
COVID-19 Vaccination Is Not Associated with Psychiatric Adverse Events: A Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Searching Strategy
2.2. Study Selection
2.3. Types of Exposures and Outcomes
2.4. Measures
2.5. Types of Moderators
2.6. Quality Assessment
2.7. Statistical Analysis
2.8. Assessment of Heterogeneity
2.9. Assessment of Publication Bias
3. Results
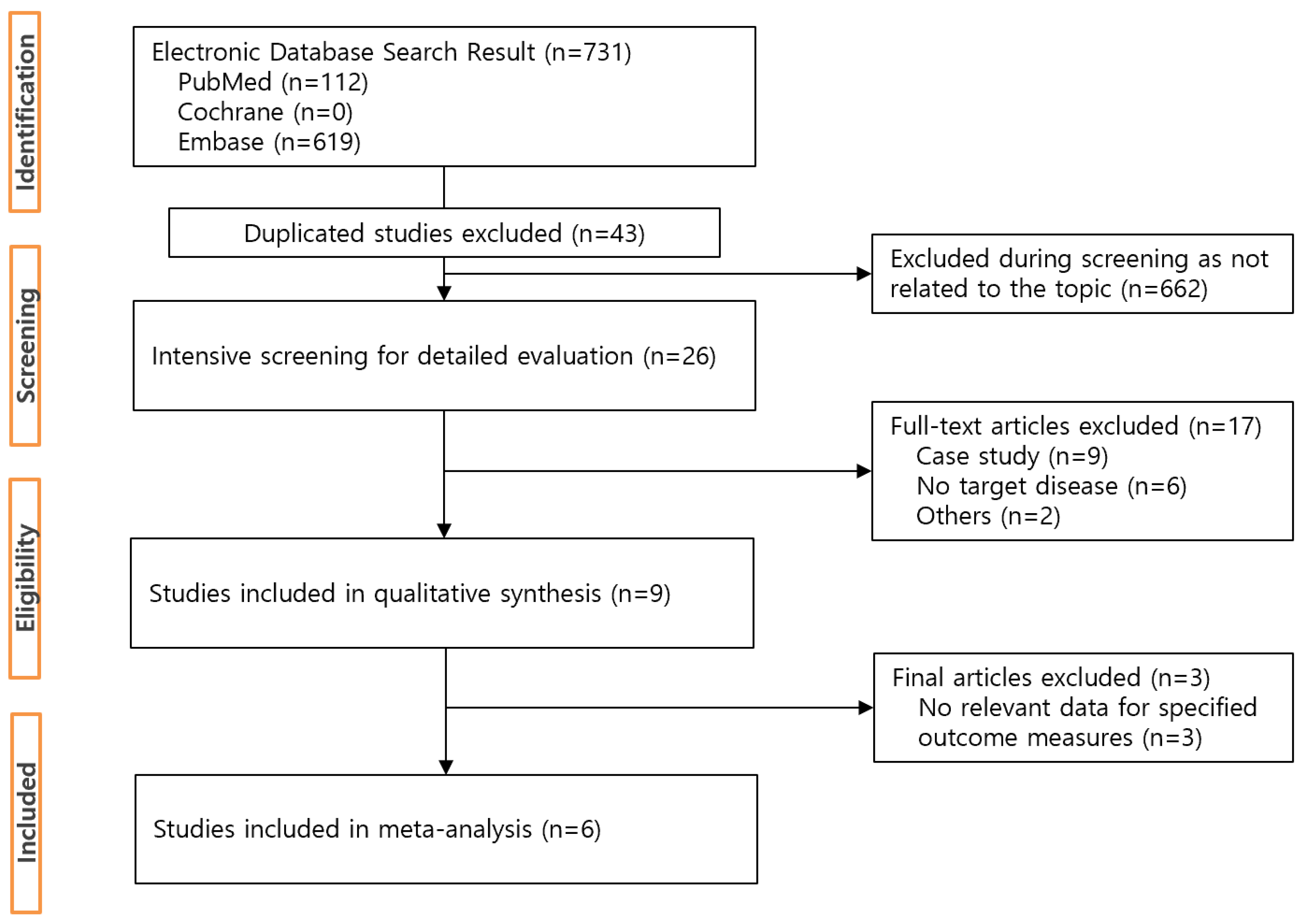
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Quality Assessment
