
Immunogenicity and SARS-CoV-2 Infection following the Fourth BNT162b2 Booster Dose among Health Care Workers

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Serology Assays
2.2. Statistical Analysis
3. Results
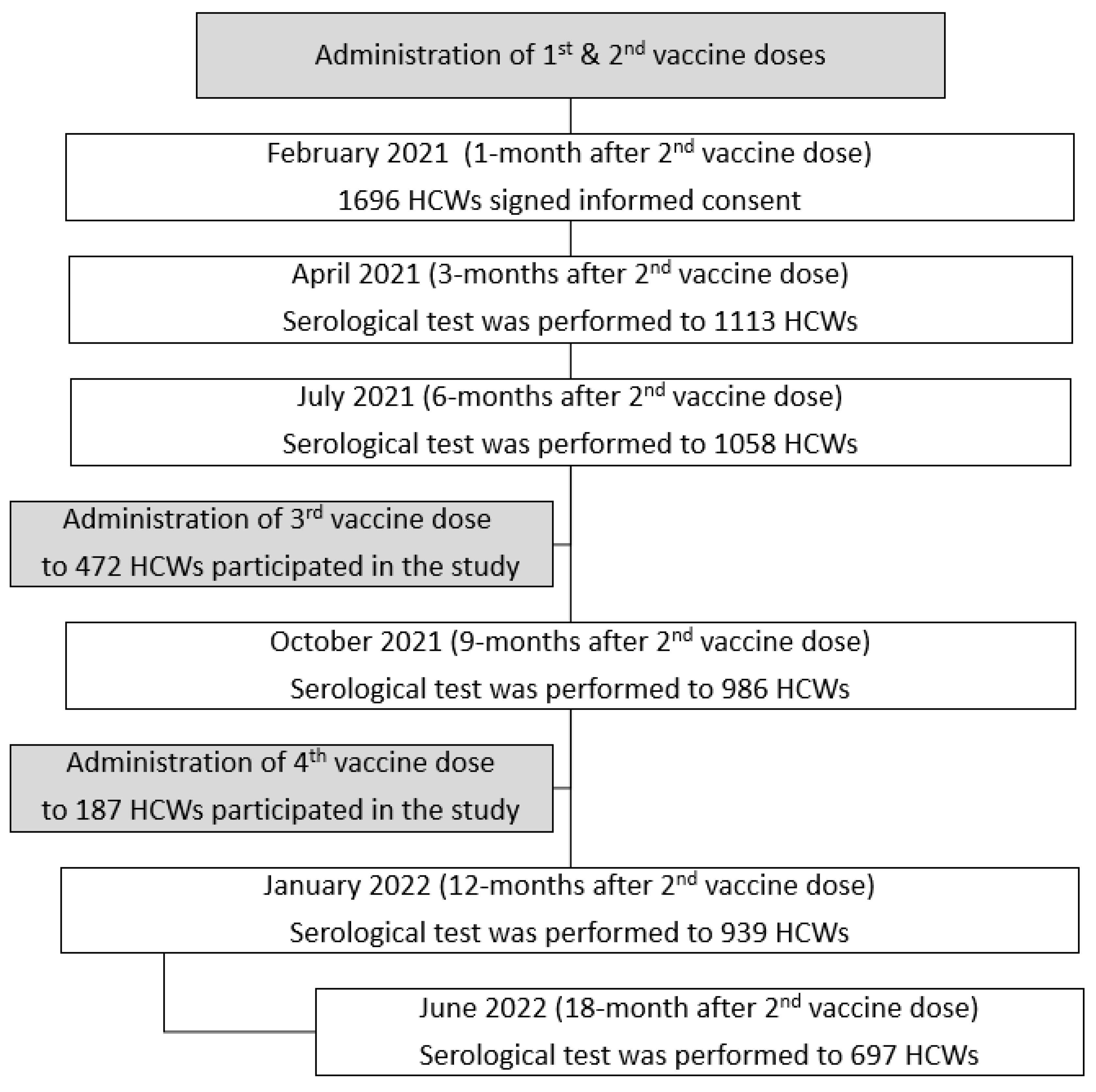
3.1. Description of the Study Population
3.2. SARS-CoV-2 Infection among Participants
3.3. Multivariate Analysis of the Independent Association between the Number of Vaccine Doses and the Risk of SARS-CoV-2
3.4. ROC Analysis
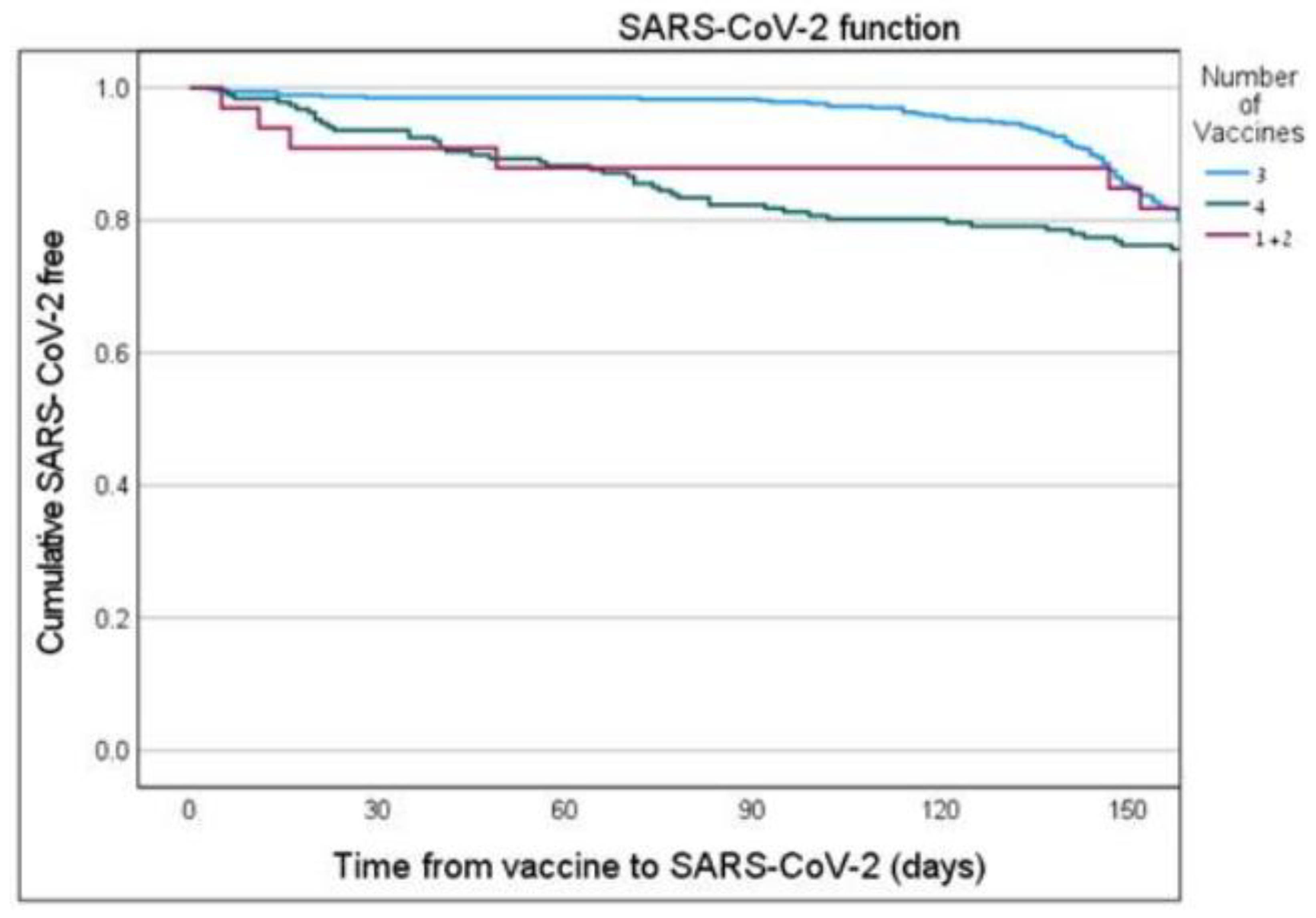
3.5. Kaplan–MeierSARS-CoV-2 Free “Survival” Analysis
3.6. Perception of Severity of Illness
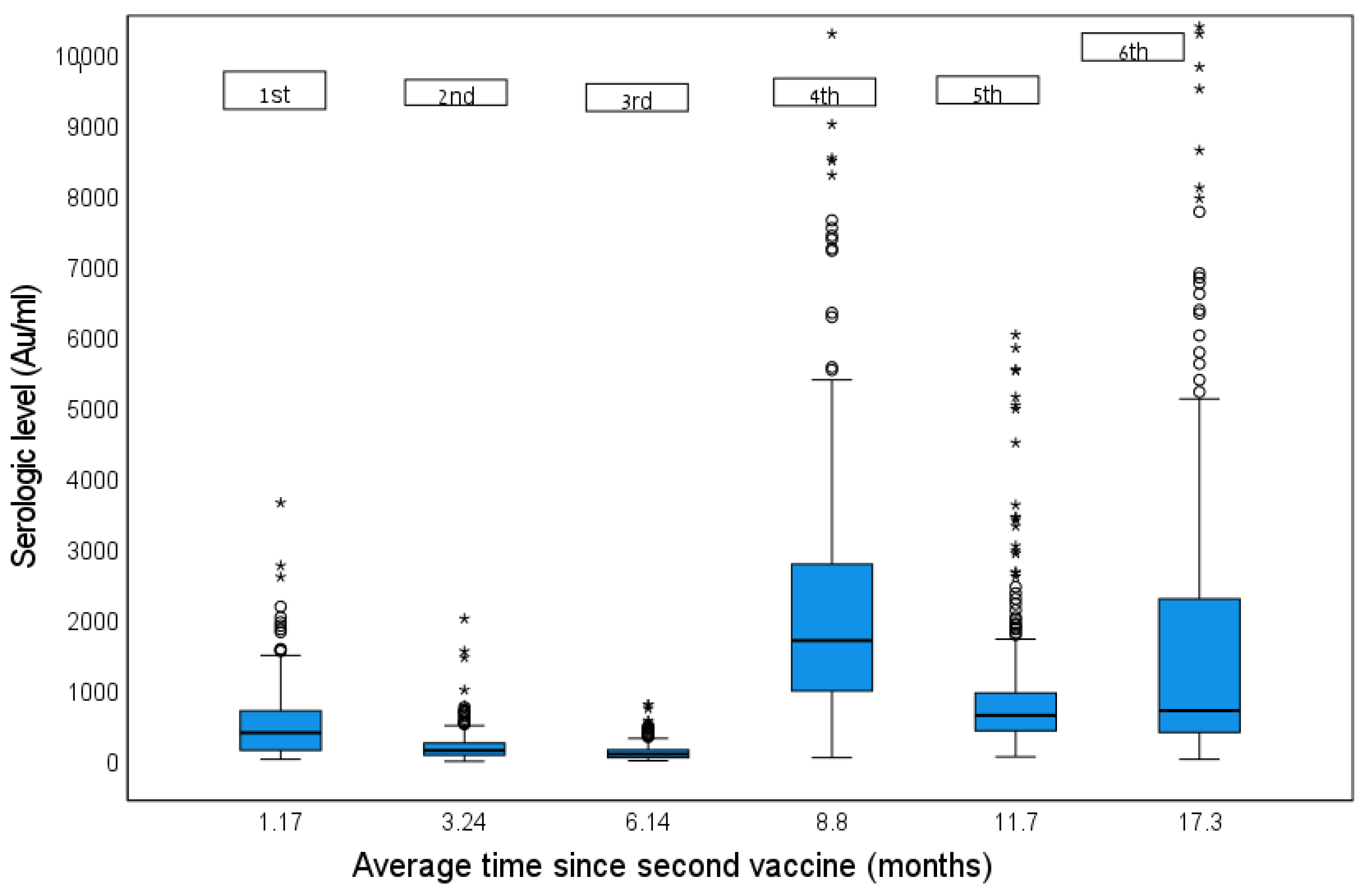
3.7. Serology Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kliker, L.; Zuckerman, N.; Atari, N.; Barda, N.; Gilboa, M.; Nemet, I.; Abd Elkader, B.; Fratty, I.S.; Jaber, H.; Mendelson, E.; et al. COVID-19 vaccination and BA.1 breakthrough infection induce neutralising antibodies which are less efficient against BA.4 and BA.5 Omicron variants, Israel, March to June 2022. Eurosurveillance 2022, 27, 2200559. [Google Scholar] [CrossRef]
- Patalon, T.; Saciuk, Y.; Peretz, A.; Perez, G.; Lurie, Y.; Maor, Y.; Gazit, S. Waning effectiveness of the third dose of the BNT162b2 mRNA COVID-19 vaccine. Nat. Commun. 2022, 13, 3203. [Google Scholar] [CrossRef] [PubMed]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Ferdinands, J.M.; Rao, S.; Dixon, B.E.; Mitchell, P.K.; DeSilva, M.B.; Irving, S.A.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.J.; et al. Waning of vaccine effectiveness against moderate and severe covid-19 among adults in the US from the VISION network: Test negative, case-control study. BMJ 2022, 379, e072141. [Google Scholar] [CrossRef] [PubMed]
