
Death and Disability Reported with Cases of Vaccine Anaphylaxis Stratified by Administration Setting: An Analysis of the Vaccine Adverse Event Reporting System from 2017 to 2022
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
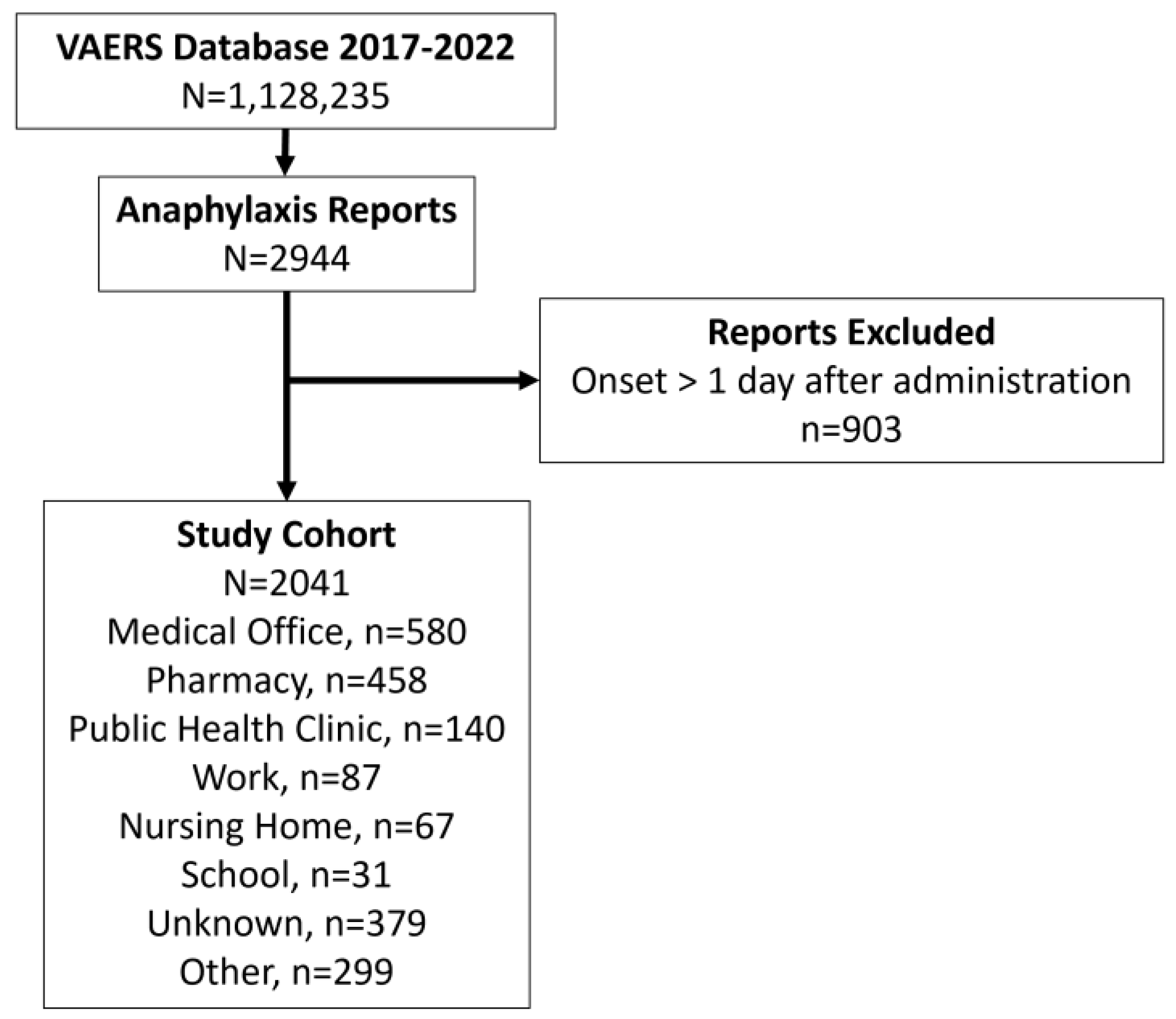
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Descriptive Data
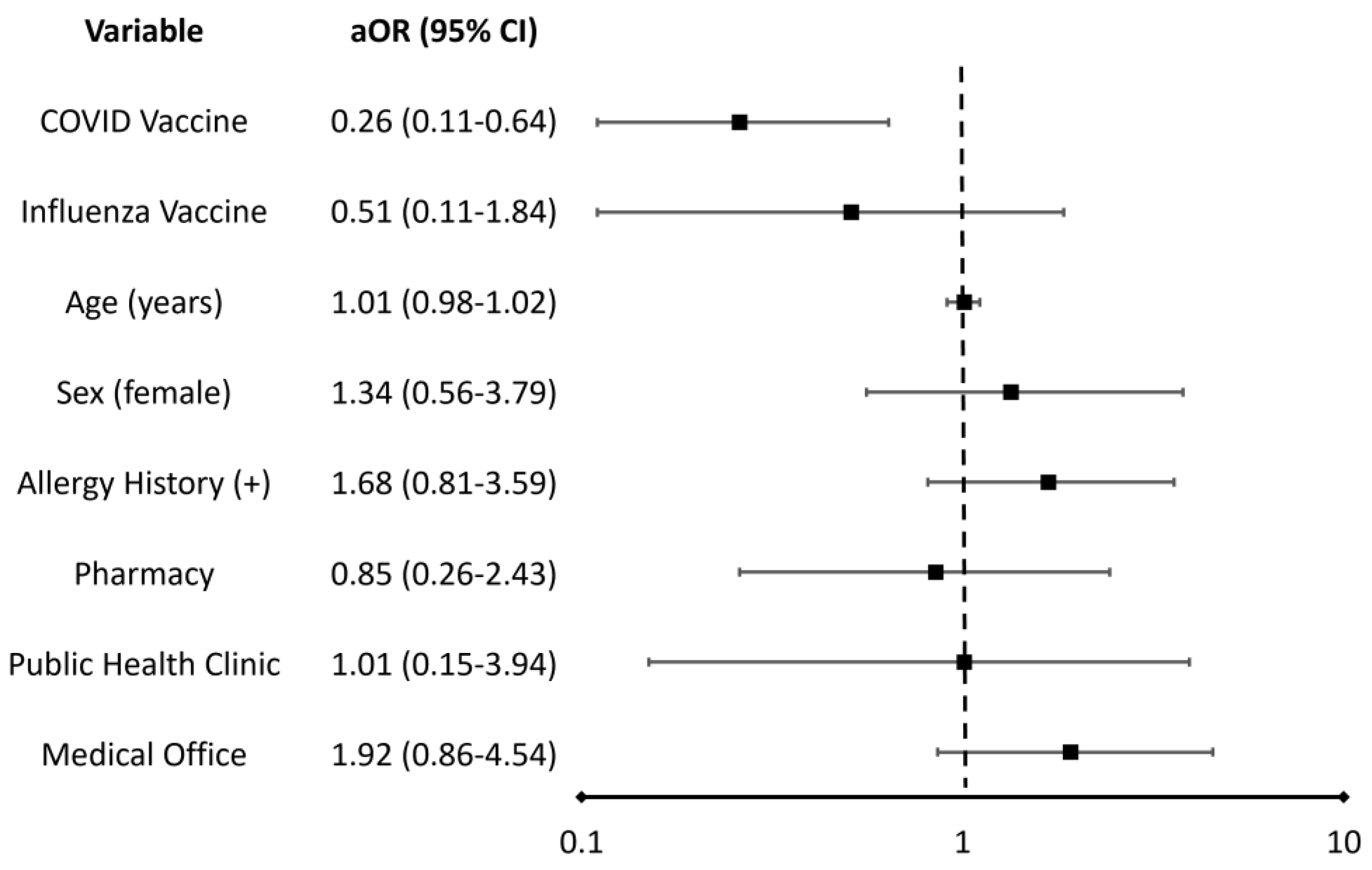
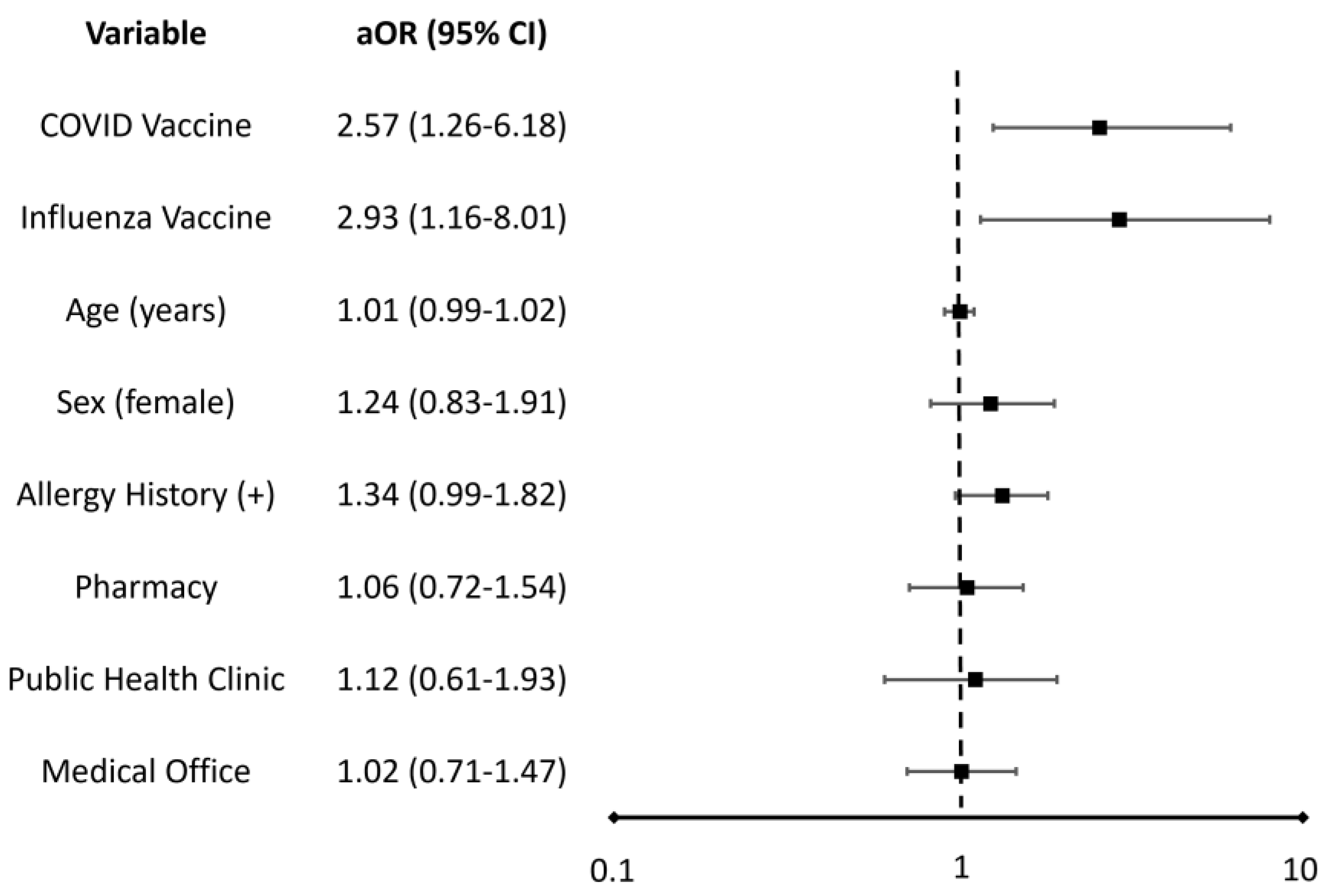
3.2. Outcome Data and Main Results
4. Discussion
4.1. Interpretation of Results
4.2. Limitations and Generalizability
4.3. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sampath, V.; Rabinowitz, G.; Shah, M.; Jain, S.; Diamant, Z.; Jesenak, M.; Rabin, R.; Vieths, S.; Agache, I.; Akdis, M.; et al. Vaccines and allergic reactions: The past, the current COVID-19 pandemic, and future perspectives. Allergy 2021, 76, 1640–1660. [Google Scholar] [CrossRef] [PubMed]
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Scobie, H.M.; Johnson, A.G.; Suthar, A.B.; Severson, R.; Alden, N.B.; Balter, S.; Bertolino, D.; Blythe, D.; Brady, S.; Cadwell, B.; et al. Monitoring Incidence of COVID-19 Cases, Hospitalizations, and Deaths by Vaccination Status–13 U.S.; Jurisdictions, April 4–July 17, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- McNeil, M.M.; DeStefano, F. Vaccine-associated hypersensitivity. J. Allergy Clin. Immunol. 2018, 141, 463–472. [Google Scholar] [PubMed] [Green Version]