3.4. Outcome Findings
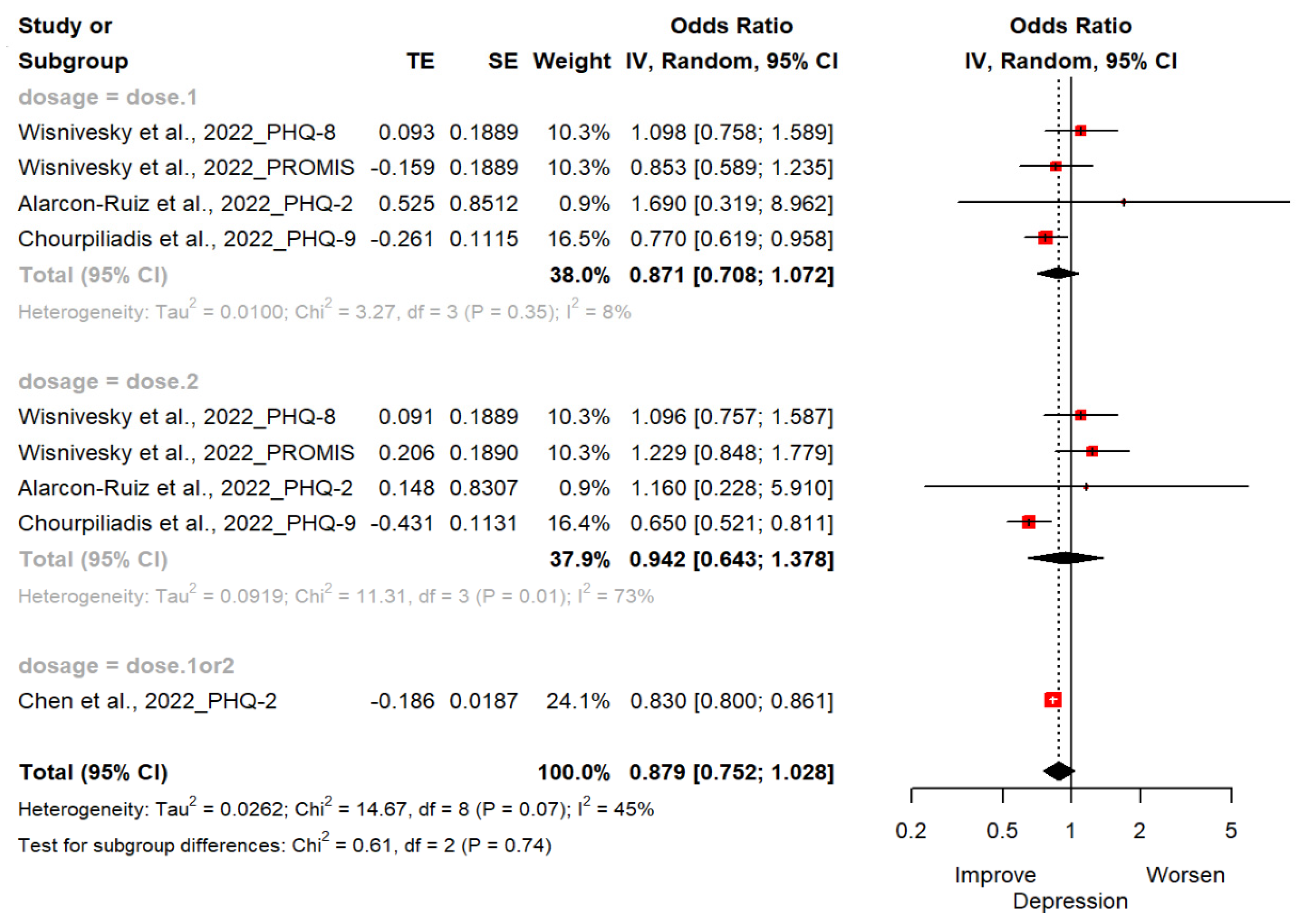
3.4.1. Depression
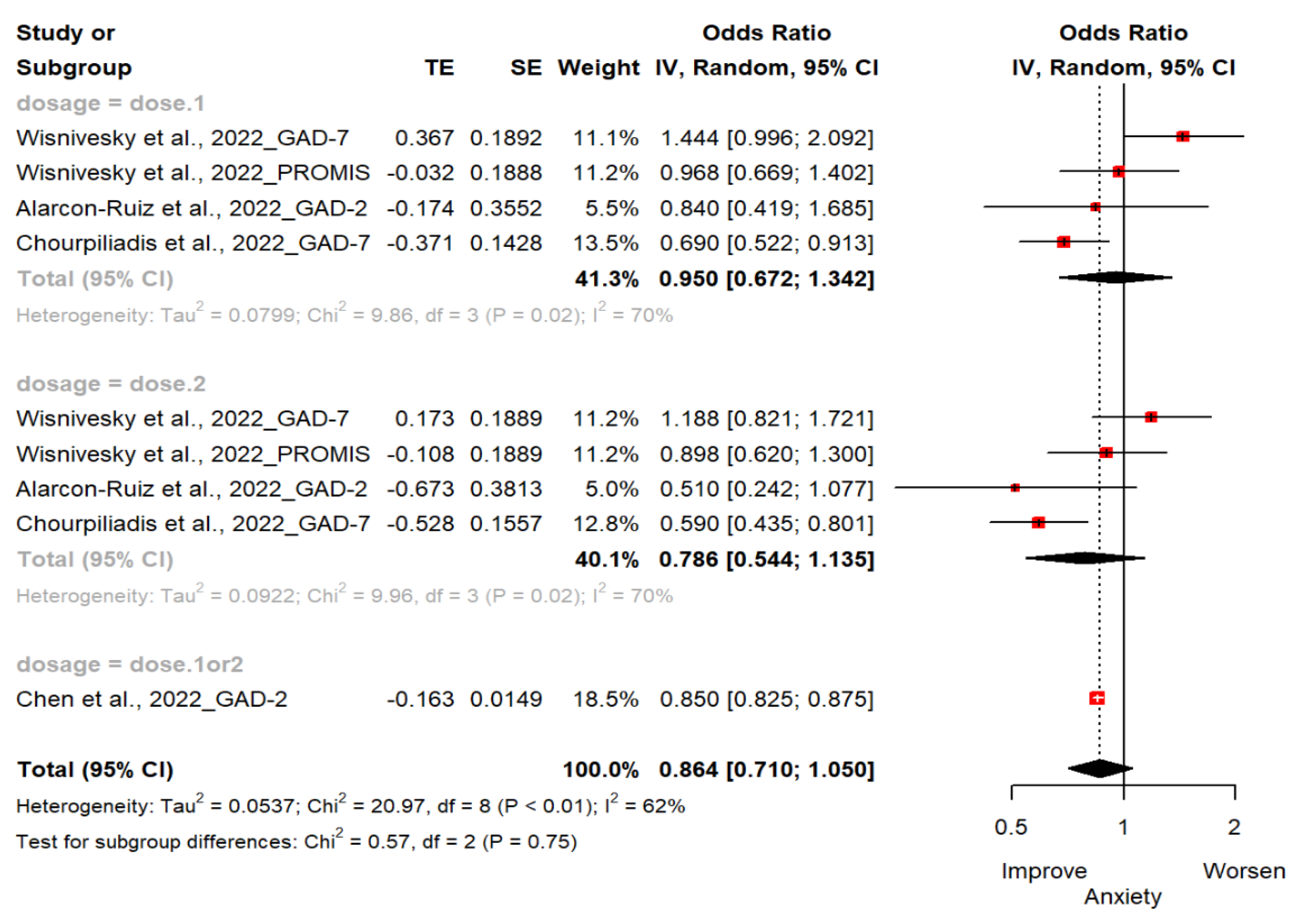
3.4.2. Anxiety
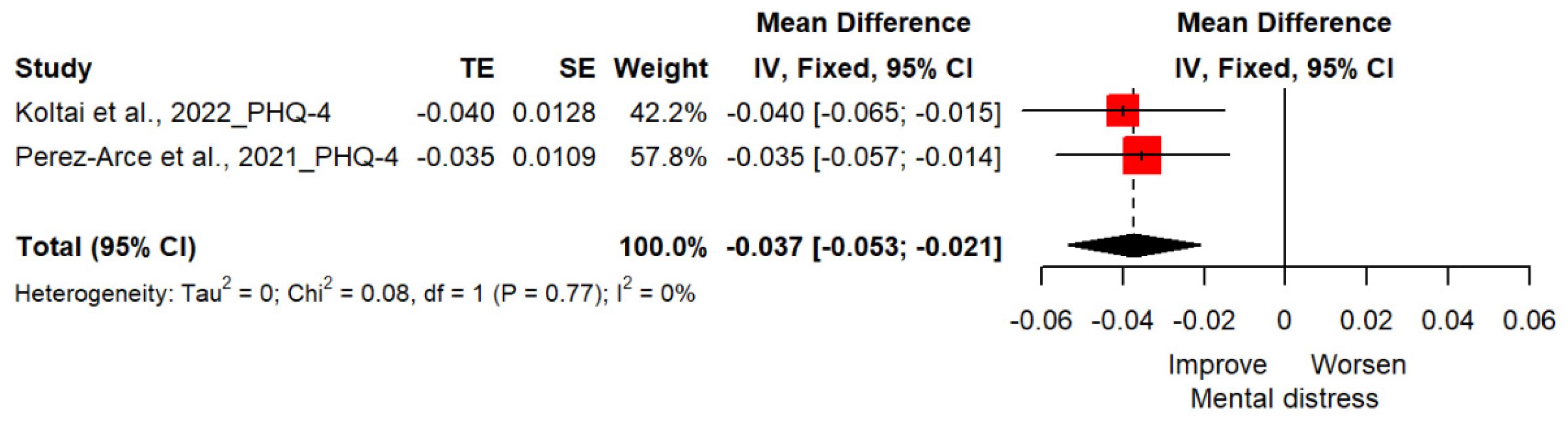
3.4.3. Distress
