
Equity-Informative Economic Evaluations of Vaccines: A Systematic Literature Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Data Extraction
2.3. Quality Assessment
2.4. Data Synthesis
3. Results
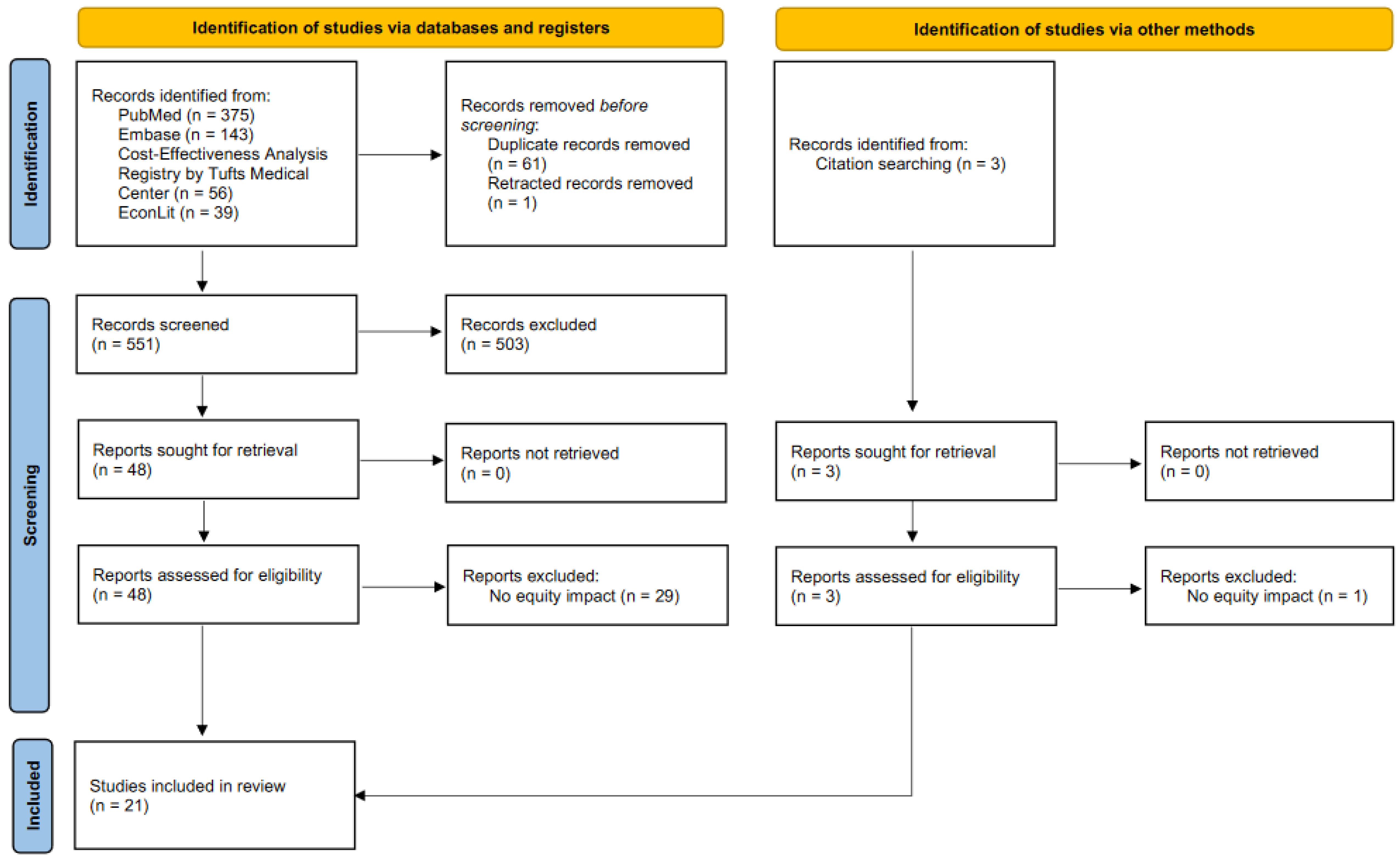
3.1. Study Selection
3.2. Study Characteristics
3.3. How Equity Has Been Incorporated into Equity-Informative Economic Evaluations of Vaccines
3.3.1. Overall Methods
3.3.2. Existing Inequities across Equity-Relevant Subpopulations
3.3.3. Vaccination Programs Evaluated
3.3.4. Health and Non-Health Benefits of Vaccination Programs
3.4. Summary of Study Findings on Cost-Effectiveness and Health Equity Impact
3.5. Reporting Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization; UNICEF. Progress and Challenges with Achieving Universal Immunization Coverage 2021 WHO/UNICEF Estimates Geneva: World Health Organization. 2022. Available online: https://cdn.who.int/media/docs/default-source/immunization/wuenic-progress-and-challenges-15-july-2022.pdf?sfvrsn=b5eb9141_7&download=true (accessed on 3 February 2023).
