine to C19-VAL (Days)/Site | Main Finding | Elements |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Single center reprospective study | Yoshikawa T. (2022) [38] | Japan | 433 | 65 ± 11 | No past and current LAD related disease and COVID-19 | 300 (69.28) | NR | 2 (most) | NR/all for ipsilateral axillary | Incidence of C19-VAL is significantly higher in young age and female | Young age and female |
| Shin M. (2021) [45] | Korea | 31 | 45 ± 5 | No history of malignancy, vaccination before 18F-FDG PET/CT | 11 (35) | AstraZeneca | NR | 4–29/bilateral axillary, supraclavicular | Percentage of C19-VAL is significantly higher in female, FDG-avid deltoid muscle can be a helpful sign to presume the reactive LN | Female and reactive change | |
| Park JY. (2022) [20] | Korea | 413 | 48 ± 12 | No history of malignancy, vaccination within 12 weeks, vaccination before ultrasonography | 10 (2.42) | Moderna (19); AstraZeneca (64); Pfizer-BioNTech (330) | 2 (257) | 1–82/axillary | 48.9% cases with C19-VAL. Incidence of C19-VAL is significantly higher in young age, mRNA vaccine and post 1st dose as well as decreased as days from vaccination | Young age, mRNA vaccine, 1st dose, and days post-vaccination | |
| Nishino M. (2021) [10] | USA | 232 | 40–96 | All with lung cancer, CT scans prior and post vaccination | 88 (37.9) | Moderna (28); Pfizer-BioNTech (204) | 2 | 7–68/axillary, subpectoral | 9% cases with C19-VAL. Incidence of C19-VAL is significantly higher in female and in Moderna | Female and Moderna | |
| Cocco G. (2021) [18] | Italy | 24 | 25–74 | Without fever and no history of hematological malignancy, autoimmune disease and vaccination before ultrasonography | 10 (41.6) | Moderna (3); AstraZeneca (8); Pfizer-BioNTech (13) | Least 1 | NR/axillary, supraclavicular | All cases with C19-VAL Percentage of C19-VAL is significantly higher post 1 dose vaccination | 1st dose | |
| El-Sayed MS. (2021) [13] | UK | 204 | 68 ± 11 | Without LAD pathologies, vaccination within 12 weeks and before 18F-FDG PET/CT | 98 (48) | AstraZeneca (43); Pfizer-BioNTech (62); unknown (99) | 2 (87) | Up to 70/axillary | 36% cases with C19-VAL. Incidence of C19-VAL is significantly higher in young age, vector vaccine and female | Young aged, vector vaccine and female | |
| Ah-Thiane L. (2022) [42] | France | 226 | 67–76 | Most prostate cancer, vaccination before ultrasonography, MRI, or 18F-FDG PET/CT | 212 (93.8) | Moderna (11); AstraZeneca (60); Pfizer-BioNTech (152); Janssen (3) | 2 (124) | 14–51/axillary and supraclavicular | 42.5% cases with C19-VAL. Incidence of C19-VAL was significant higher post the 1st vaccination | 1st dose | |
| Maimone S. (2022) [44] | US | 2304 | 30–92 | Vaccination before screening mammography | NR | Moderna (1109); Pfizer-BioNTech (1135); other (41); unknown (18) | 2 (1883) | 0–28 and >28/ipsilateral axillary | 1% cases with C19-VAL. Incidence of C19-VAL was significantly decreased as days from vaccination | Days post-vaccination | |
| Eifer M. (2022) [43] | Israel | 426 Immunosuppressive treatment (82), hemato-logical malignancy (75) | 67 ± 12 | Vaccination before PET/CT and without malignancy involving axillary LN | 219 (51) | Pfizer-BioNTech | 2 (103) | 5–18/axillary | Incidence of C19-VAL is significantly higher in young age, 2nd vaccination and increased in days post last vaccination, but lower in immunosuppressive treatment and hematologic malignancy | Young age, 2nd vaccination, days post-vaccination, immunosuppressive, and hematologic malignancy | |
| Cohen D. (2021) [88] | Germany | 137 Recent anti-CD20 (34), no recent anti-CD20 (68) | >16 | Hematologic malignancy without MHL | 75 (54.7) | NR | Either of 1 or 2 | 6–27/ipsilateral axillary or supraclavicular | Incidence of C19-VAL in recent anti-CD20 vs. no recent anti-CD20 (8.8 vs. 41.1%, significant) | B cell germinal center response | |
| Case series | Fernández-Prada M. (2021) [19] | Spain | 20 | 20–60 | Autoimmune disease (4), thyroid cancer (2) | 0 | Pfizer-BioNTech (19) Moderna (1) | 2 (14) | 0–4/supraclavicular | 12 of 20 patients reported high injection site, biopsy of LN from two type vaccines revealed reactive change | High injected site and reactive change |
| García-Molina F. (2021) [36] | Spain | 6 | 27–62 | NR | NR | Pfizer-BioNTech | 1 | 5/axillary or supraclavicular | Cytological for FNA and biopsy: nonspecific chronic adenitis, resolution of ALAD and SLAD after anti-inflammation drug | Inflammation | |
| Özütemiz C. (2021) [48] | USA | 2 | 62 | Current metastatic breast cancer (1), two cancer history | 1 (50%) | Moderna (1) Pfizer-BioNTech (1) | 3 | 1–2/ipsilateral axillary | Due to imaging and vaccine history, reactive LN | Reactive change | |
| Heaven CL. (2022) [47] | New Zealand | 5 | 41–76 | High suspicion of cancer | 2 (40%) | Pfizer-BioNTech | 2 | 7–34/bilateral cervical | Biopsy: reactive follicular hyperplasia with no evidence of atypia or malignancy | Reactive change | |
| Hagen C. (2021) [49] | Switzerland | 5 | 41–66 | Lung cancer (2), neuroendocrine tumor (1) | 2 (40%) | Pfizer-BioNTech (2) Moderna (3) | 1 (3) | 3–33/bilateral axillary, supraclavicular | FNA: reactive follicular hyperplasia | Reactive change | |
| Brown AH. (2021) [46] | UK | 2 | 48, 67 | Breast cancer for right (1) and for left (1) | 0 | NR | NR | 14, 21/ipsilateral axillary, subpectoral | FNA: reactive change without malignancy | Reactive change | |
| Case report | Goldman S. (2021) [86] | Belgium | 1 | 66 | Hypercholesterolemia, type 2 diabetes, recent cervical lymphadenopathies | 1 | Pfizer-BioNTech | 2 | 150/ipsilateral supraclavicular, cervical, left axillary and abdomen | FNA of CLN: atypical T cell infiltrate with high endothelial venules proliferation; NGS: positive AITL, the number and distribution of LAD increased after 3rd vaccination | AITL |
