
Skin Testing and Basophil Activation Testing Is Useful for Assessing Immediate Reactions to Polyethylene Glycol-Containing Vaccines

Abstract
:1. Introduction
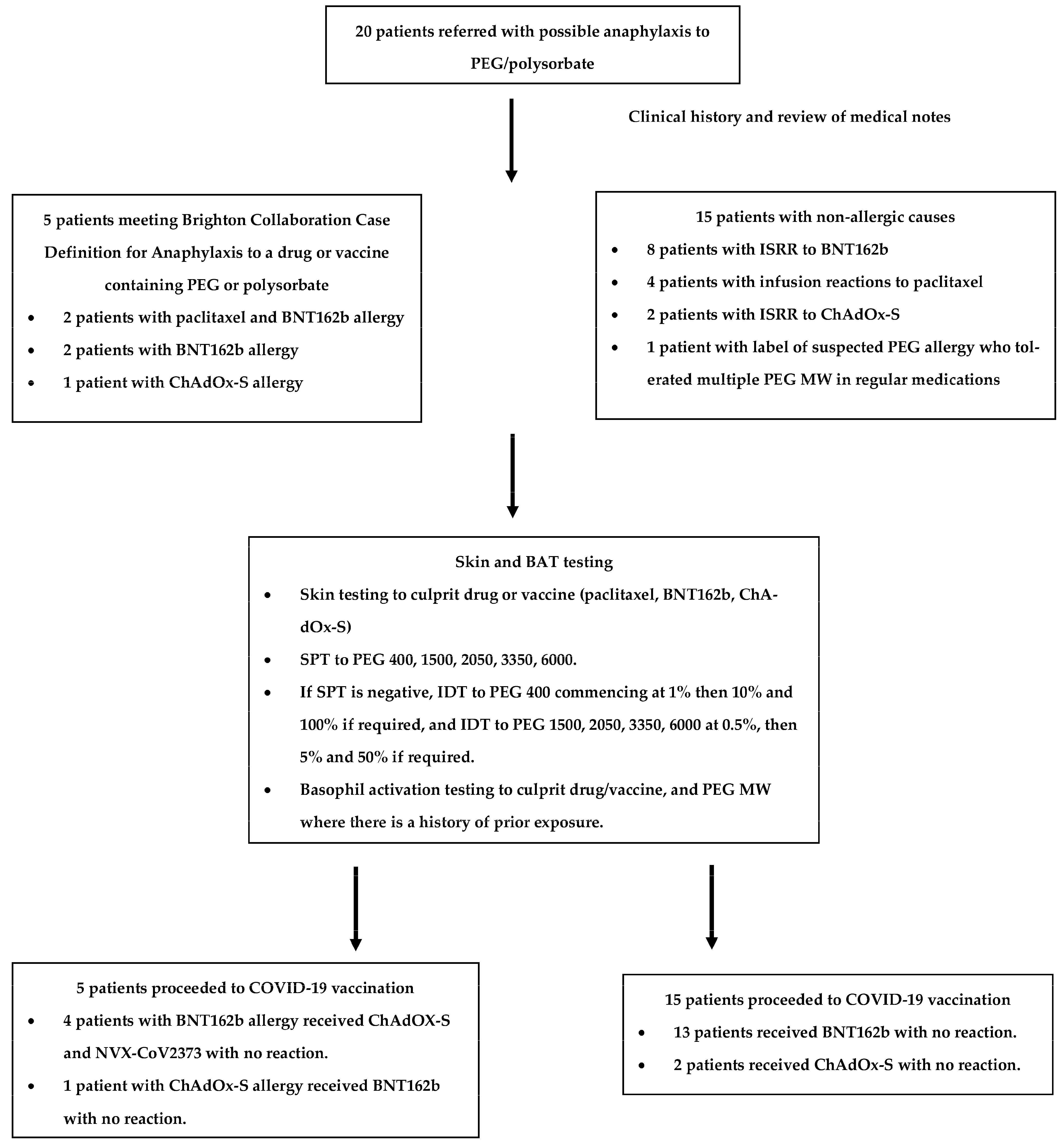
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sampath, V.; Rabinowitz, G.; Shah, M.; Jain, S.; Diamant, Z.; Jesenak, M.; Rabin, R.; Vieths, S.; Agache, I.; Akdis, M.; et al. Vaccines and allergic reactions: The past, the current COVID-19 pandemic, and future perspectives. Allergy 2021, 76, 1640–1660. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, D.D.; Peavy, R.D.; Gilfillan, A.M. Mechanisms of mast cell signaling in anaphylaxis. J. Allergy Clin. Immunol. 2009, 124, 639–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CDC. Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine—United States, 14–23 December 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 46–51. [Google Scholar] [CrossRef]
- CDC. Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Moderna COVID-19 Vaccine—United States. 21 December 2020–10 January 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 125–129. [Google Scholar] [CrossRef]
- McNeil, M.M.; Weintraub, E.S.; Duffy, J.; Sukumaran, L.; Jacobsen, S.J.; Klein, N.P.; Hambidge, S.J.; Lee, G.M.; Jackson, L.A.; Irving, S.A.; et al. Risk of anaphylaxis after vaccination in children and adults. J. Allergy Clin. Immunol. 2015, 137, 868–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNeil, M.M. Vaccine-Associated Anaphylaxis. Curr. Treat. Options Allergy 2019, 6, 297–308. [Google Scholar] [CrossRef]
- Jang, H.-J.; Shin, C.Y.; Kim, K.-B. Safety Evaluation of Polyethylene Glycol (PEG) Compounds for Cosmetic Use. Toxicol. Res. 2015, 31, 105–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanomedicine and the COVID-19 vaccines. Nat. Nanotechnol. 2020, 15, 963. [CrossRef]
- Coors, E.A.; Seybold, H.; Merk, H.F.; Mahler, V. Polysorbate 80 in medical products and nonimmunologic anaphylactoid reactions. Ann. Allergy Asthma Immunol. 2005, 95, 593–599. [Google Scholar] [CrossRef]
- Turner, P.J.; Ansotegui, I.J.; Campbell, D.E.; Cardona, V.; Ebisawa, M.; El-Gamal, Y.; Fineman, S.; Geller, M.; Gonzalez-Estrada, A.; Greenberger, P.A.; et al. COVID-19 vaccine-associated anaphylaxis: A statement of the World Allergy Organization Anaphylaxis Committee. World Allergy Organ. J. 2021, 14, 100517. [Google Scholar] [CrossRef]
- Wenande, E.; Garvey, L.H. Immediate-type hypersensitivity to polyethylene glycols: A review. Clin. Exp. Allergy 2016, 46, 907–922. [Google Scholar] [CrossRef] [PubMed]
- Sellaturay, P.; Nasser, S.; Ewan, P. Polyethylene Glycol–Induced Systemic Allergic Reactions (Anaphylaxis). J. Allergy Clin. Immunol. Pract. 2021, 9, 670–675. [Google Scholar] [CrossRef]
