
Tetanus and Diphtheria Seroprotection among Children Younger Than 15 Years in Nigeria, 2018: Who Are the Unprotected Children?

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Sampling
2.2. Laboratory Methods and Testing
2.2.1. Antigens and Couplings
2.2.2. Sample Preparation and Bead Assay
2.2.3. Quality Control and Assurance
2.2.4. Cutoffs and Interpolation
2.3. Statistical Analyses
3. Results
3.1. General Demographics of Study Population
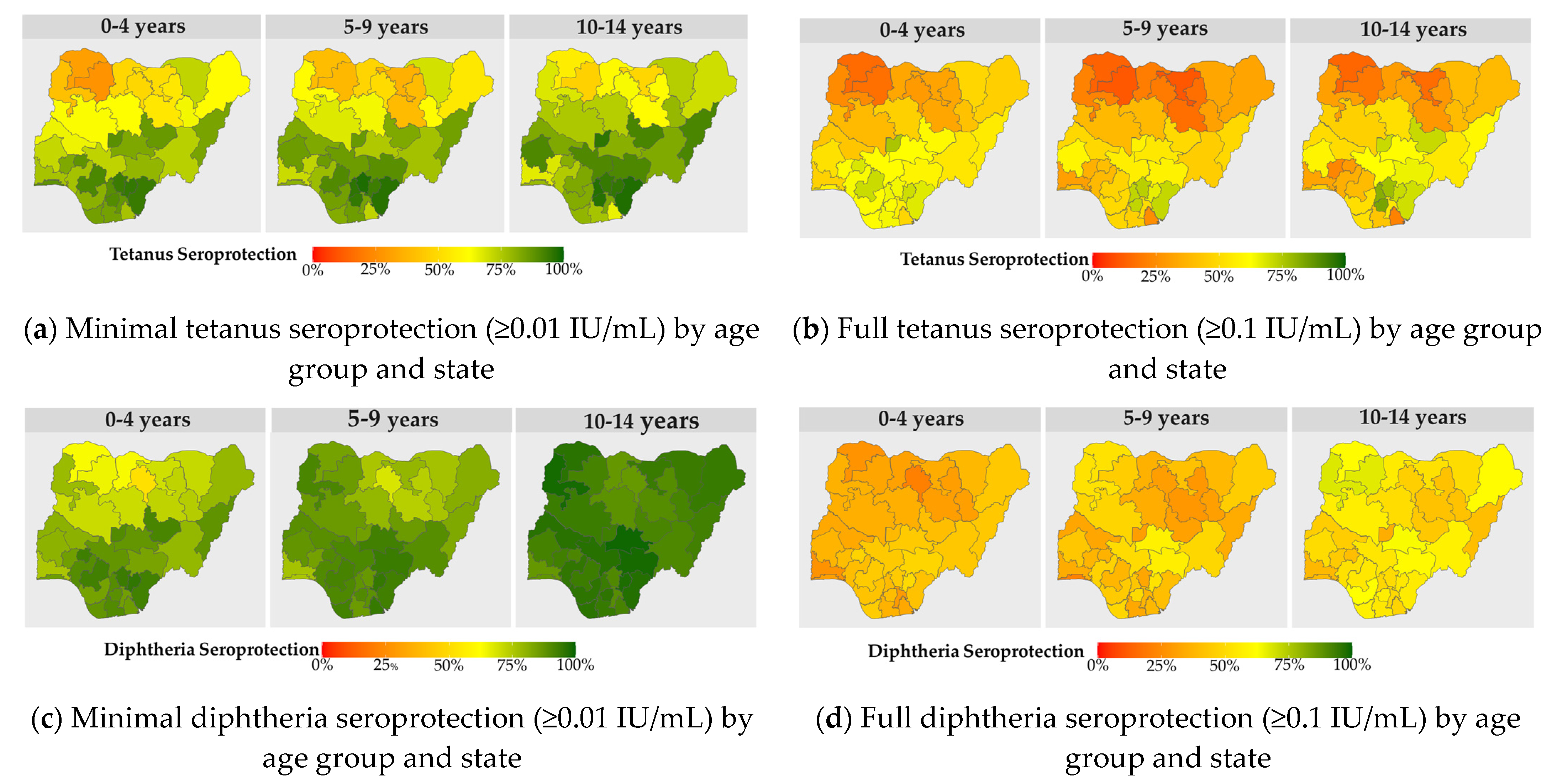
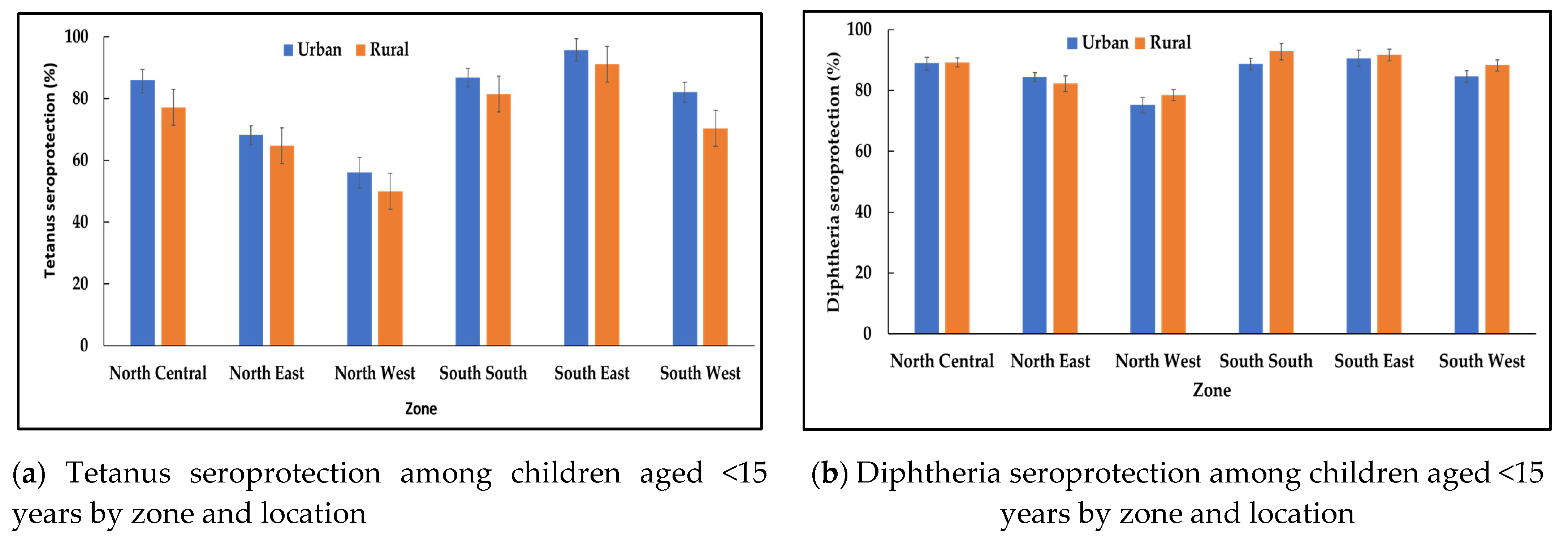
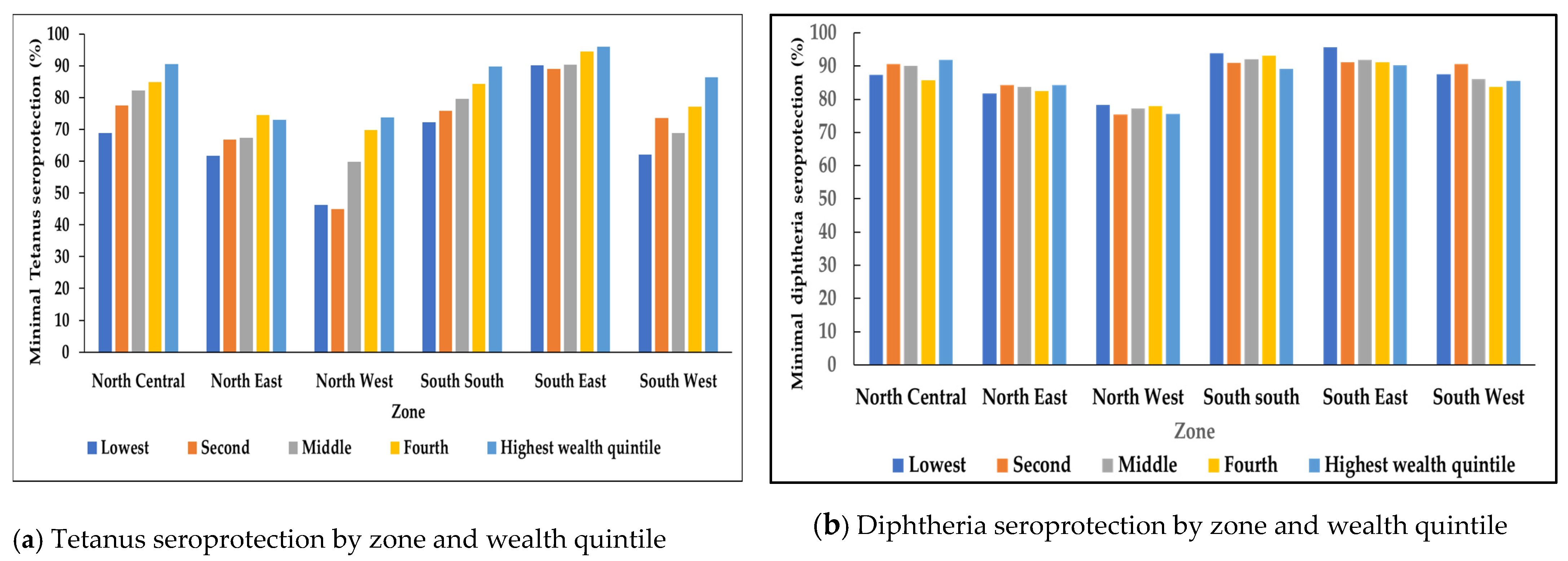
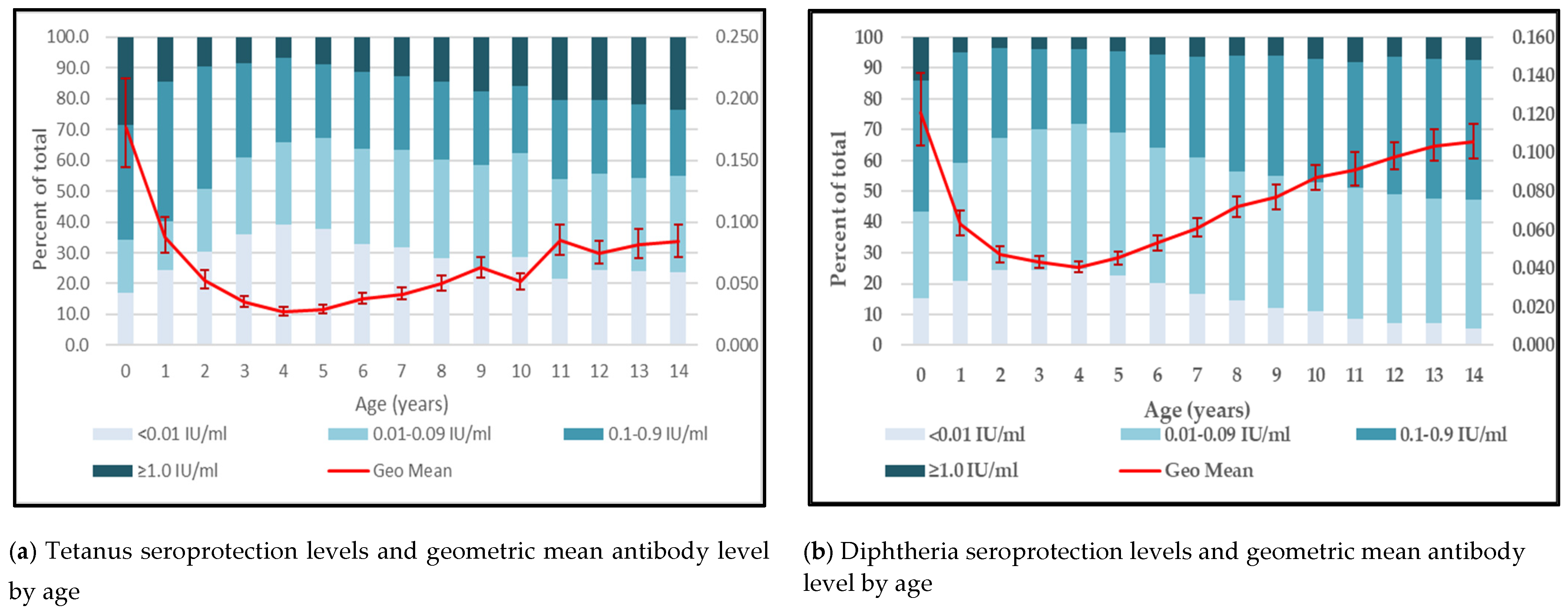
3.2. Tetanus and Diphtheria Seroprotection
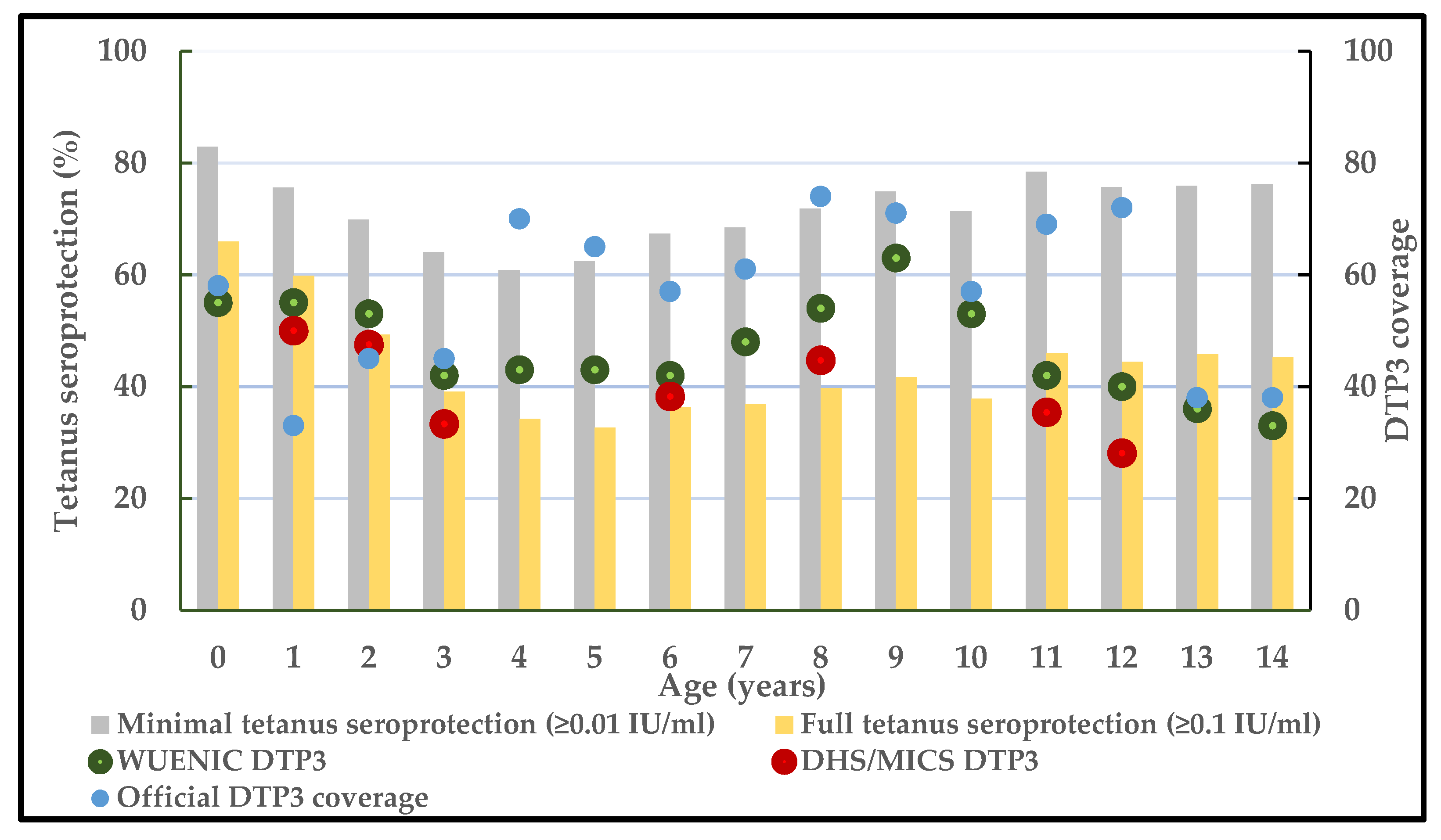
3.3. Triangulation of Tetanus Seroprotection and Vaccination Coverage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacNeil, A.; Lee, C.W.; Dietz, V. Issues and considerations in the use of serologic biomarkers for classifying vaccination history in household surveys. Vaccine 2014, 32, 4893–4900. [Google Scholar] [CrossRef]