| Wolfson S. (2022) [50] | USA | 2 | 50, 60 | No (1), simultaneously left ductal carcinoma | 0 | Moderna | 1 | 10, 63/ipsilateral axillary | FNA: begin reactive LN for no medical history, biopsy: metastatic adenocarcinoma for left ductal carcinoma patients | Reactive change | |
| Mizutani M. (2022) [85] | Japan | 2 | 67, 80 | NR | 1 | Pfizer-BioNTech | 2 | 14, 1/left axillary | Persistent ALAD from 1st dose vaccination and gradually enlarged post 2nd dose, finally diagnosed as DLBC by IHC of biopsy | DLBCL | |
| Sekizawa A. (2022) [84] | Japan | 1 | 80 | Hypertension, angina pectoris, mitral valve regurgitation, ovarian tumor | 0 | Pfizer-BioNTech | 2 | 21/ipsilateral temporal cervical, submandibular, and jugular | Persistent ipsilateral temporal after 1st dose vaccination, and sudden enlarged post 2nd dose, finally diagnosed as MZL | MZL | |
| Sasa S. (2022) [87] | Japan | 1 | 80 | Right breast | 0 | Pfizer-BioNTech | 2 | 90/ipsilateral axillary | Multilobulated cystic mass and branches on ultrasonography, finally diagnosed as lymphangioma and resected | Lymphangioma | |
| Saito K. (2022) [41] | Japan | 1 | 66 | Current malaise and oral bleeding and purpura | 0 | Pfizer-BioNTech | 1 | 2/systematic | Low platelet count, markedly increased megakaryocytes in bone marrow, and present of serum anti-glycoprotein IIb/IIIa, finally diagnosed ITP | ITP | |
| Hoffmann C. (2022) [90] | Germany | 1 | 20 | Fever, centigrade, loss of appetite, malaise, weakness, and exertional dyspnea post vaccination | 1 | Pfizer-BioNTech | 2 | 18/supraclavicular, axillary | iMDC post vaccination | iMDC | |
| Girardin FR. (2022) [89] | Switzerland | 1 | 40 | Recent EBV infection | 0 | Moderna | 2 | 1/bilateral axillary and supraclavicular | EBV positive parafollicular immunoblastic cells in LN, induce repeated and extend C19-VAL through enhancing the vaccine immunity | EBV | |
| Cha HG. (2022) [66] | Korea | 1 | 66 | Injection site tenderness and fatigue post 1st dose, acute idiopathic thrombocytopenic purpura | 0 | AstraZeneca | 2 | 3/ipsilateral supraclavicular | Persistent LAD up to 8 weeks, further revealed multiple FDG avid-LNs not limited in supraclavicular, LN biopsy of SLN: chronic granulomatous inflammation, PCR positive for TB | TB | |
| Ganga K. (2021) [24] | USA | 1 | 58 | Hypertension | 1 | Moderna | NR | 2/left neck | FNA for LN of left neck: negative for malignancy and positive for inflammatory cells, improvement and resolution of neck swelling and dysphagia by antibiotic treatment | Inflammation | |
| Cheong KM. (2022) [80] | Taiwan | 1 | 32 | NR | 0 | AstraZeneca | 1 | 2/lower neck | Neck lymphadenitis diagnosed on ultrasonography | Inflammation | |
| Andresciani F. (2022) [79] | Italy | 1 | 62 | Prostate cancer | 1 | Pfizer-BioNTech | 2 | 21/ipsilateral axillary, paratracheal, paraaortic, subcarinal, and bilateral hilar | Choline intensity decreased in LN, finally diagnosed as inflammatory LN, not oncological disease | Inflammation | |
| Tsumura Y. (2022) [83] | Japan | 1 | 31 | Metastatic Ewing sarcoma | 0 | Pfizer-BioNTech | NR | 21/ipsilateral axillary | An inflammatory lesion rather than metastatic lymph node swelling | Inflammation | |
| Tan HM. (2021) [39] | Singapore | 2 | 18, 34 | Current fever | 1 | Pfizer-BioNTech | 1–2 | 17–35/left axillary, supraclavicular, subpectoral | Fever, transient leukopenia, LAD, negative for infection, necrotizing lymphadenitis in LN biopsy, finally diagnosed KD | KD | |
| Caocci G. (2022) [40] | Italy | 1 | 38 | Recent fever for ten day, chills, and fatigue, C19-VAL post 1st dose | 0 | Pfizer-BioNTech | 2 | 31/left axillary | Fever, negative for infection, leukopenia, LAD, and biopsy of LN: histiocytic necrotizing lymphadenitis (numerous CD68+ histiocytes and CD3+ T cells, few CD20+ B cells), finally diagnosed KD | KD | |
| Kashiwada T. (2022) [82] | Japan | 1 | 27 | Recent repeated fever, C19-VAL post 1st dose | 0 | Pfizer-BioNTech | 2 | 68/ipsilateral axillary | Fever, negative for infection, leukopenia, LAD, and necrotizing lymphadenitis in LN biopsy, finally diagnosed KD | KD | |
| Guan YY. (2022) [81] | China | 1 | 36 | Current fever and fatigue | Sinopharm | 1 | 28/left cervical, neck | Fever, LAD and necrotizing lymphadenitis (numerous CD68+ histiocytes and CD3+ T cells, few CD20+ B cells) in LN, finally diagnosed KD | KD | ||
| Xu GY. (2021) [51] | USA | 1 | 72 | Mantle cell lymphoma | 1 | Pfizer-BioNTech | NR | 2/ipsilateral axillary | With FDG-avid deltoid muscle, reactive LN, recurrent lymphoma | Reactive change | |
| Özütemiz C.(2021) [8] | USA | 2 | 38, 46 | Breast cancer (1) | 0 | Pfizer-BioNTech | 2 (1) | 8–15/ipsilateral axillary, supraclavicular | Biopsy: reactive follicular hyperplasia in lymph node without any evident of breast cancer and malignancy | Reactive change | |
| Nawwar AA. (2021) [52] | UK | 1 | 75 | Prostate cancer | 1 | AstraZeneca | 1 | 3/ipsilateral axillary | With 18F-Choline-avid left deltoid muscle, reactive active LN | Reactive change | |
| Mitchell OR. (2021) [53] | UK | 2 | 47, 55 | NR | 0 | NR | NR | 3/ipsilateral supraclavicular | Reactive LN by clinical and ultrasonographic examination | Reactive change | |
| Ulaner GA. (2021) [54] | Canada | 1 | 68 | Current right melanoma | 1 | Moderna | 1 | 21/ipsilateral axillary | Unlike metastasis of right melanoma, reactive to vaccination | Reactive change | |
| Wong FC. (2022) [55] | USA | 1 | 74 | Prostate cancer | 1 | Moderna | 2 | 6/ipsilateral axillary | Unlike metastasis of prostate cancer and findings for C19-VAL, considering to reactive to vaccination | Reactive change | |
| Garreffa E. (2021) [56] | UK | 1 | 38 | NR | 0 | Pfizer-BioNTech | 1 | 7/ipsilateral clavicle | Reactive LN by ultrasonographic examination | Reactive change | |
| Prieto PA. (2021) [57] | USA | 1 | 48 | Melanoma | 0 | Moderna | 1 | 5/ipsilateral axillary, neck | Biopsy: consistent with reactive LN and negative of melanoma | Reactive change | |