- Fisher, A.A. Immediate and delayed allergic contact reactions to polyethylene glycol. Contact Dermat. 1978, 4, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Wylon, K.; Dölle, S.; Worm, M. Polyethylene glycol as a cause of anaphylaxis. Allergy, Asthma Clin. Immunol. 2016, 12, 67. [Google Scholar] [CrossRef] [Green Version]
- Sellaturay, P.; Nasser, S.; Islam, S.; Gurugama, P.; Ewan, P.W. Polyethylene glycol (PEG) is a cause of anaphylaxis to the Pfizer/BioNTech mRNA COVID-19 vaccine. Clin. Exp. Allergy 2021, 51, 861–863. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Codesido, S.; Rosado, A.; Durana, A.D.D.; Arias, T.A.; González-Moreno, A.; Alonso, M.T. Hypersensitivity to Covid-19 Vaccine Confirmed by a Positive Skin Test Result: A Case Report. J. Investig. Allergol. Clin. Immunol. 2021, 31, 524–525. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.-H.; Stone, C.A.; Jakubovic, B.; Phillips, E.J.; Sussman, G.; Park, J.; Hoang, U.; Kirshner, S.L.; Levin, R.; Kozlowski, S. Anti-PEG IgE in anaphylaxis associated with polyethylene glycol. J. Allergy Clin. Immunol. Pract. 2020, 9, 1731–1733.e3. [Google Scholar] [CrossRef]
- Picard, M.; Drolet, J.-P.; Masse, M.-S.; Filion, C.A.; Al-Muhizi, F.; Fein, M.; Copaescu, A.; Isabwe, G.A.C.; Blaquière, M.; Primeau, M.-N. Safety of COVID-19 vaccination in patients with polyethylene glycol allergy: A case series. J. Allergy Clin. Immunol. Pract. 2021, 10, 620–625.e1. [Google Scholar] [CrossRef]
- Klimek, L.; Novak, N.; Cabanillas, B.; Jutel, M.; Bousquet, J.; Akdis, C. Allergenic components of the mRNA-1273 vaccine for COVID-19: Possible involvement of polyethylene glycol and IgG-mediated complement activation. Allergy 2021, 76, 3307–3313. [Google Scholar] [CrossRef]
- Greenhawt, M.; Abrams, E.M.; Shaker, M.; Chu, D.K.; Khan, D.; Akin, C.; Alqurashi, W.; Arkwright, P.; Baldwin, J.L.; Ben-Shoshan, M.; et al. The Risk of Allergic Reaction to SARS-CoV-2 Vaccines and Recommended Evaluation and Management: A Systematic Review, Meta-Analysis, GRADE Assessment, and International Consensus Approach. J. Allergy Clin. Immunol. Pract. 2021, 9, 3546–3567. [Google Scholar] [CrossRef]
- Krantz, M.; Bruusgaard-Mouritsen, M.; Koo, G.; Phillips, E.; Stone, C.; Garvey, L. Anaphylaxis to the first dose of mRNA SARS-CoV-2 vaccines: Don’t give up on the second dose. Allergy 2021, 76, 2916–2920. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization Stress-Related Response: A Manual for Program Managers and Health Professionals to Prevent, Identify and Respond to Stress-Related Responses Following Immunization; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Taylor, S.; Asmundson, G.J. Immunization stress-related responses: Implications for vaccination hesitancy and vaccination processes during the COVID-19 pandemic. J. Anxiety Disord. 2021, 84, 102489. [Google Scholar] [CrossRef] [PubMed]
