
Indian Biosimilars and Vaccines at Crossroads–Replicating the Success of Pharmagenerics
 , ,
, , 
Abstract
:1. Introduction
2. History, Scope and Evolution of Biotechnology Companies in India
3. Methodology
4. Global vs. Indian Biotech Endeavors
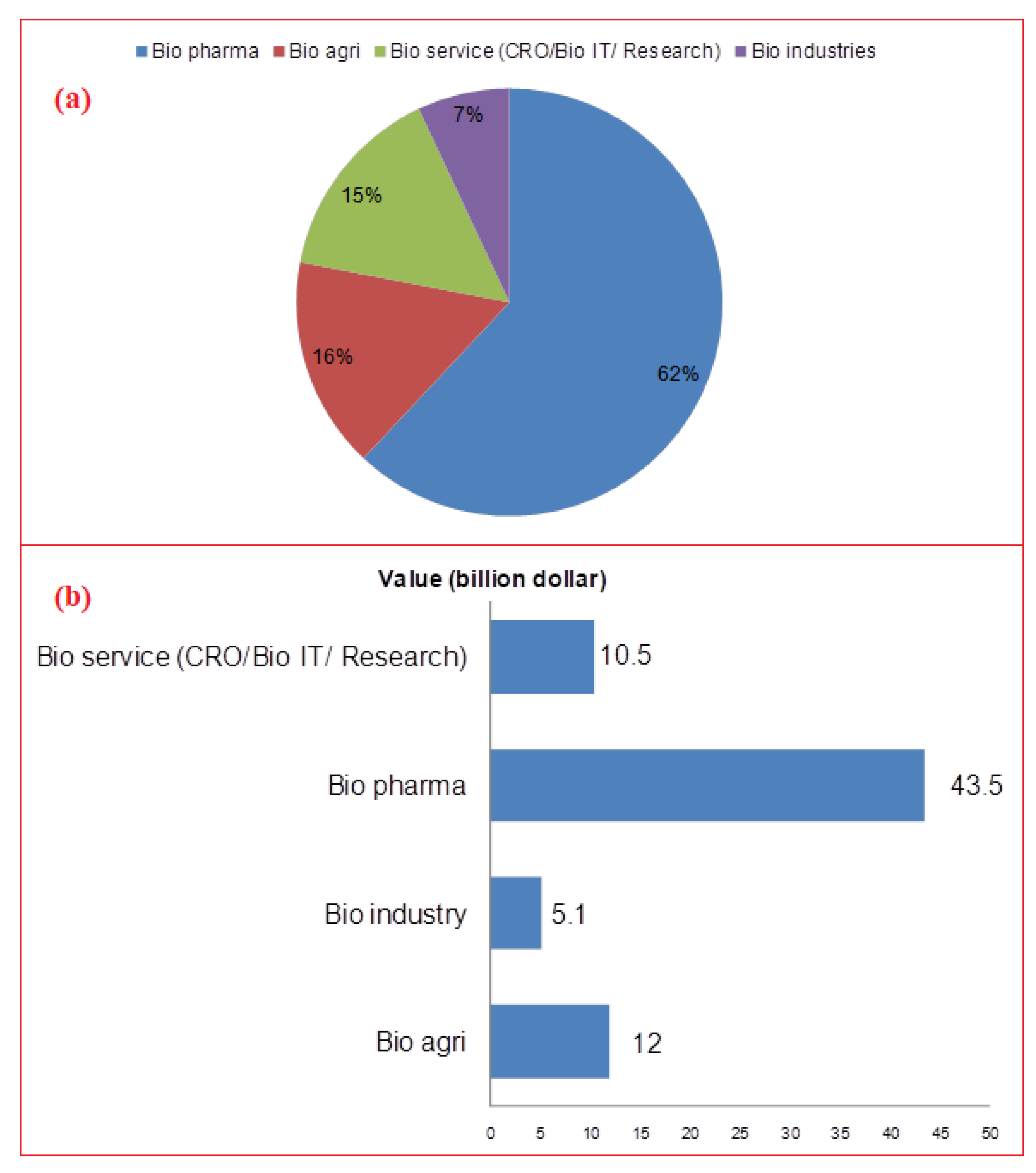
5. Market size and Current Scenario of Indian Biotech Companies in Biopharma Sector
6. Healthcare Scenario, Translational Research—Initiatives, Prospects and Bottlenecks
7. What Ails Indian Biotech Going Global?
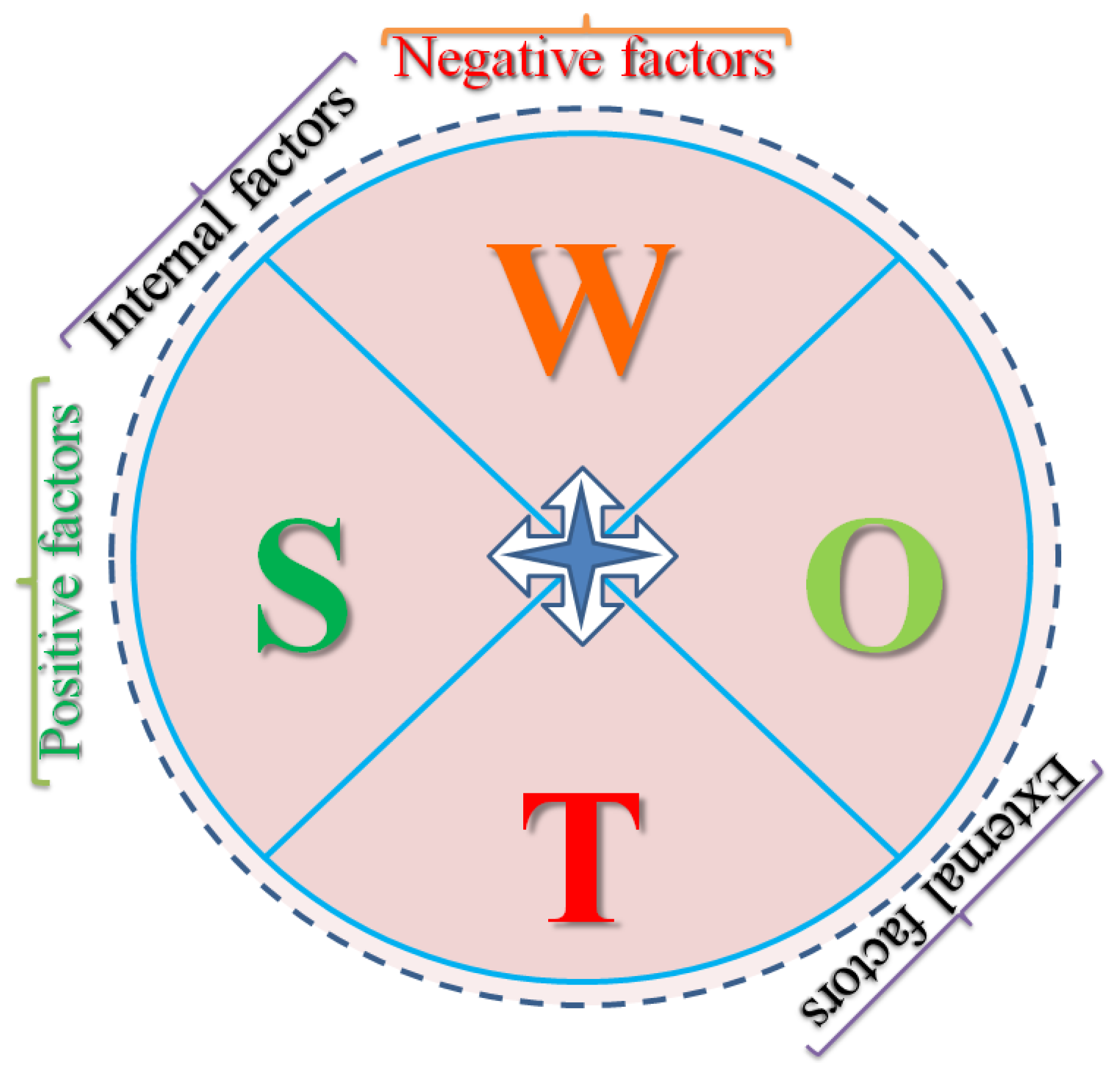
7.1. SWOT Analysis of Indian Biotechnology Industry in General and Biosimilars in Particular
7.2. Lack of Innovation
7.3. Lack of Ventures
7.4. Loose Ignition Grant System
7.5. Lack of Leadership Vision
7.6. Quality Human Resource
7.7. Status of Industry-Academia Partnering
7.8. Mindset Issues—Need to Embrace the State-of-Art Technologies
7.9. Lack of Internal (Industry-Exposed) Expertise
7.10. Budget-Funding
7.11. Market Needs and Response to Competitive Pressures
- 1.