- Cutts, F.T.; Hanson, M. Seroepidemiology: An underused tool for designing and monitoring vaccination programmes in low- and middle-income countries. Trop. Med. Int. Health 2016, 21, 1086–1098. [Google Scholar] [CrossRef]
- E Metcalf, C.J.; Farrar, J.; Cutts, F.T.; Basta, N.E.; Graham, A.L.; Lessler, J.; Ferguson, N.M.; Burke, D.S.; Grenfell, B.T. Use of serological surveys to generate key insights into the changing global landscape of infectious disease. Lancet 2016, 388, 728–730. [Google Scholar] [CrossRef] [PubMed]
- Arnold, B.F.; Scobie, H.M.; Priest, J.W.; Lammie, P.J. Integrated serologic surveillance of population immunity and disease transmission. Emerg. Infect. Dis. 2018, 24, 1188–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scobie, H.M.; Mao, B.; Buth, S.; Wannemuehler, K.A.; Sørensen, C.; Kannarath, C.; Jenks, M.H.; Moss, D.M.; Priest, J.W.; Soeung, S.C.; et al. Tetanus Immunity among Women Aged 15 to 39 Years in Cambodia: A National Population-Based Serosurvey, 2012. Clin. Vaccine Immunol. 2016, 23, 546–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, K.S.; White, J.M.; Andrews, N.J.; Borrow, R.; Stanford, E.; Newton, E.; Pebody, R.G. Immunity to tetanus and diphtheria in the UK in 2009. Vaccine 2012, 30, 7111–7117. [Google Scholar] [PubMed]
- Deming, M.S.; Roungo, J.B.; Kristiansen, M.; Heron, I.; Yango, A.; Guenengafo, A.; Ndamobissi, R. Tetanus toxoid coverage as an indicator of serological protection against neonatal tetanus. Bull. World. Health Organ. 2002, 80, 696–703. [Google Scholar]
- Scobie, H.M.; Patel, M.; Martin, D.; Mkocha, H.; Njenga, S.M.; Odiere, M.R.; Pelletreau, S.; Priest, J.W.; Thompson, R.; Won, K.Y.; et al. Tetanus Immunity Gaps in Children 5–14 Years and Men ≥15 Years of Age Revealed by Integrated Disease Serosurveillance in Kenya, Tanzania, and Mozambique. Am. J. Trop. Med. Hyg. 2017, 96, 415–420. [Google Scholar] [CrossRef]