| Roca B. (2021) [58] | Spain | 1 | 29 | NR | 0 | Pfizer-BioNTech | 1 | 7/ipsilateral supraclavicular | C19-VAL disappeared over the next few weeks | Reactive change | |
| Tan JHN. (2021) [59] | Singapore | 1 | 34 | No malignancy history | 0 | Pfizer-BioNTech | 1 | 1/ipsilateral supraclavicular | FNA: reactive follicular hyperplasia | Reactive change | |
| Gable AD. (2021) [60] | USA | 1 | 24 | Current ED, never smoker, no medical or surgical history, no ED related disease | 1 | NR | 2 | 4/ipsilateral axillary | ED due to typical bronchial carcinoid and LAD significant reduced later | Reactive change | |
| Suleman A. (2021) [61] | Canada | 1 | 38 | Current left Hodgkin lymphoma | 0 | Pfizer-BioNTech | 1 | 7/ipsilateral axillary | Reduced later | Reactive change | |
| Tintle S. (2021) [62] | USA | 1 | 23 | Asthma, eczema, and hypothyroidism, simultaneously fever and acute kidney injury | 0 | Moderna | 2 | 7/left axillary and abdomen | Biopsy of ALN: reactive lymphadenitis | Reactive change | |
| Weeks JK. (2021) [63] | USA | 1 | 50 | Current sigmoid adenocarcinoma | 0 | Moderna | 2 | 30/bilateral axillary | Improvement of C19-VAL | Reactive change | |
| Mori M. (2022) [64] | Japan | 1 | 30 | NR | 0 | Pfizer-BioNTech | 1 | 9/axillary | Resolution later | Reactive change | |
| Tzankov A. (2021) [65] | Switzerland | 1 | 30 | Current right papillary thyroid cancer | 1 | Moderna | 1 | 21/left axillary | Biopsy: extrafollicular proliferation of B-blasts and resolution later | Reactive change | |
| Chan HP. (2022) [66] | Taiwan | 1 | 71 | Thyroid cancer, right renal cell carcinoma | 1 | Moderna | 1 | 6/ipsilateral axillary | Due to imaging and vaccine history, reactive to vaccination | Reactive change | |
| Adin ME. (2022) [67] | USA | 1 | 41 | Simultaneously right breast cancer | 0 | Moderna | 2 | 16/ipsilateral axillary, | Due to imaging and vaccine history, reactive to vaccination | Reactive change | |
| Kang ES. (2022) [68] | South Korea | 1 | 59 | Simultaneously SCC of the right mandibular gingiva | 1 | Moderna | 2 | 10/ipsilateral axillary, bilateral cervical | FNA: only small lymphoid cells, reactive to vaccination | Reactive change | |
| Yu Q. (2022) [69] | China | 1 | 34 | Allergic disease, tuberculosis, past malignant tumors, recent infection, trauma | 0 | Sinovac | 2 | 120/ipsilateral axillary | FNA: reactive hyperplasia and resolution later, reactive to vaccination | Reactive change | |
| Ashoor A. (2021) [70] | Italy | 3 | 61–72 | No (2), simultaneously breast cancer (1) | 0 | AstraZeneca | 1 (1), 2 (2) | 1–27/ipsilateral axillary | Imaging is normal and biopsy: benign reactive changes, reactive to vaccination | Reactive change | |
| Lee SM. (2022) [71] | South Korea | 1 | 21 | NR | 1 | Pfizer-BioNTech | 2 | 2/ipsilateral axillary | Radial neuropathy associated with ipsilateral ALAD, FNA: reactive hyperplasia | Reactive change | |
| Kado S. (2022) [72] | Japan | 1 | 31 | NR | 0 | Pfizer-BioNTech | 1 | 8/ipsilateral clavicle, scapular | FNA: follicular hyperplasia and resolution later, reactive to vaccination | Reactive change | |
| Aalberg JJ. (2021) [73] | USA | 1 | 73 | Metastatic renal cell carcinoma to lung and bone | Moderna | 2 | 2/ipsilateral axillary | With FDG avid-ipsilateral deltoid muscle and FNA: polymorphous lymphoid population with no evidence of metastasis | Reactive change | ||
| Cardoso F. (2021) [74] | Portugal | 1 | 48 | Usual contraceptive medication, Mercilon® | 0 | Pfizer-BioNTech | 2 | 1/right cervical | Due to persistent LAD after first dose, FNA: reactive follicular hyperplasia | Reactive change | |
| Lam DL. (2022) [75] | USA | 1 | 39 | Simultaneously right breast cancer | 0 | Pfizer-BioNTech | 2 | 1/ipsilateral axillary | C19-VAL resolution later, FNA for sentinel LN: negative metastasis and consistent with reactive to vaccination | Reactive change | |
| Musaddaq B. (2021) [76] | UK | 1 | 57 | Left breast cancer, simultaneously right breast cancer | 0 | Astra Zeneca | 1 | 3/ipsilateral axillary | IHC: reactive LN with follicular hyperplasia and without metastasis cancer | Reactive change | |
| Dirven I. (2022) [77] | Belgium | 1 | 60 | MEN 1 syndrome and simultaneously right lung nodule | 0 | Pfizer-BioNTech | 1 | 13/ipsilateral axillary | FNA: LN with a benign reactive pattern without metastatic disease | Reactive change | |
| Pudis M. (2021) [78] | Spain | 1 | 30 | Neuroendocrine tumor | 0 | Pfizer-BioNTech | 2 | 40/bilateral axillary, unilateral supraclavicular and cervical | No infection, Biopsy: benign reactive LN with CD10+ B cell population, immune system activation to vaccination | Reactive change |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
- ■
- Database:
- PubMed
- EMBASE
- Web of Science
- ■
- Last search date: 6 September. 2022
- ■
- Year cover of search: 1 December. 2020–31 October. 2022
- ■
- Search terms:
- ■
- PubMed (n = 465)
- ■
- EMBASE (n = 1356)
- ■
- Web of Science (n = 236)
References
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). OurWorldInData.org. 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 30 November 2022).
- Centers for Disease Control and Prevention. Benefits of Getting A COVID-19 Vaccine. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/vaccine-benefits.html (accessed on 30 November 2022).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Pfizer-BioNTech COVID-19 Vaccine Reactions and Adverse Events. 2021. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/reactogenicity.html (accessed on 30 November 2022).
- Centers for Disease Control and Prevention. The Moderna COVID-19 Vaccine’s Local Reactions, Systemic Reactions, Adverse Events, and Serious Adverse Events. 2022. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/moderna/Reactogenicity.html (accessed on 30 November 2022).