- Interchangeability: FDA needs ‘an interchangeable biological product which is similar to an existing FDA-approved reference product’. This allows substitution of the reference product with the interchangeable biologic by a pharmacist without the interference of the clinician who prescribed the reference biologic [114].
- 2.
- Naming: WHO follows the International Non-proprietary Name (INN) for generic products. Several other countries have adopted their unique naming convention. EU follows INN while Japan adopt INN with BS as suffix, US also follows INN with four-letter suffixes [115].
- 3.
- Labelling: After approval, the insert should clearly indicate whether the data were generated on a similar biologic or innovator product, including differences in characterization and the extent of similarity with the reference biologic on safety, immunogenicity, and efficacy for the awareness of patient and professionals. Moreover, the COOL (country of origin labelling) law applies, since 2003 [116].
7.12. Filling the Gaps in International B2B and B2C Collaborations, and Handholding
7.13. Lack of Diversification
7.14. Regulatory Affairs and IPR
8. Indian Vaccines in the Global Market
9. Visionary Perspective and Conclusion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mounho-Zamora, B. Chapter 6—Regulatory Standards for the Approval of Biosimilar Products: A Global Review. In Nonclinical Development of Novel Biologics, Biosimilars, Vaccines and Specialty Biologics; Elsevier B.V.: London, UK, 2013; pp. 159–184. [Google Scholar] [CrossRef]
- Farhat, F.; Torres, A.; Park, W.; De Lima Lopes, G.; Mudad, R.; Ikpeazu, C.; Aad, S.A. The Concept of Biosimilars: From Characterization to Evolution—A Narrative Review. Oncologist 2018, 23, 346–352. [Google Scholar] [CrossRef] [Green Version]
- Patel, P.K.; King, C.R.; Feldman, S.R. Biologics and biosimilars. J. Dermatol. Treat. 2015, 26, 299–302. [Google Scholar] [CrossRef]
- Singh, G. Chapter 22—Biosimilars. In Pharmaceutical Medicine and Translational Clinical Research; Elsevier B.V.: London, UK, 2018; pp. 355–367. [Google Scholar] [CrossRef]
- Mirkov, S. Biosimilars: How similar is a biosimilar—A practical guide for pharmacists. J. Pharm. Pract. Res. 2018, 48, 442–449. [Google Scholar] [CrossRef]
- Mohapatra, R.K.; Kuppili, S.; Suvvari, T.K.; Kandi, V.; Behera, A.; Verma, S.; Kudrat-E-Zahan; Biswal, S.K.; Al-Noor, T.H.; El-ajaily, M.M.; et al. SARS-CoV-2 and its variants of concern including Omicron: A never ending pandemic. Chem. Biol. Drug Des. 2022, 99, 769–788. [Google Scholar] [CrossRef]
- Mohapatra, R.K.; Mahal, A.; Kutikuppala, L.V.S.; Pal, M.; Kandi, V.; Sarangi, A.K.; Obaidullah, A.J.; Mishra, S. Renewed global threat by the novel SARS-CoV-2 variants ‘XBB, BF.7, BQ.1, BA.2.75, BA.4.6’: A discussion. Front. Virol. 2022, 2, 1077155. [Google Scholar] [CrossRef]
- Mohapatra, R.K.; Tiwari, R.; Sarangi, A.K.; Islam, R.; Chakraborty, C.; Dhama, K. Omicron (B.1.1.529) variant of SARSCoV-2–Concerns, challenges and recent updates. J. Med. Virol. 2022, 94, 2336–2342. [Google Scholar] [CrossRef]
- Mohapatra, R.K.; Kandi, V.; Mishra, S.; Sarangi, A.K.; Pradhan, M.K.; Mohapatra, P.K.; Behera, A.; Dhama, K. Emerging novel sub-lineage BA.2.75: The next dominant omicron variant? Int. J. Surg. 2022, 104, 106835. [Google Scholar] [CrossRef]
- Bhatia, S.; Goli, D. Introduction to Pharmaceutical Biotechnology. Volume 1, Basic Techniques and Concepts; IOP Publishing: Bristol, UK, 2018; ISBN 978-0-7503-1299-8/978-0-7503-1300-1. [Google Scholar]
- Raju, P. World History of Modern Biotechnology and its Applications. Biotechnol. Indian J. 2016, 12, 107. [Google Scholar]
- Nogrady, B. How Indian biotech is driving innovation. Nature 2018, 564, S53–S55. [Google Scholar] [CrossRef]
- Thorsteinsdóttir, H.; Quach, U.; Daar, A.S.; Singer, P.A. Conclusions: Promoting biotechnology innovation in developing countries. Nat. Biotechnol. 2004, 22 (Suppl. S12), DC48–DC52. [Google Scholar] [CrossRef]
- Das Bhowmik, S.S.; Brinin, A.K.; Williams, B.; Mundree, S.G. Sugarcane biotechnology: Tapping unlimited potential. In Sugarcane-Based Biofuels and Bioproducts; Wiley Blackwell: Hoboken, NJ, USA, 2016; pp. 23–52. [Google Scholar]
- Seuba, X.; Correa, C. Digital Competitiveness Papers Biotechnology in India: Its Policy and Normative Framework. 2010. Available online: http://forum2010.biocat.cat/pdf/biotechnology-2520in-2520india_-2520its-2520policy$1.pdf (accessed on 8 October 2022).
- Chakma, J.; Sammut, S.M.; Agrawal, A. Life sciences venture capital in emerging markets. Nat. Biotechnol. 2013, 31, 195–201. [Google Scholar] [CrossRef]
- Kirchhoff, C.F.; Wang, X.Z.M.; Conlon, H.D.; Anderson, S.; Ryan, A.M.; Bose, A. Biosimilars: Key regulatory considerations and similarity assessment tools. Biotechnol. Bioeng. 2017, 114, 2696–2705. [Google Scholar] [CrossRef] [Green Version]
- Rathore, A.S.; Chhabra, H.; Bhargava, A. Approval of Biosimilars: A Review of Unsuccessful Regulatory Filings. Expert Opin. Biol. Ther. 2021, 21, 19–28. [Google Scholar] [CrossRef]
- Sharma, M.; Swarup, R. The way ahead—The new technology in an old society. In Biotechnology in India I; Advances in Biochemical Engineering/Biotechnology: Berlin/Heidelberg, Germany; Springer: Berlin/Heidelberg, Germany, 2003; Volume 84, pp. 1–48. [Google Scholar] [CrossRef]
- Konde, V. Biotechnology in India: Public-private partnerships. J. Commer. Biotechnol. 2008, 14, 43–55. [Google Scholar] [CrossRef]
- Saberwal, G. Giving voice to India’s entrepreneurs. Nat. Biotechnol. 2013, 31, 104–107. [Google Scholar] [CrossRef]
- Meil, P.; Salzman, H. Technological entrepreneurship in India. J. Entrep. Emerg. Econ. 2017, 9, 65–84. [Google Scholar] [CrossRef]
- Meher, B.R.; Balan, S.; Mohanty, R.R.; Jena, M.; Das, S. Biosimilars in India; Current status and future perspectives. J. Pharm. Bioallied Sci. 2019, 11, 12–15. [Google Scholar] [CrossRef]
- Rathore, A.S.; Li, Y.; Chhabra, H.; Lohiya, A. FDA Warning Letters: A Retrospective Analysis of Letters Issued to Pharmaceutical Companies from 2010–2020. J. Pharm. Innov. 2022. [Google Scholar] [CrossRef]
- Prakash, U.G. Biosimilars Pharmaceutical Market in India: Current Status, Challenges and Future Perspective. Biosci. Biotechnol. Res. Commun. 2021, 14, 47–54. [Google Scholar] [CrossRef]
- Biopharmaceutical Innovation: Which Countries Rank the Best?-DCAT Value Chain Insights. 13 April 2016. Available online: https://www.dcatvci.org/features/biopharmaceutical-innovation-which-countries-rank-the-best/ (accessed on 7 September 2022).