- Travassos, M.A.; Beyene, B.; Adam, Z.; Campbell, J.D.; Mulholland, N.; Diarra, S.S.; Kassa, T.; Oot, L.; Sequeira, J.; Reymann, M.; et al. Immunization Coverage Surveys and Linked Biomarker Serosurveys in Three Regions in Ethiopia. PLoS ONE 2016, 11, e0149970. [Google Scholar] [CrossRef]
- Minta, A.A.; Andre-Alboth, J.; Childs, L.; Nace, D.; Rey-Benito, G.; Boncy, J.; Adrien, P.; Francois, J.; Charles, N.P.J.; Blot, V.; et al. Seroprevalence of measles, rubella, tetanus, and diphtheria antibodies among children in Haiti, 2017. Am. J. Trop. Med. Hyg. 2020, 103, 1717–1725. [Google Scholar] [CrossRef]
- Cheng, A.; Ghanem-Uzqueda, A.; Hoff, N.A.; Ashbaugh, H.; Doshi, R.H.; Mukadi, P.; Budd, R.; Higgins, S.G.; Randall, C.; Gerber, S.; et al. Tetanus seroprotection among children in the democratic republic of the Congo, 2013–2014. PLoS ONE 2022, 17, e0268703. [Google Scholar] [CrossRef] [PubMed]
- Heron, I.; Hey, A.S.; Kurtzhals, J.A.L.; Okong’o-Odera, E.A.; Kjeldsen, K. Immunity to Tetanus and Diphtheria in.Rural Africa. Am. J. Trop. Med. Hyg. 1997, 56, 576–579. [Google Scholar]
- Campbell, J.D.; Pasetti, M.F.; Oot, L.; Adam, Z.; Tefera, M.; Beyane, B.; Mulholland, N.; Steinglass, R.; Krey, R.; Chen, W.H.; et al. Linked vaccination coverage surveys plus serosurveys among Ethiopian toddlers undertaken three years apart to compare coverage and serologic evidence of protection in districts implementing the RED-QI approach. Vaccine 2021, 39, 5802–5813. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Vaccine Preventable Diseases Surveillance Standards: Annex 2 Tetanus Serosurveys. Available online: https://www.who.int/publications/m/item/vaccine-preventable-diseases-surveillance-standards-annex2 (accessed on 25 January 2023).