- Chalkias, S.; Harper, C.; Vrbicky, K.; Walsh, S.R.; Essink, B.; Brosz, A.; McGhee, N.; Tomassini, J.E.; Chen, X.; Chang, Y.; et al. A Bivalent Omicron-Containing Booster Vaccine against Covid-19. N. Engl. J. Med. 2022, 387, 1279–1291. [Google Scholar] [CrossRef]
- Magen, O.; Waxman, J.G.; Makov-Assif, M.; Vered, R.; Dicker, D.; Hernán, M.A.; Lipsitch, M.; Reis, B.Y.; Balicer, R.D.; Dagan, N. Fourth Dose of BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2022, 386, 1603–1614. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of Covid-19 mRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Amir, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection by a Fourth Dose of BNT162b2 against Omicron in Israel. N. Engl. J. Med. 2022, 386, 1712–1720. [Google Scholar] [CrossRef]
- Cohen, M.J.; Oster, Y.; Moses, A.E.; Spitzer, A.; Benenson, S.; Israeli-Hospitals 4th Vaccine Working Group. Association of Receiving a Fourth Dose of the BNT162b Vaccine with SARS-CoV-2 Infection among Health Care Workers in Israel. JAMA Netw. Open. 2022, 5, e2224657. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Hein, S.; Mhedhbi, I.; Zahn, T.; Sabino, C.; Benz, N.I.; Husria, Y.; Renelt, P.M.; Braun, F.; Oberle, D.; Maier, T.J.; et al. Quantitative and Qualitative Difference in Antibody Response against Omicron and Ancestral SARS-CoV-2 after Third and Fourth Vaccination. Vaccines 2022, 10, 796. [Google Scholar] [CrossRef] [PubMed]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Canetti, M.; Gilboa, M.; Asraf, K.; Indenboim, V.; Weiss-Ottolenghi, Y.; Amit, S.; Zubli, D.; Doolman, R.; Mendelson, E.; et al. The Association Between Pre-Booster Vaccination Antibody Levels and the Risk of SARS-CoV-2 Infection. Clin. Infect. Dis. 2022, ciac886. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, S.; Tkatch, R.; Kraemer, S.; Fellows, A.; McGinn, M.; Schaeffer, J.; Yeh, C.S. COVID-19 Era Social Isolation among Older Adults. Geriatrics 2021, 6, 52. [Google Scholar] [CrossRef]
