
Immune Responses to SARS-CoV-2 Infection and Vaccine in a Big Italian COVID-19 Hospital: An 18-Month Follow-Up
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
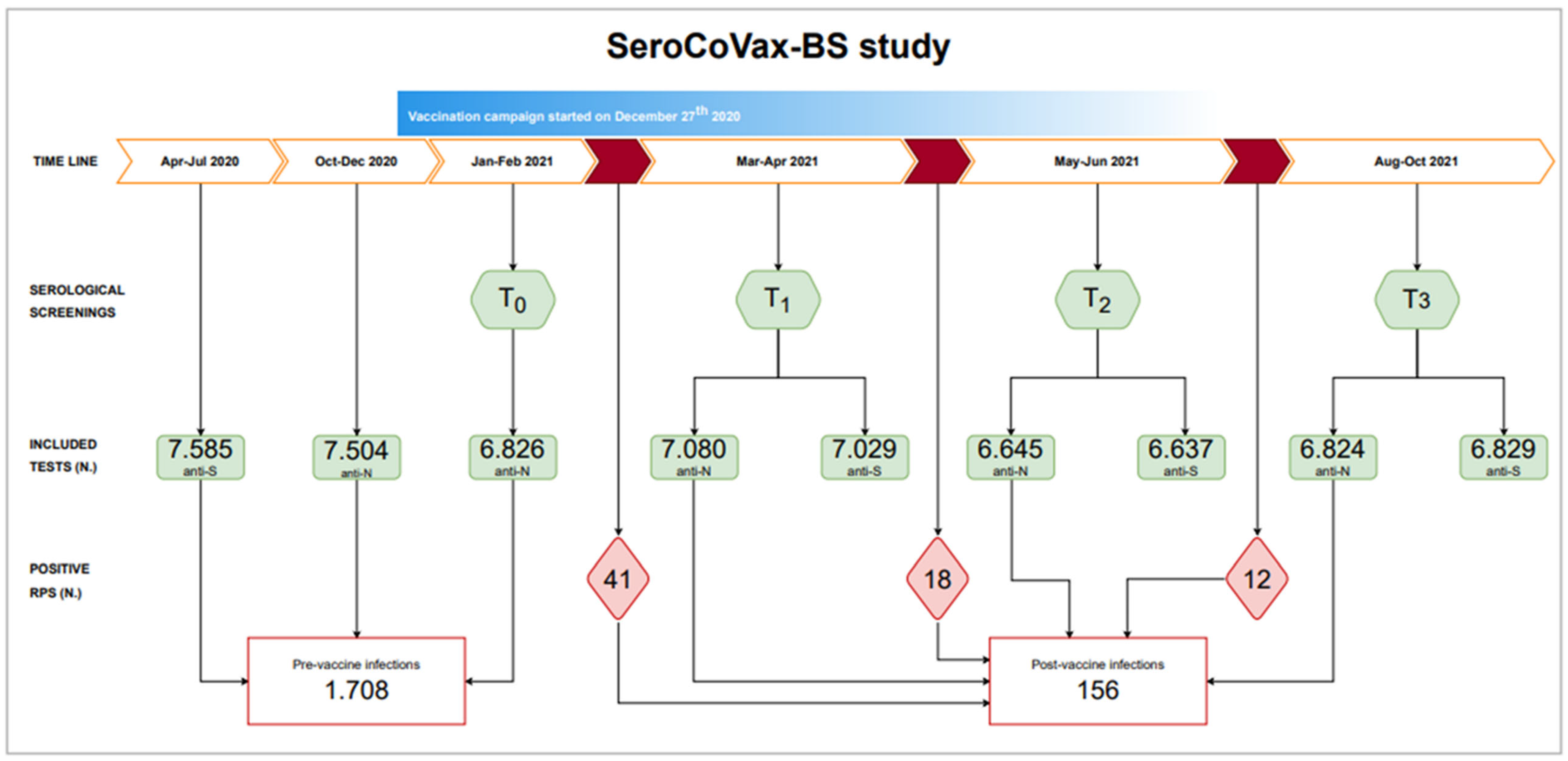
2.1. Study Design
2.2. Cohort
2.3. Patient and Public Involvement
2.4. Serological Assays
2.5. Anti-SARS-CoV-2 T-Cell Response
2.6. Statistical Analysis
3. Results
3.1. Epidemiologic Evidence of Pre-Vaccine SARS-CoV-2 Infections
3.2. Anti-N Antibody Titres