- Biosimilars Market, Global Forecasts to 2026. Available online: https://www.marketsandmarkets.com/Market-Reports/biosimilars-40.html (accessed on 7 September 2022).
- Generics and Biosimilars Initiative, Biosimilars Development Moving to Asia. 2018. Available online: https://www.gabionline.net/reports/Biosimilars-development-moving-to-Asia (accessed on 7 September 2022).
- Biosimilars-The India Story, RAS LSS. 2017. Available online: https://www.raslss.com/biosimilars-the-india-story/#gsc.tab=0 (accessed on 7 September 2022).
- Biocon-India’s Largest Biopharmaceutical Company. Available online: https://archive.biocon.com/ (accessed on 7 September 2022).
- How Did Johnson & Johnson Beat Back Remicade’s Biosim? Call It the Art of the Deal|Fierce Pharma. Available online: https://www.fiercepharma.com/pharma/what-s-behind-johnson-johnson-s-successful-remicade-defense-and-can-it-last (accessed on 7 September 2022).
- Biosimilars–Pfizer Annual Review 2017. Available online: https://www.pfizer.com/sites/default/files/investors/financial_reports/annual_reports/2017/our-innovation/biosimilars/index.html (accessed on 7 September 2022).
- Mylan, N.V. Mylan and Biocon Launch Trastuzumab Biosimilar, OgivriTM (Trastuzumab-Dkst), in the U.S. Available online: https://investor.mylan.com/news-releases/news-release-details/mylan-and-biocon-launch-trastuzumab-biosimilar-ogivritm (accessed on 7 September 2022).
- Biogen Launches First US Biosimilar with Samsung Bioepis. Available online: https://www.fiercepharma.com/marketing/biogen-launches-first-us-biosimilar-samsung-bioepis-copycat-roches-lucentis-40-discount (accessed on 7 September 2022).
- Eli Lilly and Company (LLY) Company Profile, News, Rankings, Fortune. Available online: https://fortune.com/company/eli-lilly/ (accessed on 7 September 2022).
- FDA Approves Coherus’ CIMERLITM (Ranibizumab-Eqrn) as the First and Only Interchangeable Biosimilar to Lucentis® for All Five Indications, with 12 Months of Interchangeability Exclusivity, Coherus BioSciences Inc. Available online: https://investors.coherus.com/news-releases/news-release-details/fda-approves-coherus-cimerlitm-ranibizumab-eqrn-first-and-only (accessed on 7 September 2022).
- Holz, F.G.; Oleksy, P.; Ricci, F.; Kaiser, P.K.; Kiefer, J.; Schmitz-Valckenberg, S. Efficacy and Safety of Biosimilar FYB201 Compared with Ranibizumab in Neovascular Age-Related Macular Degeneration. Ophthalmology 2022, 129, 54–63. [Google Scholar] [CrossRef]
- Sharma, A.; Kumar, N.; Parachuri, N.; Regillo, C.; Bandello, F.; Kuppermann, B. Biosimilar ranibizumab interchangeability: What does it mean to retinal physicians? Eye 2022. [Google Scholar] [CrossRef] [PubMed]
- Merck Launches Ontruzant®, First Trastuzumab Biosimilar in Europe-Big Molecule Watch. Available online: https://www.bigmoleculewatch.com/2018/03/13/merck-launches-ontruzant-first-trastuzumab-biosimilar-in-europe/ (accessed on 7 September 2022).
- U.S. FDA Approves Cyltezo® (Adalimumab-Adbm) as First Interchangeable Biosimilar with Humira®|Boehringer-Ingelheim.us. Available online: https://www.boehringer-ingelheim.us/press-release/us-fda-approves-cyltezo-adalimumab-adbm-first-interchangeable-biosimilar-humira (accessed on 7 September 2022).
- Fresenius Kabi Gets FDA Approval for Biosimilar Stimufend. Available online: https://news.bloomberglaw.com/health-law-and-business/fresenius-kabi-gets-fda-approval-for-biosimilar-stimufend (accessed on 7 September 2022).
- STADA Becomes Majority Shareholder of BIOCEUTICALS Arzneimittel AG, STADA. Available online: https://www.stada.com/blog/posts/2018/august/stada-becomes-majority-shareholder-of-bioceuticals-arzneimittel-ag (accessed on 7 September 2022).
- History, MABXIENCE, from Lab to Life. Available online: https://www.mabxience.com/company-history/ (accessed on 7 September 2022).
- FDA OKs First Biosimilar of Roche’s Blockbuster AMD Drug Lucentis. Available online: https://pharmaphorum.com/news/fda-oks-first-biosimilar-of-roches-blockbuster-amd-drug-lucentis/ (accessed on 7 September 2022).
- FDA Approves First Biosimilar Enoxaparin Sodium. Available online: https://gabionline.net/biosimilars/news/FDA-approves-first-biosimilar-enoxaparin-sodium (accessed on 7 September 2022).
- FDA Approves Nucala as the First and Only Biologic Treatment for Hypereosinophilic Syndrome (HES), GSK. Available online: https://www.gsk.com/en-gb/media/press-releases/fda-approves-nucala-as-the-first-and-only-biologic-treatment-for-hypereosinophilic-syndrome-hes/ (accessed on 7 September 2022).
- Teva and Celltrion Announce the Availability of TRUXIMA® (Rituximab-Abbs) Injection, the First Biosimilar to Rituxan® (Rituximab) in the United States. Available online: https://www.tevapharm.com/news-and-media/latest-news/teva-and-celltrion-announce-the-availability-of-truxima-rituximab-abbs-injection-the-first-biosimilar/ (accessed on 7 September 2022).
- Gan & Lee Pharmaceuticals Concludes Phase 3 Studies of Gan & Lee Insulin Glargine (GL-GLA)–Gan & Lee Pharmaceuticals. Available online: https://ganlee.us/press-releases/gan-lee-pharmaceuticals-concludes-phase-3-studies-of-gan-lee-insulin-glargine/ (accessed on 7 September 2022).
- Amega, History. Available online: http://www.amegabiotech.com/?page_id=18 (accessed on 7 September 2022).
- Celltrion Healthcare. Available online: https://www.celltrionhealthcare.com/en-us/products/product/?pkey=5 (accessed on 7 September 2022).
- Eye on Pharma: Chong Kun Dang’s Darbepoetin Alfa Biosimilar Approved. Available online: https://www.centerforbiosimilars.com/view/eye-on-pharma-chong-kun-dangs-darbepoetin-alfa-biosimilar-approved (accessed on 7 September 2022).