3.5. Moderator Analysis
3.5.1. Depression
3.5.2. Anxiety
3.6. Assessment of Heterogeneity
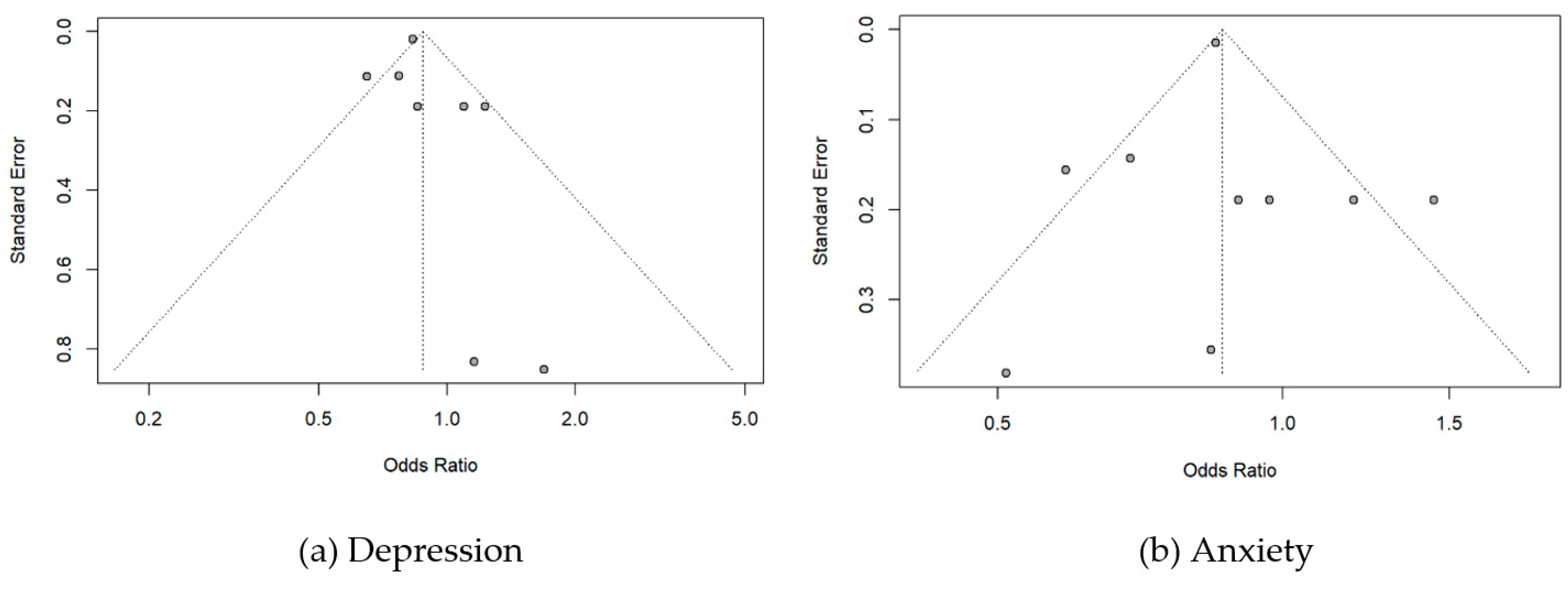
3.7. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://COVID19.who.int (accessed on 1 November 2022).