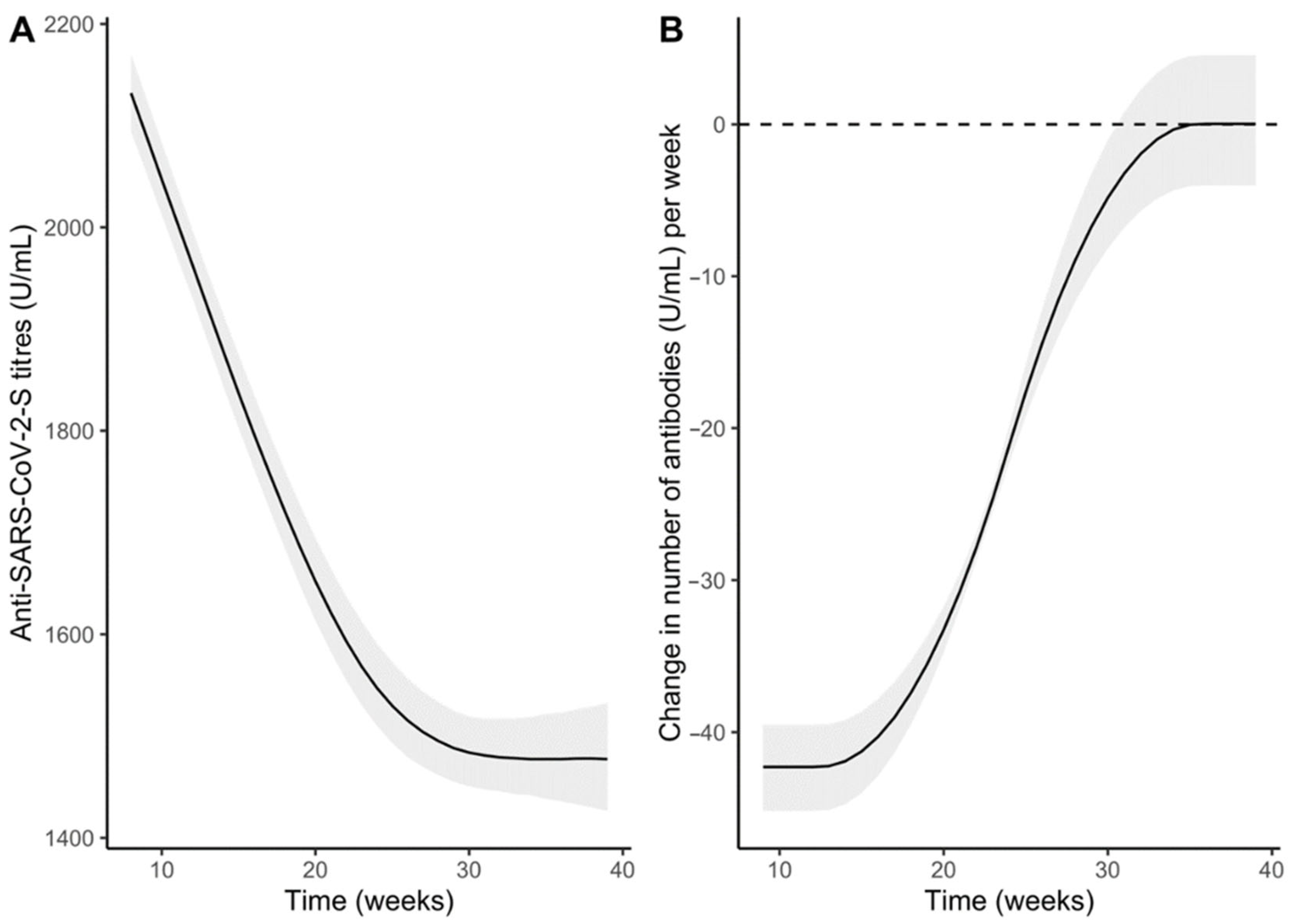
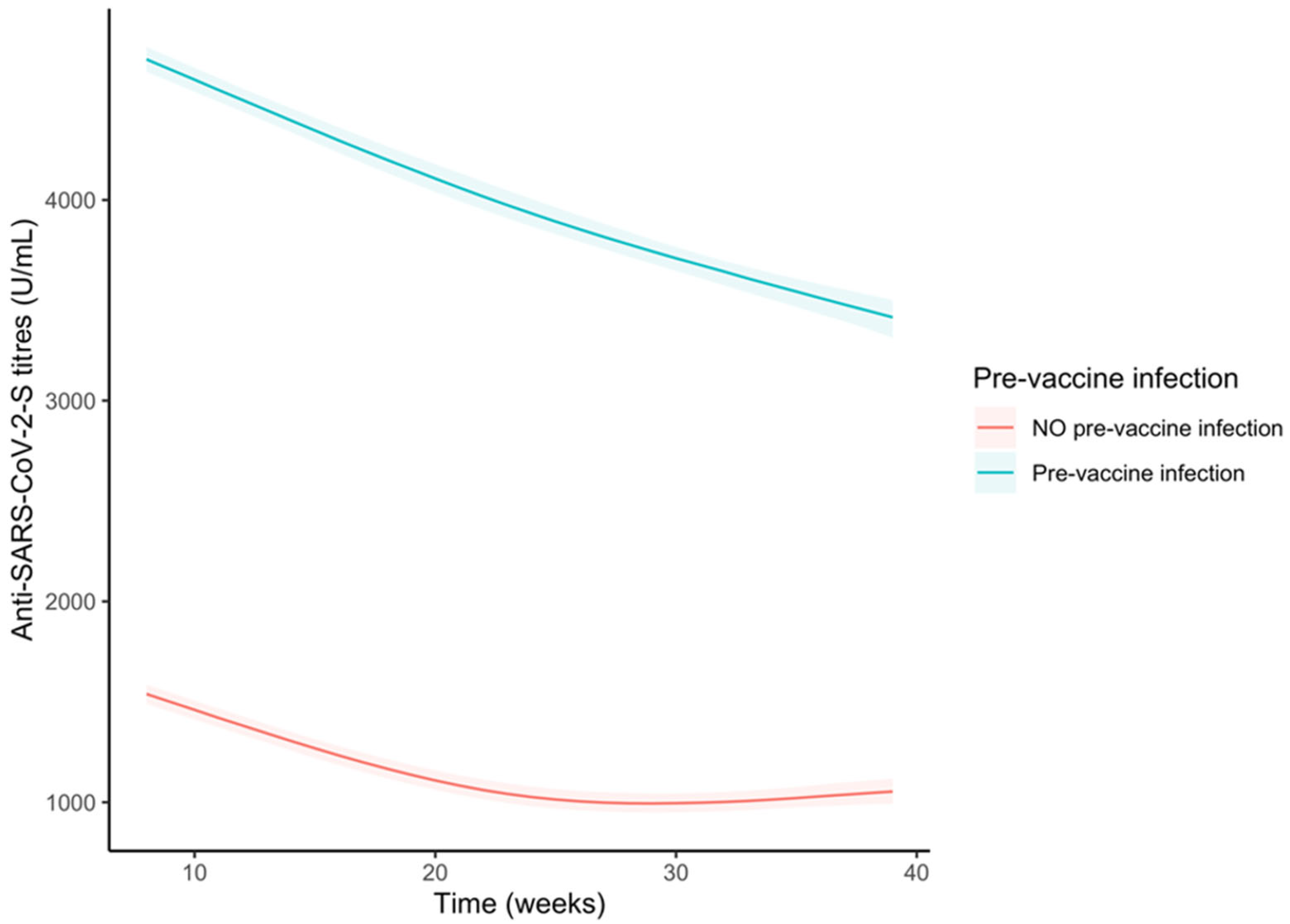
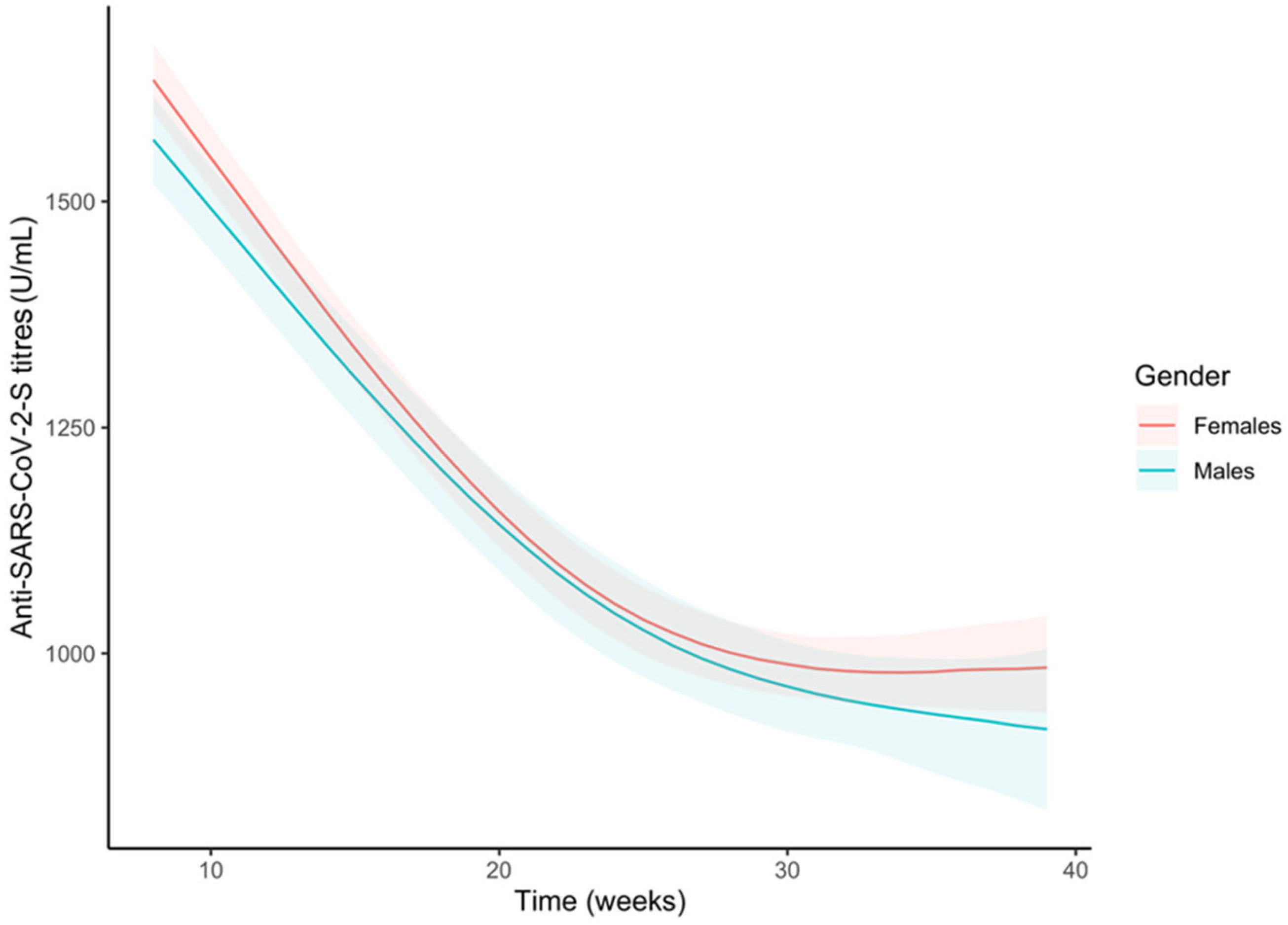
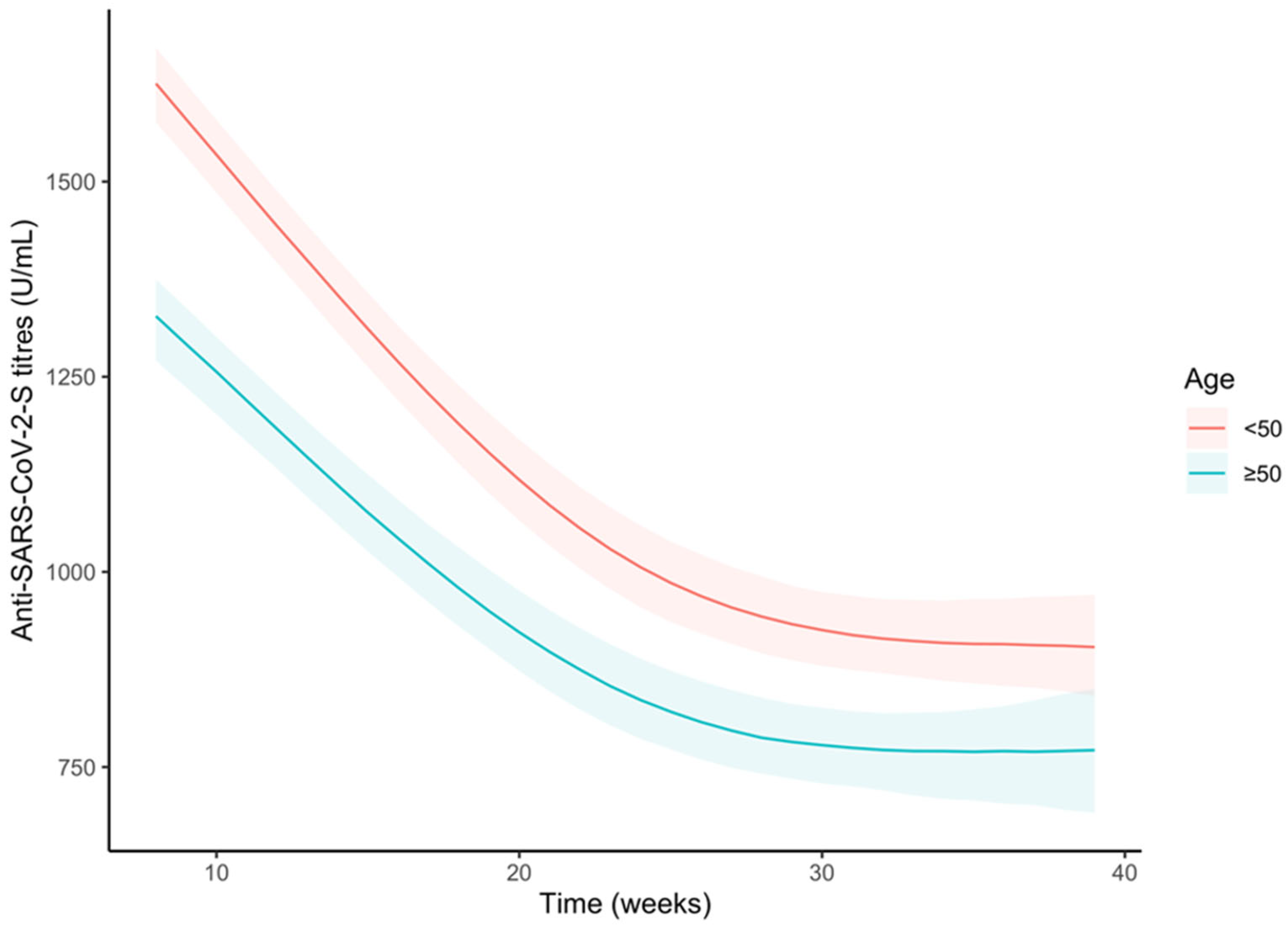
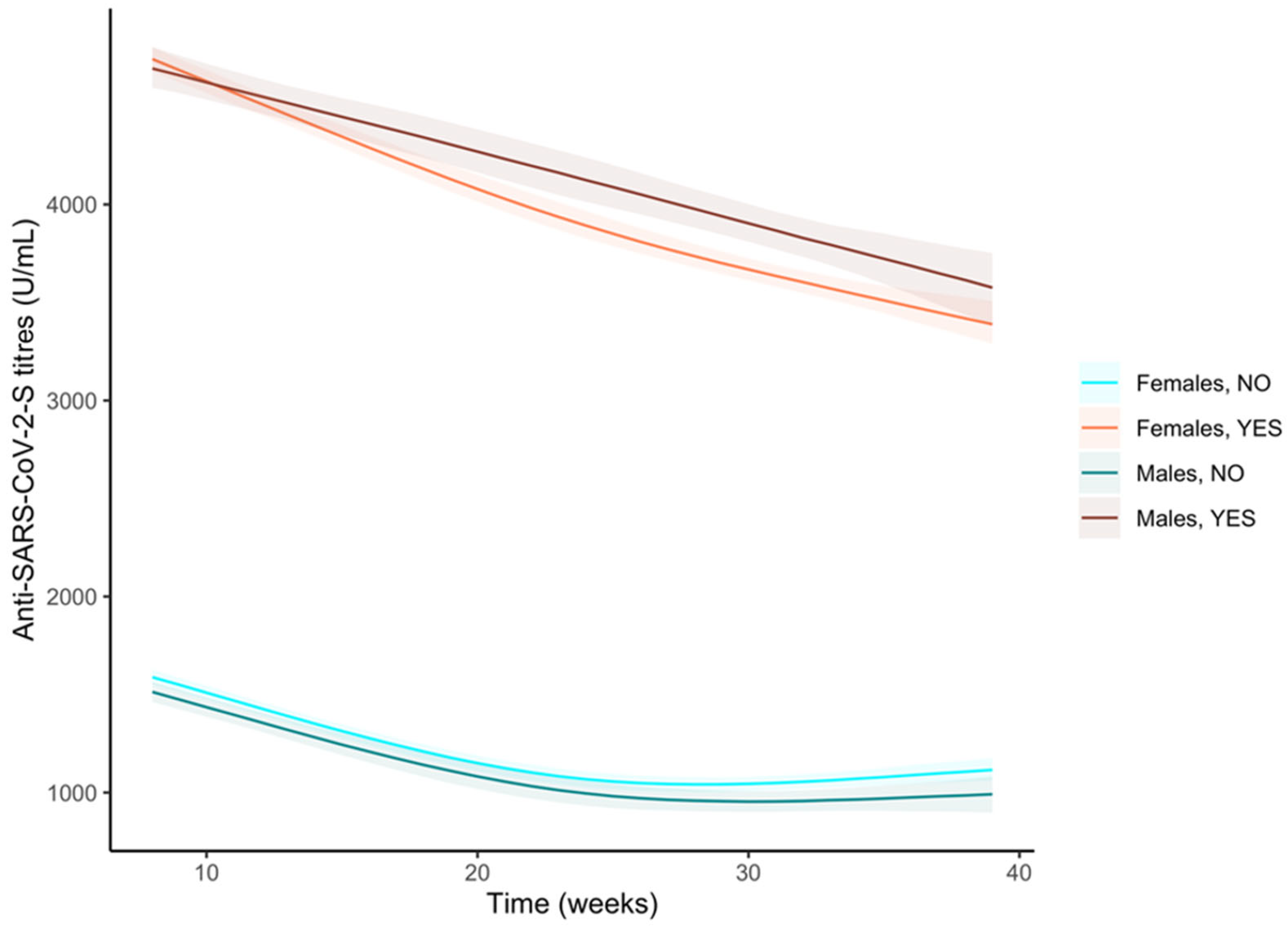
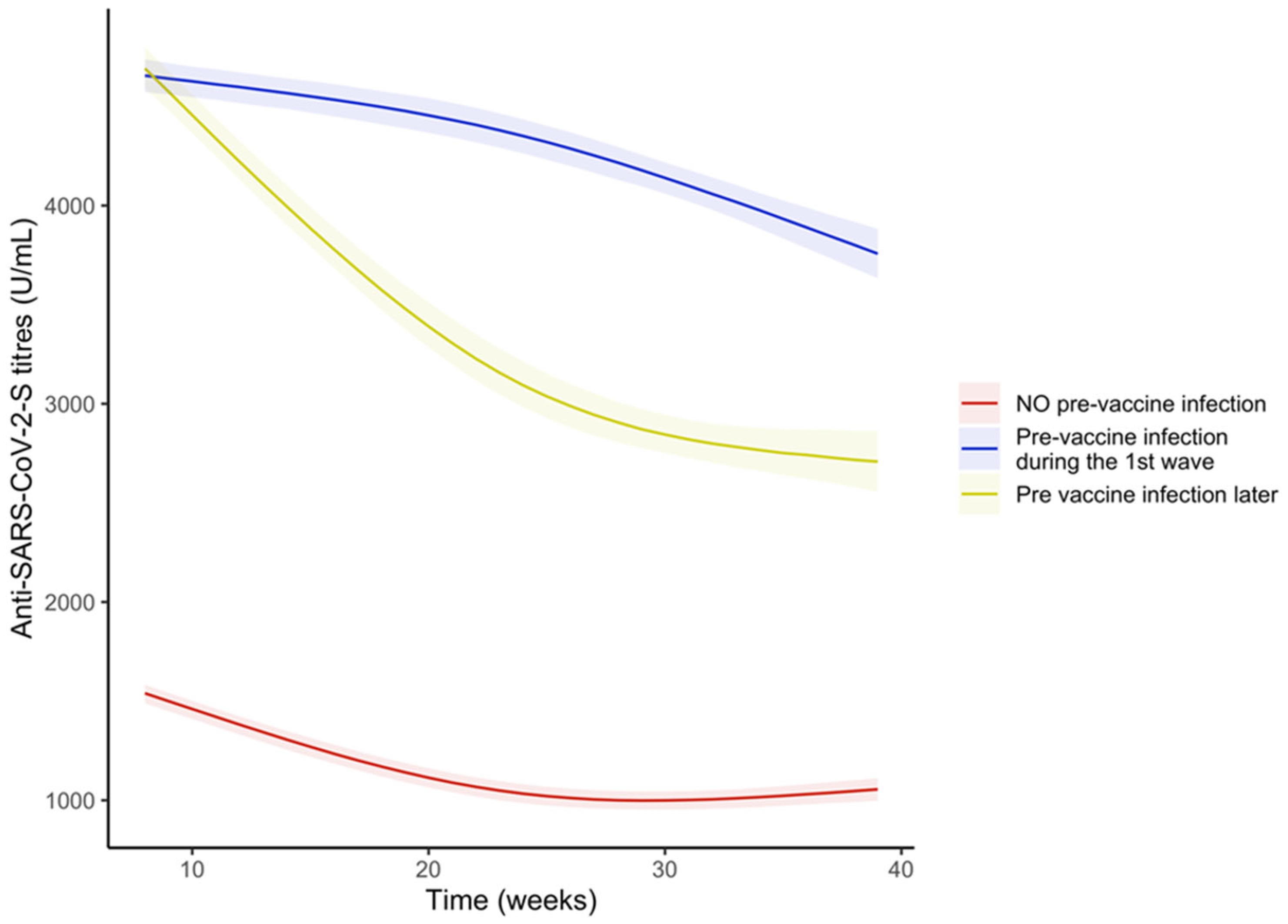
3.3. Anti-S Antibody Titres
3.4. Anti-SARS-CoV-2 T-Cell Response in Vaccinated Seronegative Subjects
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lamb, Y.N. BNT162b2 mRNA COVID-19 Vaccine: First Approval. Drugs 2021, 81, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Huang, H.; Ju, J. Impact of vaccination on the COVID-19 pandemic in US states. Sci. Rep. 2022, 12, 1554. [Google Scholar] [CrossRef]
- Harrison, S.; Walters, B.; Simmons, Z.; Cook, M.; Clark, R. The Effectiveness of Vaccination against Long COVID A Rapid Evidence Briefing. UK Health Security Agency. February 2022. Available online: https://ukhsalibrary.koha-ptfs.co.uk/covid19rapidreviews/ (accessed on 11 May 2022).
- Harris, R.J.; Whitaker, H.J.; Andrews, N.J.; Aiano, F.; Amin-Chowdhury, Z.; Flood, J.; Borrow, R.; Linley, E.; Ahmad, S.; Stapley, L.; et al. Serological surveillance of SARS-CoV-2: Six-month trends and antibody response in a cohort of public health workers. J. Infect. 2021, 82, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.J.; Foulkes, S.; Charlett, A.; Atti, A.; Monk, E.J.; Simmons, R.; Wellington, E.; Cole, M.J.; Saei, A.; Oguti, B.; et al. SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: A large, multicentre, prospective cohort study (SIREN) [published correction appears in Lancet. 8 May 2021, 397,1710]. Lancet 2021, 397, 1459–1469. [Google Scholar] [CrossRef] [PubMed]
- Harvey, R.A.; Rassen, J.A.; Kabelac, C.A.; Turenne, W.; Leonard, S.; Klesh, R.; Meyer, W.A.; Kaufman, H.W.; Anderson, S.; Cohen, O.; et al. Association of SARS-CoV-2 Seropositive Antibody Test with Risk of Future Infection. JAMA Intern. Med. 2021, 181, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Letizia, A.G.; Ge, Y.; Vangeti, S.; Goforth, C.; Weir, D.L.; Kuzmina, N.A.; Balinsky, C.A.; Chen, H.W.; Ewing, D.; Soares-Schanoski, A.; et al. SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: A prospective cohort study. Lancet Respir. Med. 2021, 9, 712–720. [Google Scholar] [CrossRef]
- Available online: https://statistichecoronavirus.it/coronavirus-italia/coronavirus-lombardia/dettaglio/31-12-2020/ (accessed on 11 May 2022).