- Dalal, S.; Samuelson, J.; Reed, J.; Yakubu, A.; Ncube, B.; Baggaley, R. Tetanus disease and deaths in men reveal need for vaccination. Bull. World Health Organ. 2016, 94, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Woldeamanuel, Y.W.; Andemeskel, A.T.; Kyei, K.; Woldeamanuel, M.W.; Woldeamanuel, W. Case fatality of adult tetanus in Africa: Systematic review and meta-analysis. J. Neurol. Sci. 2016, 368, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Besa, N.C.; Coldiron, M.E.; Bakri, A.; Raji, A.; Nsuami, M.J.; Rousseau, C.; Hurtado, N.; Porten, K. Diphtheria outbreak with high mortality in northeastern Nigeria. Epidemiol. Infect. 2014, 142, 797–802. [Google Scholar] [CrossRef] [Green Version]
- Sadoh, A.E.; Oladokun, R.E. Re-emergence of diphtheria and pertussis: Implications for Nigeria. Vaccine 2012, 30, 7221–7228. [Google Scholar] [CrossRef] [PubMed]
- The Guardian Nigeria. NCDC Confirm 123 Diphtheria Cases, 38 Deaths in 4 States. Available online: https://guardian.ng/news/ncdc-confirms-123-diphtheria-cases-38-deaths-in-4-states/ (accessed on 26 January 2023).
- World Health Organization. Tetanus vaccines: WHO position paper–February 2017. Wkly. Epidemiol. Rec. 2017, 92, 53–76. [Google Scholar]
- World Health Organization. Diphtheria vaccines: WHO position paper–August 2017. Wkly. Epidemiol. Rec. 2017, 92, 417–436. [Google Scholar]
- Federal Ministry of Health, Nigeria. Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS) 2018: Technical Report. Abuja, Nigeria. October 2019. Available online: https://www.naiis.ng/resource/NAIIS-Report-2018.pdf (accessed on 1 February 2023).
- Scobie, H.M.; Khetsuriani, N.; Efstratiou, A.; Priest, J.W. Validation of a diphtheria toxoid multiplex bead assay for serosurveys. Diagn. Microbiol. Infect. Dis. 2021, 100, 115371. [Google Scholar] [CrossRef]
- Plotkin, S.O.W.; Offit, P.; Edwards, K.M. Plotkin’s Vaccines, 7th ed.; Elsevier: Philadelphia, PA, USA, 2018. [Google Scholar]
- World Health Organization (Ed.) The Immunological Basis for Immunization Series: Module 3: Tetanus Update 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization (Ed.) The Immunological Basis for Immunization Series: Module 2: Diphtheria Update 2009; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization. Immunization Dashboard. Diphtheria Tetanus Toxoid and Pertussis (DTP)3 Vaccination Coverage: Nigeria. Available online: https://immunizationdata.who.int/pages/coverage/DTP.html?CODE=NGA&ANTIGEN=DTPCV3&YEAR= (accessed on 1 February 2023).
- Demographic Health Surveys: Nigeria. Available online: https://dhsprogram.com/search/index.cfm?_srchd=1&bydoctype=publication&bypubtype=5%2C21%2C26%2C30%2C39%2C100&bycountry=30 (accessed on 1 February 2023).
- Multiple Indicator Cluster Surveys: Nigeria. Available online: https://mics.unicef.org/surveys (accessed on 1 February 2023).
