
Monkeypox Cross-Sectional Survey of Knowledge, Attitudes, Practices, and Willingness to Vaccinate among University Students in Pakistan
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting and Population
2.3. Study Instrument
2.4. Data Collection
2.5. Measures
2.5.1. Knowledge
2.5.2. Attitude
2.5.3. Perception
2.6. Sample Size Determination
2.7. Statistical Analysis
3. Results
3.1. Baseline Socio-Demographic Characteristics
3.2. Knowledge of Respondents toward Mpox
3.3. Attitudes of Respondents for Vaccination toward Mpox
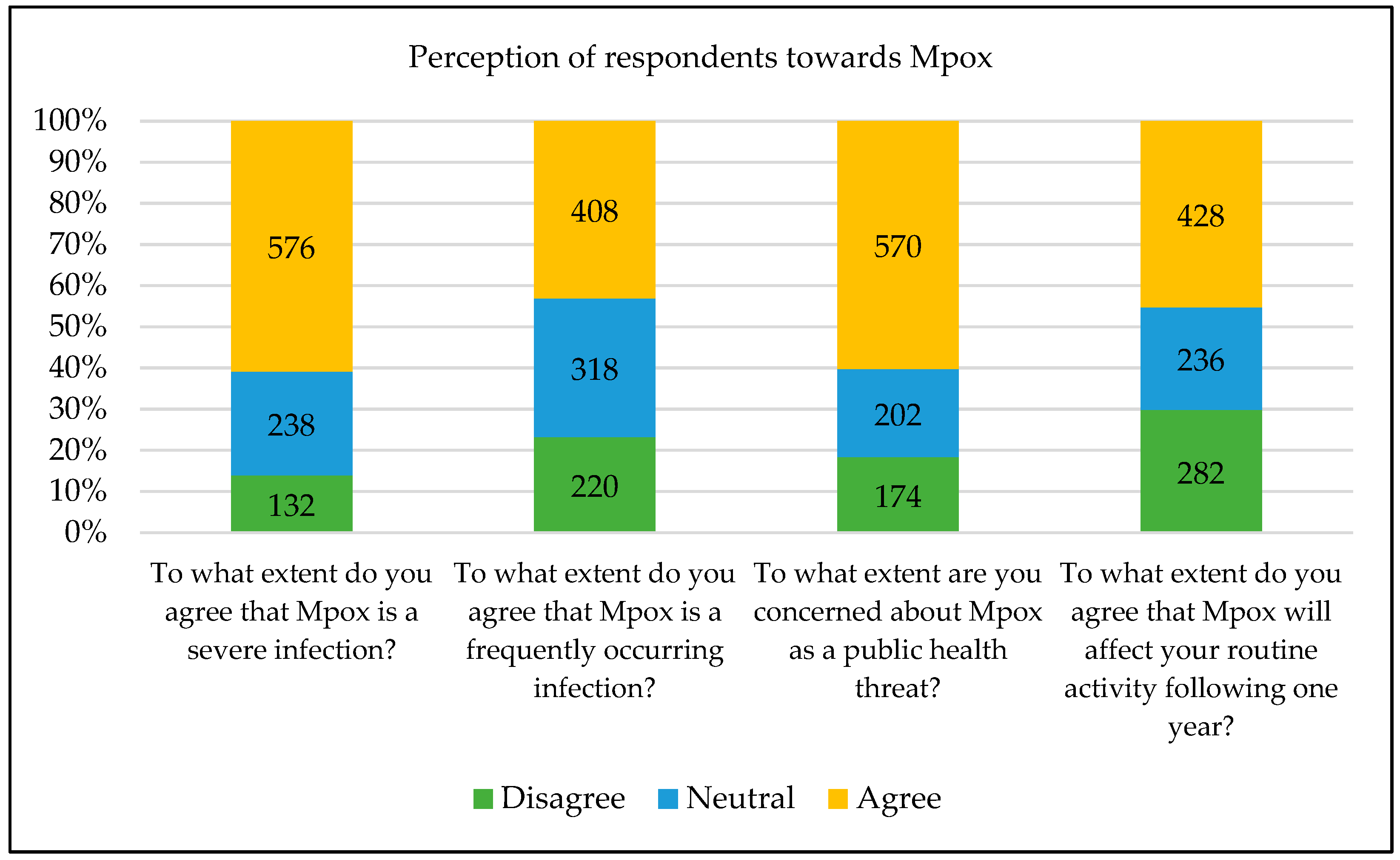
3.4. Perception of Respondents toward Mpox
3.5. Association between Socio-Demographics with Knowledge and Attitude of Mpox
3.6. Factors Associated with Knowledge of Mpox Using Linear Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Riccò, M.; Ferraro, P.; Camisa, V.; Satta, E.; Zaniboni, A.; Ranzieri, S.; Baldassarre, A.; Zaffina, S.; Marchesi, F. When a Neglected Tropical Disease Goes Global: Knowledge, Attitudes and Practices of Italian Physicians towards Monkeypox, Preliminary Results. Trop. Med. Infect. Dis. 2022, 7, 135. [Google Scholar] [CrossRef] [PubMed]
- Kabuga, A.I.; El Zowalaty, M.E. A review of the monkeypox virus and a recent outbreak of skin rash disease in Nigeria. J. Med. Virol. 2019, 91, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Aljamaan, F.; Alenezi, S.; Alhasan, K.; Saddik, B.; Alhaboob, A.; Altawil, E.S.; Alshahrani, F.; Alrabiaah, A.; Alaraj, A.; Alkriadees, K.; et al. Healthcare Workers’ Worries and Monkeypox Vaccine Advocacy during the First Month of the WHO Monkeypox Alert: Cross-Sectional Survey in Saudi Arabia. Vaccines 2022, 10, 1408. [Google Scholar] [CrossRef]
- Mileto, D.; Riva, A.; Cutrera, M.; Moschese, D.; Mancon, A.; Meroni, L.; Giacomelli, A.; Bestetti, G.; Rizzardini, G.; Gismondo, M.R.; et al. New challenges in human monkeypox outside Africa: A review and case report from Italy. Travel Med. Infect. Dis. 2022, 49, 102386. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Mahzoum, K.; Al-Tammemi, A.B.; Alkurtas, M.; Mirzaei, F.; Kareem, N.; Al-Naimat, H.; Jardaneh, L.; Al-Majali, L.; AlHadidi, A.; et al. Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. Healthcare 2022, 10, 1722. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 2022 Monkeypox Outbreak: Global Trends. 2022. Available online: https://worldhealthorg.shinyapps.io/mpx_global/#section-fns2 (accessed on 25 November 2022).
- Luo, Q.; Han, J. Preparedness for a monkeypox outbreak. Infect. Med. 2022, 1, 124–134. [Google Scholar] [CrossRef]
- Kaler, J.; Hussain, A.; Flores, G.; Kheiri, S.; Desrosiers, D. Monkeypox: A Comprehensive Review of Transmission, Pathogenesis, and Manifestation. Cureus 2022, 14, e26531. [Google Scholar] [CrossRef]
- Tiecco, G.; Degli Antoni, M.; Storti, S.; Tomasoni, L.R.; Castelli, F.; Quiros-Roldan, E. Monkeypox, a Literature Review: What Is New and Where Does This Concerning Virus Come From? Viruses 2022, 14, 1894. [Google Scholar] [CrossRef]
