
A Case Series and Literature Review of Telogen Effluvium and Alopecia Universalis after the Administration of a Heterologous COVID-19 Vaccine Scheme


Abstract
:1. Introduction
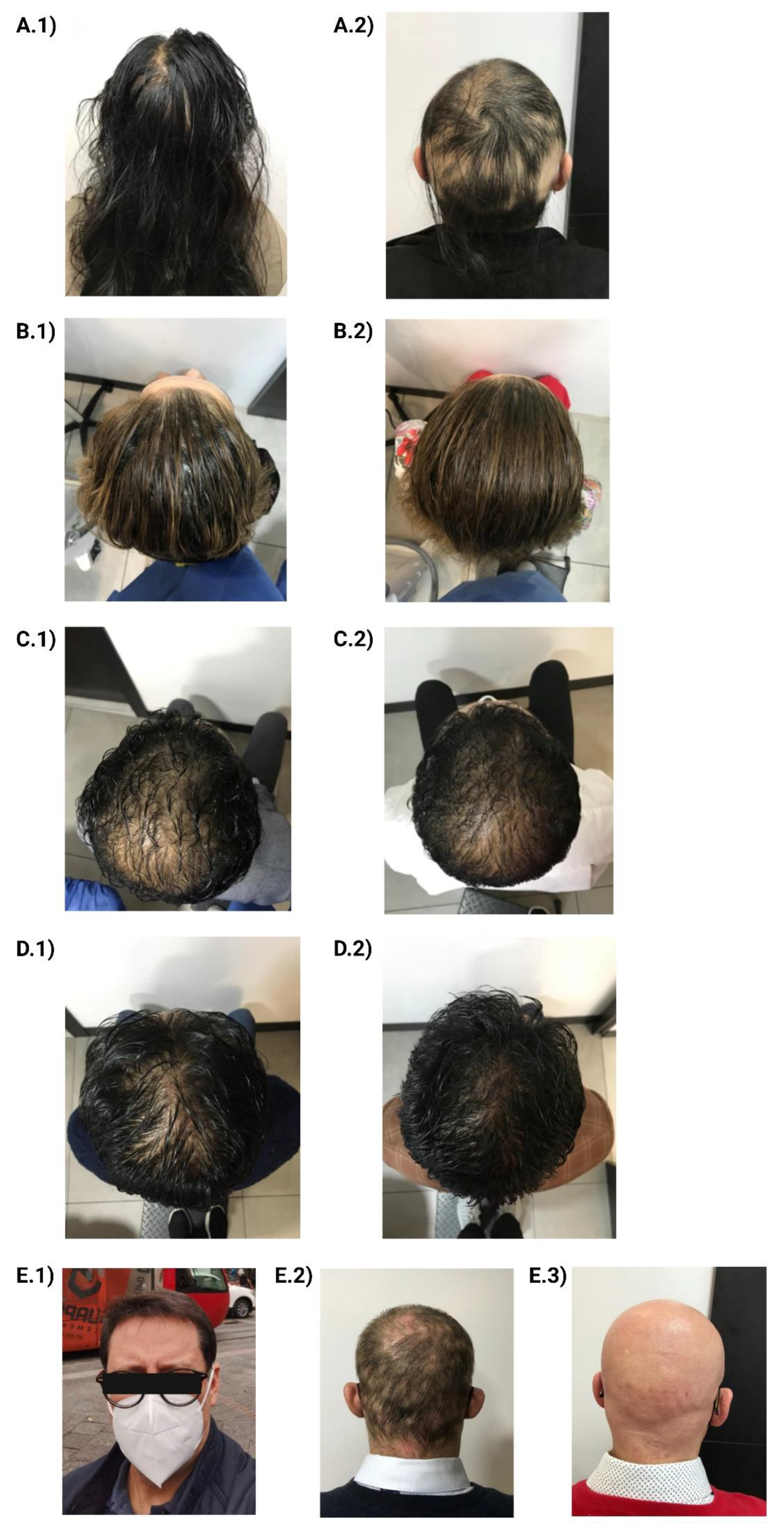
2. Cases Presentation
2.1. Case 1
2.2. Case 2
2.3. Case 3
2.4. Case 4
2.5. Case 5
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Drummond, M.; Chevat, C.; Lothgren, M. Do We Fully Understand the Economic Value of Vaccines? Vaccine 2007, 25, 5945–5957. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Prado, E.; Simbaña-Rivera, K.; Gómez- Barreno, L.; Rubio-Neira, M.; Guaman, L.P.; Kyriakidis, N.C.; Muslin, C.; Jaramillo, A.M.G.; Barba-Ostria, C.; Cevallos-Robalino, D.; et al. Clinical, Molecular, and Epidemiological Characterization of the SARS-CoV-2 Virus and the Coronavirus Disease 2019 (COVID-19), a Comprehensive Literature Review. Diagn. Microbiol. Infect. Dis. 2020, 98, 115094. [Google Scholar] [CrossRef] [PubMed]
- Krause, P.R.; Gruber, M.F. Emergency Use Authorization of COVID Vaccines—Safety and Efficacy Follow-up Considerations. N. Engl. J. Med. 2020, 383, e107. [Google Scholar] [CrossRef] [PubMed]
- Tatar, M.; Faraji, M.R.; Montazeri Shoorekchali, J.; Pagán, J.A.; Wilson, F.A. The Role of Good Governance in the Race for Global Vaccination during the COVID-19 Pandemic. Sci. Rep. 2021, 11, 22440. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.M.; Romero, J.R.; Bell, B.P. Postapproval Vaccine Safety Surveillance for COVID-19 Vaccines in the US. JAMA 2020, 324, 1937–1938. [Google Scholar] [CrossRef]
- Troiano, G.; Nardi, A. Vaccine Hesitancy in the Era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef]
- Kaur, R.J.; Dutta, S.; Bhardwaj, P.; Charan, J.; Dhingra, S.; Mitra, P.; Singh, K.; Yadav, D.; Sharma, P.; Misra, S. Adverse Events Reported From COVID-19 Vaccine Trials: A Systematic Review. Indian J. Clin. Biochem. 2021, 36, 427–439. [Google Scholar] [CrossRef]
- Ortiz-Prado, E.; Izquierdo-Condoy, J.S.; Fernandez-Naranjo, R.; Simbaña-Rivera, K.; Vásconez-González, J.; Naranjo, E.P.L.; Cordovez, S.; Coronel, B.; Delgado-Moreira, K.; Jimbo-Sotomayor, R. A Comparative Analysis of a Self-Reported Adverse Events Analysis after Receiving One of the Available SARS-CoV-2 Vaccine Schemes in Ecuador. Vaccines 2022, 10, 1047. [Google Scholar] [CrossRef]