- Glatman-Freedman, A.; Nichols, K.A. The effect of social determinants on immunization programs. Hum. Vaccin. Immunother. 2012, 8, 293–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aheto, J.M.K.; Pannell, O.; Dotse-Gborgbortsi, W.; Trimner, M.K.; Tatem, A.J.; Rhoda, D.A.; Cutts, F.T.; Utazi, C.E. Multilevel analysis of predictors of multiple indicators of childhood vaccination in Nigeria. PLoS ONE 2022, 17, e0269066. [Google Scholar] [CrossRef]
- Kawakatsu, Y.; Adolph, C.; Mosser, J.F.; Baffoe, P.; Cheshi, F.; Aiga, H.; Watkins, D.; Sherr, K.H. Factors consistently associated with utilization of essential maternal and child health services in Nigeria: Analysis of the five Nigerian national household surveys (2003–2018). BMJ Open 2022, 12, e061747. [Google Scholar] [CrossRef] [PubMed]
- Utazi, C.E.; Aheto, J.M.; Wigley, A.; Tejedor-Garavito, N.; Bonnie, A.; Nnanatu, C.C.; Wagai, J.; Williams, C.; Setayesh, H.; Tatem, A.J.; et al. Mapping the distribution of zero-dose children to assess the performance of vaccine delivery strategies and their relationships with measles incidence in Nigeria. Vaccine 2023, 41, 170–181. [Google Scholar] [CrossRef]
- Malande, O.O.; Munube, D.; Afaayo, R.N.; Annet, K.; Bodo, B.; Bakainaga, A.; Ayebare, E.; Njunwamukama, S.; Mworozi, E.A.; Musyoki, A.M. Barriers to effective uptake and provision of immunization in a rural district in Uganda. PLoS ONE 2019, 14, e0212270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasudevan, L.; Baumgartner, J.N.; Moses, S.; Ngadaya, E.; Mfinanga, S.G.; Ostermann, J. Parental concerns and uptake of childhood vaccines in rural Tanzania—A mixed methods study. BMC Public Health 2020, 20, 1573. [Google Scholar] [CrossRef]
- Bwaka, A.; Bita, A.; Lingani, C.; Fernandez, K.; Durupt, A.; Mwenda, J.M.; Mihigo, R.; Djingarey, M.H.; Ronveaux, O.; Prezios, M.P. Status of the rollout of the meningococcal serogroup A conjugate vaccine in African Meningitis belt countries in 2018. J. Infect. Dis. 2019, 220, S140–S147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Epidemic meningitis control in countries of the African meningitis belt, 2017. Wkly. Epidemiol. Rec. 2018, 14, 173–184. [Google Scholar]
- Meningitis Vaccine Project. Available online: https://www.meningvax.org/developingconjugatevaccine.html (accessed on 1 February 2023).
- Basta, N.E.; Borrow, R.; Berthe, A.; Onwuchekwa, U.; Dembele, A.T.; Almond, R.; Frankland, S.; Patel, S.; Wood, D.; Nascimento, M.; et al. Higher Tetanus Toxoid Immunity 2 Years After PsA-TT Introduction in Mali. Clin. Infect. Dis. 2015, 61, S578–S585. [Google Scholar] [CrossRef] [Green Version]
- Borrow, R.; Tang, Y.; Yakubu, A.; Kulkami, P.S.; LaForce, F.M. MenAfriVac as an antitetanus vaccine. Clin. Infect. Dis. 2015, 61, S570–S577. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics. Demographic Statistics Bulletin: 2017. Available online: https://www.nigerianstat.gov.ng/download/775 (accessed on 1 February 2023).
- National Bureau of Statistics (NBS) and United Nations Children’s Fund (UNICEF). Multiple Indicator Cluster Survey 2021, Survey Findings Report; National Bureau of Statistics and United Nations Children’s Fund: Abuja, Nigeria, 2022.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number (N = 31,456) | Percentage | |
|---|---|---|
| Age group | ||
| 0–4 | 9487 | 30.2 |
| 5–9 | 12,435 | 39.5 |
| 10–14 | 9534 | 30.3 |
| Sex | ||
| Female | 15,425 | 49.0 |
| Male | 16,031 | 51.0 |
| Geopolitical zone | ||
| North central | 4634 | 14.7 |
| North east | 5045 | 16.0 |
| North west | 8784 | 27.9 |
| South south | 4387 | 13.9 |