- Roselló, S.; Blasco, I.; Fabregat, L.G.; Cervantes, A.; Jordan, K. Management of infusion reactions to systemic anticancer therapy: ESMO Clinical Practice Guidelines. Ann. Oncol. 2017, 28, iv100–iv118. [Google Scholar] [CrossRef] [PubMed]
- Banerji, A.; Wickner, P.G.; Saff, R.; Stone, C.A., Jr.; Robinson, L.B.; Long, A.A.; Wolfson, A.R.; Williams, P.; Khan, D.A.; Phillips, E.; et al. mRNA Vaccines to Prevent COVID-19 Disease and Reported Allergic Reactions: Current Evidence and Suggested Approach. J. Allergy Clin. Immunol. Pract. 2021, 9, 1423–1437. [Google Scholar] [CrossRef]
- Ieven, T.; Van Weyenbergh, T.; Vandebotermet, M.; Devolder, D.; Breynaert, C.; Schrijvers, R. Tolerability of polysorbate 80–containing COVID-19 vaccines in confirmed polyethylene glycol–allergic patients. J. Allergy Clin. Immunol. Pract. 2021, 9, 4470–4472.e1. [Google Scholar] [CrossRef]
- Barbaud, A.; Garvey, L.H.; Arcolaci, A.; Brockow, K.; Mori, F.; Mayorga, C.; Bonadonna, P.; Atanaskovic-Markovic, M.; Moral, L.; Zanoni, G.; et al. Allergies and COVID-19 vaccines: An ENDA/EAACI Position paper. Allergy 2022, 77, 2292–2312. [Google Scholar] [CrossRef] [PubMed]
- Bruusgaard-Mouritsen, M.J.B.; Poulsen, L.; Johansen, J.; Garvey, L. Optimizing investigation of suspected allergy to polyethylene glycols. J. Allergy Clin. Immunol. Pract. 2022, 149, 168–175.e4. [Google Scholar] [CrossRef] [PubMed]
- Eberlein, B.; Sonja, M.; Fischer, J.; Darsow, U.; Biedermann, T.; Brockow, K. Do basophil activation tests help elucidate allergic reactions to the ingredients in COVID-19 vaccines? Allergy 2022, 77, 2924–2936. [Google Scholar] [CrossRef] [PubMed]
- Joshi, D.; Alsentzer, E.; Edwards, K.; Norton, A.; Williams, S.E. An algorithm developed using the Brighton Collaboration case definitions is more efficient for determining diagnostic certainty. Vaccine 2014, 32, 3469–3472. [Google Scholar] [CrossRef]
- Li, J.; Best, O.G.; Rose, M.A.; Green, S.L.; Fulton, R.B.; Fernando, S.L. Integrating basophil activation tests into evaluation of perioperative anaphylaxis to neuromuscular blocking agents. Br. J. Anaesth. 2019, 123, e135–e143. [Google Scholar] [CrossRef]
- Mortz, C.G.; Kjaer, H.F.; Rasmussen, T.H.; Rasmussen, H.M.; Garvey, L.H.; Bindslev-Jensen, C. Allergy to polyethylene glycol and polysorbates in a patient cohort: Diagnostic work-up and decision points for vaccination during the COVID-19 pandemic. Clin. Transl. Allergy 2022, 12, e12111. [Google Scholar] [CrossRef] [PubMed]