- CDC COVID-19 Response Team; Food and Drug Administration. Allergic Reactions Including Anaphylaxis after Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine-United States, December 14–23, 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 46–51. [Google Scholar] [CrossRef]
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for Adverse Events after COVID-19 mRNA Vaccination. JAMA 2021, 326, 1390–1399. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Anastassopoulou, C.; Hatziantoniou, S.; Poland, G.A.; Tsakris, A. Anaphylaxis rates associated with COVID-19 vaccines are comparable to those of other vaccines. Vaccine 2022, 40, 183–186. [Google Scholar] [CrossRef]
- Kim, M.A.; Lee, Y.W.; Kim, S.R.; Kim, J.-H.; Min, T.K.; Park, H.-S.; Shin, M.; Ye, Y.-M.; Lee, S.; Lee, J.; et al. COVID-19 Vaccine-associated Anaphylaxis and Allergic Reactions: Consensus Statements of the KAAACI Urticaria/Angioedema/Anaphylaxis Working Group. Allergy Asthma Immunol. Res. 2021, 13, 526–544. [Google Scholar]
- Shaker, M.S.; Wallace, D.V.; Golden, D.B.; Oppenheimer, J.; Bernstein, J.A.; Campbell, R.L.; Dinakar, C.; Ellis, A.; Greenhawt, M.; Khan, D.A.; et al. Anaphylaxis-a 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) analysis. J. Allergy Clin. Immunol. 2020, 145, 1082–1123. [Google Scholar]
- Centers for Disease Control and Prevention. Vaccines and Immunizations. Preparing for the Potential Management of Anaphylaxis. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/managing-anaphylaxis.html (accessed on 16 October 2022).
- Office of the Assistant Secretary of Health. Guidance for PREP Act Coverage for Qualified Pharmacy Technicians and State-Authorized Pharmacy Interns for Childhood Vaccines, COVID-19 Vaccines, and COVID-19 Testing. HHS. Available online: https://www.hhs.gov/sites/default/files/prep-act-guidance.pdf (accessed on 16 October 2022).
- Isenor, J.E.; Edwards, N.T.; Alia, T.A.; Slayter, K.L.; MacDougall, D.M.; McNeil, S.A.; Bowles, S.K. Impact of pharmacists as immunizers on vaccination rates: A systematic review and meta-analysis. Vaccine 2016, 34, 5708–5723. [Google Scholar] [CrossRef]
- Le, L.M.; Veettil, S.K.; Donaldson, D.; Kategeaw, W.; Hutubessy, R.; Lambach, P.; Chaiyakunapruk, N. The impact of pharmacist involvement on immunization uptake and other outcomes: An updated systematic review and meta-analysis. J. Am. Pharm. Assoc. 2022, 62, 1499–1513. [Google Scholar] [CrossRef] [PubMed]