- Graham, B.S. Rapid COVID-19 vaccine development. Science 2020, 368, 945–946. [Google Scholar] [CrossRef] [PubMed]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 vaccines at pandemic speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Al Khames Aga, Q.A.; Alkhaffaf, W.H.; Hatem, T.H.; Nassir, K.F.; Batineh, Y.; Dahham, A.T.; Shaban, D.; Al Khames Aga, L.A.; Agha, M.Y.; Traqchi, M. Safety of COVID-19 vaccines. J. Med. Virol. 2021, 93, 6588–6594. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, I.; Faheem, A.; Padhy, S.K.; Menon, V. Psychiatric adverse reactions to COVID-19 vaccines: A rapid review of published case reports. Asian J. Psychiatry 2022, 71, 103129. [Google Scholar] [CrossRef] [PubMed]
- Perez-Lloret, S.; Petrovsky, N.; Alami, A.; Crispo, J.A.; Mattison, D.; Otero-Losada, M.; Capani, F.; Krewski, D. Disproportionality analysis of adverse neurological and psychiatric reactions with the ChAdOx1 (Oxford-AstraZeneca) and BNT162b2 (Pfizer-BioNTech) COVID-19 vaccines in the United Kingdom. medRxiv 2021. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- CDC. Myocarditis and Pericarditis After mRNA COVID-19 Vaccination. Children 2021, 8, 607. [Google Scholar] [CrossRef]
- Honigsbaum, M. “An inexpressible dread”: Psychoses of influenza at fin-de-siècle. Lancet 2013, 381, 988–989. [Google Scholar] [CrossRef]
- Tiller, J.W. Depression and anxiety. Med. J. Aust. 2013, 199, S28–S31. [Google Scholar] [CrossRef]
- Pandey, K.; Thurman, M.; Johnson, S.D.; Acharya, A.; Johnston, M.; Klug, E.A.; Olwenyi, O.A.; Rajaiah, R.; Byrareddy, S.N. Mental health issues during and after COVID-19 vaccine era. Brain Res. Bull. 2021, 176, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talevi, D.; Socci, V.; Carai, M.; Carnaghi, G.; Faleri, S.; Trebbi, E.; di Bernardo, A.; Capelli, F.; Pacitti, F. Mental health outcomes of the CoViD-19 pandemic. Riv. Di Psichiatr. 2020, 55, 137–144. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group*, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, L.; Deng, J.; Min, S.; Peng, L.; Chen, Q. Ketamine in electroconvulsive therapy for depressive disorder: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 104, 144–156. [Google Scholar] [CrossRef]
- Thombs, B.D.; Benedetti, A.; Kloda, L.A.; Levis, B.; Nicolau, I.; Cuijpers, P.; Gilbody, S.; Ioannidis, J.; McMillan, D.; Patten, S.B. The diagnostic accuracy of the Patient Health Questionnaire-2 (PHQ-2), Patient Health Questionnaire-8 (PHQ-8), and Patient Health Questionnaire-9 (PHQ-9) for detecting major depression: Protocol for a systematic review and individual patient data meta-analyses. Syst. Rev. 2014, 3, 124. [Google Scholar]
- Alarcon-Ruiz, C.A.; Romero-Albino, Z.; Soto-Becerra, P.; Huarcaya-Victoria, J.; Runzer-Colmenares, F.M.; Romani-Huacani, E.; Villarreal-Zegarra, D.; Maguiña, J.L.; Apolaya-Segura, M.; Cuba-Fuentes, S. Effects of vaccination against COVID-19 on the emotional health of Peruvian older adults. medRxiv 2022. [Google Scholar] [CrossRef]
- Chen, S.; Aruldass, A.R.; Cardinal, R.N. Mental health outcomes after SARS-CoV-2 vaccination in the United States: A national cross-sectional study. J. Affect. Disord. 2022, 298, 396–399. [Google Scholar] [CrossRef]
- Chourpiliadis, C.; Lovik, A.; Kähler, A.K.; Valdimarsdóttir, U.A.; Frans, E.M.; Nyberg, F.; Sullivan, P.F.; Fang, F. Short-term improvement of mental health after a COVID-19 vaccination. medRxiv 2022. [Google Scholar] [CrossRef]
