

Monkeypox Vaccine Acceptance among Ghanaians: A Call for Action

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Setting
2.2. Study Participants and Sample Size
2.3. Studied Variables
2.4. Data Collection Tool
2.5. Operational Definitions
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Participants’ Demographics
3.2. Intention to Receive MPOX Vaccine
3.3. Association between Different Population Criteria and Intention to Receive MPOX Vaccine
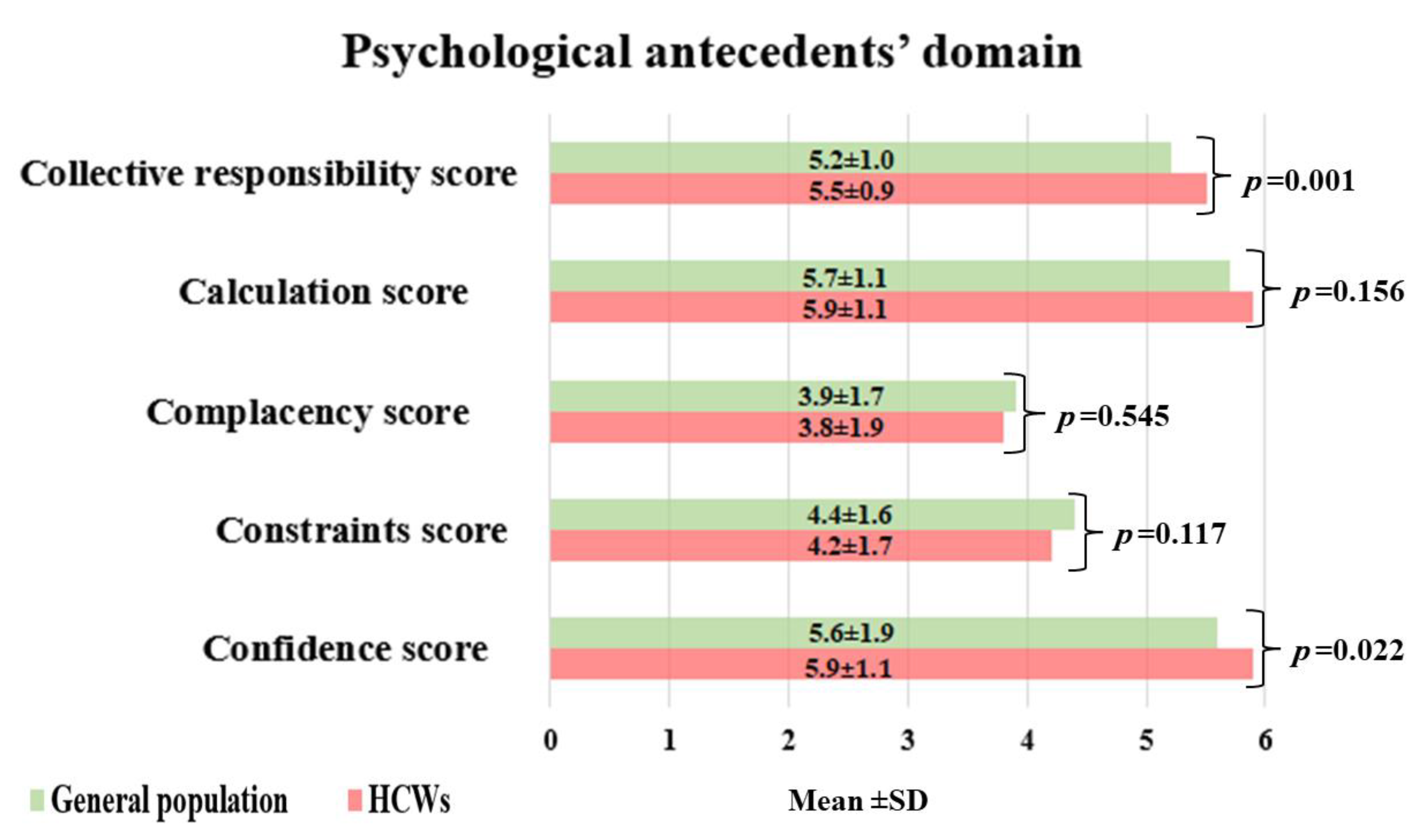
3.4. The Psychological Antecedents of HCWs and the General Population toward MPOX Vaccine
3.5. Determinants of MPOX Vaccine Acceptance among the Studied Ghanaian Population
4. Discussion
4.1. Confidence
4.2. Collective Reasonability
4.3. Refusal of Other Vaccines
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harapan, H.; Ophinni, Y.; Megawati, D.; Frediansyah, A.; Mamada, S.S.; Salampe, M.; Bin Emran, T.; Winardi, W.; Fathima, R.; Sirinam, S. Monkeypox: A Comprehensive Review. Viruses 2022, 14, 2155. [Google Scholar] [CrossRef] [PubMed]
- Mauldin, M.R.; McCollum, A.M.; Nakazawa, Y.J.; Mandra, A.; Whitehouse, E.R.; Davidson, W.; Zhao, H.; Gao, J.; Li, Y.; Doty, J. Exportation of monkeypox virus from the African continent. J. Infect. Dis. 2022, 225, 1367–1376. [Google Scholar] [CrossRef] [PubMed]
- Ligon, B.L. Monkeypox: A review of the history and emergence in the Western hemisphere. In Seminars in Pediatric Infectious Diseases; Elsevier: Amsterdam, The Netheralnds, 2004; pp. 280–287. [Google Scholar]
- Durski, K.N.; McCollum, A.M.; Nakazawa, Y.; Petersen, B.W.; Reynolds, M.G.; Briand, S.; Djingarey, M.H.; Olson, V.; Damon, I.K.; Khalakdina, A. Emergence of monkeypox—West and central Africa, 1970–2017. Morb. Mortal. Wkly. Rep. 2018, 67, 306. [Google Scholar] [CrossRef] [PubMed]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox—A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef]
- World Health Organization. Multi-Country Monkeypox Outbreak: Situation Update. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON396 (accessed on 10 January 2023).
- World Health Organization. Monkeypox Outbreak: Global Trends. Available online: https://worldhealthorg.shinyapps.io/MPOX_global (accessed on 10 January 2023).
- World Health Organization. Multi-Country Monkeypox Outbreak in Non-Endemic Countries. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON385 (accessed on 10 January 2023).