- Najeeb, H.; Huda, Z. Monkeypox virus: A spreading threat for Pakistan? Ann. Med. Surg. 2022, 79, 103977. [Google Scholar] [CrossRef]
- Billioux, B.J.; Mbaya, O.T.; Sejvar, J.; Nath, A. Neurologic complications of smallpox and monkeypox: A review. JAMA Neurol. 2022, 79, 1180–1186. [Google Scholar] [CrossRef]
- Nath, S.D.; Islam, A.M.K.; Majumder, K.; Rimti, F.H.; Das, J.; Tabassum, M.N.; Oishee, A.N.; Mahmood, T.; Paul, M.; Akhter, M.; et al. Assessment of Knowledge on Human Monkeypox Virus among General Population in Bangladesh: A Nationwide Cross-Sectional Study. medRxiv 2022. [Google Scholar] [CrossRef]
- Meo, S.A.; Al-Khlaiwi, T.; Aljofan, Z.F.; Alanazi, A.I.; Meo, A.S. Public Perceptions of the Emerging Human Monkeypox Disease and Vaccination in Riyadh, Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 1534. [Google Scholar] [CrossRef]
- Temsah, M.-H.; Aljamaan, F.; Alenezi, S.; Abouammoh, N.; Alhasan, K.; Dasuqi, S.A.; Alhaboob, A.; Hamad, M.A.; Halwani, R.; Alrabiaah, A.; et al. Monkeypox Disease (MPOX) Perceptions among Healthcare Workers versus General Population during the First Month of the WHO Alert: Cross-Sectional Survey in Saudi Arabia. Vaccines 2022, 10, 2071. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Ophinni, Y.; Megawati, D.; Frediansyah, A.; Mamada, S.S.; Salampe, M.; Bin Emran, T.; Winardi, W.; Fathima, R.; Sirinam, S.; et al. Monkeypox: A Comprehensive Review. Viruses 2022, 14, 2155. [Google Scholar] [CrossRef] [PubMed]
- Ladhani, S.N.; Aiano, F.; Edwards, D.S.; Perkins, S.; Khan, W.M.; Iyanger, N.; Whittaker, E.; Cohen, J.M.; Ho, D.; Hopkins, S.; et al. Very low risk of monkeypox among staff and students after exposure to a confirmed case in educational settings, England, May to July 2022. Eurosurveillance 2022, 27, 2200734. [Google Scholar] [CrossRef]
- Abdullah, M.A. The Impending Threat of Monkeypox: Responsiveness of Pakistan’s Health System. J. Islam. Med. Dent. Coll. 2022, 11, 60–61. [Google Scholar] [CrossRef]
- Ghoto, A.; Talpur, G.H.M.; Kamboh, S.A. Estimation and forecasting of the inflation, interest, literacy and unemployment rate of Pakistan using nonlinear regression models. Indian J. Sci. Technol. 2021, 14, 251–258. [Google Scholar] [CrossRef]
- Riad, A.; Drobov, A.; Rozmarinová, J.; Drapáčová, P.; Klugarová, J.; Dušek, L.; Pokorná, A.; Klugar, M. Monkeypox Knowledge and Vaccine Hesitancy of Czech Healthcare Workers: A Health Belief Model (HBM)-Based Study. Vaccines 2022, 10, 2022. [Google Scholar] [CrossRef]
- Sallam, M.; Eid, H.; Awamleh, N.; Al-Tammemi, A.B.; Barakat, M.; Athamneh, R.Y.; Hallit, S.; Harapan, H.; Mahafzah, A. Conspiratorial Attitude of the General Public in Jordan towards Emerging Virus Infections: A Cross-Sectional Study Amid the 2022 Monkeypox Outbreak. Trop. Med. Infect. Dis. 2022, 7, 411. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Knowledge of human monkeypox viral infection among general practitioners: A cross-sectional study in Indonesia. Ann. Trop. Med. Parasitol. 2020, 114, 68–75. [Google Scholar] [CrossRef]