- Wisnivesky, J.P.; Govindarajulu, U.; Bagiella, E.; Goswami, R.; Kale, M.; Campbell, K.N.; Meliambro, K.; Chen, Z.; Aberg, J.A.; Lin, J.J. Association of Vaccination with the Persistence of Post-COVID Symptoms. J. Gen. Intern. Med. 2022, 37, 1748–1753. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Löwe, B. An ultra-brief screening scale for anxiety and depression: The PHQ–4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [PubMed] [Green Version]
- Perez-Arce, F.; Angrisani, M.; Bennett, D.; Darling, J.; Kapteyn, A.; Thomas, K. COVID-19 vaccines and mental distress. PLoS ONE 2021, 16, e0256406. [Google Scholar] [CrossRef] [PubMed]
- Koltai, J.; Raifman, J.; Bor, J.; McKee, M.; Stuckler, D. COVID-19 vaccination and mental health: A difference-in-difference analysis of the understanding America study. Am. J. Prev. Med. 2022, 62, 679–687. [Google Scholar] [CrossRef]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef]
- Hays, R.D.; Spritzer, K.L.; Schalet, B.D.; Cella, D. PROMIS®-29 v2. 0 profile physical and mental health summary scores. Qual. Life Res. 2018, 27, 1885–1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Newcastle-Ottawa Quality Assessment Scale Cohort Studies; University of Ottawa: Ottawa, ON, Canada, 2014. [Google Scholar]
- Singh, G.P.; Jaswal, S. COVID vaccination and mental health: An Indian perspective. Asian J. Psychiatry 2022, 67, 102950. [Google Scholar] [CrossRef]
- Nguyen, M. The Psychological Benefits of COVID-19 Vaccination. Advances in Public Health 2021, 2021, 1718800. [Google Scholar] [CrossRef]
- Bergman, Y.S.; Palgi, Y.; Ben-David, B.; Bodner, E. COVID-19 Vaccinations and Anxiety in Middle-Aged and Older Jews and Arabs in Israel: The Moderating Roles of Ethnicity and Subjective Age. J. Appl. Gerontol. 2022, 41, 1843–1850. [Google Scholar] [CrossRef]
- Badami, Z.A.; Mustafa, H.; Maqsood, A.; Aijaz, S.; Altamash, S.; Lal, A.; Saeed, S.; Ahmed, N.; Yousofi, R.; Heboyan, A. Comparison of General Anxiety among Healthcare Professionals before and after COVID-19 Vaccination. Vaccines 2022, 10, 2076. [Google Scholar] [CrossRef]
- Sasaki, N.; Kuroda, R.; Tsuno, K.; Imamura, K.; Kawakami, N. COVID-19 vaccination did not improve employee mental health: A prospective study in an early phase of vaccination in Japan. Neuropsychopharmacol. Rep. 2022, 42, 230–232. [Google Scholar] [CrossRef]
- Williams, K.; Frech, A.; Carlson, D.L. Marital status and mental health. In A Handbook for the Study of Mental Health: Social Contexts, Theories, and Systems; Cambridge University Press: Cambridge, UK, 2010; Volume 2, pp. 306–320. [Google Scholar]
- Umberson, D.; Thomeer, M.B.; Williams, K. Family status and mental health: Recent advances and future directions. In Handbook of the Sociology of Mental Health; Springer: Dordrecht, The Netherlands, 2013; pp. 405–431. [Google Scholar]
- Gutiérrez-Rojas, L.; Porras-Segovia, A.; Dunne, H.; Andrade-González, N.; Cervilla, J.A. Prevalence and correlates of major depressive disorder: A systematic review. Braz. J. Psychiatry 2020, 42, 657–672. [Google Scholar] [CrossRef]
- Buckman, J.E.; Saunders, R.; Stott, J.; Arundell, L.-L.; O’Driscoll, C.; Davies, M.R.; Eley, T.C.; Hollon, S.D.; Kendrick, T.; Ambler, G. Role of age, gender and marital status in prognosis for adults with depression: An individual patient data meta-analysis. Epidemiol. Psychiatr. Sci. 2021, 30, e42. [Google Scholar] [CrossRef] [PubMed]