- Eid, D.; Osborne, J.; Borowicz, B. Moving the Needle: A 50-State and District of Columbia Landscape Review of Laws Regarding Pharmacy Technician Vaccine Administration. Pharmacy 2019, 7, 168. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, S.; Sullivan, D. Assessing Pharmacists’ Attitudes and Barriers Involved with Immunizations. Innov Pharm. 2014, 5, 1–5. [Google Scholar] [CrossRef]
- Westrick, S.C.; Patterson, B.J.; Kader, M.S.; Rashid, S.; Buck, P.O.; Rothholz, M.C. National survey of pharmacy-based immunization services. Vaccine 2018, 36, 5657–5664. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Vaccine Adverse Event Reporting System (VAERS). Available online: https://vaers.hhs.gov/about.html (accessed on 16 October 2022).
- Medical Dictionary for Regulatory Activities. Available online: https://www.meddra.org/ (accessed on 16 October 2022).
- American College of Allergy, Asthma and Immunology. Anaphylaxis: Causes, Symptoms and Treatment. Available online: https://acaai.org/allergies/symptoms/anaphylaxis/ (accessed on 16 October 2022).
- GraphPad Prism, Version 9.3.0 for Windows; GraphPad Software: San Diego, CA, USA, 2021. Available online: www.graphpad.com(accessed on 11 November 2022).