- Mortazavi, S. COVID-19 Vaccination–Associated Axillary Adenopathy: Imaging Findings and Follow-Up Recommendations in 23 Women. Am. J. Roentgenol. 2021, 217, 857–858. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Sales, R.M.; Babagbemi, K.; Levy, A.D.; McGrath, A.L.; Drotman, M.; Dodelzon, K. Unilateral axillary adenopathy in the setting of COVID-19 vaccine: Follow-up. Clin. Imaging 2021, 80, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Zütemiz, C.; Krystosek, L.A.; Church, A.L.; Chauhan, A.; Ellermann, J.M.; Domingo-Musibay, E.; Steinberger, D. Lymphadenopathy in COVID-19 Vaccine Recipients: Diagnostic Dilemma in Oncologic Patients. Radiology 2021, 300, E296–E300. [Google Scholar] [CrossRef]
- Avner, M.; Orevi, M.; Caplan, N.; Popovtzer, A.; Lotem, M.; Cohen, J.E. COVID-19 vaccine as a cause for unilateral lymphadenopathy detected by 18F-FDG PET/CT in a patient affected by melanoma. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2659–2660. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Hatabu, H.; Ricciuti, B.; Vaz, V.; Michael, K.; Awad, M.M. Axillary Lymphadenopathy after Coronavirus Disease 2019 Vaccinations in Patients with Thoracic Malignancy: Incidence, Predisposing Factors, and Imaging Characteristics. J. Thorac. Oncol. 2022, 17, 154–159. [Google Scholar] [CrossRef]
- Grimm, L.; Destounits, S.; Dogan, B.; Daly, C.; Tuite, C.; Sonnenblick, E.; Milch, H.; Net, J.; Dodelzon, K.; Yang, R.; et al. Revised SBI Recommendations for the Management of Axillary Adenopathy in Patients with Recent COVID-19 Vaccination. Society of Breast Imaging Patient Care and Delivery Committee. 2022. Available online: https://www.sbi-online.org/sbi-recommendations-position-statements (accessed on 30 November 2022).
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 30 November 2022).
- El-Sayed, M.S.; Wechie, G.N.; Low, C.S.; Adesanya, O.; Rao, N.; Leung, V.J. The incidence and duration of COVID-19 vaccine-related reactive lymphadenopathy on 18F-FDG PET-CT. Clin. Med. 2021, 21, e633–e638. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.E.; Zuckerman, S.P.; Conant, E.F. Management of Unilateral Axillary Lymphadenopathy Detected on Breast MRI in the Era of COVID-19 Vaccination. Am. J. Roentgenol. 2021, 217, 831–834. [Google Scholar] [CrossRef]
- Mitchell, O.R.; Couzins, M.; Dave, R.; Bekker, J.; Brennan, P.A. COVID-19 vaccination and low cervical lymphadenopathy in the two week neck lump clinic-a follow up audit. Br. J. Oral Maxillofac. Surg. 2021, 59, 720–721. [Google Scholar] [CrossRef]
- Abou-Foul, A.K.; Ross, E.; Abou-Foul, M.; George, A.P. Cervical lymphadenopathy following coronavirus disease 2019 vaccine: Clinical characteristics and implications for head and neck cancer services. J. Laryngol. Otol. 2021, 135, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Igual-Rouilleault, A.C.; Soriano, I.; Quan, P.L.; Fernández-Montero, A.; Elizalde, A.; Pina, L. Unilateral axillary adenopathy induced by COVID-19 vaccine: US follow-up evaluation. Eur. Radiol. 2022, 32, 3199–3206. [Google Scholar] [CrossRef]
- Cocco, G.; Pizzi, A.D.; Fabiani, S.; Cocco, N.; Boccatonda, A.; Frisone, A.; Scarano, A.; Schiavone, C. Lymphadenopathy after the Anti-COVID-19 Vaccine: Multiparametric Ultrasound Findings. Biology 2021, 10, 652. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Prada, M.; Rivero-Calle, I.; Calvache-González, A.; Martinón-Torres, F. Acute onset supraclavicular lymphadenopathy coinciding with intramuscular mRNA vaccination against COVID-19 may be related to vaccine injection technique, Spain, January and February 2021. Euro. Surveill. 2021, 26, 2100193. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Lee, J.Y.; Yi, S.Y. Axillary Lymphadenopathy on Ultrasound after COVID-19 Vaccination and Its Influencing Factors: A Single-Center Study. J. Clin. Med. 2022, 11, 238. [Google Scholar] [CrossRef]
- Mehta, N.; Sales, R.M.; Babagbemi, K.; Levy, A.D.; McGrath, A.L.; Drotman, M.; Dodelzon, K. Unilateral axillary Adenopathy in the setting of COVID-19 vaccine. Clin. Imaging 2021, 75, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Adin, M.E.; Isufi, E.; Kulon, M.; Pucar, D. Association of COVID-19 mRNA Vaccine with Ipsilateral Axillary Lymph Node Reactivity on Imaging. JAMA Oncol. 2021, 7, 1241. [Google Scholar] [CrossRef] [PubMed]
- Ahn, R.W.; Mootz, A.R.; Brewington, C.C.; Abbara, S. Axillary Lymphadenopathy after mRNA COVID-19 Vaccination. Radiol. Cardiothorac. Imaging 2021, 3, e210008. [Google Scholar] [CrossRef]
- Ganga, K.; Solyar, A.Y.; Ganga, R. Massive Cervical Lymphadenopathy Post-COVID-19 Vaccination. Ear Nose Throat J. 2021. [Google Scholar] [CrossRef]
- Cocco, G.; Pizzi, A.D.; Taraschi, A.L.; Boccatonda, A.; Corvino, A.; Ucciferri, C.; Falasca, K.; Caulo, M.; Vecchiet, J. Atypical Sites of Lymphadenopathy after Anti-COVID-19 Vaccine: Ultrasound Features. Medicina 2022, 58, 197. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.; Jia, W.; Shi, J.; Yuan, C.; Zhang, Y.; Chen, M. Role of Elastography in Axillary Examination of Patients with Breast Cancer. J. Ultrasound Med. 2018, 37, 699–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Studdiford, J.; Lamb, K.; Horvath, K.; Altshuler, M.; Stonehouse, A. Development of Unilateral Cervical and Supraclavicular Lymphadenopathy after Human Papilloma Virus Vaccination. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2008, 28, 1194–1197. [Google Scholar] [CrossRef]