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 Vaccines: Comparison of Biological, Pharmacological Characteristics and Adverse Effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [CrossRef]
- Shimabukuro, T. Allergic Reactions Including Anaphylaxis after Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine—United States, December 14-23, 2020. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2021, 21, 1332–1337. [Google Scholar] [CrossRef]
- Essam, R.; Ehab, R.; Al-Razzaz, R.; Khater, M.W.; Moustafa, E.A. Alopecia Areata after ChAdOx1 NCoV-19 Vaccine (Oxford/AstraZeneca): A Potential Triggering Factor? J. Cosmet. Dermatol. 2021, 20, 3727–3729. [Google Scholar] [CrossRef]
- Rossi, A.; Magri, F.; Michelini, S.; Caro, G.; Di Fraia, M.; Fortuna, M.C.; Pellacani, G.; Carlesimo, M. Recurrence of Alopecia Areata after COVID-19 Vaccination: A Report of Three Cases in Italy. J. Cosmet. Dermatol. 2021, 20, 3753–3757. [Google Scholar] [CrossRef] [PubMed]
- Strazzulla, L.C.; Wang, E.H.C.; Avila, L.; Sicco, K.L.; Brinster, N.; Christiano, A.M.; Shapiro, J. Alopecia Areata: Disease Characteristics, Clinical Evaluation, and New Perspectives on Pathogenesis. J. Am. Acad. Dermatol. 2018, 78, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Vañó-Galván, S.; Hermosa-Gelbard, Á.; Sánchez-Neila, N.; Miguel-Gómez, L.; Saceda-Corralo, D.; Rodrigues-Barata, R.; Ma, D.-L.; Jaén, P. Pulse Corticosteroid Therapy with Oral Dexamethasone for the Treatment of Adult Alopecia Totalis and Universalis. J. Am. Acad. Dermatol. 2016, 74, 1005–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Kim, B.J.; Lee, Y.B.; Lee, W.-S. Hair Regrowth Outcomes of Contact Immunotherapy for Patients With Alopecia Areata: A Systematic Review and Meta-Analysis. JAMA Dermatol. 2018, 154, 1145–1151. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Lee, H.; Lee, C.H.; Lee, W.-S. Comorbidities in Alopecia Areata: A Systematic Review and Meta-Analysis. J. Am. Acad. Dermatol. 2019, 80, 466–477.e16. [Google Scholar] [CrossRef]
- VAERS Vaccine Adverse Events Reporting System—Data. Available online: https://vaers.hhs.gov/data.html (accessed on 20 November 2022).