- Ober, R.J.; Radu, C.G.; Ghetie, V.; Ward, E.S. Differences in promiscuity for antibody-FcRn interactions across species: Implications for therapeutic antibodies. Int. Immunol. 2001, 13, 1551–1559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda-Hernández, M.P.; López-Morales, C.A.; Piña-Lara, N.; Perdomo-Abúndez, F.C.; Pérez, N.O.; Revilla-Beltri, J.; Molina-Pérez, A.; Estrada-Marín, L.; Flores-Ortiz, L.F.; Ruiz-Argüelles, A.; et al. Pharmacokinetic Comparability of a Biosimilar Trastuzumab Anticipated from Its Physicochemical and Biological Characterization. Biomed Res. Int. 2015, 2015, 874916. [Google Scholar] [CrossRef] [Green Version]
- Apotex Builds Momentum in Canada’s Biosimilar Market after World’s First Approval. Available online: https://www1.apotex.com/global/about-us/press-center/2018/06/01/apotex-builds-momentum-in-canadas-biosimilar-market-after-worlds-first-approval (accessed on 7 September 2022).
- JCR Launches the First Biosimilar Agalsidase Beta. Available online: https://www.centerforbiosimilars.com/view/jcr-launches-the-first-biosimilar-agalsidase-beta (accessed on 7 September 2022).
- Gedeon Richter’s Biosimilar Product Wins the 2020 Hungarian Innovation Grand Prize. Available online: https://www.gedeonrichter.com/en/news/210329 (accessed on 7 September 2022).
- BIOCAD Announces the First Trastuzumab Biosimilar Approved by the Ministry of Health of the Russian Federation, Business Wire. Available online: https://www.businesswire.com/news/home/20160120005889/en/BIOCAD-Announces-the-First-Trastuzumab-Biosimilar-Approved-by-the-Ministry-of-Health-of-the-Russian-Federation (accessed on 7 September 2022).
- Khilji, S.E.; Mroczkowski, T.; Assudani, R. Balancing growth and innovation in Indian biotech firms. South Asian J. Glob. Bus. Res. 2012, 1, 256–275. [Google Scholar] [CrossRef]
- Balancing Growth and Innovation in Indian Biotech Firms, Emerald Insight. Available online: https://www.emerald.com/insight/content/doi/10.1108/20454451211252769/full/html?fullSc=1&utm_source=TrendMD&utm_medium=cpc&utm_campaign=South_Asian_Journal_of_Global_Business_Research_TrendMD_1&WT.mc_id=Emerald_TrendMD_1 (accessed on 4 September 2022).
- Mohapatra, R.K.; Mishra, S.; Azam, M.; Dhama, K. COVID-19, WHO guidelines, pedagogy, and respite. Open Med. 2021, 16, 491–493. [Google Scholar] [CrossRef]
- The Impact of COVID-19 and the Policy Response in India. Available online: https://www.brookings.edu/blog/future-development/2020/07/13/the-impact-of-covid-19-and-the-policy-response-in-india/ (accessed on 7 September 2022).
- COVID-19 and the Food and Agriculture Sector: Issues and Policy Responses. Available online: https://www.oecd.org/coronavirus/policy-responses/covid-19-and-the-food-and-agriculture-sector-issues-and-policy-responses-a23f764b/ (accessed on 7 September 2022).
- WHO. BCG vaccine: WHO position paper, February 2018–recommendations. Vaccine 2018, 36, 3408–3410. [Google Scholar] [CrossRef]
- Anonymous. 2022. Available online: https://www.indiascienceandtechnology.gov.in/covid-19-vaccine/list-licensed-human-vaccine-manufacturing-facilities-india (accessed on 19 November 2022).
- Kumar, S. India in the Global Vaccine Market Prior to and during COVID-19; ISID: New Delhi, India, 2022. [Google Scholar]
- Malviya, J.; Giri, P.; Rathore, B.; Suryawanshi, R.; Jain, A.; Chincholikar, P.; Koshy, D.M. Application and historical aspects of vaccine development for human healthcare. Life Sci. Inform. Publ. 2022. [Google Scholar] [CrossRef]
- Ghosh, P.K. Indian Vaccines Industry Addressing Human Health Challenges. In Forum for Indian Science Diplomacy (FISD), Science Diplomacy Case Studies; RIS: New Delhi, India, 2019; Available online: https://fisd.in/sites/default/files/Publication/FISD-Case-Study_P-K-Ghosh.pdf (accessed on 1 January 2023).
- Kaufmann, S.H. Highly affordable vaccines are critical for our continued efforts to reduce global childhood mortality. Hum. Vaccines Immunother. 2019, 15, 2660–2665. [Google Scholar] [CrossRef]
- Biosimilar Developers and the Battle against COVID-19. Available online: https://www.centerforbiosimilars.com/view/biosimilar-developers-and-the-battle-against-covid19 (accessed on 7 September 2022).
- Emerging Trends for Biologics and Biosimilars in India, LexOrbis. Available online: https://www.lexorbis.com/emerging-trends-for-biologics-and-biosimilars-in-india/ (accessed on 7 September 2022).
- Seyhan, A.A. Lost in translation: The valley of death across preclinical and clinical divide–identification of problems and overcoming obstacles. Transl. Med. Commun. 2019, 4, 18. [Google Scholar] [CrossRef] [Green Version]
- Perloff, J.; Rushforth, A.; Welch, L.C.; Daudelin, D.; Suchman, A.L.; Gittell, J.H.; Santos, H.; Beswick, J.; Moore, S.; Selker, H.P. Intervening to enhance collaboration in translational research: A relational coordination approach. J. Clin. Transl. Sci. 2017, 1, 218–225. [Google Scholar] [CrossRef] [Green Version]
- Bano, R.; Gupta, S.; Shekhar, C. Translational research in biomedical sciences in India: Challenges, observations & national perspectives. Indian J. Med. Res. 2020, 152, 335–341. [Google Scholar]
- Kurki, P.; Kang, H.-N.; Ekman, N.; Knezevic, I.; Weise, M.; Wolff-Holz, E. Regulatory Evaluation of Biosimilars: Refinement of Principles Based on the Scientific Evidence and Clinical Experience. BioDrugs 2022, 36, 359–371. [Google Scholar] [CrossRef]
- Jadhav, M.; Jadhav, P. What’s ailing India’s research funding agencies? Nat. India 2013. [Google Scholar] [CrossRef]
- Pachouri, A.; Sharma, S. ADBI Working Paper Series Barriers to Innovation in Indian Small and Medium-Sized Enterprises Asian Development Bank Institute. 2016. Available online: http://www.adb.org/publications/barriers-innovation-indian-small-and-medium-sized- (accessed on 7 September 2022).
- Frew, S.E.; Rezaie, R.; Sammut, S.M.; Ray, M.; Daar, A.S.; Singer, P.A. India’s health biotech sector at a crossroads. Nat. Biotechnol. 2007, 25, 403–417. [Google Scholar] [CrossRef]
- India Lacks Enough Angel Investors to Fund Start-Ups: Nasscom—The Economic Times. Available online: https://economictimes.indiatimes.com/small-biz/startups/india-lacks-enough-angel-investors-to-fund-start-ups-nasscom/articleshow/49578399.cms?from=mdr (accessed on 11 October 2022).
- Research and Development Expenditure (% of GDP) Data. Available online: https://data.worldbank.org/indicator/GB.XPD.RSDV.GD.ZS (accessed on 7 September 2022).
- Lack of Private Sector Investment Cripples India’s Growth-BW Businessworld. Available online: https://www.businessworld.in/article/Lack-Of-Private-Sector-Investment-Cripples-India-s-Growth/28-07-2017-123067/ (accessed on 7 September 2022).
- The Challenges and Opportunities of Innovating in India, ORF. Available online: https://www.orfonline.org/expert-speak/challenges-opportunities-innovating-india/ (accessed on 7 September 2022).
- India’s Health Biotech Sector at a Crossroads|Nature Biotechnology. Available online: https://www.nature.com/articles/nbt0407-403 (accessed on 7 September 2022).