- Luxi, N.; Giovanazzi, A.; Arcolaci, A.; Bonadonna, P.; Crivellaro, M.A.; Cutroneo, P.M.; Ferrajolo, C.; Furci, F.; Guidolin, L.; Moretti, U.; et al. Allergic Reactions to COVID-19 Vaccines: Risk Factors, Frequency, Mechanisms and Management. BioDrugs 2022, 36, 443–458. [Google Scholar] [CrossRef] [PubMed]
- Alhumaid, S.; Al Mutair, A.; Al Alawi, Z.; Rabaan, A.A.; Tirupathi, R.; Alomari, M.A.; Alshakhes, A.S.; Alshawi, A.M.; Ahmed, G.Y.; Almusabeh, H.M.; et al. Anaphylactic and nonanaphylactic reactions to SARS-CoV-2 vaccines: A systematic review and meta-analysis. Allergy Asthma Clin. Immunol. 2021, 17, 109. [Google Scholar] [CrossRef]
- Turner, P.J.; Ansotegui, I.J.; Campbell, D.E.; Cardona, V.; Ebisawa, M.; El-Gamal, Y.; Fineman, S.; Geller, M.; Gonzalez-Estrada, A.; Greenberger, P.A.; et al. COVID-19 vaccine-associated anaphylaxis: A statement of the World Allergy Organization Anaphylaxis Committee. World Allergy Organ. J. 2021, 14, 100517. [Google Scholar] [CrossRef]
- Shimabukuro, T.; Nair, N. Allergic Reactions Including Anaphylaxis after Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine. JAMA 2021, 325, 780–781. [Google Scholar] [CrossRef]
- Risma, K.A.; Edwards, K.M.; Hummell, D.S.; Little, F.F.; Norton, A.E.; Stallings, A.; Wood, R.A.; Milner, J. Potential mechanisms of anaphylaxis to COVID-19 mRNA vaccines. J. Allergy Clin. Immunol. 2021, 147, 2075–2082. [Google Scholar] [CrossRef]
- Webb, L.M.; Lieberman, P. Anaphylaxis: A review of 601 cases. Ann. Allergy Asthma Immunol. 2006, 97, 39–43. [Google Scholar] [CrossRef]
- Ross, M.P.; Ferguson, M.; Street, D.; Klontz, K.; Schroeder, T.; Luccioli, S. Analysis of food-allergic and anaphylactic events in the National Electronic Injury Surveillance System. J. Allergy Clin. Immunol. 2008, 121, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Poulos, L.M.; Waters, A.M.; Correll, P.K.; Loblay, R.H.; Marks, G.B. Trends in hospitalizations for anaphylaxis, angioedema, and urticaria in Australia, 1993–1994 to 2004–2005. J. Allergy Clin. Immunol. 2007, 120, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Hox, V.; Desai, A.; Bandara, G.; Gilfillan, A.M.; Metcalfe, D.D.; Olivera, A. Estrogen increases the severity of anaphylaxis in female mice through enhanced endothelial nitric oxide synthase expression and nitric oxide production. J. Allergy Clin. Immunol. 2015, 135, 729–736.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvati, L.; Vitiello, G.; Parronchi, P. Gender differences in anaphylaxis. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 417–424. [Google Scholar] [CrossRef]
- Johann-Liang, R.; Josephs, S.; Dreskin, S.C. Analysis of anaphylaxis cases after vaccination: 10-year review from the National Vaccine Injury Compensation Program. Ann. Allergy Asthma Immunol. 2011, 106, 440–443. [Google Scholar] [CrossRef]
- Miller, E.R.; McNeil, M.M.; Moro, P.L.; Duffy, J.; Su, J.R. The reporting sensitivity of the Vaccine Adverse Event Reporting System (VAERS) for anaphylaxis and for Guillain-Barré syndrome. Vaccine 2020, 38, 7458–7463. [Google Scholar] [CrossRef]
- Rizk, J.G.; Forthal, D.N.; Kalantar-Zadeh, K.; Mehra, M.R.; Lavie, C.J.; Rizk, Y.; Pfeiffer, J.P.; Lewin, J.C. Expanded Access Programs, compassionate drug use, and Emergency Use Authorizations during the COVID-19 pandemic. Drug Discov. Today 2021, 26, 593–603. [Google Scholar] [CrossRef]
- Grabenstein, J.D. Essential services: Quantifying the contributions of America’s pharmacists in COVID-19 clinical interventions. J. Am. Pharm. Assoc. 2022, 62, 1929–1945. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Influenza (Flu). Influenza Vaccinations Administered in Pharmacies and Physician Medical Offices, Adults, United States. Available online: https://www.cdc.gov/flu/fluvaxview/dashboard/vaccination-administered.html (accessed on 19 December 2022).