- Pereira, M.P.; Flores, P.; Neto, A.S. Neck and supraclavicular lymphadenopathy secondary to 9-valent human papillomavirus vaccination. BMJ Case Rep. 2019, 12, e231582. [Google Scholar] [CrossRef] [PubMed]
- Shirone, N.; Shinkai, T.; Yamane, T.; Uto, F.; Yoshimura, H.; Tamai, H.; Imai, T.; Inoue, M.; Kitano, S.; Kichikawa, K.; et al. Axillary lymph node accumulation on FDG-PET/CT after influenza vaccination. Ann. Nucl. Med. 2012, 26, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Panagiotidis, E.; Exarhos, D.; Housianakou, I.; Bournazos, A.; Datseris, I. FDG uptake in axillary lymph nodes after vaccination against pandemic (H1N1). Eur. Radiol. 2010, 20, 1251–1253. [Google Scholar] [CrossRef]
- Casey, C.G.; Iskander, J.K.; Roper, M.H.; Mast, E.E.; Wen, X.J.; Török, T.J.; Chapman, L.E.; Swerdlow, D.L.; Morgan, J.; Hef-felfinger, J.D.; et al. Adverse events associated with smallpox vaccination in the United States, January–October 2003. JAMA 2005, 294, 2734–2743. [Google Scholar] [CrossRef] [Green Version]
- Dorfman, R.F.; Herweg, J.C. Live, attenuated measles virus vaccine. Inguinal lymphadenopathy complicating administration. JAMA 1966, 198, 320–321. [Google Scholar] [CrossRef] [PubMed]
- Goraya, J.S.; Virdi, V.S. Bacille Calmette-Guérin lymphadenitis. Postgrad. Med. J. 2002, 78, 327–329. [Google Scholar] [CrossRef] [Green Version]
- Hartsock, R.J. Postvaccinial lymphadenitis. Hyperplasia of lymphoid tissue that simulates malignant lymphomas. Cancer 1968, 21, 632–649. [Google Scholar] [CrossRef]
- De Giorgis, S.; Garlaschi, A.; Brunetti, N.; Tosto, S.; Rescinito, G.; Monetti, F.; Oddone, C.; Massa, B.; Pitto, F.; Calabrese, M.; et al. Axillary adenopathy after COVID-19 vaccine in patients undergoing breast ultrasound. J. Ultrason. 2021, 21, 361–364. [Google Scholar] [CrossRef] [PubMed]
- García-Molina, F.; Cegarra-Navarro, M.F.; Andrade-Gonzales, R.J.; Martinez-Díaz, F. Cytologic and histologic features of COVID-19 post-vaccination lymphadenopathy. Cytojournal 2021, 18, 34. [Google Scholar] [CrossRef] [PubMed]
- Teefey, S.A.; Middleton, W.D.; Turner, J.S.; Ellebedy, A.H.; Suessen, T.; Wallendorf, M.; O’Halloran, J.A.; Presti, R. SARS-CoV-2 mRNA Vaccination Causes Prolonged Increased Cortical Thickening and Vascularity in Ipsilateral Axillary Lymph Nodes. J. Ultrasound Med. 2022, 41, 2849–2858. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; Miki, S.; Nakao, T.; Koshino, S.; Hayashi, N.; Abe, O. Axillary Lymphadenopathy after Pfizer-BioNTech and Moderna COVID-19 Vaccination: MRI Evaluation. Radiology 2022, 306, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.M.; Hue, S.S.-S.; Wee, A.; See, K.C. Kikuchi–Fujimoto Disease Post COVID-19 Vaccination: Case Report and Review of Literature. Vaccines 2021, 9, 1251. [Google Scholar] [CrossRef] [PubMed]
- Caocci, G.; Fanni, D.; Porru, M.; Greco, M.; Nemolato, S.; Firinu, D.; Faa, G.; Scuteri, A.; La Nasa, G. Kikuchi-Fujimoto disease associated with hemophagocytic lymphohistiocytosis following the BNT162b2 mRNA COVID-19 vaccination. Haematologica 2022, 107, 1222–1225. [Google Scholar] [CrossRef]
- Saito, K.; Ichikawa, S.; Hatta, S.; Katsuoka, Y.; Harigae, H.; Izumi, T. Vincristine therapy for severe and refractory immune thrombocytopenia following COVID-19 vaccination. Ann. Hematol. 2022, 101, 885–887. [Google Scholar] [CrossRef]
- Ah-Thiane, L.; Ferrer, L.; Maucherat, B.; Fleury, V.; Le Thiec, M.; Rusu, D.; Rousseau, C. Vaccine-Related Lymph Nodes: The Emerging Pitfalls of 18F-Fluorocholine and 68Ga-PSMA-11 PET/CT in the Era of COVID-19 Vaccination. Clin. Nucl. Med. 2022, 47, 575–582. [Google Scholar] [CrossRef]
- Eifer, M.; Tau, N.; Alhoubani, Y.; Kanana, N.; Domachevsky, L.; Shams, J.; Keret, N.; Gorfine, M.; Eshet, Y. COVID-19 mRNA Vaccination: Age and Immune Status and Its Association with Axillary Lymph Node PET/CT Uptake. J. Nucl. Med. 2022, 63, 134–139. [Google Scholar] [CrossRef]
- Maimone, S.; Robinson, K.A.; Advani, P.P.; Li, Z.; Gococo-Benore, D.A.; Qosja, N.; Ashai, A.M.; Mummareddy, A.; Chumsri, S. Limiting Screening Mammography Recalls for Vaccine-Induced Adenopathy, a Single Institution Experience. Acad. Radiol. 2022, 29, 1480–1485. [Google Scholar] [CrossRef]
- Shin, M.; Hyun, C.Y.; Choi, Y.H.; Choi, J.Y.; Lee, K.H.; Cho, Y.S. COVID-19 Vaccination-Associated Lymphadenopathy on FDG PET/CT: Distinctive Features in Adenovirus-Vectored Vaccine. Clin. Nucl. Med. 2021, 46, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.H.; Shah, S.; Groves, A.M.; Wan, S.; Malhotra, A. The Challenge of Staging Breast Cancer with PET/CT in the Era of COVID Vaccination. Clin. Nucl. Med. 2021, 46, 1006–1010. [Google Scholar] [CrossRef]
- Heaven, C.L.; Barber, L.; Ahmadi, O.; Selvarajah, K.; Shetty, S. COVID-19 vaccine associated cervical lymphadenopathy: A case series. ANZ J. Surg. 2022, 92, 2286–2291. [Google Scholar] [CrossRef]
- Özütemiz, C.; Potter, D.A.; Özütemiz, A.; Steinberger, D. Lymphadenopathy after the Third Covid-19 Vaccine. Curr. Probl. Cancer Case Rep. 2021, 4, 100127. [Google Scholar] [CrossRef] [PubMed]
- Hagen, C.; Nowack, M.; Messerli, M.; Saro, F.; Mangold, F.; Bode, P.K. Fine needle aspiration in COVID-19 vaccine-associated lymphadenopathy. Swiss Med. Wkly. 2021, 151, w20557. [Google Scholar] [CrossRef]
- Wolfson, S.; Kim, E. Breast Cancer Screening and Axillary Adenopathy in the Era of COVID-19 Vaccination. Radiology 2023, 306, 222040. [Google Scholar] [CrossRef]