| South east | 4000 | 12.7 |
| South west | 4606 | 14.6 |
| Location | ||
| Urban | 13,008 | 41.4 |
| Rural | 18,448 | 58.6 |
| Tetanus ≥ 0.01 IU/mL | Tetanus ≥ 0.1 IU/mL | Diphtheria ≥ 0.01 IU/mL | Diphtheria ≥ 0.1 IU/mL | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | n | Percentage (95% CI) | p-Value | n | Percentage (95% CI) | p-Value | n | Percentage (95% CI) | p Value | n | Percentage (95% CI) | p Value | |
| Overall | 31,456 | 22,727 | 70.9 (69.9–72.0) | - | 13,698 | 42.2 (41.2–43.3) | - | 26,702 | 84.3 (83.6–85.0) | - | 13,200 | 41.7 (40.9–42.5) | - |
| Age group (years) | |||||||||||||
| 0–4 | 9487 | 6663 | 68.4 (66.9–70.0) | <0.0001 | 4579 | 46.4 (44.8–48.0) | <0.0001 | 7484 | 77.2 (75.8–78.6) | <0.0001 | 3472 | 35.0 (33.7–36.3) | <0.0001 |
| 5–9 | 12,435 | 8793 | 68.5 (67.1–69.8) | 4863 | 37.0 (35.8–38.3) | 10,425 | 82.5 (81.5–83.4) | 4920 | 38.4 (37.3–39.6) | ||||
| 10–14 | 9534 | 7271 | 75.4 (74.2–76.6) | 4256 | 43.8 (42.4–45.2) | 8793 | 92.1 (91.3–92.8) | 4808 | 50.5 (49.2–51.7) | ||||
| Sex | |||||||||||||
| Female | 15,425 | 11,147 | 70.9 (69.7–72.1) | 0.9231 | 6473 | 40.6 (39.4–41.8) | <0.0001 | 12,920 | 83.0 (82.1–83.9) | <0.0001 | 5943 | 38.0 (37.1–39.0) | <0.0001 |
| Male | 16,031 | 11,580 | 71.0 (69.8–72.1) | 7225 | 43.8 (42.6–45.0) | 13,782 | 85.6 (84.7–86.3) | 7257 | 45.2 (44.1–46.2) | ||||
| Zone | |||||||||||||
| North central | 4634 | 3718 | 79.8 (77.3–82.1) | <0.0001 | 2463 | 53.5 (50.6–56.3) | <0.0001 | 4116 | 89.2 (87.9–90.4) | <0.0001 | 2134 | 46.7 (44.6–48.8) | <0.0001 |
| North east | 5045 | 3359 | 65.8 (63.2–68.2) | 1920 | 37.3 (34.9–39.9) | 4139 | 83.0 (81.5–84.5) | 1984 | 40.6 (38.6–42.6) | ||||
| North west | 8784 | 4608 | 52.8 (50.5–55.1) | 2326 | 26.6 (24.6–28.7) | 6870 | 77.1 (75.5–78.6) | 3593 | 40.3 (38.6–42.0) | ||||
| South south | 4387 | 3648 | 83.1 (81.2–84.8) | 2176 | 49.2 (47.0–51.5) | 3999 | 91.6 (90.7–92.5) | 1951 | 45.2 (43.3- 47.2) | ||||
| South east | 4000 | 3716 | 93.0 (91.8–94.0) | 2707 | 68.0 (65.8–70.1) | 3640 | 91.3 (90.2–92.2) | 1810 | 45.6 (43.8–47.5) | ||||
| South west | 4606 | 3678 | 79.6 (77.9–81.3) | 2106 | 45.7 (43.7–47.7) | 3938 | 85.5 (84.2–86.7) | 1728 | 36.6 (34.8–38.4) | ||||
| Location | |||||||||||||
| Urban | 13,008 | 9894 | 74.4 (72.7–76.1) | <0.0001 | 6247 | 46.1 (44.5–47.9) | <0.0001 | 10,893 | 83.0 (81.8–84.1) | 0.0026 | 5034 | 38.4 (37.2–39.6) | <0.0001 |
| Rural | 18,448 | 12,833 | 68.2 (66.7–69.6) | 7451 | 39.1 (37.7–40.6) | 15,809 | 85.4 (84.4–86.3) | 8166 | 44.3 (43.2–45.5) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tohme, R.A.; Scobie, H.M.; Okunromade, O.; Olaleye, T.; Shuaib, F.; Jegede, T.; Yahaya, R.; Nnaemeka, N.; Lawal, B.; Egwuenu, A.; et al. Tetanus and Diphtheria Seroprotection among Children Younger Than 15 Years in Nigeria, 2018: Who Are the Unprotected Children? Vaccines 2023, 11, 663. https://doi.org/10.3390/vaccines11030663
Tohme RA, Scobie HM, Okunromade O, Olaleye T, Shuaib F, Jegede T, Yahaya R, Nnaemeka N, Lawal B, Egwuenu A, et al. Tetanus and Diphtheria Seroprotection among Children Younger Than 15 Years in Nigeria, 2018: Who Are the Unprotected Children? Vaccines. 2023; 11(3):663. https://doi.org/10.3390/vaccines11030663
Chicago/Turabian StyleTohme, Rania A., Heather M. Scobie, Oyeladun Okunromade, Temitope Olaleye, Faisal Shuaib, Tunde Jegede, Ridwan Yahaya, Ndodo Nnaemeka, Bola Lawal, Abiodun Egwuenu, and et al. 2023. "Tetanus and Diphtheria Seroprotection among Children Younger Than 15 Years in Nigeria, 2018: Who Are the Unprotected Children?" Vaccines 11, no. 3: 663. https://doi.org/10.3390/vaccines11030663