- Kim, L.; Garg, S.; O’Halloran, A.; Whitaker, M.; Pham, H.; Anderson, E.J.; Armistead, I.; Bennett, N.M.; Billing, L.; Como-Sabetti, K.; et al. Risk Factors for Intensive Care Unit Admission and In-hospital Mortality among Hospitalized Adults Identified through the US Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET). Clin. Infect. Dis. 2021, 72, e206–e214. [Google Scholar] [CrossRef]
- Canetti, M.; Barda, N.; Gilboa, M.; Indenbaum, V.; Asraf, K.; Gonen, T.; Weiss-Ottolenghi, Y.; Amit, S.; Doolman, R.; Mendelson, E.; et al. Six-Month Follow-up after a Fourth BNT162b2 Vaccine Dose. N. Engl. J. Med. 2022, 387, 2092–2094. [Google Scholar] [CrossRef]
- Hussein, K.; Shachor-Meyouhas, Y.; Dabaja-Younis, H.; Szwarcwort-Cohen, M.; Tarabeia, J.; Weissman, A.; Mekel, M.; Hyams, G.; Halberthal, M. COVID-19: Healthcare Workers May Be at Greater Risk Outside Their Work Environment-A Retrospective Observational Study. Rambam Maimonides Med. J. 2022, 13, e0011. [Google Scholar] [CrossRef]
- Brodin, P. Immune determinants of COVID-19 disease presentation and severity. Nat. Med. 2021, 27, 28–33. [Google Scholar] [CrossRef]
- Shachor-Meyouhas, Y.; Hussein, K.; Szwarcwort-Cohen, M.; Weissman, A.; Mekel, M.; Dabaja-Younis, H.; Hyams, G.; Horowitz, N.A.; Kaplan, M.; Halberthal, M. Single BNT162b2 vaccine dose produces seroconversion in under 60 s cohort. Vaccine 2021, 39, 6902–6906. [Google Scholar] [CrossRef]
- Altarawneh, H.N.; Chemaitelly, H.; Ayoub, H.H.; Tang, P.; Hasan, M.R.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Coyle, P.; Al-Kanaani, Z.; et al. Effects of Previous Infection and Vaccination on Symptomatic Omicron Infections. N. Engl. J. Med. 2022, 387, 21–34. [Google Scholar] [CrossRef]