- World Health Organization. Immunization Agenda 2030: A Global Strategy to Leave No One Behind Geneva: World Health Organization. 2020. Available online: https://cdn.who.int/media/docs/default-source/immunization/strategy/ia2030/ia2030-draft-4-wha_b8850379-1fce-4847-bfd1-5d2c9d9e32f8.pdf?sfvrsn=5389656e_69&download=true (accessed on 3 February 2023).
- World Health Organization. WHO Guide for Standardization of Economic Evaluations of Immunization Programmes; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Kristensen, F.B.; Mäkelä, M.; Neikter, S.A.; Rehnqvist, N.; Håheim, L.L.; Mørland, B.; Milne, R.; Nielsen, C.P.; Busse, R.; Lee-Robin, S.H.; et al. European network for Health Technology Assessment, EUnetHTA: Planning, development, and implementation of a sustainable European network for Health Technology Assessment. Int. J. Technol. Assess. Health Care 2009, 25, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Ward, T.; Mujica-Mota, R.E.; Spencer, A.E.; Medina-Lara, A. Incorporating Equity Concerns in Cost-Effectiveness Analyses: A Systematic Literature Review. Pharmacoeconomics 2022, 40, 45–64. [Google Scholar] [CrossRef] [PubMed]
- Assebe, L.F.; Kwete, X.J.; Wang, D.; Liu, L.; Norheim, O.F.; Jbaily, A.; Verguet, S.; Johansson, K.A.; Tolla, M.T. Health gains and financial risk protection afforded by public financing of selected malaria interventions in Ethiopia: An extended cost-effectiveness analysis. Malar. J. 2020, 19, 41. [Google Scholar] [CrossRef] [PubMed]
- Driessen, J.; Olson, Z.D.; Jamison, D.T.; Verguet, S. Comparing the health and social protection effects of measles vaccination strategies in Ethiopia: An extended cost-effectiveness analysis. Soc. Sci. Med. 2015, 139, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, K.A.; Memirie, S.T.; Pecenka, C.; Jamison, D.T.; Verguet, S. Health Gains and Financial Protection from Pneumococcal Vaccination and Pneumonia Treatment in Ethiopia: Results from an Extended Cost-Effectiveness Analysis. PLoS ONE 2015, 10, e0142691. [Google Scholar] [CrossRef]
- Levin, C.E.; Sharma, M.; Olson, Z.; Verguet, S.; Shi, J.F.; Wang, S.M.; Qiao, Y.L.; Jamison, D.T.; Kim, J.J. An extended cost-effectiveness analysis of publicly financed HPV vaccination to prevent cervical cancer in China. Vaccine 2015, 33, 2830–2841. [Google Scholar] [CrossRef] [Green Version]
- Loganathan, T.; Jit, M.; Hutubessy, R.; Ng, C.W.; Lee, W.S.; Verguet, S. Rotavirus vaccines contribute towards universal health coverage in a mixed public-private healthcare system. Trop. Med. Int. Health 2016, 21, 1458–1467. [Google Scholar] [CrossRef] [Green Version]
- Pecenka, C.J.; Johansson, K.A.; Memirie, S.T.; Jamison, D.T.; Verguet, S. Health gains and financial risk protection: An extended cost-effectiveness analysis of treatment and prevention of diarrhoea in Ethiopia. BMJ Open 2015, 5, e006402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portnoy, A.; Sweet, S.; Desalegn, D.; Memirie, S.T.; Kim, J.J.; Verguet, S. Health gains and financial protection from human papillomavirus vaccination in Ethiopia: Findings from a modelling study. Health Policy Plan. 2021, 36, 891–899. [Google Scholar] [CrossRef]
- Verguet, S.; Murphy, S.; Anderson, B.; Johansson, K.A.; Glass, R.; Rheingans, R. Public finance of rotavirus vaccination in India and Ethiopia: An extended cost-effectiveness analysis. Vaccine 2013, 31, 4902–4910. [Google Scholar] [CrossRef]