- Paudyal, V.; Fialová, D.; Henman, M.C.; Hazen, A.; Okuyan, B.; Lutters, M.; Cadogan, C.; Da Costa, F.A.; Galfrascoli, E.; Pudritz, Y.M.; et al. Pharmacists’ involvement in COVID-19 vaccination across Europe: A situational analysis of current practice and policy. Int. J. Clin. Pharm. 2021, 43, 1139–1148. [Google Scholar] [CrossRef]
- Bohlke, K.; Davis, R.L.; Marcy, S.M.; Braun, M.M.; DeStefano, F.; Black, S.B.; Mullooly, J.P.; Thompson, R.S. Risk of anaphylaxis after vaccination of children and adolescents. Pediatrics 2003, 112, 815–820. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, W.P.; Hauben, M. Data mining for signals in spontaneous reporting databases: Proceed with caution. Pharmacoepidemiol Drug Saf. 2007, 16, 359–365. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Medical Office (n = 580) | Pharmacy (n = 458) | Public Health Clinic (n = 140) | All Other * (n = 863) | Total (n = 2041) |
|---|---|---|---|---|---|
| Sex (female) | 471 (81.2%) | 356 (77.7%) | 116 (82.9%) | 687 (79.6%) | 1630 (79.9%) |
| Age (years) | 40.4 ± 19.2 | 43.2 ± 16.4 | 43.9 ± 17.6 | 45.4 ± 16.5 | 43.3 ± 17.5 |
| Age (<18 years) | 80 (13.8%) | 30 (6.6%) | 12 (8.6%) | 31 (3.6%) | 153 (7.5%) |
| Allergy History (+) | 373 (64.3%) | 163 (35.6%) | 95 (67.9%) | 297 (34.4%) | 928 (45.5%) |
| Vaccine Type: Coronavirus Influenza Tetanus Zoster Other | 461 (79.5%) 38 (6.6%) 30 (5.2%) 2 (0.3%) 49 (8.4%) | 400 (87.3%) 32 (6.9%) 1 (0.2%) 17 (3.7%) 8 (1.7%) | 126 (90.0%) 3 (2.1%) 5 (3.6%) 1 (0.7%) 5 (3.6%) | 751 (87.1%) 48 (5.6%) 8 (0.9%) 12 (1.4%) 44 (5.1%) | 1738 (85.2%) 121 (5.9%) 44 (2.2%) 32 (1.6%) 106 (5.2%) |
| Hospitalization | 76 (13.1%) | 24 (5.2%) | 13 (9.3%) | 106 (12.3%) | 219 (10.7%) |
| Death & Disability | 18 (3.1%) | 5 (1.1%) | 2 (1.4%) | 10 (1.2%) | 35 (1.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klosko, R.C.; Lynch, S.E.; Cabral, D.L.; Nagaraju, K.; Johnston, Y.A.; Steinberg, J.D.; McCall, K.L. Death and Disability Reported with Cases of Vaccine Anaphylaxis Stratified by Administration Setting: An Analysis of the Vaccine Adverse Event Reporting System from 2017 to 2022. Vaccines 2023, 11, 276. https://doi.org/10.3390/vaccines11020276
Klosko RC, Lynch SE, Cabral DL, Nagaraju K, Johnston YA, Steinberg JD, McCall KL. Death and Disability Reported with Cases of Vaccine Anaphylaxis Stratified by Administration Setting: An Analysis of the Vaccine Adverse Event Reporting System from 2017 to 2022. Vaccines. 2023; 11(2):276. https://doi.org/10.3390/vaccines11020276
Chicago/Turabian StyleKlosko, Rachel C., Sarah E. Lynch, Danielle L. Cabral, Kanneboyina Nagaraju, Yvonne A. Johnston, Joshua D. Steinberg, and Kenneth L. McCall. 2023. "Death and Disability Reported with Cases of Vaccine Anaphylaxis Stratified by Administration Setting: An Analysis of the Vaccine Adverse Event Reporting System from 2017 to 2022" Vaccines 11, no. 2: 276. https://doi.org/10.3390/vaccines11020276