- Shachor-Meyouhas, Y.; Hussein, K.; Dabaja-Younis, H.; Szwarcwort-Cohen, M.; Almog, R.; Weissman, A.; Mekel, M.; Hyams, G.; Horowitz, N.A.; Gepstein, V.; et al. Immunogenicity trends 1 and 3 months after second BNT162B2 vaccination among healthcare workers in Israel. Clin. Microbiol. Infect. 2022, 28, e1–e450. [Google Scholar] [CrossRef] [PubMed]
- North, C.M.; Barczak, A.; Goldstein, R.H.; Healy, B.C.; Finkelstein, D.M.; Ding, D.D.; Kim, A.; Boucau, J.; Shaw, B.; Gilbert, R.F.; et al. Determining the Incidence of Asymptomatic SARS-CoV-2 Among Early Recipients of COVID-19 Vaccines (DISCOVER-COVID-19): A Prospective Cohort Study of Healthcare Workers Before, During and After Vaccination. Clin. Infect. Dis. 2022, 74, 1275–1278. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Xu, Y.; Sun, C.; Wang, X.; Guo, Y.; Qiu, S.; Ma, K. A systematic review of asymptomatic infections with COVID-19. J. Microbiol. Immunol. Infect. 2021, 54, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Heymann, D.L.; Teo, Y.Y.; Garcia, P.J. Diagnostics for COVID-19: Moving from pandemic response to control. Lancet 2022, 399, 757–768. [Google Scholar] [CrossRef]
- Lustig, Y.; Sapir, E.; Regev-Yochay, G.; Cohen, C.; Fluss, R.; Olmer, L.; Indenbaum, V.; Mandelboim, M.; Doolman, R.; Amit, S.; et al. BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: A prospective, single-centre, longitudinal cohort study in health-care workers. Lancet Respir. Med. 2021, 9, 999–1009. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | OR | 95% CI | p |
|---|---|---|---|
| Sex | |||
| Male | 1 | ||
| Female | 1.99 | 1.30–3.05 | 0.002 |
| Age (years) | |||
| 60+ | 1 | ||
| 50–60 | 1.30 | 0.80–2.10 | NS |
| 40–50 | 1.77 | 1.07–2.92 | 0.026 |