- Farooq, F.; Rathore, F.A. COVID-19 vaccination and the challenge of infodemic and disinformation. J. Korean Med. Sci. 2021, 36, e78. [Google Scholar] [CrossRef] [PubMed]
- Ophinni, Y.; Frediansyah, A.; Sirinam, S.; Megawati, D.; Stoian, A.M.; Enitan, S.S.; Akele, R.Y.; Sah, R.; Pongpirul, K.; Abdeen, Z. Monkeypox: Immune response, vaccination and preventive efforts. Narra J. 2022, 2. [Google Scholar] [CrossRef]
- Xiang, Y.; White, A. Monkeypox virus emerges from the shadow of its more infamous cousin: Family biology matters. Emerg. Microbes Infect. 2022, 11, 1768–1777. [Google Scholar] [CrossRef]
- Siddiqui, M.O.; Syed, M.A.; Tariq, R.; Mansoor, S. Multicounty outbreak of monkeypox virus—Challenges and recommendations. J. Med. Virol. 2022, 95, e27966. [Google Scholar] [CrossRef] [PubMed]
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5c validated tool: An online survey in 13 Arab countries. PloS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef]
- Shaaban, R.; Ghazy, R.M.; Elsherif, F.; Ali, N.; Yakoub, Y.; Aly, M.O.; ElMakhzangy, R.; Abdou, M.S.; McKinna, B.; Elzorkany, A.M.; et al. COVID-19 Vaccine Acceptance among Social Media Users: A Content Analysis, Multi-Continent Study. Int. J. Environ. Res. Public Health 2022, 19, 5737. [Google Scholar] [CrossRef]
- Elbarazi, I.; Yacoub, M.; Reyad, O.A.; Abdou, M.S.; Elhadi, Y.A.M.; Kheirallah, K.A.; Ababneh, B.F.; Hamada, B.A.; El Saeh, H.M.; Ali, N. Exploring enablers and barriers toward COVID-19 vaccine acceptance among Arabs: A qualitative study. Int. J. Disaster Risk Reduct. 2022, 82, 103304. [Google Scholar] [CrossRef] [PubMed]
- Ghazy, R.M.; Abdou, M.S.; Awaidy, S.; Sallam, M.; Elbarazi, I.; Youssef, N.; Fiidow, O.A.; Mehdad, S.; Hussein, M.F.; Adam, M.F. Acceptance of COVID-19 vaccine booster doses using the health belief model: A cross-sectional study in low-middle-and high-income countries of the East Mediterranean region. Int. J. Environ. Res. Public Health 2022, 19, 12136. [Google Scholar] [CrossRef] [PubMed]
- Abdelmoneim, S.A.; Sallam, M.; Hafez, D.M.; Elrewany, E.; Mousli, H.M.; Hammad, E.M.; Elkhadry, S.W.; Adam, M.F.; Ghobashy, A.A.; Naguib, M. COVID-19 vaccine booster dose acceptance: Systematic review and meta-analysis. Trop. Med. Infect. Dis. 2022, 7, 298. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 10 January 2023).