- Renaud-Charest, O.; Lui, L.M.; Eskander, S.; Ceban, F.; Ho, R.; Di Vincenzo, J.D.; Rosenblat, J.D.; Lee, Y.; Subramaniapillai, M.; McIntyre, R.S. Onset and frequency of depression in post-COVID-19 syndrome: A systematic review. J. Psychiatr. Res. 2021, 144, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Mazza, M.G.; Palladini, M.; Poletti, S.; Benedetti, F. Post-COVID-19 depressive symptoms: Epidemiology, pathophysiology, and pharmacological treatment. CNS Drugs 2022, 36, 681–702. [Google Scholar] [CrossRef] [PubMed]
- Kong, X.; Zheng, K.; Tang, M.; Kong, F.; Zhou, J.; Diao, L.; Wu, S.; Jiao, P.; Su, T.; Dong, Y. Prevalence and factors associated with depression and anxiety of hospitalized patients with COVID-19. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Huang, E.; Zuo, Q.K. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: A meta-analysis. Ann. New York Acad. Sci. 2021, 1486, 90–111. [Google Scholar] [CrossRef]
- McKnight-Eily, L.R.; Okoro, C.A.; Strine, T.W.; Verlenden, J.; Hollis, N.D.; Njai, R.; Mitchell, E.W.; Board, A.; Puddy, R.; Thomas, C. Racial and ethnic disparities in the prevalence of stress and worry, mental health conditions, and increased substance use among adults during the COVID-19 pandemic—United States, April and May 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 162. [Google Scholar] [CrossRef]
- Lee, H.; Singh, G.K. Monthly trends in self-reported health status and depression by race/ethnicity and socioeconomic status during the COVID-19 Pandemic, United States, April 2020–May 2021. Ann. Epidemiol. 2021, 63, 52–62. [Google Scholar] [CrossRef]
- Mann, F.D.; Krueger, R.F.; Vohs, K.D. Personal economic anxiety in response to COVID-19. Personal. Individ. Differ. 2020, 167, 110233. [Google Scholar] [CrossRef]
- Gaynor, T.S.; Wilson, M.E. Social vulnerability and equity: The disproportionate impact of COVID-19. Public Adm. Rev. 2020, 80, 832–838. [Google Scholar] [CrossRef]
- Fordham, M.; Lovekamp, W.E.; Thomas, D.S.; Phillips, B.D. Understanding social vulnerability. Soc. Vulnerability Disasters 2013, 2, 1–29. [Google Scholar]
- Kim, S.J.; Bostwick, W. Social vulnerability and racial inequality in COVID-19 deaths in Chicago. Health Educ. Behav. 2020, 47, 509–513. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Design | Sample Size (Mean Age) | Population (Exposed Cohort, Non-Exposed Cohort) | Follow Up Period | Exposure | Outcome Measurements | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Exposed Cohort | Non-Exposed Cohort | Depression | Anxiety | Distress | ||||||
| Wisnivesky et al., 2022 [21] | USA | prospective cohort | 453 (49.9) | COVID-19 patients (324, 129) | 6 months | COVID-19 vaccinated | COVID-19 unvaccinated | PHQ-8, PROMIS-29 | GAD-7, PROMIS-29 | – |
| Alarcon-Ruiz et al., 2022 [18] | Peru | prospective cohort | 861 (72.2) | older adults in Peru (794, 67) | 1 month | COVID-19 vaccinated | COVID-19 unvaccinated | PHQ-2 | GAD-2 | – |
| Chen et al., 2022 [19] | USA | Cross -sectional | 453,167 (55.0) | adults in USA (236,757, 216,410) | - | COVID-19 vaccinated | COVID-19 unvaccinated | PHQ-2 | GAD-2 | – |
| Chourpiliadis et al., 2022 [20] | Sweden | prospective cohort | 7925 (53.4) | adults in Sweden (7056, 869) | 1 month | COVID-19 vaccinated | COVID-19 unvaccinated | PHQ-9 | GAD-7 | – |
| Koltai et al., 2022 [24] | USA | prospective cohort | 8090 (51.0) | adults in USA (–) | 2 weeks | COVID-19 vaccinated | COVID-19 unvaccinated | – | – | PHQ-4 |