- Comelli, A.; Focà, E.; Sansone, E.; Tomasi, C.; Albini, E.; Quiros-Roldan, E.; Tomasoni, L.R.; Sala, E.; Bonfanti, C.; Caccuri, F.; et al. Serological Response to SARS-CoV-2 in Health Care Workers Employed in a Large Tertiary Hospital in Lombardy, Northern Italy. Microorganisms 2021, 9, 488. [Google Scholar] [CrossRef]
- Healy, B.; Khan, A.; Metezai, H.; Blyth, I.; Asad, H. The impact of false-positive COVID-19 results in an area of low prevalence. Clin. Med. 2021, 21, e54–e56. [Google Scholar] [CrossRef]
- Bruni, M.; Cecatiello, V.; Diaz-Basabe, A.; Lattanzi, G.; Mileti, E.; Monzani, S.; Pirovano, L.; Rizzelli, F.; Visintin, C.; Bonizzi, G.; et al. Persistence of Anti-SARS-CoV-2 Antibodies in Non-Hospitalized COVID-19 Convalescent Health Care Workers. J. Clin. Med. 2020, 9, 3188. [Google Scholar] [CrossRef]
- Krutikov, M.; Palmer, T.; Tut, G.; Fuller, C.; Azmi, B.; Giddings, R.; Shrotri, M.; Kaur, N.; Sylla, P.; Lancaster, T.; et al. Prevalence and duration of detectable SARS-CoV-2 nucleocapsid antibodies in staff and residents of long-term care facilities over the first year of the pandemic (VIVALDI study): Prospective cohort study in England. Lancet Healthy Longev. 2022, 3, e13–e21. [Google Scholar] [CrossRef]
- Sansone, E.; Sala, E.; Tiraboschi, M.; Albini, E.; Lombardo, M.; Indelicato, A.; Rosati, C.; Boniotti, M.B.; Castelli, F.; De Palma, G. Effectiveness of BNT162b2 Vaccine Against SARS-CoV-2 Among Healthcare Workers: Effectiveness of HCWs Vaccination Against SARS-CoV-2. Med. Lav. 2021, 112, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Pani, A.; Cento, V.; Vismara, C.; Campisi, D.; Di Ruscio, F.; Romandini, A.; Senatore, M.; Schenardi, P.A.; Gagliardi, O.M.; Giroldi, S.; et al. The results of the RENAISSANCE Study: Response to BNT162b2 COVID-19 vacciNe-short- And long-term Immune valuati valuation in health Care workErs. Mayo Clin. Proc. 2021, 96, 2966–2979. [Google Scholar] [CrossRef] [PubMed]
- Centers for diseases control and Prevention-COVID-19 Data Surveillance. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html (accessed on 6 June 2022).
- L’Huillier, A.G.; Meyer, B.; Andrey, D.O.; Arm-Vernez, I.; Baggio, S.; Didierlaurent, A.; Eberhardt, C.S.; Eckerle, I.; Grasset-Salomon, C.; Huttner, A.; et al. Antibody persistence in the first 6 months following SARS-CoV-2 infection among hospital workers: A prospective longitudinal study. Clin. Microbiol. Infect. 2021, 27, 784.e1–784.e8. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Bensliman, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef]
- Sansone, E.; Sala, E.; Tiraboschi, M.; Albini, E.; Lombardo, M.; Indelicato, A.; Rosati, C.; Boniotti, M.B.; Castelli, F.; De Palma, G. Effectiveness of BNT162b2 vaccine against the B.1.1.7 variant of SARS-CoV-2 among healthcare workers in Brescia. Italy J. Infect. 2021, 83, e17–e18. [Google Scholar] [CrossRef]
- Oertelt-Prigione, S. The influence of sex and gender on the immune response. Autoimmun. Rev. 2012, 11, A479–A485. [Google Scholar] [CrossRef]
- Furman, D.; Hejblum, B.P.; Simon, N.; Jojic, V.; Dekker, C.L.; Thiébaut, R.; Tibshirani, R.J.; Davis, M.M. Systems analysis of sex differences reveals an immunosuppressive role for testosterone in the response to influenza vaccination. Proc. Natl. Acad. Sci. USA 2014, 111, 869–874. [Google Scholar] [CrossRef] [Green Version]
- Sankaran-Walters, S.; Macal, M.; Grishina, I.; Nagy, L.; Goulart, L.; Coolidge, K.; Li, J.; Fenton, A.; Williams, T.; Miller, M.K.; et al. Sex differences matter in the gut: Effect on mucosal immune activation and inflammation. Biol. Sex Differ. 2013, 4, 10. [Google Scholar] [CrossRef] [Green Version]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and Gender Differences in the Outcomes of Vaccination over the Life Course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef] [PubMed]