- Palnitkar, U. Growth of Indian biotech companies, in the context of the international biotechnology industry. J. Commer. Biotechnol. 2005, 11, 146–154. [Google Scholar] [CrossRef]
- de Rond, M. Strategic Alliances as Social Facts: Business, Biotechnology, and Intellectual History; Cambridge University Press: Cambridge, UK, 2009. [Google Scholar] [CrossRef]
- Lakhotia, S.C. Research fund crunch, real or created, is hitting India’s academia on the wrong side. Proc. Indian Natl. Sci. Acad. 2018, 84, 545–547. [Google Scholar] [CrossRef]
- Föller, A. Leadership management needs in evolving biotech companies. Nat. Biotechnol. 2002, 20, BE64. [Google Scholar] [CrossRef]
- Kumar, N.K.; Quach, U.; Thorsteinsdóttir, H.; Somsekhar, H.; Daar, A.S.; Singer, P.A. Indian biotechnology—Rapidly evolving and industry led. Nat. Biotechnol. 2004, 22, DC31–DC36. [Google Scholar] [CrossRef]
- Why Indian Entrepreneurs Need Business Training and up Skilling. Available online: https://inc42.com/resources/why-indian-entrepreneurs-need-business-training-and-up-skilling/ (accessed on 7 September 2022).
- Jayaraman, K.S. Biotech boom. Nature 2005, 436, 480–483. [Google Scholar] [CrossRef]
- Ghose, T.K.; Ghosh, P. Biotechnology in India I; Advances in Biochemical Engineering/Biotechnology: Berlin/Heidelberg, Germany; Springer: Berlin/Heidelberg, Germany, 2003; ISBN 9783662145920. [Google Scholar]
- Wong, P.K.; Singh, A. Do co-publications with industry lead to higher levels of university technology commercialization activity? Scientometrics 2013, 97, 245–265. [Google Scholar] [CrossRef]
- Abramo, G.; D’Angelo, C.A.; Costa, F. University-industry research collaboration: A model to assess university capability. High. Educ. 2011, 62, 163–181. [Google Scholar] [CrossRef] [Green Version]
- Tijssen, R.J.W.; van Leeuwen, T.N.; van Wijk, E. Benchmarking university-industry research cooperation worldwide: Performance measurements and indicators based on co-authorship data for the world’s largest universities. Res. Eval. 2009, 18, 13–24. [Google Scholar] [CrossRef]
- Abramo, G.; D’Angelo, C.A.; Solazzi, M. Assessing public-private research collaboration: Is it possible to compare university performance? Scientometrics 2010, 84, 173–197. [Google Scholar] [CrossRef]
- Tijssen, R.J.W. Co-authored research publications and strategic analysis of public-private collaboration. Res. Eval. 2012, 21, 204–215. [Google Scholar] [CrossRef]
- Perkmann, M.; Walsh, K. The two faces of collaboration: Impacts of university-industry relations on public research. Ind. Corp. Change 2009, 18, 1033–1065. [Google Scholar] [CrossRef]
- Biotechnology in Israel. Available online: https://www.jewishvirtuallibrary.org/biotechnology-in-israel (accessed on 7 September 2022).
- Isrealli-Home Improvement. Available online: https://www.isrealli.org/ (accessed on 7 September 2022).
- Singh, S. Enrichment and Strengthening of Indian Biotechnology Industry along with Academic Interface. Int. J. Educ. Adm. Policy Stud. 2014, 6, 154–158. [Google Scholar]
- Tewari, R. Industry-Academia R&D Ecosystem in India—An Evidence Based Study; DL Printing Press: Punjab, India, 2017; Available online: https://cpr.puchd.ac.in/wp-content/uploads/2017/05/Industry-Academia-RD-Ecosystem-in-India.pdf (accessed on 7 September 2022).
- Kang, H.N.; Knezevic, I. Regulatory evaluation of biosimilars throughout their product life-cycle. Bull. World Health Organ. 2018, 96, 281–285. [Google Scholar] [CrossRef]
- Uppal, A.; Chakrabarti, R.; Chirmule, N.; Rathore, A.; Atouf, F. Biopharmaceutical Industry Capability Building in India: Report from a Symposium. J. Pharm. Innov. 2021, 17, 1555–1562. [Google Scholar] [CrossRef]
- Perkmann, M.; Tartari, V.; McKelvey, M.; Autio, E.; Broström, A.; D’Este, P.; Fini, R.; Geuna, A.; Grimaldi, R.; Hughes, A.; et al. Academic engagement and commercialisation: A review of the literature on university-industry relations. Res. Policy 2013, 42, 423–442. [Google Scholar] [CrossRef]
- Perkmann, M.; Neely, A.; Walsh, K. How should firms evaluate success in university-industry alliances? A performance measurement system. R D Manag. 2011, 41, 202–216. [Google Scholar] [CrossRef]
- de Fuentes, C.; Dutrénit, G. Best channels of academia-industry interaction for long-term benefit. Res. Policy 2012, 41, 1666–1682. [Google Scholar] [CrossRef] [Green Version]
- Guerrero, M.; Urbano, D. The development of an entrepreneurial university. J. Technol. Transf. 2012, 37, 43–74. [Google Scholar] [CrossRef]
- Narin, F.; Hamilton, K.S.; Olivastro, D. The increasing linkage between U.S. technology and public science. Res. Policy 1997, 26, 317–330. [Google Scholar] [CrossRef]
- Calvert, J.; Patel, P. University-industry research collaborations in the UK: Bibliometric trends. Sci. Public Policy 2003, 30, 85–96. [Google Scholar] [CrossRef]
- Levy, R.; Roux, P.; Wolff, S. An analysis of science-industry collaborative patterns in a large European University. J. Technol. Transf. 2009, 34, 1–23. [Google Scholar] [CrossRef]
- Finkelstein, A. Static and dynamic effects of health policy: Evidence from the vaccine industry. Q. J. Econ. 2004, 119, 527–564. [Google Scholar] [CrossRef]
- Rezaie, R.; McGahan, A.M.; Frew, S.E.; Daar, A.S.; Singer, P.A. Emergence of biopharmaceutical innovators in China, India, Brazil, and South Africa as global competitors and collaborators. Health Res. Policy Syst. 2012, 10, 18. [Google Scholar] [CrossRef] [Green Version]
- Rezaie, R.; Singer, P.A. Global health or global wealth? Nat. Biotechnol. 2010, 28, 907–909. [Google Scholar] [CrossRef]
- Jois, R.; Mukherjee, S.; Rajeswari, S.; Rath, P.; Goyal, V.; Gupta, D. Similar biologics in India: A story of access or potential for compromise? Indian J. Med. Res. 2020, 152, 456. [Google Scholar] [CrossRef]
- Biosimilar and Interchangeable Products, FDA. Available online: https://www.fda.gov/drugs/biosimilars/biosimilar-and-interchangeable-products (accessed on 11 October 2022).
- Guidance on the Use of International Nonproprietary Names (Inns) for Pharmaceutical Substances. 2017. Available online: http://apps.who.int/bookorders. (accessed on 11 October 2022).
- Biosimilar Development, Review, and Approval, FDA. Available online: https://www.fda.gov/drugs/biosimilars/biosimilar-development-review-and-approval (accessed on 11 October 2022).
- India as a Pharma Innovation Hub: An Interview with Dr. Reddy’s Prasad|McKinsey. Available online: https://www.mckinsey.com/featured-insights/future-of-asia/india-as-a-pharma-innovation-hub-an-interview-with-dr-reddys-g-v-prasad (accessed on 11 October 2022).
- Greene, W. The Emergence of India’s Pharmaceutical Industry and Implications for the U.S. Generic Drug Market. 2007. Available online: https://www.usitc.gov/publications/332/EC200705A.pdf (accessed on 11 October 2022).
- Reddy, K.S. India led health innovation(s) for achieving the SDG health goal in the global South. Perspect. Public Health 2022, 142, 20–21. [Google Scholar] [CrossRef]
- Taking India’s Life Sciences Industry to the Global Stage-Article-Kearney. Available online: https://www.kearney.com/covid-19/article/-/insights/taking-indias-life-sciences-industry-to-the-global-stage (accessed on 12 October 2022).