- Khan, S.; Akbar, S.M.F.; Yahiro, T.; Al Mahtab, M.; Kimitsuki, K.; Nishizono, A. Unprecedented rise of monkeypox in Europe and America: Are Asian countries ready for a new outbreak during the ongoing COVID-19 pandemic? J. Glob. Health 2022, 12, 03066. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Al-Mahzoum, K.; Dardas, L.A.; Al-Tammemi, A.B.; Al-Majali, L.; Al-Naimat, H.; Jardaneh, L.; AlHadidi, F.; Al-Salahat, K.; Al-Ajlouni, E.; et al. Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses. Medicina 2022, 58, 924. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.K.; Abdulqadirb, S.O.; Omar, R.M.; Abdullah, A.J.; Rahman, H.A.; Hussein, S.H.; M-Amin, H.I.; Chandran, D.; Sharma, A.K.; Dhama, K.; et al. Study of knowledge, attitude and anxiety in Kurdistan-region of Iraqi population during the monkeypox outbreak in 2022: An online cross-sectional study. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Alsanafi, M.; Al-Mahzoum, K.; Sallam, M. Monkeypox Knowledge and Confidence in Diagnosis and Management with Evaluation of Emerging Virus Infection Conspiracies among Health Professionals in Kuwait. Pathogens 2022, 11, 994. [Google Scholar] [CrossRef]
- Alshahrani, N.Z.; Alzahrani, F.; Alarifi, A.M.; Algethami, M.R.; Alhumam, M.N.; Ayied, H.A.M.; Awan, A.Z.; Almutairi, A.F.; Bamakhrama, S.A.; Almushari, B.S.; et al. Assessment of Knowledge of Monkeypox Viral Infection among the General Population in Saudi Arabia. Pathogens 2022, 11, 904. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Bianco, L.; Da Molin, G.; Mancini, R.; Sciacchitano, S.; Ferracuti, S.; Liguori, G.; Orsi, G.B.; Napoli, C. “Monkeypox: What Do You Know about That?” Italian Adults’ Awareness of a New Epidemic. Pathogens 2022, 11, 1285. [Google Scholar] [CrossRef]
- Kumar, N.; Sulaiman, S.A.S.; Hashmi, F.K. An evaluation of public understanding regarding COVID-19 in Sindh, Pakistan: A focus on knowledge, attitudes and practices. J. Res. Pharm. 2021, 25, 881–889. [Google Scholar] [CrossRef]
- Winters, M.S.; Malik, A.A.; Omer, S.B. Attitudes of the US general public towards Monkeypox. medRxiv 2022. [Google Scholar] [CrossRef]
- Salim, N.A.; Septadina, I.S.; Permata, M.; Hudari, H. Knowledge, attitude, and perception of anticipating 2022 global human monkeypox infection among internal medicine residents at palembang indonesia: An online survey. J. Kedokt. dan Kesehat. Publ. Ilm. Fak. Kedokt. Univ. Sriwij. 2022, 9, 253–262. [Google Scholar] [CrossRef]
- Kumar, N.; Sulaiman, S.A.S.; Hashmi, F.K.; Qureshi, A.; Shaib, M.; Alam, S.; Hussain, M. Survey data of public in Sindh Pakistan regarding willingness to accept COVID-19 vaccination. PLoS ONE 2022, 17, e0270900. [Google Scholar] [CrossRef]