- Xu, G.M.; Lu, Y.M. COVID-19 mRNA Vaccination–Induced Lymphadenopathy Mimics Lymphoma Progression on FDG PET/CT. Clin. Nucl. Med. 2021, 46, 353–354. [Google Scholar] [CrossRef] [PubMed]
- Nawwar, A.A.; Searle, J.; Singh, R.; Lyburn, I.D. Oxford-AstraZeneca COVID-19 vaccination induced lymphadenopathy on [18F]Choline PET/CT-not only an FDG finding. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2657–2658. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, O.R.; Dave, R.; Bekker, J.; Brennan, P.A. Supraclavicular lymphadenopathy following COVID-19 vaccination: An increasing presentation to the two-week wait neck lump clinic? Br. J. Oral Maxillofac. Surg. 2021, 59, 384–385. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Giuliano, P. 18F-FDG–Avid Lymph Nodes after COVID-19 Vaccination on 18F-FDG PET/CT. Clin. Nucl. Med. 2021, 46, 433–434. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.C.; Martiniova, L.; Masrani, A.; Ravizzini, G.C. 18F-Fluciclovine–Avid Reactive Axillary Lymph Nodes After COVID-19 Vaccination. Clin. Nucl. Med. 2022, 47, 154–155. [Google Scholar] [CrossRef]
- Garreffa, E.; York, J.; Turnbull, A.; Kendrick, D. Regional lymphadenopathy following COVID-19 vaccination: Considerations for primary care management. Br. J. Gen. Pract. 2021, 71, 284–285. [Google Scholar] [CrossRef]
- Prieto, P.A.; Mannava, K.; Sahasrabudhe, D.M. COVID-19 mRNA vaccine-related adenopathy mimicking metastatic mela-noma. Lancet Oncol. 2021, 22, e281. [Google Scholar] [CrossRef] [PubMed]
- Roca, M.M.; Roca, B.; Rambla, M. Supraclavicular lymphadenopathy secondary to COVID-19 BNT162b2 vaccine. J. Postgrad. Med. 2021, 67, 180–181. [Google Scholar] [CrossRef] [PubMed]
- Tan, N.J.H.; Tay, K.X.J.; Wong, S.B.J.; Nga, M.E. COVID-19 post-vaccination lymphadenopathy: Report of cytological findings from fine needle aspiration biopsy. Diagn. Cytopathol. 2021, 49, E467–E470. [Google Scholar] [CrossRef]
- Gable, A.D.; Hughes, S.M.; Miller, R.J. A 24-Year-Old Man with Hemoptysis Found to Have a Chest Mass and Contralateral Axillary Lymphadenopathy. Chest 2021, 160, e289–e293. [Google Scholar] [CrossRef] [PubMed]
- Suleman, A.; Bilbily, A.; Cheung, M.; Chodirker, L. Hypermetabolic lymphadenopathy on positron emission tomography scan following COVID-19 vaccination: A mimicker of disease progression in Hodgkin lymphoma. Ejhaem 2021, 2, 678–679. [Google Scholar] [CrossRef] [PubMed]
- Tintle, S.; Chen, M. Lymphadenopathy with florid lymphoid and Langerhans cell hyperplasia and hemophagocytosis mimicking lymphoma after COVID-19 mRNA vaccination. EJHaem 2021, 2, 845–847. [Google Scholar] [CrossRef]
- Weeks, J.K.; O’Brien, S.R.; Rosenspire, K.C.; Dubroff, J.G.; Pantel, A.R. Evolving Bilateral Hypermetabolic Axillary Lymphadenopathy on FDG PET/CT Following 2-Dose COVID-19 Vaccination. Clin. Nucl. Med. 2021, 46, 1011–1012. [Google Scholar] [CrossRef]
- Mori, M.; Fujioka, T.; Yashima, Y.; Yamaga, E.; Nakagawa, T.; Kubota, K.; Tateishi, U. Deep axillary lymphadenopathy after coronavirus disease 2019 vaccination: A case report. J. Med. Ultrason. 2022, 49, 111–112. [Google Scholar] [CrossRef]
- Tzankov, A.; Rössle, M. Extrafollicular proliferation of B-blasts: Morphologic correlate to Spikevax-induced lymphadenopathy. Clin. Case Rep. 2022, 10, e5398. [Google Scholar] [CrossRef]
- Chan, H.-P.M.; Shen, D.H.-Y.M.; Yang, M.-H.; Hu, C.; Tyan, Y.-C. Incidental Finding of Moderna COVID-19 Vaccination–Related Axillary Lymphadenopathy on 201Tl Myocardial Perfusion Imaging. Clin. Nucl. Med. 2022, 47, e302–e303. [Google Scholar] [CrossRef]
- Adin, M.E.; Wu, J.; Isufi, E.; Tsui, E.; Pucar, D. Ipsilateral Malignant Axillary Lymphadenopathy and Contralateral Reactive Lymph Nodes in a COVID-19 Vaccine Recipient with Breast Cancer. J. Breast Cancer 2022, 25, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.S.; Kim, M.Y. Bilateral Cervical Lymphadenopathy after mRNA COVID-19 Vaccination on Oral Squamous Cell Car-cinoma Patient: A Case Report. Diagnostics 2022, 12, 1518. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Jiang, W.; Chen, N.; Li, J.; Wang, X.; Li, M.; Wang, D.; Jiang, L. Misdiagnosis of Reactive Lymphadenopathy Remotely after COVID-19 Vaccination: A Case Report and Literature Review. Front. Immunol. 2022, 13, 875637. [Google Scholar] [CrossRef] [PubMed]
- Ashoor, A.; Shephard, J.; Lissidini, G.; Nicosia, L. Axillary Adenopathy in Patients with Recent Covid-19 Vaccination: A New Diagnostic Dilemma. Korean J. Radiol. 2021, 22, 2124–2126. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Hong, J.Y.; Kim, S.Y.; Na, S.J. Ipsilateral Radial Neuropathy after COVID-19 mRNA Vaccination in an Immuno-competent Young Man. Yonsei Med. J. 2022, 63, 966–970. [Google Scholar] [CrossRef] [PubMed]
- Kado, S.; Kamiya, K.; Iwabuchi, S.; Kajii, E.; Ohtsuki, M. Unilateral lymphadenopathy associated with COVID-19 vaccination. J. Cutan. Immunol. Allergy 2021, 5, 100–101. [Google Scholar] [CrossRef]
- Aalberg, J.J.; Collins, T.P.; Dobrow, E.M. Axillary lymphadenopathy in a renal cell carcinoma patient after COVID-19 Vaccination. Radiol. Case Rep. 2021, 16, 2164–2167. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Reis, A.; Osório, C.; Scigliano, H.; Nora, M. A Case of Cervical Lymphadenopathy after Vaccination against COVID-19. Cureus 2021, 13, e15050. [Google Scholar] [CrossRef] [PubMed]