- Mazumdar-Shaw, K. Leveraging affordable innovation to tackle India’s healthcare challenge. IIMB Manag. Rev. 2018, 30, 37–50. [Google Scholar] [CrossRef]
- Rezaie, A. Health Technology Innovation by Indigenous Enterprises in China, India and Brazil. 2011. Available online: https://tspace.library.utoronto.ca/bitstream/1807/31296/1/Rezaie_Abdolrahim_201106_PhD_Thesis.pdf (accessed on 12 October 2022).
- Zhang, Y.P.; Deng, M.M. Enforcing pharmaceutical and biotech patent rights in China. Nat. Biotechnol. 2008, 26, 1235–1240. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Leydesdorff, L. The emergence of China as a leading nation in science. Res. Policy 2006, 35, 83–104. [Google Scholar] [CrossRef] [Green Version]
- Minisman, G.; Bhanushali, M.; Conwit, R.; Wolfe, G.I.; Aban, I.; Kaminski, H.J.; Cutter, G. Implementing Clinical Trials on an International Platform: Challenges and Perspectives. J. Neurol. Sci. 2012, 313, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Shenoy, P. Multi-regional clinical trials and global drug development. Perspect. Clin. Res 2016, 7, 62. [Google Scholar] [CrossRef]
- Facts about the Current Good Manufacturing Practices (CGMPs), FDA. Available online: https://www.fda.gov/drugs/pharmaceutical-quality-resources/facts-about-current-good-manufacturing-practices-cgmps (accessed on 12 October 2022).
- India Risks Missing Boat as Biosimilars Shake up Drug Industry, Reuters. Available online: https://www.reuters.com/article/us-india-biosimilars-idINKCN0S82OQ20151014 (accessed on 4 September 2022).
- Kang, H.N.; Thorpe, R.; Knezevic, I.; Blades, C.D.R.Z.; Levano, M.C.; Chew, J.Y.; Chilufya, M.B.; Chirachanakul, P.; Chua, H.M.; Farahani, A.V.; et al. The regulatory landscape of biosimilars: WHO efforts and progress made from 2009 to 2019. Biologicals 2020, 65, 1–9. [Google Scholar] [CrossRef]
- Part 1: India Works on Guidelines for Biological Products. Available online: https://www.centerforbiosimilars.com/view/india-works-on-its-guidelines-for-biological-products (accessed on 7 September 2022).
- Dey, S. Biocon: Taking a Crack at the Global Biosimilar Market. South Asian J. Bus. Manag. Cases 2018, 8, 100–110. [Google Scholar] [CrossRef]
- Vikram; Deep, A.; Manita; Rana, A.C.; Yadav, M.; Marwaha, R.K. Biosimilars Regulation in the United States and FDA Approved Biosimilars from 2015–2018. Appl. Clin. Res. Clin. Trials Regul. Aff. 2019, 7, 12–29. [Google Scholar] [CrossRef]
- Derbyshire, M. Patent expiry dates for best-selling biologicals. GaBI J. 2015, 4, 178–179. [Google Scholar]
- Roach, M.; Cohen, W.M. Lens or Prism? Patent citations as a measure of knowledge flows from public research. Manag. Sci. 2013, 59, 504–525. [Google Scholar] [CrossRef]
- Kang, H.N.; Thorpe, R.; Knezevic, I.; Casas Levano, M.; Chilufya, M.B.; Chirachanakul, P.; Chua, H.M.; Dalili, D.; Foo, F.; Gao, K.; et al. Regulatory challenges with biosimilars: An update from 20 countries. Ann. N. Y. Acad. Sci. 2021, 1491, 42–59. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.; Ewesuedo, R.; Lula, S.; Zacharchuk, C. Biosimilars for the Treatment of Cancer: A Systematic Review of Published Evidence. BioDrugs 2017, 31. [Google Scholar] [CrossRef] [Green Version]
- Vulto, A.G.; Jaquez, O.A. The process defines the product: What really matters in biosimilar design and production? Rheumatology 2017, 56 (Suppl. S4), iv14–iv29. [Google Scholar] [CrossRef] [Green Version]
- Dolinar, R.O.; Edelman, S.; Heinemann, L.; Home, P.; Goyal, S.; Polonsky, W.H.; Schellekens, H. Impact of Biosimilar Insulins on Clinical Practice: Meeting Report. J. Diabetes Sci. Technol. 2014, 8, 179–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbogast, L.W.; Delaglio, F.; Schiel, J.E.; Marino, J.P. Multivariate analysis of 2D 1H, 13C methyl NMR spectra of monoclonal antibody therapeutics to facilitate assessment of higher order structure. Anal. Chem. 2017, 89, 11839–11845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alten, R.; Cronstein, B.N. Clinical trial development for biosimilars. Semin. Arthritis Rheum. 2015, 44 (Suppl. S6), S2–S8. [Google Scholar] [CrossRef] [Green Version]
- Edmondson, R.; Broglie, J.J.; Adcock, A.F.; Yang, L. Three-dimensional cell culture systems and their applications in drug discovery and cell-based biosensors. Assay Drug Dev. Technol. 2014, 12, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Barlas, S. FDA Guidance on Biosimilar Interchangeability Elicits Diverse Views: Current and Potential Marketers Complain About Too-High Hurdles. Pharm. Ther. 2017, 42, 509. [Google Scholar]
- Chow, S.-C. Assessing biosimilarity and interchangeability of biosimilar products under the Biologics Price Competition and Innovation Act. Generics Biosimilars Initiat. J. 2013, 2, 20–25. [Google Scholar] [CrossRef]
- Lu, Y.; Chow, S.C.; Zhang, Z.Z. Statistical Designs for Assessing Interchangeability of Biosimilar Products. Drug Des. 2014, 03, 109. [Google Scholar] [CrossRef] [Green Version]
- Legislations on Biosimilar Interchangeability in the US and EU–Developments Far from Visibility. Available online: https://www.gabionline.net/sponsored-articles/Legislations-on-biosimilar-interchangeability-in-the-US-and-EU-developments-far-from-visibility (accessed on 12 October 2022).
- Madhavi, Y. The issue of equity in primary vaccine technology development and its implications on the implementation of vaccine policy in India. Soc. Sci. Health News Lett. 2001, 2, 5–17. [Google Scholar]
- Madhavi, Y. Vaccine Policy in India. PLoS Med. 2005, 2, e127. [Google Scholar] [CrossRef]
- Huzair, F.; Sturdy, S. Biotechnology and the transformation of vaccine innovation: The case of the hepatitis B vaccines 1968–2000. Stud. Hist. Philos. Sci. Part C Stud. Hist. Philos. Biol. Biomed. Sci. 2017, 64, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, R.K.; El-Shall, N.A.; Tiwari, R.; Nainu, F.; Kandi, V.; Sarangi, A.K.; Mohammed, T.A.; Desingu, P.A.; Chakraborty, C.; Dhama, K. Need of booster vaccine doses to counteract the emergence of SARS-CoV-2 variants in the context of the Omicron variant and increasing COVID-19 cases: An update. Hum. Vaccines Immunother. 2022, 18, e2065824. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, R.K.; Mishra, S.; Kandi, V.; Sarangi, A.K.; Zahan, K.-E.; Ali, M.S.; Sahoo, R.N.; Alam, N.; Pattnaik, G.; Dhama, K. Emerging Monkeypox cases amid the ongoing COVID-19 pandemic in Indian subcontinent: A probable healthcare challenge for the South East Asia. Front. Public Health 2022, 10, 1066425. [Google Scholar] [CrossRef]
- Guerin, P.J.; Singh-Phulgenda, S.; Strub-Wourgaft, N. The consequence of COVID-19 on the global supply of medical products: Why Indian generics matter for the world? F1000Research 2020, 9, 225. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Negishi, M.; Nishizawa, M. Coauthorship linkages between universities and industry in Japan. Res. Eval. 2007, 16, 299–309. [Google Scholar] [CrossRef]
- Sakakibara, M.; Branstetter, L. Do Stronger Patents Induce More Innovation? Evidence from the 1988 Japanese Patent Law Reforms. Rand. J. Econ. 2001, 32, 77. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, P. Indian pharma threatened by COVID-19 shutdowns in China. Lancet 2020, 395, 675. [Google Scholar] [CrossRef]
- Serum Institute of India|Manufacturer of Vaccines & Immuno-biologicals-GMP Vaccine Manufacturer. Available online: https://www.seruminstitute.com/ (accessed on 4 September 2022).