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Hatmal, M.M.M.; Al-Hatamleh, M.A.; Olaimat, A.N.; Ahmad, S.; Hasan, H.; Ahmad Suhaimi, N.A.; Albakri, K.A.; Abedalbaset Alzyoud, A.; Kadir, R.; Mohamud, R. Comprehensive literature review of monkeypox. Emerg. Microbes Infect. 2022, 11, 2600–2631. [Google Scholar] [CrossRef]
- Betsch, C.; Habersaat, K.B.; Deshevoi, S.; Heinemeier, D.; Briko, N.; Kostenko, N.; Kocik, J.; Böhm, R.; Zettler, I.; Wiysonge, C.S. Sample study protocol for adapting and translating the 5C scale to assess the psychological antecedents of vaccination. BMJ Open 2020, 10, e034869. [Google Scholar] [CrossRef] [Green Version]
- Sallam, M.; Ghazy, R.M.; Al-Salahat, K.; Al-Mahzoum, K.; AlHadidi, N.M.; Eid, H.; Kareem, N.; Al-Ajlouni, E.; Batarseh, R.; Ababneh, N.A. The role of psychological factors and vaccine conspiracy beliefs in influenza vaccine hesitancy and uptake among Jordanian healthcare workers during the COVID-19 pandemic. Vaccines 2022, 10, 1355. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Abd ElHafeez, S.; Shaaban, R.; Elbarazi, I.; Abdou, M.S.; Ramadan, A.; Kheirallah, K.A. Determining the Cutoff Points of the 5C Scale for Assessment of COVID-19 Vaccines Psychological Antecedents among the Arab Population: A Multinational Study. J. Prim. Care Community Health 2021, 12, 21501327211018568. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Okeh, D.U.; Sallam, M.; Hussein, M.; Ismail, H.M.; Yazbek, S.; Mahboob, A.; Abd ElHafeez, S. Psychological Antecedents of Healthcare Workers towards Monkeypox Vaccination in Nigeria. Vaccines 2022, 10, 2151. [Google Scholar] [CrossRef]
- Epi-Info. Sample Size Calculation. Available online: https://www.openepi.com/SampleSize/SSCohort.htm (accessed on 10 January 2023).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann Intern Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Khaity, A.; Hasan, H.; Albakri, K.; Elsayed, H.; HA, H.A.; Islam, F.; Dhawan, M.; Ghaith, H.S.; Emran, T.B. Monkeypox from Congo 1970 to Europe 2022; is there a difference? Int. J. Surg. 2022, 104, 106827. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.K.; Petersen, B.W.; Whitehill, F.; Razeq, J.H.; Isaacs, S.N.; Merchlinsky, M.J.; Campos-Outcalt, D.; Morgan, R.L.; Damon, I.; Sánchez, P.J.; et al. Use of JYNNEOS (Smallpox and Monkeypox Vaccine, Live, Nonreplicating) for Preexposure Vaccination of Persons at Risk for Occupational Exposure to Orthopoxviruses: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Osterholm, M.T.; Gellin, B. Confronting 21st-century monkeypox. Science 2022, 377, 349. [Google Scholar] [CrossRef] [PubMed]
- Ghazy, R.M.; Hammad, E.M.; Hall, M.A.; Mahboob, A.; Zeina, S.; Elbanna, E.H.; Fadl, N.; Abdelmoneim, S.A.; ElMakhzangy, R.; Hammad, H.M.; et al. How can imported monkeypox break the borders? A rapid systematic review. Comp. Immunol. Microbiol. Infect. Dis. 2023, 92, 101923. [Google Scholar] [CrossRef]