| <40 | 1.58 | 0.89–2.81 | NS |
| Smoking | |||
| Smoker | 1 | ||
| Non-smoker | 0.62 | 0.34–1.14 | NS |
| Chronic lung disease | |||
| No | 1 | ||
| Yes | 2.99 | 1.05–8.56 | 0.041 |
| Number of vaccines | |||
| Vaccine 1 and 2 | 1 | ||
| Vaccine 3 | 0.18 | 0.08–0.41 | <0.0001 |
| Vaccine 4 | 0.05 | 0.02–0.12 | <0.0001 |
| Serology #6 | 1 * | 1 | <0.0001 |
| SARS-CoV-2 Negative (N = 374, 54.0%) | SARS CoV-2 Positive ≥ 6 m (N = 105, 15.0%) | SARS CoV-2 Positive < 6 m (N = 213, 31.0%) | P | |
|---|---|---|---|---|
| Age (years) | 52.9 ± 11.4 | 49.8 ± 10.03 | 50.5 ± 10.14 | P1 = 0.032 P2 = 0.034 P3 = NS |
| Age group (years) <40 40–50 50–60 60+ | 53 (14%) 94 (25%) 123 (33%) 104 (28%) | 18 (17%) 35 (34%) 38 (36%) 14 (13%) | 34 (16%) 65 (30%) 65 (31%) 49 (23%) | P = 0.081 |
| Sex Male Female | 109 (29%) 265 (71%) | 24 (23%) 81 (77%) | 31 (15%) 182 (85%) | P < 0.001 P1 = NS P2 < 0.001 P3 = NS |
| BMI | 26.0 ± 4.2 | 25.5 ± 4.7 | 26.04 ± 5.12 | P = NS |
| Heart disease | 21 (5.6%) | 9 (8.6%) | 12 (5.6%) | P = NS |
| Chronic lung disease | 7 (1.9%) | 10 (9.5%) | 5 (2.3%) | P < 0.001 P1,3 = 0.008 P2 = NS |
| Active oncologic disease | 1 (0.3%) | 1 (0.95%) | 1 (0.47%) | NA |
| Autoimmune disease | 27 (7.2%) | 6 (5.7%) | 17 (8.0%) | P = NS |
| Intestinal disease | 5 (1.3%) | 3 (2.9%) | 3 (1.4%) | P = NS |
| Hypothyroidism | 46 (12.3%) | 6 (5.7%) | 25 (11.7%) | P = NS |
| Chronic renal failure | 2 (0.5%) | 0 (0%) | 1 (0.47%) | NA |
| Treatment with dialyzes | 0 (0%) | 0 (0%) | 1 (0.47%) | NA |
| Smoking | 42 (11.2%) | 12 (11.4%) | 12 (5.6%) | P = 0.066 |
| Immunosuppressive therapy | 8 (2.1%) | 2 (1.9%) | 5 (2.3%) | P = NS |
| *Sixth serology level | 702 [385–2200] | 2220 [988–5105] | 2510 [1220–4755] | P1,2 < 0.001 P3 = NS |
| N = 697 | |
|---|---|