- Lulli, L.G.; Baldassarre, A.; Mucci, N.; Arcangeli, G. Prevention, Risk Exposure, and Knowledge of Monkeypox in Occupational Settings: A Scoping Review. Trop. Med. Infect. Dis. 2022, 7, 276. [Google Scholar] [CrossRef] [PubMed]
- Bates, B.R.; Grijalva, M.J. Knowledge, attitudes, and practices towards monkeypox during the 2022 outbreak: An online cross-sectional survey among clinicians in Ohio, USA. J. Infect. Public Health 2022, 15, 1459–1465. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.K.; Petersen, B.W.; Whitehill, F.M.D.V.; Razeq, J.H.; Isaacs, S.N.; Merchlinsky, M.J.; Campos-Outcalt, D.; Morgan, R.L.; Damon, I.; Sánchez, P.J.; et al. Use of JYNNEOS (Smallpox and Monkeypox Vaccine, Live, Nonreplicating) for Preexposure Vaccination of Persons at Risk for Occupational Exposure to Orthopoxviruses: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 734. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, C.; Bhattacharya, M.; Sharma, A.R.; Dhama, K. Monkeypox virus vaccine evolution and global preparedness for vaccination. Int. Immunopharmacol. 2022, 113, 109346. [Google Scholar] [CrossRef] [PubMed]
- Bankuru, S.V.; Kossol, S.; Hou, W.; Mahmoudi, P.; Rychtář, J.; Taylor, D. A game-theoretic model of Monkeypox to assess vaccination strategies. Peerj 2020, 8, e9272. [Google Scholar] [CrossRef]
- Bhattacharya, M.; Dhama, K.; Chakraborty, C. Recently spreading human monkeypox virus infection and its transmission during COVID-19 pandemic period: A travelers’ prospective. Travel Med. Infect. Dis. 2022, 49, 102398. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Categories | Frequency | Percentage |
|---|---|---|---|
| Gender | Female | 514 | 54.3 |
| Male | 432 | 45.7 | |
| Age (Mean ± SD.) | 22.5 ± 3.5 | ||
| Age groups (years) | 18–22 | 503 | 53.2 |
| 23–27 | 383 | 40.5 | |
| 28 and above | 60 | 6.3 | |
| Region | Sindh | 668 | 70.6 |
| Punjab | 166 | 17.5 | |
| Khyber Pakhtunkhwa | 42 | 4.4 | |
| Azad Kashmir | 36 | 3.8 | |
| Baluchistan | 26 | 2.7 | |
| Gilgit | 8 | 0.8 | |
| Education | Undergraduate | 867 | 91.6 |
| Post-graduate | 79 | 8.4 | |
| Discipline | Pharmaceutical Sciences | 669 | 70.7 |
| Medical Sciences | 136 | 14.4 | |
| Biological Sciences | 63 | 6.7 | |
| Others * | 78 | 8.2 | |
| Family income (monthly) in PKR | <50,000 PKR | 520 | 55.0 |
| 50,001–100,000 | 281 | 29.7 | |
| >100,000 | 145 | 15.3 | |
| Aware of Mpox before 2022 | No | 646 | 68.3 |
| Yes | 300 | 31.7 | |
| Received university-level information on Mpox | No | 748 | 79.1 |
| Yes | 198 | 20.9 | |
| Previous COVID-19 vaccination | No | 76 | 8.0 |
| Yes | 870 | 92.0 | |
| Previous seasonal flu vaccination | No | 590 | 62.4 |
| Yes | 356 | 37.6 | |
| Variables | Accuracy (n) | Frequency |
|---|---|---|
| K1. The Mpox virus is not a new discovery. | 542 | 57.3 |
| K2. The Mpox virus circulates only among primates, including humans. | 516 | 54.5 |