- Titanji, B.K.; Tegomoh, B.; Nematollahi, S.; Konomos, M.; Kulkarni, P.A. Monkeypox: A Contemporary Review for Healthcare Professionals. Open Forum Infect. Dis. 2022, 9, ofac310. [Google Scholar] [CrossRef]
- Lulli, L.G.; Baldassarre, A.; Mucci, N.; Arcangeli, G. Prevention, Risk Exposure, and Knowledge of Monkeypox in Occupational Settings: A Scoping Review. Trop. Med. Infect. Dis. 2022, 7, 276. [Google Scholar] [CrossRef]
- Riad, A.; Drobov, A.; Rozmarinová, J.; Drapáčová, P.; Klugarová, J.; Dušek, L.; Pokorná, A.; Klugar, M. Monkeypox Knowledge and Vaccine Hesitancy of Czech Healthcare Workers: A Health Belief Model (HBM)-Based Study. Vaccines 2022, 10, 2022. [Google Scholar] [CrossRef]
- Ulloque-Badaracco, J.R.; Alarcón-Braga, E.A.; Hernandez-Bustamante, E.A.; Al-kassab-Córdova, A.; Benites-Zapata, V.A.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Acceptance towards Monkeypox Vaccination: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 1248. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- Zaeck, L.M.; Lamers, M.M.; Verstrepen, B.E.; Bestebroer, T.M.; van Royen, M.E.; Götz, H.; Shamier, M.C.; van Leeuwen, L.P.M.; Schmitz, K.S.; Alblas, K.; et al. Low levels of monkeypox virus-neutralizing antibodies after MVA-BN vaccination in healthy individuals. Nat. Med. 2022, 1–9. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Editor’s Choice: Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, L.A.B.; Gallant, A.J.; Cogan, N.; Rasmussen, S.; Young, D.; Williams, L. Older adults’ vaccine hesitancy: Psychosocial factors associated with influenza, pneumococcal, and shingles vaccine uptake. Vaccine 2021, 39, 3520–3527. [Google Scholar] [CrossRef] [PubMed]
- Lounis, M.; Bencherit, D.; Rais, M.A.; Riad, A. COVID-19 Vaccine Booster Hesitancy (VBH) and Its Drivers in Algeria: National Cross-Sectional Survey-Based Study. Vaccines 2022, 10, 621. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Overall (N = 605) | |
|---|---|---|
| Age | Mean ± SD | 30.0 ± 6.8 |
| [Min, Max] | [18.0, 67.0] | |
| Sex | Female | 237 (39.2) |
| Male | 368 (60.8) | |
| Residence | Urban | 152 (25.2) |
| Rural | 450 (74.8) | |
| Marital status | Have a partner | 40 (6.6) |
| Married | 153 (25.3) | |
| Single | 412 (68.1) | |
| Education | Pre-college/high school | 82 (13.6) |
| Professional/technical | 20 (3.3) | |
| Bachelor degree | 290 (47.9) | |
| Diploma | 161 (26.6) | |
| Post-graduate | 52 (8.6) | |
| Income | Low income | 327 (54.0) |
| Middle income | 268 (44.3) | |
| Upper income | 10 (1.7) | |
| Region | Greater Accra | 314 (51.9) |
| Ashanti | 113 (18.7) | |
| Other | 178 (29.4) | |
| Occupation | Not healthcare worker | 408 (67.4) |
| Nurse/midwife | 52 (8.6) | |
| Pharmacy technician | 7 (1.2) | |