- Lam, D.L.; Flanagan, M.R. Axillary Lymphadenopathy after COVID-19 Vaccination in a Woman with Breast Cancer. JAMA 2022, 327, 175–176. [Google Scholar] [CrossRef]
- Musaddaq, B.; Brown, A.; Dluzewski, S.; Marafioti, T.; Malhotra, A. Axillary lymphadenopathy in a high-risk breast screening patient following the COVID-19 vaccine: A diagnostic conundrum. BJR case Rep. 2022, 7, 20210063. [Google Scholar] [CrossRef] [PubMed]
- Dirven, I.; Bravenboer, B.; Raeymaeckers, S.; Andreescu, C.E. Lymphadenopathy after COVID-19 vaccination in patients with endocrine cancer: Two case reports. Endocrinol. Diabetes Metab. Case Rep. 2022, 2022, 220–258. [Google Scholar] [CrossRef] [PubMed]
- Pudis, M.; Conejero, J.L.V.; Marcuartu, J.J.M.; Romera, M.C. 68Ga-DOTATOC-avid lymphadenopathies induced from COVID-19 mRNA vaccination. Jpn. J. Clin. Oncol. 2021, 51, 1765. [Google Scholar] [CrossRef] [PubMed]
- Andresciani, F.; Ricci, M.; Grasso, R.F.; Zobel, B.B.; Quattrocchi, C.C. COVID-19 vaccination simulating lymph node progres-sion in a patient with prostate cancer. Radiol. Case Rep. 2022, 17, 2996–2999. [Google Scholar] [CrossRef] [PubMed]
- Cheong, K.M.; Tsai, T.-Y. A Woman with Painful Neck after COVID-19 Vaccination. Ann. Emerg. Med. 2022, 79, e13–e14. [Google Scholar] [CrossRef]
- Guan, Y.; Xia, X.; Lu, H. Kikuchi–Fujimoto disease following vaccination against COVID-19. J. Hematop. 2022, 15, 21–23. [Google Scholar] [CrossRef]
- Kashiwada, T.; Saito, Y.; Terasaki, Y.; Shirakura, Y.; Shinbu, K.; Tanaka, T.; Tanaka, Y.; Seike, M.; Gemma, A. Kikuchi-Fujimoto disease can present as delayed lymphadenopathy after COVID-19 vaccination. Hum. Vaccines Immunother. 2022, 18, 2071080. [Google Scholar] [CrossRef]
- Tsumura, Y.; Asakura, K.; Takahashi, I.; Akaihata, M.; Takahashi, Y.; Ishida, Y. New mimic of relapse or regional lymph node metastasis in a cancer survivor: A case of mRNA COVID-19 vaccine-induced lymphadenitis with high FDG uptake. Immunol. Med. 2022, 45, 45–47. [Google Scholar] [CrossRef]
- Sekizawa, A.; Hashimoto, K.; Kobayashi, S.; Kozono, S.; Kobayashi, T.; Kawamura, Y.; Kimata, M.; Fujita, N.; Ono, Y.; Obuchi, Y.; et al. Rapid progression of marginal zone B-cell lymphoma after COVID-19 vaccination (BNT162b2): A case report. Front. Med. 2022, 9, 963393. [Google Scholar] [CrossRef]
- Mizutani, M.; Mitsui, H.; Amano, T.; Ogawa, Y.; Deguchi, N.; Shimada, S.; Miwa, A.; Kawamura, T.; Ogido, Y. Two cases of axillary lymphadenopathy diagnosed as diffuse large B-cell lymphoma developed shortly after BNT162b2 COVID-19 vac-cination. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e613–e615. [Google Scholar] [CrossRef]
- Goldman, S.; Bron, D.; Tousseyn, T.; Vierasu, I.; Dewispelaere, L.; Heimann, P.; Cogan, E.; Goldman, M. Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot: A Case Report. Front. Med. 2021, 8, 798095. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.; Krauthammer, S.H.; Cohen, Y.C.; Perry, C.; Avivi, I.; Herishanu, Y.; Even-Sapir, E. Correlation between BNT162b2 mRNA Covid-19 vaccine-associated hypermetabolic lymphadenopathy and humoral immunity in patients with hematologic malignancy. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3540–3549. [Google Scholar] [CrossRef]
- Girardin, F.R.; Tzankov, A.; Pantaleo, G.; Livio, F.; Greub, G. Multifocal lymphadenopathies with polyclonal reactions primed after EBV infection in a mRNA-1273 vaccine recipient. Swiss Med. Wkly. 2022, 152, w30188. [Google Scholar] [CrossRef]
- Hoffmann, C.; Wechselberger, T.; Drexel, H.; Dertinger, S.; Dirnhofer, S.; Pierson, S.K.; Fajgenbaum, D.C.; Kessler, A. Idiopathic Multicentric Castleman Disease Occurring Shortly after mRNA SARS-CoV-2 Vaccine. Vaccines 2022, 10, 1725. [Google Scholar] [CrossRef]
- Alhossan, A.; Alsaran, A.K.; Almahmudi, A.H.; Aljohani, Z.S.; Albishi, M.R.; Almutairi, A.K. Adverse Events of COVID-19 Vaccination among the Saudi Population: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 2089. [Google Scholar] [CrossRef] [PubMed]
- Bshesh, K.; Khan, W.; Vattoth, A.L.; Janjua, E.; Nauman, A.; Almasri, M.; Ali, A.M.; Ramadorai, V.; Mushannen, B.; Al Subaie, M.; et al. Lymphadenopathy post-COVID-19 vaccination with increased FDG uptake may be falsely attributed to oncological disorders: A systematic review. J. Med. Virol. 2022, 94, 1833–1845. [Google Scholar] [CrossRef] [PubMed]
- Co, M.; Wong, P.C.P.; Kwong, A. COVID-19 vaccine associated axillary lymphadenopathy–A systematic review. Cancer Treat. Res. Commun. 2022, 31, 100546. [Google Scholar] [CrossRef] [PubMed]
- Chua, T.H.; Takano, A. Pathological Findings in COVID-19 and Non-COVID-19 Vaccine-Associated Lymphadenopathy: A Systematic Review. J. Clin. Med. 2022, 11, 6290. [Google Scholar] [CrossRef] [PubMed]
- Garreffa, E.; Hamad, A.; O’Sullivan, C.C.; Hazim, A.Z.; York, J.; Puri, S.; Turnbull, A.; Robertson, J.F.; Goetz, M.P. Regional lymphadenopathy following COVID-19 vaccination: Literature review and considerations for patient management in breast cancer care. Eur. J. Cancer 2021, 159, 38–51. [Google Scholar] [CrossRef]
- Ryan, F.J.; Norton, T.S.; McCafferty, C.; Blake, S.J.; Stevens, N.E.; James, J.; Eden, G.L.; Tee, Y.C.; Benson, S.C.; Masavuli, M.G.; et al. A systems immunology study comparing innate and adaptive immune responses in adults to COVID-19 mRNA and adenovirus vectored vaccines. Cell Rep. Med. 2023, 100971. [Google Scholar] [CrossRef]