- UK Government Coronavirus (COVID-19) Vaccines Adverse Reactions. Available online: https://www.gov.uk/government/publications/coronaviruscovid-19-vaccine-adverse-reactions (accessed on 20 November 2022).
- Ganjei, Z.; Yazdan Panah, M.; Rahmati, R.; Zari Meidani, F.; Mosavi, A. COVID-19 Vaccination and Alopecia Areata: A Case Report and Literature Review. Clin. Case Rep. 2022, 10, e6039. [Google Scholar] [CrossRef]
- Scollan, M.E.; Breneman, A.; Kinariwalla, N.; Soliman, Y.; Youssef, S.; Bordone, L.A.; Gallitano, S.M. Alopecia Areata after SARS-CoV-2 Vaccination. JAAD Case Rep. 2021, 20, 1–5. [Google Scholar] [CrossRef]
- Chen, C.-H.; Chen, Y.-Y.; Lan, C.-C.E. Intractable Alopecia Areata Following the Second Dose of COVID-19 Vaccination: Report of Two Cases. Dermatol. Ther. 2022, 35, e15689. [Google Scholar] [CrossRef]
- Gallo, G.; Mastorino, L.; Tonella, L.; Ribero, S.; Quaglino, P. Alopecia Areata after COVID-19 Vaccination. Clin. Exp. Vaccine Res. 2022, 11, 129–132. [Google Scholar] [CrossRef]
- Lin, D.A.; Zaken, G.A.; Sanz, J.; Miteva, M. Induction of Alopecia Areata after COVID-19 Vaccination: A Case Report in the United States. J. Egypt. Women’s Dermatol. Soc. 2022, 19, 199. [Google Scholar] [CrossRef]
- Wise, R.P.; Kiminyo, K.P.; Salive, M.E. Hair Loss after Routine Immunizations. JAMA 1997, 278, 1176–1178. [Google Scholar] [CrossRef]
- Thompson, J.M.; Park, M.K.; Qureshi, A.A.; Cho, E. Race and Alopecia Areata amongst US Women. J. Investig. Dermatol. Symp. Proc. 2018, 19, S47–S50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández, M.; Alarcón, G.S.; Calvo-Alén, J.; Andrade, R.; McGwin, G.; Vilá, L.M.; Reveille, J.D.; LUMINA Study Group. A Multiethnic, Multicenter Cohort of Patients with Systemic Lupus Erythematosus (SLE) as a Model for the Study of Ethnic Disparities in SLE. Arthritis Rheum. 2007, 57, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Ghoreishi, M.; Martinka, M.; Dutz, J.P. Type 1 Interferon Signature in the Scalp Lesions of Alopecia Areata. Br. J. Dermatol. 2010, 163, 57–62. [Google Scholar] [CrossRef]
- Goh, C. Hepatitis C Treatment and Alopecia Totalis. J. Investig. Dermatol. Symp. Proc. 2013, 16, S59–S60. [Google Scholar] [CrossRef] [Green Version]
- Notarte, K.I.; Catahay, J.A.; Velasco, J.V.; Pastrana, A.; Ver, A.T.; Pangilinan, F.C.; Peligro, P.J.; Casimiro, M.; Guerrero, J.J.; Gellaco, M.M.L.; et al. Impact of COVID-19 Vaccination on the Risk of Developing Long-COVID and on Existing Long-COVID Symptoms: A Systematic Review. eClinicalMedicine 2022, 53, 101624. [Google Scholar] [CrossRef]