| Physician/physician assistant | 27 (4.5) | |
| Public health personal | 103 (17.0) | |
| Laboratory technician | 8 (1.3) | |
| Chronic diseases | No | 578 (95.5) |
| Yes | 27 (4.5) | |
| COVID-19 vaccination | Fully vaccinated | 399 (66.0) |
| Not going to take the vaccine | 105 (17.3) | |
| Took the first dose, going to take the second | 84 (13.9) | |
| Took the first dose and will not take the second | 17 (2.8) | |
| Know someone passed due to MOPX | I do not know | 71 (11.8) |
| No | 518 (85.6) | |
| Yes | 16 (2.6) | |
| MPOX infection | No | 551 (91.1) |
| Yes | 54 (8.9) | |
| Psychological antecedents | Confidence score | 5.7 ± 1.1 |
| Constraints score | 4.3 ± 1.6 | |
| Complacency score | 3.9 ± 1.8 | |
| Calculation score | 5.8 ± 1.1 | |
| Collective responsibility score | 5.3 ± 1.0 |
| Demographic Characteristics Total (N = 605) | Reject Vaccination N (%) | Accept Vaccination N (%) | p-Value | |
|---|---|---|---|---|
| Age | Mean ± SD | 29.4 ± 6.5 | 30.8 ± 7.1 | 0.013 |
| Sex | Female | 143 (60.3) | 94 (39.7) | 0.013 |
| Male | 183 (49.7) | 185 (60.3) | ||
| Residence | Rural | 72 (47.4) | 80 (52.6) | 0.078 |
| Urban | 254 (56.4) | 199 (43.8) | ||
| Marital status | Have a partner | 23 (57.5) | 17 (42.5) | 0.278 |
| Married | 74 (48.4) | 79 (51.6) | ||
| Single | 229 (55.6) | 183 (44.4 | ||
| Educational level | Pre-college/high school | 42(51.2) | 40(48.8) | 0.264 |
| Professional/technical | 11(55.0) | 9(45.0) | ||
| Undergraduate (Bachelor) | 165(56.9) | 125(43.1) | ||
| Diploma | 77(47.8) | 84(52.2) | ||
| Post-graduate | 31(50.6) | 21(40.4) | ||
| Income | Low income | 168 (51.4) | 159 (48.6) | 0.369 |
| Middle income | 153 (57.1) | 115 (42.9) | ||
| Upper income | 5 (50.0) | 5 (50.0) | ||
| Region | Ashanti | 62 (54.9) | 51 (45.1) | 0.196 |
| Greater Accra | 178 (56.7) | 136 (43.3) | ||
| Others | 86 (48.3) | 92 (51.7) | ||
| Occupation | HCWs | 88 (44.7) | 109 (55.3) | <0.001 |
| Not healthcare worker | 238 (58.3) | 170 (41.7) | ||
| Chronic diseases | No | 314 (54.3) | 264 (45.7) | 0.418 |
| Yes | 12 (44.4) | 15 (55.6) | ||
| COVID-19 vaccination | Fully vaccinated | 182 (45.6) | 217 (54.4) | <0.001 |
| Not going to take the vaccine | 85 (81.0) | 20 (19.0) | ||
| Took first dose, going to take the second | 47 (56.0) | 37 (44.0) | ||
| Took first dose, will not take the second | 12 (70.6) | 5 (29.4) | ||
| Know someone who passed due to MPOX | I do not know | 41 (57.7) | 30 (42.3) | 0.155 |
| No | 280 (54.1) | 238 (45.9) | ||
| Yes | 5 (31.3) | 11 (68.8) | ||
| MPOX infection | No | 305 (55.4) | 246 (44.6) | 0.030 |
| Yes | 21 (38.9) | 33 (61.1) | ||
| Psychological antecedents | Confidence score | 5.3 ± 1.3 | 6.2 ± 0.7 | <0.001 |
| Constraints score | 4.4 ± 1.5 | 4.2 ± 1.7 | 0.059 | |
| Complacency score | 4.0 ± 1.7 | 3.8 ± 1.9 | 0.091 | |