- Chakma, J.; Masum, H.; Perampaladas, K.; Heys, J.; Singer, P.A. Indian vaccine innovation: The case of Shantha Biotechnics. Global Health 2011, 7, 9. [Google Scholar] [CrossRef] [Green Version]
- Biological E Ltd. Available online: https://biologicale.com/ (accessed on 4 September 2022).
- History & Milestones-Bharat Biotech-A Leading Biotech Company. Available online: https://www.bharatbiotech.com/history_milestones.html (accessed on 4 September 2022).
- Panacea Biotec. Available online: https://www.panaceabiotec.com/en (accessed on 4 September 2022).
- Dr. Reddy’s Laboratories-Multinational Pharmaceutical Company. Available online: https://www.drreddys.com/8 (accessed on 4 September 2022).
- Clinical Research Services, Regenerative Medicine, Specialty Pharmaceuticals|Reliance Life Sciences-LifeSciences. Available online: https://rellife.com/ (accessed on 4 September 2022).
- Zydus Pharma Research Center|Vaccine Technology Centre in India. Available online: https://www.zyduslife.com/research (accessed on 4 September 2022).
- Indian Immunologicals Ltd (IIL)|Leading Animal & Human Vaccine Manufacturer-IIL. Available online: https://www.indimmune.com/ (accessed on 4 September 2022).
- Burnouf, T. Modern Plasma Fractionation. Transfus. Med. Rev. 2007, 21, 101. Available online: /pmc/articles/PMC7125842/ (accessed on 7 September 2022). [CrossRef]
- Biotechnology Industry Research Assistance Council (BIRAC). Available online: https://birac.nic.in/big.php/ (accessed on 4 September 2022).
- Biotechnology Industry Research Assistance Council (BIRAC)-Home. Available online: https://www.birac.nic.in/ (accessed on 4 September 2022).
- Biotechnology Industry Research Assistance Council (BIRAC)-Biotechnology Ignition Grant (BIG) Scheme. Available online: www.birac.nic.in (accessed on 4 September 2022).
- Biotechnology Industry Research Assistance Council (BIRAC). A Government of India Enterprise Biotechnology Ignition Grant (BIG) Igniting New Ideas…Scheme Guidelines. Available online: https://birac.nic.in/big.php (accessed on 7 September 2022).
- Biotechnology Industry Research Assistance Council (BIRAC)-New. Available online: https://birac.nic.in/desc_new.php?id=217 (accessed on 7 September 2022).
- Biotechnology Industry Research Assistance Council (BIRAC)-New. Available online: https://birac.nic.in/desc_new.php?id=216 (accessed on 7 September 2022).
- Biotechnology Industry Research Assistance Council (BIRAC)-New. Promoting Academic Research Conversion to Enterprise (PACE). Available online: https://birac.nic.in/desc_new.php?id=286 (accessed on 7 September 2022).
- Biotechnology Industry Research Assistance Council (BIRAC)-BioNEST. Available online: https://birac.nic.in/bionest.php (accessed on 7 September 2022).
- What are Equity Mutual Funds? Meaning, Types, Benefits, Return & Taxation. Available online: https://www.sbimf.com/en-us/what-are-equity-mutual-funds (accessed on 7 September 2022).
- IMPRINT India Initiative. Available online: https://imprint-india.org/ (accessed on 7 September 2022).
- Association of Biotechnology Led Enterprises. Available online: https://www.ableindia.in/ (accessed on 7 September 2022).



{kind=link}
{kind=link}
| Triggering Factor | Beneficiary Organisation | Speciality Area | References |
|---|---|---|---|
| Scientists or local individual from various industrial sectors | XCyton Diagnostics (Bengaluru) | Diagnostics | [21] |
| GangaGen (Bengaluru) | Antimicrobials | ||
| Shanta Biotechnics (Hyderabad)–now part of Sanofi | Biogenerics, diagnostics, contract research | ||
| Cytogenomics (Bengaluru) | Bioinformatics | ||
| Bigtec (Bengaluru) Brilliant Bio Pharma Private Limited (Hyderabad) | Bioinformatics Veterinary Vaccines | ||
| Companies venturing into biotech | Serum Institute of India (Pune) | Vaccines, biosimilars | [21] |
| Biocon (Bengaluru) | Generics, biologics, biosimilars | ||
| Infosys (Bengaluru); Tata Consultancy Services (Mumbai) | Bioinformatics | ||
| Zydus Cadila | Generics, biologics, biosimilars | ||
| Bioogical E (Hyderabad) | Vaccines. Biologics | ||
| Intas Pharmaceuticals (Ahmedabad) | Generics, biogenerics, contract manufacturing | ||
| Emcure–Gennova (Pune) | Biosimilars, Novel Vaccines | ||
| Panacea Biotec (New Delhi) | Generics, vaccines | ||
| Wockhardt (Mumbai) | Generics, biologics, vaccines | ||
| Dr. Reddy’s Laboratories (Hyderabad) | Generics, vaccines, biosimilars, biologics | ||
| GVK Biosciences (Hyderabad) | Generics, biogenerics | ||
| Jubilant Biosys (Bengaluru) | Bioinformatics, contract research | ||
| Academic scientist to bioentrepreneur | Bangalore Genei (Bengaluru) | Reagents supply, contract research | [21] |
| Avesthagen (Bengaluru) | Plant biotech, diagnostics, nutraceuticals, contract research | ||
| Strand Life Sciences (Bengaluru) | Bioinformatics | ||
| Microtest Innovations (Bengaluru) | Diagnostics | ||
| Industry professionals or academic scientists from overseas | Molecular Connections (Bengaluru); Cell | Bioinformatics, systems biology | [12,21] |
| Bhat Biotech (Bengaluru) | Diagnostics | ||
| Bharat Biotech International (Hyderabad) | Vaccines, Biosimilars | ||
| Genotypic Technologies (Bengaluru) | Bioinformatics, contract research | ||
| Connexios Life Sciences (Bengaluru) | Systems biology | ||
| Ocium Biosolutions, Mapmygenome (Hyderabad) | Bioinformatics, Diagnostics | ||
| Multinational company setting up in India | Quintiles India (Bengaluru); Accelrys (Bengaluru) | Bioinformatics, contract research | [21] |
| Merck KGaA (Bengaluru); MWG (Bengaluru); Thermo-Fisher (Bengaluru); Sartorius (Bengaluru); DuPont (Hyderabad) | Reagents and equipment supply, customised bioservices; R&D facilities | ||
| GlaxoSmithKline Pharmaceuticals Ltd., Mumbai | Generics, Vaccines | ||
| Govt. initiated biotech company | Indian Immunologicals (Hyderabad); Human Biological Institute (Ooty) | Vaccines (Animal and Human) | - |
| Bharat Immunological and Biologicals Corporation Limited (BIBCOL), (Bulandsahar, UP) | Vaccines | ||
| Indian Vaccine Corporation Limited (Delhi) | |||