| Mean age in years ± sd (range) | 51.7 ± 10.8 (19.7–86.6) |
| Age groups Till 30 30–40 40–50 50–60 60+ | 16 (2%) 89 (13%) 194 (28%) 229 (33%) 169 (24%) |
| Gender Male Female | 164 (23.5%) 533 (76.5%) |
| Mean serology level ± sd (median) | 2694.8 ± 3369.8 (1370) |
| Mean BMI ± sd (range) | 25.9 ± 4.59 (17.2–49.0) |
| BMI categories ≤24.9 25–30 ≥30 | 252 (45.5%) 212 (38%) 91 (16.5%) |
| Heart disease | 42 (6%) |
| Chronic lung disease | 22 (3%) |
| Active oncologic disease | 21 (3%) |
| Autoimmune disease | 50 (7.2%) |
| Intestinal disease | 11 (1.6%) |
| Hypothyroidism | 77 (11.0%) |
| Chronic renal failure disease | 3 (0.4%) |
| Treatment with dialyzes | 1 (0.1%) |
| Smoking | 67 (9.6%) |
| Receiving immunosuppressive treatments | 15 (2.2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shachor-Meyouhas, Y.; Dabaja-Younis, H.; Magid, A.; Leiba, R.; Szwarcwort-Cohen, M.; Almog, R.; Mekel, M.; Weissman, A.; Hyams, G.; Gepstein, V.; et al. Immunogenicity and SARS-CoV-2 Infection following the Fourth BNT162b2 Booster Dose among Health Care Workers. Vaccines 2023, 11, 283. https://doi.org/10.3390/vaccines11020283
Shachor-Meyouhas Y, Dabaja-Younis H, Magid A, Leiba R, Szwarcwort-Cohen M, Almog R, Mekel M, Weissman A, Hyams G, Gepstein V, et al. Immunogenicity and SARS-CoV-2 Infection following the Fourth BNT162b2 Booster Dose among Health Care Workers. Vaccines. 2023; 11(2):283. https://doi.org/10.3390/vaccines11020283
Chicago/Turabian StyleShachor-Meyouhas, Yael, Halima Dabaja-Younis, Avi Magid, Ronit Leiba, Moran Szwarcwort-Cohen, Ronit Almog, Michal Mekel, Avi Weissman, Gila Hyams, Vardit Gepstein, and et al. 2023. "Immunogenicity and SARS-CoV-2 Infection following the Fourth BNT162b2 Booster Dose among Health Care Workers" Vaccines 11, no. 2: 283. https://doi.org/10.3390/vaccines11020283