- Izquierdo-Condoy, J.S.; Fernandez-Naranjo, R.; Vasconez-González, E.; Cordovez, S.; Tello-De-la-Torre, A.; Paz, C.; Delgado-Moreira, K.; Carrington, S.; Viscor, G.; Ortiz-Prado, E. Long COVID at Different Altitudes: A Countrywide Epidemiological Analysis. Int. J. Environ. Res. Public. Health 2022, 19, 14673. [Google Scholar] [CrossRef]
- Vásconez-González, J.; Fernandez-Naranjo, R.; Izquierdo-Condoy, J.S.; Delgado-Moreira, K.; Cordovez, S.; Tello-De-la-Torre, A.; Paz, C.; Castillo, D.; Izquierdo-Condoy, N.; Carrington, S.J.; et al. Comparative Analysis of Long-Term Self-Reported COVID-19 Symptoms among Pregnant Women. J. Infect. Public Health 2023, 16, 430–440. [Google Scholar] [CrossRef]


{kind=link}
| N. | Sex | Age (Years) | Ethnicity | Family History | Personal History | Vaccine Received | Symptoms | Post-Vaccination Onset Time | Therapy | Evolution |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 27 | Mestizo | No | AU, Polycystic ovary | Pfizer, SinoVac, and AstraZeneca (Booster) | Alopecia universalis | 8 days | Mesotherapy and pulses of dexamethasone and Clobetasol propionate 0.5% topical | 25% |
| 2 | F | 51 | Mestizo | Hypothyroidism (grandmother) | AH | Pfizer, SinoVac, and AstraZeneca (Booster) | Telogen effluvium | 3 days | Mesotherapy | 80% |
| 3 | M | 34 | Mestizo | DM 2, AH (grandmother) | COVID-19 | Pfizer, SinoVac, and AstraZeneca (Booster) | Telogen effluvium | 10 days | Mesotherapy | 50% |
| 4 | M | 40 | Mestizo | No | COVID-19 | Pfizer, SinoVac, and AstraZeneca (Booster) | Telogen effluvium | 7 days | Mesotherapy | 90% |
| 5 | M | 59 | Mestizo | No | AH, COVID-19 | Pfizer, SinoVac, and AstraZeneca (Booster) | Alopecia universalis | 17 days | Mesotherapy and pulses of dexamethasone and Clobetasol propionate 0.5% topical | 15% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández Arroyo, J.; Izquierdo-Condoy, J.S.; Ortiz-Prado, E. A Case Series and Literature Review of Telogen Effluvium and Alopecia Universalis after the Administration of a Heterologous COVID-19 Vaccine Scheme. Vaccines 2023, 11, 444. https://doi.org/10.3390/vaccines11020444
Hernández Arroyo J, Izquierdo-Condoy JS, Ortiz-Prado E. A Case Series and Literature Review of Telogen Effluvium and Alopecia Universalis after the Administration of a Heterologous COVID-19 Vaccine Scheme. Vaccines. 2023; 11(2):444. https://doi.org/10.3390/vaccines11020444
Chicago/Turabian StyleHernández Arroyo, Jenny, Juan S. Izquierdo-Condoy, and Esteban Ortiz-Prado. 2023. "A Case Series and Literature Review of Telogen Effluvium and Alopecia Universalis after the Administration of a Heterologous COVID-19 Vaccine Scheme" Vaccines 11, no. 2: 444. https://doi.org/10.3390/vaccines11020444