- Risma, K.A. COVID-19 mRNA vaccine allergy. Curr. Opin. Pediatr. 2021, 33, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Kelso, J.M. IgE-mediated allergy to polyethylene glycol (PEG) as a cause of anaphylaxis to mRNA COVID-19 vaccines. Clin. Exp. Allergy 2021, 52, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Troelnikov, A.; Perkins, G.; Yuson, C.; Ahamdie, A.; Balouch, S.; Hurtado, P.R.; Hissaria, P. Basophil reactivity to BNT162b2 is mediated by PEGylated lipid nanoparticles in patients with PEG allergy. J. Allergy Clin. Immunol. 2021, 148, 91–95. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Anaphylaxis | Immunization Stress-Related Responses | |||
|---|---|---|---|---|
| Acute stress response | Vasovagal reaction | Infusion reaction, including the cytokine release syndrome | ||
| Skin | Urticaria Erythema Pruritus Angioedema Rhinoconjunctivitis | Pallor Diaphoresis Cold and clammy | Pallor Diaphoresis Cold and clammy | Erythema Urticaria Pruritus |
| Cardiovascular | Tachycardia Hypotension Cardiac arrest | Tachycardia Hypertension | Bradycardia Hypotension | Hypotension |
| Respiratory | Cough Stridor Wheeze Respiratory arrest | Hyperventilation | Normal to deep breaths | Wheeze |
| Gastrointestinal | Nausea Vomiting Abdominal cramping | Nausea | Nausea Vomiting | Nausea Vomiting Abdominal cramping Diarrhea |
| Neurological | Uneasiness Restlessness Agitation Loss of consciousness with no response to supine position | Fearfulness Light-headedness Dizziness Paraesthesia Spasms of hands and/or feet | Transient loss of consciousness with good response to supine position | |
| Patient | Age (Years) | Gender (M/F) | Culprit Drug | Atopy | Brighton Collaboration Case Definition for Anaphylaxis [30] | Time from Reaction to Assessment | Intradermal Skin Test Results | BAT Results | History of Exposure to PEG | Outcome of COVID-19 Vaccination |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 58 | F | Paclitaxel (containing PEG 35-castor oil) | nil | Level 1 Anaphylaxis Sudden onset and rapid progression of Major Criteria: - Generalized pruritus with rash, and - Measured hypotension | 1 year, 4 months | Paclitaxel 0.12 mg/mL +ve | Paclitaxel -ve | n/p | |
| BNT162b 10% +ve | BNT162b CD63 -ve CD203c +ve | BNT162b allergy: Systemic reaction to BNT162b 10% skin test characterized by generalized itch and rash. | ||||||||
| PEG 2050 50% +ve 5% +ve | PEG 2050 CD63 +ve CD203c -ve | |||||||||
| ChAdOx-S 10% -ve | ChAdOx-S -ve | ChAdOx-S tolerated. | ||||||||
| Polysorbate 80 20% -ve | n/p | |||||||||