- Cookson, R.; Mirelman, A.J.; Griffin, S.; Asaria, M.; Dawkins, B.; Norheim, O.F.; Verguet, S.; Culyer, A.J. Using cost-effectiveness analysis to address health equity concerns. Value Health 2017, 20, 206–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avanceña, A.L.; Prosser, L.A. Examining Equity Effects of Health Interventions in Cost-Effectiveness Analysis: A Systematic Review. Value Health 2021, 24, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Dukhanin, V.; Searle, A.; Zwerling, A.; Dowdy, D.W.; Taylor, H.A.; Merritt, M.W. Integrating social justice concerns into economic evaluation for healthcare and public health: A systematic review. Soc. Sci. Med. 2018, 198, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Johri, M.; Norheim, O.F. Can cost-effectiveness analysis integrate concerns for equity? Systematic review. Int. J. Technol. Assess. Health Care 2012, 28, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Lal, A.; Moodie, M.; Peeters, A.; Carter, R. Inclusion of equity in economic analyses of public health policies: Systematic review and future directions. Aust. N Z J. Public Health 2018, 42, 207–213. [Google Scholar] [CrossRef]
- Yang, F.; Katumba, K.R.; Griffin, S. Incorporating health inequality impact into economic evaluation in low-and middle-income countries: A systematic review. Expert Rev. Pharm. Outcomes Res. 2022, 22, 17–25. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ Clin. Res. Ed. 2021, 372, n71. [Google Scholar]
- Husereau, D.; Drummond, M.; Augustovski, F.; de Bekker-Grob, E.; Briggs, A.H.; Carswell, C.; Caulley, L.; Chaiyakunapruk, N.; Greenberg, D.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 explanation and elaboration: A report of the ISPOR CHEERS II good practices task force. Value Health 2022, 25, 10–31. [Google Scholar] [CrossRef]
- Welch, V.A.; Petkovic, J.; Jull, J.; Hartling, L.; Klassen, T.; Kristjansson, E.; Pardo, J.P.; Petticrew, M.; Stott, D.J.; Thomson, D.; et al. Equity and specific populations. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 433–449. [Google Scholar]
- Anderson, I.V.J.D.; Pecenka, C.J.; Bagamian, K.H.; Rheingans, R.D. Effects of geographic and economic heterogeneity on the burden of rotavirus diarrhea and the impact and cost-effectiveness of vaccination in Nigeria. PLoS ONE 2020, 15, e0232941. [Google Scholar] [CrossRef]
- Bell, G.J.; Loop, M.; Topazian, H.M.; Hudgens, M.; Mvalo, T.; Juliano, J.J.; Kamthunzi, P.; Tegha, G.; Mofolo, I.; Hoffman, I.; et al. Case reduction and cost-effectiveness of the RTS,S/AS01 malaria vaccine alongside bed nets in Lilongwe, Malawi. Vaccine 2020, 38, 4079–4087. [Google Scholar] [CrossRef]
- Blakely, T.; Kvizhinadze, G.; Karvonen, T.; Pearson, A.L.; Smith, M.; Wilson, N. Cost-effectiveness and equity impacts of three HPV vaccination programmes for school-aged girls in New Zealand. Vaccine 2014, 32, 2645–2656. [Google Scholar] [CrossRef] [PubMed]
- Goldie, S.J.; Daniels, N. Model-based analyses to compare health and economic outcomes of cancer control: Inclusion of disparities. J. Natl. Cancer Inst. 2011, 103, 1373–1386. [Google Scholar] [CrossRef] [PubMed]
- Rheingans, R.; Atherly, D.; Anderson, J. Distributional impact of rotavirus vaccination in 25 GAVI countries: Estimating disparities in benefits and cost-effectiveness. Vaccine 2012, 30, A15–A23. [Google Scholar] [CrossRef] [PubMed]
- Rheingans, R.; Anderson, I.V.J.D.; Anderson, B.; Chakraborty, P.; Atherly, D.; Pindolia, D. Estimated impact and cost-effectiveness of rotavirus vaccination in India: Effects of geographic and economic disparities. Vaccine 2014, 32, A140–A150. [Google Scholar] [CrossRef] [Green Version]