| K3. In most cases, Mpox does not present with the symptoms of an uncomplicated influenza-like illness. | 430 | 45.5 |
| K4. Mpox infection is associated with typical skin lesions. | 766 | 81.0 |
| K5. Asymptomatic patients cannot transmit the Mpox virus to others. | 270 | 28.5 |
| K6. European cases of Mpox have been mostly travel-associated. | 522 | 55.2 |
| K7. Currently, there is no specific vaccine against Mpox approved. | 550 | 58.1 |
| K8. Currently, there is no specific drug against Mpox approved. | 500 | 52.9 |
| K9. Recipients of the smallpox vaccine may need further vaccination shots against Mpox. | 550 | 58.1 |
| K10. Mpox causes more severe illness in children than in adults. | 548 | 57.9 |
| K11. Mpox infection is associated with a high rate of systemic complications. | 558 | 59.0 |
| K12. The skin rash associated with Mpox is typically synchronous (in a pattern). | 536 | 56.7 |
| K13. Standard preventive measures are effective in preventing Mpox infection. | 592 | 62.6 |
| K14. Mpox can survive for several days on contaminated surfaces. | 544 | 57.5 |
| K15. Mode of transmission. | 546 | 57.7 |
| K16. The usual case-fatality ratio of Mpox. | 214 | 22.6 |
| Knowledge level | ||
| Poor | 160 | 16.9 |
| Average | 726 | 76.7 |
| Good | 60 | 6.3 |
| Statements | Response | Frequency | Percentage |
|---|---|---|---|
| A1. I am willing to receive the smallpox vaccine to prevent Mpox infection. | Disagree | 206 | 21.8 |
| Neutral | 210 | 22.2 | |
| Agree | 530 | 56.0 | |
| A2. If made available, I am willing to receive the Mpox vaccine. | Disagree | 148 | 15.6 |
| Neutral | 158 | 16.7 | |
| Agree | 640 | 67.7 | |
| A3. I am willing to pay to receive a vaccine against Mpox. | Disagree | 270 | 28.5 |
| Neutral | 342 | 36.2 | |
| Agree | 334 | 35.3 | |
| A4. Will you get vaccinated against Mpox (if the government provides a free vaccine)? | Disagree | 270 | 28.5 |
| Neutral | 342 | 36.2 | |
| Agree | 334 | 35.3 | |
| Attitude levels | Negative | 104 | 11.0 |
| Neutral | 648 | 68.5 | |
| Positive | 194 | 20.5 |
| Variable | n (%) | Knowledge | p-Value | Attitude | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Poor | Average | Good | Negative | Neutral | Positive | ||||
| Gender | |||||||||
| Female | 514 (54.3) | 88 | 400 | 26 | 0.210 | 48 | 344 | 122 | 0.012 |
| Male | 432 (45.7) | 72 | 326 | 34 | 56 | 304 | 72 | ||
| Age groups | |||||||||
| 18–22 | 503 (53.2) | 86 | 385 | 32 | 0.184 | 62 | 361 | 80 | 0.002 |
| 23–27 | 383 (40.5) | 60 | 295 | 28 | 34 | 247 | 102 | ||
| 28 and above | 60 (6.3) | 14 | 46 | 0 | 8 | 40 | 12 | ||
| Academic | |||||||||
| Undergraduate | 867 (91.6) | 134 | 675 | 58 | <0.001 | 96 | 606 | 165 | <0.001 |
| Post-graduate | 79 (8.4) | 26 | 51 | 2 | 8 | 42 | 29 | ||
| Discipline | |||||||||
| Pharmaceutical Sciences | 669 (70.7) | 92 | 529 | 48 | <0.001 | 60 | 471 | 138 | <0.001 |
| Medical Sciences | 136 (14.4) | 16 | 112 | 8 | 22 | 80 | 34 | ||