| Perez-Arce et al., 2021 [23] | USA | panel | 8027 (53.8) | adults in USA (1643, 6384) | 2 weeks | COVID-19 vaccinated | COVID-19 unvaccinated | – | – | PHQ-4 |
| □ | □ | Selection | □ | Comparability | Outcome □ | Total Score | Quality Power | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| □ | [A] | [B] | [C] | [D] | □ | [E] | □ | [F] | [G] | [H] | □ | ||
| Wisnivesky et al., 2022 [21] | ★ | ★ | ★ | ★ | □ | ★★ | □ | ★ | ★ | □ | □ | ★★★★★★★★ (8) | Good |
| Alarcon-Ruiz et al., 2022 [18] | ★ | ★ | ★ | □ | ★★ | □ | ★ | ★ | ★ | □ | ★★★★★★★★ (8) | Good | |
| Chen et al., 2022 [19] | ★ | ★ | ★ | □ | ★★ | □ | ★ | ★ | □ | □ | ★★★★★★★ (7) | Good | |
| Chourpiliadis et al., 2022 [20] | ★ | ★ | ★ | □ | ★★ | □ | ★ | ★ | ★ | □ | ★★★★★★★★ (8) | Good | |
| Koltai et al., 2022 [24] | ★ | ★ | ★ | ★ | □ | ★★ | □ | ★ | ★ | □ | □ | ★★★★★★★★ (8) | Good |
| Perez-Arce et al., 2021 [23] | ★ | ★ | ★ | ★ | □ | ★★ | □ | ★ | ★ | □ | □ | ★★★★★★★★ (8) | Good |
| Depression | Anxiety | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | k | Coefficient (95% CI) | OR (95% CI) | p-Value * | p-Value † | k | Coefficient (95% CI) | OR (95% CI) | p-Value * | p-Value † | |
| No. of participants | 9 | −0.00 (−0.00 to 0.00) | 0.679 | 9 | −0.00 (−0.00 to 0.00) | 0.932 | |||||
| Follow up period | 8 | 0.02 (0.01 to 0.03) | 0.001 | 8 | 0.03 (0.01 to 0.04) | <0.001 | |||||
| Age | 0.441 | 0.366 | |||||||||
| >60 | 2 | 1.39 (0.43 to 4.56) | 2 | 0.66 (0.36 to 1.22) | |||||||
| <60 | 7 | 0.87 (0.75 to 1.02) | 7 | 0.89 (0.72 to 1.10) | |||||||
| Female rate | 9 | 0.060 | 9 | 0.006 | |||||||
| >70% | 4 | −1.20 (−2.78 to 0.37) | 0.73 (0.58 to 0.91) | 0.134 | 4 | −2.04 (−3.93 to −0.16) | 0.65 (0.50 to 0.83) | 0.034 | |||
| Others | 5 | 0.95 (0.81 to 1.12) | 5 | 0.99 (0.83 to 1.19) | |||||||
| Race | 0.008 | 0.497 | |||||||||
| White | 3 | −0.92 (−1.48 to −0.35) | 0.78 (0.69 to 0.88) | 0.001 | 3 | 0.36 (−0.17 to 0.88) | 0.77 (0.52 to 1.14) | 0.182 | |||
| Others | 6 | 1.07 (0.88 to 1.30) | 6 | 0.91 (0.70 to 1.16) | |||||||
| Married | 0.038 | 0.017 | |||||||||
| Yes | 2 | 0.71 (0.56 to 0.89) | 2 | 0.64 (0.48 to 0.85) | |||||||
| No | 7 | 0.96 (0.81 to 1.13) | 7 | 0.96 (0.81 to 1.13) | |||||||
| History of COVID-19 | 0.011 | 0.007 | |||||||||
| Yes | 4 | 1.06 (0.87 to 1.29) | 4 | 1.11 (0.88 to 1.39) | |||||||
| No | 5 | 0.78 (0.69 to 0.88) | 5 | 0.73 (0.61 to 0.88) | |||||||
| Measures | 0.015 | 0.791 | |||||||||
| PHQ-2 | 3 | 0.83 (0.78 to 0.88) | GAD-2 | 3 | 0.76 (0.50 to 1.17) | ||||||
| PHQ-8 | 2 | 1.10 (0.84 to 1.43) | GAD-7 | 4 | 0.90 (0.64 to 1.25) | ||||||
| PHQ-9 | 2 | 0.71 (0.60 to 0.83) | PROMIS-29 | 2 | 0.93 (0.58 to 1.51) | ||||||
| PROMIS-29 | 2 | □ | 1.02 (0.79 to 1.33) | □ | □ | □ | □ | □ | □ | □ | □ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-E.; Shim, S.-R.; Youn, J.-H.; Han, H.-W. COVID-19 Vaccination Is Not Associated with Psychiatric Adverse Events: A Meta-Analysis. Vaccines 2023, 11, 194. https://doi.org/10.3390/vaccines11010194
Lee S-E, Shim S-R, Youn J-H, Han H-W. COVID-19 Vaccination Is Not Associated with Psychiatric Adverse Events: A Meta-Analysis. Vaccines. 2023; 11(1):194. https://doi.org/10.3390/vaccines11010194
Chicago/Turabian StyleLee, Sang-Eun, Sung-Ryul Shim, Jung-Hae Youn, and Hyun-Wook Han. 2023. "COVID-19 Vaccination Is Not Associated with Psychiatric Adverse Events: A Meta-Analysis" Vaccines 11, no. 1: 194. https://doi.org/10.3390/vaccines11010194