- Rheingans, R.; Anderson, I.V.J.D.; Bagamian, K.H.; Pecenka, C.J. Effects of geographic and economic heterogeneity on rotavirus diarrhea burden and vaccination impact and cost-effectiveness in the Lao People’s Democratic Republic. Vaccine 2018, 36, 7868–7877. [Google Scholar] [CrossRef]
- Rheingans, R.; Anderson, I.V.J.D.; Bagamian, K.H.; Laytner, L.A.; Pecenka, C.J.; Gilani, S.S.; Ahmed, M. Effects of geographic and economic heterogeneity on the burden of rotavirus diarrhea and the impact and cost-effectiveness of vaccination in Pakistan. Vaccine 2018, 36, 7780–7789. [Google Scholar] [CrossRef]
- Wateska, A.R.; Nowalk, M.P.; Lin, C.J.; Harrison, L.H.; Schaffner, W.; Zimmerman, R.K.; Smith, K. Cost-effectiveness of adult pneumococcal vaccination policies in underserved minorities aged 50-64 years compared to the US general population. Vaccine 2019, 37, 2026–2033. [Google Scholar] [CrossRef]
- Wateska, A.R.; Nowalk, M.P.; Lin, C.J.; Harrison, L.H.; Schaffner, W.; Zimmerman, R.K.; Smith, K.J. Cost-effectiveness of revised US pneumococcal vaccination recommendations in underserved minority adults < 65-years-old. Vaccine 2022, 40, 7312–7320. [Google Scholar]
- Dawkins, B.R.; Mirelman, A.J.; Asaria, M.; Johansson, K.A.; Cookson, R.A. Distributional cost-effectiveness analysis in low- and middle-income countries: Illustrative example of rotavirus vaccination in Ethiopia. Health Policy Plan. 2018, 33, 456–463. [Google Scholar] [CrossRef]
- Urueña, A.; Pippo, T.; Betelu, M.S.; Virgilio, F.; Hernández, L.; Giglio, N.; Gentile, Á.; Diosque, M.; Vizzotti, C. Cost-effectiveness analysis of rotavirus vaccination in Argentina. Vaccine 2015, 33, A126–A134. [Google Scholar] [CrossRef]
- Chang, A.Y.; Riumallo-Herl, C.; Perales, N.A.; Clark, S.; Clark, A.; Constenla, D.; Garske, T.; Jackson, M.L.; Jean, K.; Jit, M.; et al. The equity impact vaccines may have on averting deaths and medical impoverishment in developing countries. Health Aff. 2018, 37, 316–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verguet, S.; Woldemariam, A.T.; Durrett, W.N.; Norheim, O.F.; Kruk, M.E. Is the sustainable development goal target for financial risk protection in health realistic? BMJ Glob. Health 2017, 2, e000216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verguet, S.; Kim, J.J.; Jamison, D.T. Extended cost-effectiveness analysis for health policy assessment: A tutorial. Pharmacoeconomics 2016, 34, 913–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asaria, M.; Griffin, S.; Cookson, R. Distributional cost-effectiveness analysis: A tutorial. Med. Decis. Mak. 2016, 36, 8–19. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Health Equity Impact Analysis (n = 11) | Health Equity Impact Analysis with Financial Risk Protection (n = 9) | Health Equity Impact Analysis with Equity Weighting (n = 1) | Total (n = 21) | |
|---|---|---|---|---|
| Region | ||||
| Sub-Saharan Africa | 2 | 5 | 1 | 8 (38%) |
| East Asia and Pacific | 2 | 2 | - | 4 (19%) |
| North America | 3 | - | - | 3 (14%) |
| South Asia | 2 | - | - | 2 (10%) |
| Latin America and Caribbean | 1 | - | - | 1 (5%) |
| Multiple countries | 1 | 2 | - | 3 (14%) |
| Income economy | ||||
| High-income | 4 | - | - | 4 (19%) |
| Low- and Middle-income | 7 | 9 | 1 | 17 (81%) |
| Antigen * | ||||
| Rotavirus | 6 | 4 | 1 | 11 (52%) |
| Human papilloma virus | 2 | 3 | - | 5 (24%) |
| Streptococcus pneumoniae | 2 | 2 | - | 4 (19%) |
| Malaria † | 1 | 1 | - | 2 (10%) |