- Sansone, E.; Sala, E.; Albini, E.; Tiraboschi, M.; Cipriani, L.; De Palma, G. Effectiveness of a digital data gathering system to manage the first pandemic wave among healthcare workers in a main European coronavirus disease 2019 (COVID-19) tertiary-care hospital. Antimicrob. Steward. Healthc. Epidemiol. 2022, 2, e66. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N. | Pre-Vaccine Infection Before T0 (N = 1708) | p Value * | OR (95% CI) ** | p Value ** |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 2404 | 493 (20.5%) | 0.278 | 1 (reference) | 0.002 |
| Female | 6244 | 1215 (19.5%) | 0.83 (0.73–0.93) | ||
| Age | |||||
| over 60 years | 730 | 122 (16.7%) | <0.0001 | 1 (reference) | |
| 50–59 years | 2659 | 520 (19.6%) | 1.13 (0.91–1.41) | 0.267 | |
| 40–49 years | 1992 | 397 (19.9%) | 1.14 (0.91–1.43) | 0.267 | |
| 30–39 years | 1845 | 328 (17.8%) | 1.07 (0.85–1.35) | 0.554 | |
| 20–29 years | 1422 | 341 (24.0%) | 1.57(1.24–1.98) | <0.001 | |
| Job title | |||||
| Administrative | 885 | 140 (15.8%) | <0.0001 | 1 (reference) | |
| Technician | 656 | 128 (19.5%) | 1.28 (0.98–1.67) | 0.073 | |
| Other HCW | 1500 | 323 (21.5%) | 1.49 (1.20 1.86) | <0.001 | |
| Nurse | 2648 | 615 (23.2%) | 1.58 (1.29 1.94) | <0.001 | |
| Physician | 2428 | 393 (16.2%) | 0.95 (0.76–1.18) | 0.613 | |
| External workers | 531 | 109 (20.5%) | 1.30 (0.98 1.72) | 0.067 |
| Variables | T1 (N = 7029) | T2 (N = 6637) | T3 (N = 6829) | p |
|---|---|---|---|---|
| Overall | 1458 (774–3063) | 1103 (609–2171) | 792 (428–1664) | <0.001 |
| Age groups | <0.001 | |||
| 20–29 years | 2300.5 (1355–5000) | 1770 (1121–3582) | 1244 (779–2482) | |
| 30–39 years | 1660 (959–3165) | 1216 (733–2249) | 858 (492–1709) | |
| 40–49 years | 1298.5 (702–2818) | 980 (563–1964) | 713 (398–1543) | |
| 50–59 years | 1238 (665–2566) | 950 (513–1862) | 669 (356–1427) | |
| over 60 years | 1034 (561–2173) | 763.1 (433–1535) | 551 (305–1108) | |
| Pre-vaccine SARS-CoV-2 infection | <0.001 | |||
| Yes | 5000 (5000–5000) | 5000 (3781–5000) | 4059 (2016–5000) | |
| No | 1157 (671–1900) | 896 (529–1435) | 631 (369–1078) | |
| Gender | Age | Disease | Immunosuppressive Drugs | T Cell Assay |
|---|---|---|---|---|
| Male | 45 | Transplant recipient | Unspecified | Negative |
| Male | 55 | Acute lymphoblastic leukemia; Transplant recipient | Unspecified | Negative |
| Male | 57 | Transplant recipient | Unspecified | Negative |
| Female | 31 | Wegener granulomatosis | Rituximab, prednisone | Positive |
| Female | 47 | Multiple Sclerosis | Ocrelizumab | Positive |
| Female | 52 | Neuromyelitis optica | Rituximab | Positive |
| Female | 47 | Transplant recipient | Unspecified | Not performed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sansone, E.; Bonfanti, C.; Sala, E.; Renzetti, S.; Terlenghi, L.; Matteelli, A.; Tiraboschi, M.M.; Pedrazzi, T.; Lombardo, M.; Rossi, C.; et al. Immune Responses to SARS-CoV-2 Infection and Vaccine in a Big Italian COVID-19 Hospital: An 18-Month Follow-Up. Vaccines 2023, 11, 8. https://doi.org/10.3390/vaccines11010008
Sansone E, Bonfanti C, Sala E, Renzetti S, Terlenghi L, Matteelli A, Tiraboschi MM, Pedrazzi T, Lombardo M, Rossi C, et al. Immune Responses to SARS-CoV-2 Infection and Vaccine in a Big Italian COVID-19 Hospital: An 18-Month Follow-Up. Vaccines. 2023; 11(1):8. https://doi.org/10.3390/vaccines11010008
Chicago/Turabian StyleSansone, Emanuele, Carlo Bonfanti, Emma Sala, Stefano Renzetti, Luigina Terlenghi, Alberto Matteelli, Mara Maria Tiraboschi, Tatiana Pedrazzi, Massimo Lombardo, Camillo Rossi, and et al. 2023. "Immune Responses to SARS-CoV-2 Infection and Vaccine in a Big Italian COVID-19 Hospital: An 18-Month Follow-Up" Vaccines 11, no. 1: 8. https://doi.org/10.3390/vaccines11010008