| Calculation score | 5.7 ± 1.1 | 5.9 ± 1.1 | 0.015 | |
| Collective responsibility score | 5.1 ± 1.0 | 5.6 ± 0.9 | <0.001 |
| Independent Variables | Unadjusted OR | Adjusted OR | |||
|---|---|---|---|---|---|
| Age | Mean (SD) | 29.4 (6.5) | 30.8 (7.1) | 1.03 (1.01–1.06, p = 0.013) | 1.02 (0.99–1.05, p = 0.123) |
| Gender | Female | 143 (60.3) | 94 (39.7) | - | - |
| Male | 183 (49.7) | 185 (50.3) | 1.54 (1.11–2.14, p = 0.011) | 1.48 (1.00–2.18, p = 0.049) | |
| Occupation | HCWs | 88 (44.7) | 109 (55.3) | - | - |
| Not healthcare worker | 238 (58.3) | 170 (41.7) | 0.58 (0.41–0.81, p = 0.002) | 0.86 (0.57–1.29, p = 0.468) | |
| Residence | Rural | 72 (47.4) | 80 (52.6) | - | - |
| Urban | 254 (56.1) | 199 (43.9) | 0.71 (0.49–1.02, p = 0.063) | 0.63 (0.41–0.96, p = 0.033) | |
| COVID-19 vaccination | Fully vaccinated | 182 (45.6) | 217 (54.4) | - | - |
| Not going to take the vaccine | 85 (81.0) | 20 (19.0) | 0.20 (0.11–0.33, p < 0.001) | 0.29 (0.16–0.52, p < 0.001) | |
| Took first dose, going to take the second | 47 (56.0) | 37 (44.0) | 0.66 (0.41–1.06, p = 0.086) | 0.77 (0.45–1.31, p = 0.331) | |
| Took first dose, will not take the second | 12 (70.6) | 5 (29.4) | 0.35 (0.11–0.96, p = 0.052) | 0.65 (0.18–2.09, p = 0.480) | |
| MPOX infection | No | 305 (55.4) | 246 (44.6) | - | - |
| Yes | 21 (38.9) | 33 (61.1) | 1.95 (1.11–3.50, p = 0.022) | 1.88 (0.99–3.63, p = 0.056) | |
| Confidence score | Mean (SD) | 5.3 (1.3) | 6.2 (0.7) | 2.65 (2.14–3.33, p < 0.001) | 2.45 (1.93–3.15, p < 0.001) |
| Constraints score | Mean (SD) | 4.4 (1.5) | 4.2 (1.7) | 0.91 (0.82–1.00, p = 0.059) | 0.84 (0.69–1.03, p = 0.088) |
| Complacency score | Mean (SD) | 4.0 (1.7) | 3.8 (1.9) | 0.93 (0.85–1.01, p = 0.091) | 1.07 (0.88–1.29, p = 0.513) |
| Calculation score | Mean (SD) | 5.7 (1.1) | 5.9 (1.1) | 1.20 (1.04–1.39, p = 0.016) | 0.93 (0.75–1.14, p = 0.482) |
| Collective responsibility score | Mean (SD) | 5.1 (1.0) | 5.6 (0.9) | 1.85 (1.55–2.23, p < 0.001) | 1.34 (1.02–1.75, p = 0.034) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghazy, R.M.; Yazbek, S.; Gebreal, A.; Hussein, M.; Addai, S.A.; Mensah, E.; Sarfo, M.; Kofi, A.; AL-Ahdal, T.; Eshun, G. Monkeypox Vaccine Acceptance among Ghanaians: A Call for Action. Vaccines 2023, 11, 240. https://doi.org/10.3390/vaccines11020240
Ghazy RM, Yazbek S, Gebreal A, Hussein M, Addai SA, Mensah E, Sarfo M, Kofi A, AL-Ahdal T, Eshun G. Monkeypox Vaccine Acceptance among Ghanaians: A Call for Action. Vaccines. 2023; 11(2):240. https://doi.org/10.3390/vaccines11020240
Chicago/Turabian StyleGhazy, Ramy Mohamed, Saja Yazbek, Assem Gebreal, Mai Hussein, Sylvia Agyeman Addai, Ernestina Mensah, Michael Sarfo, Agyapong Kofi, Tareq AL-Ahdal, and Gilbert Eshun. 2023. "Monkeypox Vaccine Acceptance among Ghanaians: A Call for Action" Vaccines 11, no. 2: 240. https://doi.org/10.3390/vaccines11020240