| Biological Sciences | 63 (6.7) | 22 | 41 | 0 | 6 | 41 | 16 | ||
| Others * | 78 (8.2) | 30 | 44 | 4 | 16 | 56 | 6 | ||
| Region | |||||||||
| Sindh | 668 (70.6) | 98 | 524 | 46 | <0.001 | 74 | 464 | 130 | 0.057 |
| Punjab | 166 (17.5) | 42 | 110 | 14 | 12 | 116 | 38 | ||
| Khyber Pakhtunkha | 42 (4.4) | 2 | 40 | 0 | 8 | 22 | 12 | ||
| Azad Kashmir | 36 (3.8) | 12 | 14 | 0 | 6 | 18 | 2 | ||
| Baluchistan | 26 (2.7) | 2 | 6 | 0 | 2 | 4 | 2 | ||
| Gilgit | 8 (0.8) | 4 | 32 | 0 | 2 | 24 | 10 | ||
| Variables | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| Beta Coeff | 95% CI | p-Value | Beta Coeff | 95% CI | p-Value | |
| Age | 0.013 | −0.05–0.08 | 0.697 | - | - | - |
| Gender | ||||||
| Male | 0.28 | 0.24—0.19 | 0.241 | - | - | - |
| Female | 1 | - | - | - | ||
| Academic | ||||||
| Post-graduate | −1.65 | −2.47–0.83 | <0.0001 | - | - | - |
| Undergraduate | 1 | - | - | - | ||
| Discipline | ||||||
| Pharmaceutical Sciences | 1.31 | 0.82–1.81 | <0.0001 | 2.08 | 1.47–2.70 | <0.0001 |
| Medical Sciences | 0.05 | −0.61–0.70 | 0.889 | 1.46 | 0.66–2.26 | <0.0001 |
| Biological Sciences | −1.67 | −2.58–0.75 | <0.0001 | - | - | - |
| Others * | −2.30 | −3.12–1.48 | <0.0001 | - | - | - |
| Income (PKR) | ||||||
| <50,000 | −0.11 | −0.57–0.36 | 0.655 | - | - | - |
| 50,001–100,000 | 0.38 | −0.12–0.88 | 0.138 | - | - | - |
| >100,000 | −0.41 | −1.05–0.23 | 0.206 | - | - | - |
| Aware of Mpox before 2022 | ||||||
| Yes | 1.64 | 1.16–2.13 | <0.0001 | 1.19 | 0.71–1.67 | <0.0001 |
| No | 1 | 1 | ||||
| Received University-level inform | ||||||
| Yes | 2.03 | 1.48–2.58 | <0.0001 | 1.56 | 1.00–2.12 | <0.0001 |
| No | 1 | 1 | ||||
| Previous COVID-19 vaccination | ||||||
| Yes | 1.97 | 1.13–2.80 | <0.0001 | 1.46 | 0.66–2.25 | <0.0001 |
| No | 1 | 1 | ||||
| Previous seasonal flu vaccination | ||||||
| No | 0.57 | 0.10–1.04 | 0.019 | - | - | - |
| Yes | 1 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, N.; Ahmed, F.; Raza, M.S.; Rajpoot, P.L.; Rehman, W.; Khatri, S.A.; Mohammed, M.; Muhammad, S.; Ahmad, R. Monkeypox Cross-Sectional Survey of Knowledge, Attitudes, Practices, and Willingness to Vaccinate among University Students in Pakistan. Vaccines 2023, 11, 97. https://doi.org/10.3390/vaccines11010097
Kumar N, Ahmed F, Raza MS, Rajpoot PL, Rehman W, Khatri SA, Mohammed M, Muhammad S, Ahmad R. Monkeypox Cross-Sectional Survey of Knowledge, Attitudes, Practices, and Willingness to Vaccinate among University Students in Pakistan. Vaccines. 2023; 11(1):97. https://doi.org/10.3390/vaccines11010097
Chicago/Turabian StyleKumar, Narendar, Fatima Ahmed, Muhammad Sauban Raza, Pushp Lata Rajpoot, Wajiha Rehman, Shoaib Alam Khatri, Mustapha Mohammed, Shaib Muhammad, and Rabbiya Ahmad. 2023. "Monkeypox Cross-Sectional Survey of Knowledge, Attitudes, Practices, and Willingness to Vaccinate among University Students in Pakistan" Vaccines 11, no. 1: 97. https://doi.org/10.3390/vaccines11010097