| PEG 400 100% +ve 10% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 5% +ve 0.5% -ve | PEG 3350 -ve | Movicol and Coloxyl as laxative tolerated. | ||||||||
| PEG 6000 5% +ve 0.5% -ve | n/p | Patient is not aware of exposures to PEG 6000. | ||||||||
| 2 | 38 | F | Paclitaxel (containing PEG 35-castor oil) | nil | Level 2 Anaphylaxis Sudden onset and rapid progression of: Major criteria - Generalized pruritus with rash, and - Tachypnoea Minor Criteria - Difficulty breathing without wheeze or stridor - Abdominal pain | 4 year, 8 months | Paclitaxel 0.0012 mg/mL +ve | Paclitaxel 0.012 mg/mL CD63 +ve CD203c -ve | ||
| BNT162b 10% +ve | BNT162b CD63 +ve CD203c +ve | BNT162b allergy: Systemic reaction to BNT162b 10% skin test characterized by generalized itch and rash. | ||||||||
| PEG 2050 50% +ve 5% +ve | PEG 2050 CD63 +ve CD203c +ve | |||||||||
| ChAdOx-S 10% -ve | ChAdOx-S CD63 -ve CD203c +ve | ChAdOx-S tolerated. | ||||||||
| Polysorbate 80 20% -ve | Polysorbate 80 CD63 -ve CD203c -ve | |||||||||
| PEG 400 100% +ve 10% +ve 1% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 50% -ve | PEG 3350 -ve | Movicol as laxative tolerated. | ||||||||
| PEG 6000 5% +ve 0.5% -ve | n/p | Patient is not aware of exposures to PEG 6000. | ||||||||
| 3 | 47 | F | BNT162b | nil | Level 1 Anaphylaxis Sudden onset and rapid progression of Major criteria: - Generalized pruritus with rash, and localized angioedema (facial) - Upper airway swelling (throat, uvula, and larynx) | 8 weeks | BNT162b 10% + | BNT162b -ve | BNT162b anaphylaxis. | |
| PEG 2050 50% +ve 5% +ve | PEG 2050 -ve | |||||||||
| ChAdOx-S 10% -ve | n/p | ChAdOx-S and NVX-CoV2373 tolerated. | ||||||||
| Polysorbate 80 20% -ve | n/p | |||||||||
| PEG 400 100% +ve 10% +ve 1% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 50% +ve 5% +ve 0.5% -ve | n/p | Possible use of laxatives previously with no reaction. | ||||||||
| PEG 6000 50% +ve 5% -ve | n/p | Patient is not aware of exposures to PEG 6000. | ||||||||
| 4 | 34 | F | BNT162b | nil | Level 2 Anaphylaxis Sudden onset and rapid progression of Major criteria: - Upper airway swelling (throat and uvula), tachypnoea, and increased use of accessory muscles Minor criteria: - Generalized prickle sensation - Difficulty breathing without wheeze or stridor | 8 weeks | BNT162b 10% +ve | BNT162b -ve | BNT162b anaphylaxis. | |
| PEG 2050 50% +ve 5% +ve | PEG 2050 -ve | |||||||||
| ChAdOx-S 10% -ve | n/p | ChAdOx-S and NVX-CoV2373 tolerated. | ||||||||
| Polysorbate 80 20% -ve | n/p | |||||||||
| PEG 400 100% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 50% -ve | PEG 3350 -ve | Movicol as laxative tolerated. | ||||||||
| PEG 6000 50% -ve | n/p | Patient is not aware of exposures to PEG 6000. | ||||||||