| Measles | - | 2 | - | 2 (10%) |
| Hepatitis B | - | 1 | - | 1 (5%) |
| Hemophilus influenzae type b | - | 1 | - | 1 (5%) |
| Yellow fever | - | 1 | - | 1 (5%) |
| Rubella | - | 1 | - | 1 (5%) |
| Neisseria meningitidis serogroup A | - | 1 | - | 1 (5%) |
| Japanese encephalitis | - | 1 | - | 1 (5%) |
| Health Equity Impact Analysis (n = 11) | Health Equity Impact Analysis with Financial Risk Protection (n = 9) | Health Equity Impact Analysis with Equity Weighting (n = 1) | Total (n = 21) | |
|---|---|---|---|---|
| Equity-relevant subgroups | ||||
| Socioeconomic status | 1 | 9 | 1 | 11 (52%) |
| Race/Ethnicity | 3 | - | - | 3 (14%) |
| Place of residence | 2 | - | - | 2 (10%) |
| Combination of characteristics | 5 | - | - | 5 (24%) |
| Existing inequities * | ||||
| Mortality | 10 | 6 | 1 | 17 (81%) |
| Vaccination coverage | 6 | 5 | 1 | 12 (57%) |
| Disease incidence/prevalence | 6 | 4 | 1 | 11 (52%) |
| Financial risk | - | 9 | - | 9 (43%) |
| Intervention(s) vs. Comparator(s) | ||||
| Introduction vs. No vaccination | 5 | 7 | - | 12 (57%) |
| Introduction vs. Introduction with improving vaccination coverage vs. No vaccination | 3 | - | - | 3 (14%) |
| Improving vaccination coverage vs. Status quo | 1 | 2 | 1 | 4 (19%) |
| Improving vaccination coverage vs. Status quo vs. No vaccination | 2 | - | - | 2 (10%) |
| Perspective of analysis † | ||||
| Societal (Health system and household) | 1 | 8 | - | 9 (43%) |
| Health system | 10 | - | 1 | 11 (52%) |
| Household | - | 1 | - | 1 (5%) |
| Costs * | ||||
| Direct medical costs | 11 | 9 | 1 | 21 (100%) |
| Direct non-medical costs | 1 | 8 | - | 9 (43%) |
| Indirect costs | 1 | 3 | - | 4 (19%) |
| Measurement of health benefits * | ||||
| Outcomes averted | ||||
| Deaths averted | 8 | 7 | 1 | 16 (76%) |
| DALYs averted | 6 | - | - | 6 (29%) |
| Cases averted | 4 | 1 | - | 5 (24%) |
| Hospitalizations and outpatient/clinic visits averted | 1 | 1 | - | 2 (10%) |
| Outcomes gained | ||||
| QALYs gained | 3 | - | - | 3 (14%) |
| HALYs gained | - | - | 1 | 1 (5%) |
| Years of life saved | 1 | - | - | 1 (5%) |
| Measurement of financial risk protection * | ||||
| Household OOP expenditures averted | - | 8 ‡ | - | 8 (38%) |
| Catastrophic health expenditures averted | - | 3 | - | 3 (14%) |
| Money-metric value of insurance (risk premium) | - | 2 | - | 2 (10%) |
| Impoverishments averted | - | 2 | - | 2 (10%) |
| Model type | ||||
| Dynamic | - | - | - | 0 (0%) |
| Static | 11 | 9 | 1 | 21 (100%) |
| Herd protection | ||||
| Included in base-case analysis | 1 | - | - | 1 (5%) |
| Included in scenario analysis | 2 | 2 § | - | 4 (19%) |
| Not included | 8 | 7 | 1 | 16 (76%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 World Health Organization; Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patikorn, C.; Cho, J.-Y.; Lambach, P.; Hutubessy, R.; Chaiyakunapruk, N. Equity-Informative Economic Evaluations of Vaccines: A Systematic Literature Review. Vaccines 2023, 11, 622. https://doi.org/10.3390/vaccines11030622
Patikorn C, Cho J-Y, Lambach P, Hutubessy R, Chaiyakunapruk N. Equity-Informative Economic Evaluations of Vaccines: A Systematic Literature Review. Vaccines. 2023; 11(3):622. https://doi.org/10.3390/vaccines11030622
Chicago/Turabian StylePatikorn, Chanthawat, Jeong-Yeon Cho, Philipp Lambach, Raymond Hutubessy, and Nathorn Chaiyakunapruk. 2023. "Equity-Informative Economic Evaluations of Vaccines: A Systematic Literature Review" Vaccines 11, no. 3: 622. https://doi.org/10.3390/vaccines11030622