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef]
- Youn, H.; Hong, K.-J. Non-invasive molecular imaging of immune cell dynamics for vaccine research. Clin. Exp. Vaccine Res. 2019, 8, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Yri, O.E.; Torfoss, D.; Hungnes, O.; Tierens, A.; Waalen, K.; Nordøy, T.; Dudman, S.; Kilander, A.; Wader, K.F.; Østenstad, B.; et al. Rituximab blocks protective serologic response to influenza A (H1N1) 2009 vaccination in lymphoma patients during or within 6 months after treatment. Blood 2011, 118, 6769–6771. [Google Scholar] [CrossRef] [Green Version]
- Crombie, J.L.; Sherman, A.C.; Cheng, C.-A.; Ryan, C.E.; Zon, R.; Desjardins, M.; Baker, P.; McDonough, M.; Izaguirre, N.; Bausk, B.; et al. Activity of mRNA COVID-19 vaccines in patients with lymphoid malignancies. Blood Adv. 2021, 5, 3062–3065. [Google Scholar] [CrossRef] [PubMed]
- Madelon, N.; Lauper, K.; Breville, G.; Sabater Royo, I.; Goldstein, R.; Andrey, D.O.; Grifoni, A.; Sette, A.; Kaiser, L.; Siegrist, C.A.; et al. Robust T-Cell Responses in Anti-CD20-Treated Patients Following COVID-19 Vaccination: A Prospective Cohort Study. Clin. Infect. Dis. 2022, 75, e1037–e1045. [Google Scholar] [CrossRef]
- Shields, A.M.; Venkatachalam, S.; Shafeek, S.; Paneesha, S.; Ford, M.; Sheeran, T.; Kelly, M.; Qureshi, I.; Salhan, B.; Karim, F.; et al. SARS-CoV-2 vaccine responses following CD20-depletion treatment in patients with haematological and rheumatological disease: A West Midlands Research Consortium study. Clin. Exp. Immunol. 2022, 207, 3–10. [Google Scholar] [CrossRef]
- Bettini, E.; Locci, M. SARS-CoV-2 mRNA Vaccines: Immunological Mechanism and Beyond. Vaccines 2021, 9, 147. [Google Scholar] [CrossRef]
- Lederer, K.; Castaño, D.; Gómez Atria, D.; Oguin, T.H., III; Wang, S.; Manzoni, T.B.; Muramatsu, H.; Hogan, M.J.; Amanat, F.; Cherubin, P.; et al. SARS-CoV-2 mRNA Vaccines Foster Potent Antigen-Specific Germinal Center Responses Associated with Neutralizing Antibody Generation. Immunity 2020, 53, 1281–1295.e5. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.S.; O’Halloran, J.A.; Kalaidina, E.; Kim, W.; Schmitz, A.J.; Zhou, J.Q.; Lei, T.; Thapa, M.; Chen, R.E.; Case, J.B.; et al. SARS-CoV-2 mRNA vaccines induce persistent human germinal centre responses. Nature 2021, 596, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Gee, J.; Marquez, P.; Su, J.; Calvert, G.M.; Liu, R.; Myers, T.; Nair, N.; Martin, S.; Clark, T.; Markowitz, L.; et al. First Month of COVID-19 Vaccine Safety Monitoring-United States, December 14, 2020-January 13, 2021. Morb. Mortal Wkly. Rep. 2021, 70, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.S.; Galan, A.; Watsky, K.L.; Little, A.J. Delayed Localized Hypersensitivity Reactions to the Moderna COVID-19 Vaccine: A Case Series. JAMA Dermatol. 2021, 157, 716–720. [Google Scholar] [CrossRef] [PubMed]
- McNeil, M.M.; DeStefano, F. Vaccine-associated hypersensitivity. J. Allergy Clin. Immunol. 2018, 141, 463–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potluri, T.; Fink, A.L.; Sylvia, K.E.; Dhakal, S.; Vermillion, M.S.; Steeg, L.V.; Deshpande, S.; Narasimhan, H.; Klein, S.L. Age-associated changes in the impact of sex steroids on influenza vaccine responses in males and females. NPJ Vaccines 2019, 4, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castle, S.C. Clinical Relevance of Age-Related Immune Dysfunction. Clin. Infect. Dis. 2000, 31, 578–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pozzetto, B.; Legros, V.; Djebali, S.; Barateau, V.; Guibert, N.; Villard, M.; Peyrot, L.; Allatif, O.; Fassier, J.B.; Massar-dier-Pilonchéry, A.; et al. Immunogenicity and efficacy of heterologous ChAdOx1-BNT162b2 vaccination. Nature 2021, 600, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.M.; Choi, S.M. Kikuchi-Fujimoto Disease: A Review. Arch. Pathol. Lab. Med. 2018, 142, 1341–1346. [Google Scholar] [CrossRef] [Green Version]
- Becker, A.S.; Perez-Johnston, R.; Chikarmane, S.A.; Chen, M.M.; El Homsi, M.; Feigin, K.N.; Gallagher, K.M.; Hanna, E.Y.; Hicks, M.; Ilica, A.T.; et al. Multidisciplinary Recommendations Regarding Post-Vaccine Adenopathy and Radiologic Imaging: Radi-ology Scientific Expert Panel. Radiology 2021, 300, E323–E327. [Google Scholar] [CrossRef] [PubMed]
- Seely, J.M.; Barry, M.H. The Canadian Society of Breast Imaging Recommendations for the Management of Axillary Ade-nopathy in Patients with Recent COVID-19 Vaccination-Update. Can. Assoc. Radiol. J. 2021, 72, 601–602. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, T.-C.; Shen, D.H.-Y.; Chang, C.-C.; Chan, H.-P.; Chuang, K.-P.; Yuan, C.-H.; Chen, C.-N.; Yang, M.-H.; Tyan, Y.-C. Immune Response Related to Lymphadenopathy Post COVID-19 Vaccination. Vaccines 2023, 11, 696. https://doi.org/10.3390/vaccines11030696
Ho T-C, Shen DH-Y, Chang C-C, Chan H-P, Chuang K-P, Yuan C-H, Chen C-N, Yang M-H, Tyan Y-C. Immune Response Related to Lymphadenopathy Post COVID-19 Vaccination. Vaccines. 2023; 11(3):696. https://doi.org/10.3390/vaccines11030696
Chicago/Turabian StyleHo, Tzu-Chuan, Daniel Hueng-Yuan Shen, Chin-Chuan Chang, Hung-Pin Chan, Kuo-Pin Chuang, Cheng-Hui Yuan, Ciao-Ning Chen, Ming-Hui Yang, and Yu-Chang Tyan. 2023. "Immune Response Related to Lymphadenopathy Post COVID-19 Vaccination" Vaccines 11, no. 3: 696. https://doi.org/10.3390/vaccines11030696