| 5 | 29 | F | ChAdOx-S | Allergic rhinoconjunctivitis | Level 2 Anaphylaxis Sudden onset and rapid progression of Major criteria: - Upper airway swelling (throat and uvula), tachypnoea, and increased use of accessory muscles Minor criteria: - Tachycardia, decreased level of consciousness - Difficulty breathing without wheeze or stridor | 8 weeks | ChAdOx-S 10% +ve | ChAdOx-S -ve | ChAdOx-S anaphylaxis. | |
| Polysorbate 80 20% +ve 2% -ve | n/p | |||||||||
| BNT162b 10% +ve | BNT162b -ve | BNT162b2 tolerated. | ||||||||
| PEG 2050 50% -ve | PEG 2050 -ve | |||||||||
| PEG 400 100% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 50% -ve | n/p | Patient is not aware of exposures to PEG 3350. | ||||||||
| PEG 6000 50% -ve | n/p | Patient is not aware of exposures to PEG 6000. |
| IDT | W/V | Sensitivity | Specificity | Number of Patients | ||
|---|---|---|---|---|---|---|
| PEG 1500 or 2050 | 5% | 100% | 100% | 20 | ||
| Polysorbate 80 | 20% | 100% | 90% | 20 | ||
| BNT162b2 | 10% | 100% | 83.3% | 15 | ||
| ChAdOx1-S | 10% | 100% | 100% | 6 | ||
| PEG 400 | 10% | - | 65% | 20 | ||
| PEG 400 | 1% | - | 90% | 20 | ||
| PEG 400 | 0.01% | - | 100% | 20 | ||
| PEG 3350 | 5% | - | 75% | 20 | ||
| PEG 3350 | 0.5% | - | 100% | 20 | ||
| PEG 6000 | 5% | - | 85% | 20 | ||
| PEG 6000 | 0.5% | - | 100% | 20 | ||
| BAT | CD63 | CD203c | CD63 | CD203c | ||
| PEG 1500 or 2050 | 10% | 66.6% | 33.3% | 100% | 66.6% | 12 |
| PEG 1500 or 2050 | 1% | - | 0% | 77.8% | 12 | |
| Polysorbate 80 | 10% | 0% | 0% | 100% | 50% | 5 |
| Polysorbate 80 | 1% | - | 0% | - | 75% | 5 |
| BNT162b2 | 10% | 50% | 50% | 88.9% | 87.5% | 10 |
| BNT162b2 | 5% | 0% | - | 100% | - | 10 |
| ChAdOx1-S | 10% | 0% | 0% | 100% | 75% | 6 |
| PEG 400 | 10% | - | - | 100% | 77.8% | 9 |
| PEG 400 | 0.1% | - | - | - | 88.9% | 9 |
| PEG 3350 | 10% | - | - | 100% | 83.3% | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Weir, C.; Fulton, R.; Fernando, S.L. Skin Testing and Basophil Activation Testing Is Useful for Assessing Immediate Reactions to Polyethylene Glycol-Containing Vaccines. Vaccines 2023, 11, 252. https://doi.org/10.3390/vaccines11020252
Li J, Weir C, Fulton R, Fernando SL. Skin Testing and Basophil Activation Testing Is Useful for Assessing Immediate Reactions to Polyethylene Glycol-Containing Vaccines. Vaccines. 2023; 11(2):252. https://doi.org/10.3390/vaccines11020252
Chicago/Turabian StyleLi, Jamma, Christopher Weir, Richard Fulton, and Suran L. Fernando. 2023. "Skin Testing and Basophil Activation Testing Is Useful for Assessing Immediate Reactions to Polyethylene Glycol-Containing Vaccines" Vaccines 11, no. 2: 252. https://doi.org/10.3390/vaccines11020252