| Start-up as emerging biotech company | Med Genome (Bengaluru), X Code Life (Chennai), FARCAST Biosciences (Bengaluru) | Bioinformatics, Diagnostics, drug dicovery | - |
| BUGWORKS (Bengaluru) | Antimicrobials | ||
| Pandorum (Bengaluru) | Tissue Engineering, Regenerative medicines | ||
| Oncostem Diagnostics (Bengaluru) | Diagnostics and therapy | ||
| Zumutor Biologics (Bengaluru) | Novel Immunotherapy and stem cell research. |
| Industry | Country | Flagship Biosimilar | Market Share |
|---|---|---|---|
| Johnson and Johnson | USA | Remicade (Infliximab) [31] | 48.2% |
| Pfizer | USA | Inflectra®®® (infliximab-dyyb in the US) [32] | |
| Mylan | USA | Ogivri (Trastuzumab) [33] | |
| Biogen | USA | Byooviz [34] | |
| Eli Lilly | USA | Insulin Glargine [35] | |
| Coherus Bioscience | USA | Cimerli (Ranibizumab-eqrn) [36,37,38] | |
| MSD (Merck & Co) | Germany | Ontruzant (Trastuzumab) [39] | 18.1% |
| Boehringer Ingelheim | Germany | Cyltezo (adalimumab-adbm) [40] | |
| Fresenius Kabi AG | Germany | Stimufend [41] | |
| StadaArzneimittel AG | Germany | Silapo (epoetin-zeta) [42] | |
| mABxience | Switzerland | Novex (rituximab) [43] | |
| Roche | Switzerland | Lucentis (ranibizumab) [44] | |
| Sanofi Aventis | France | Lovenox (enoxaparin sodium) [45] | |
| GlaxoSmithKline | British | Nucala (mepolizumab) [46] | |
| Teva Pharmaceutical | Israel | Truxima (rituximab-abbs) [47] | |
| Gan and Lee Pharmaceuticals | China | Glargine [48] | |
| Amega Biotech | Argentina | Neutropine (Filgrastim) [49] | |
| Samsung Biologics | South Korea | Byooviz [34] | |
| Celltrion | South Korea | Remsima [50] | |
| Chong Kun Dang | South Korea | Darbepoetin Alfa [51] | |
| Probiomed | Mexico | Trastuzumab [52,53] | |
| Apotex | Canada | Apobiologix (pegfilgrastim) [54] | |
| JCR Pharmaceuticals | Japan | Agalsidase beta [55] | |
| Gedeon Richter | Hungary | Terrosa [56] | |
| Biocad | Russia | Trastuzumab [57] |
| Product | Company Name | Active Drug Molecule | Therapeutic Use in |
|---|---|---|---|
| Glaritus | Wockhardt | Insulin Glargine | Diabetes |
| Grafeel | Dr. Reddy’s Laboratories | Filgrastin | Neutropenia |
| Pegfilgrastism | Lupin | Pegfilgrastin | Cancer, Neutropenia |
| Epofer | Emcure | Epoetin alpha | Anemia |
| Zyrop | Cadila Healthcare | Erythropeotin | Chronic kidney failure |
| Krabeva | Biocon | Bevacizumab | Colorectal cancer |
| Bevacirel | Reliance Life Sciences | ||
| Cizumab | Hetero | ||
| Erbitux | Cetuximab | Colorectal cancer | |
| Acellbia | Biocad | Rituximab | NonHodgkin Lymphoma |
| Maball | Hetero Group | ||
| maTabs | Intas Pharmaceuticals | ||
| Adafrar | Torrent Pharmaceuticals | Adalimumab | Rheumatoid Athritis, Crohn’s disease |
| CaNMab | Biocon | Transtuzumab | Breast cancer |
| Intacept | Intas Pharmaceuticals | Entanercept | Rheumatoid Athritis |
| Relibeta | Reliance Life Sciences | Interferon Beta 1a | Multiple sclerosis |
| Razumab | Intas Pharmaceuticals | Ranibizumab | Degenerative myopia |
| AbcixiRel | Reliance Life Sciences | Abciximab | Angina, Cardiac ischemia |
| Basalog | Biocon | insulin glargine | Diabetes |
| Biovac-B | Wockhardt | hepatitis B vaccine | Hepatitis B |
| FostiRel | Reliance Life Sciences | follitropin beta | Female infertility |
| Mirel | Reliance Life Sciences | reteplase | Myocardial Infraction |
| Zavinex | Cadila Health Care | Interferon alfa-2b | Chronic hepatitis B and C |
| Choriorel | Reliance Life Sciences | chorionic gonadotrophin hormone r-hCG | Female infertility |
| Sl. No. | Manufacturer | Licensed Vaccine | Target Species | Reference |
|---|---|---|---|---|
| 1. | BCG Vaccine Laboratory, Guindy, Tamilnadu, India. | Tuberculine, BCG | Human | [63,64] |
| 2. | Pasteur Institute of India, Coonoor, The Nilgiris, Tamilnadu, India. | DTP, DT, TT and inactivated rabies vaccine | Humans and canine | [64,65,66] |
| 3. | Central Research Institute, Kasauli, Solan, Himachal Pradesh, India. | Yellow fever, JE, DTP, DT, TT | Humans | [64,67] |
| 4. | BIBCOL, Chola, Uttar Pradesh, India. | bOPV | Human | [64,68] |
| 5. | Haffkine, Parle, Mumbai, India. | bOPVand mOPV | Human | [68] |
| 6. | Human biological Institute, a division of Indian Immunologicals Limited, Hyderabad, Telangana, India. | Rabies, DTP, TT, DT, Hep- B, Pentavalent (DTP+Hib+HepB) | Human and canine | [64,68] |
| 7. | HLL Biotech Ltd., Taramani, Chennai, Tamil Nadu, India. | Hep B, DTwP- HepB-Hib | Human | [68] |
| 8. | Bharat biotech International Ltd., Hyderabad, Telangana, India. | Hib, Rabies, bOPV, mOPV, DTP+Hib+HepB, Vi polysaccharide Typhoid, H1N1, DTP, DTP+HepB, Rotavirus vaccine, Inactivated JE vaccine, Typhoid+TT Conjugate Vaccine andDTP+Hep- B+Hib (Liquid), DTP+Hib, BBV152 Covaxin | Human, canine | [64,68] |
| 9. | Biological E, Hyderabad, Andhra Pradesh, India. | DTP, TT, JE bulk & DT | Humans | [64,67] |
| 10. | Biomed Pvt. Ltd., Ghaziabad, Uttar Pradesh, India. | Hib, Meningococcal Polysaccharide, bOPV, Rabies, Meningococcal polysaccharide. | ||
| 11. | Cadila Healthcare, Ahmedabad, Gujarat, India. | Rabies, H1N1, trivalent influenza | Human | [64,68] |
| 12. | Serum Institute of India, Pune, Maharastra, India. | DTP, TT, DT, Hep-B, Hib, MMR, Measles, Rubella, BCG, IPV, DTP+HepB+Hib (Liquid+lyophilised), DTP+HepB, DTP+Hib, H1N1, Meningococcal A conjugate (lyophilised), Mumps, MR, H1N1(whole virion inactivated), Measles+Mumps, Measles+Rubela, Seasonal Influenza vaccine, COVID-19 vaccine | Human | [64,67,68] |
| 13. | Shantha Biotechnics Ltd., Hyderabad, India. | DTP, DTP+HepB+Hib (Liquid), DTP+Hib, DPT+Hep B, TT, Hib, Hep-B, DT bulk, TT Bulk, Hib Bulk, Hep B Bulk, DTP bulk, DTP+HepB+Hib bulk, DTP+HepB+Hib RTF bulk, Oral cholera vaccine, IPV RTF Bulk, IPV | Human | [64,67,68] |
| Vaccines | Indian Manufacturer | Collaborator(s) | Current Regulatory Status |
|---|---|---|---|
| Covishield | Serum Institute of India, Pune, India | Oxford-AstraZeneca | Approved |
| Covaxin | BharatBiotech Int. Ltd., Hyderabad, India | Indian Council of Medical Research, National Institute of Virology | Approved |
| ZyCov-D | Cadila Healthcare Ltd., Ahmedabad, India | Department of Biotechnology, India | Approved |
| Sputinik V | Dr. Reddy’s lab, Hyderabad, India | Gamaleya National Centre, Russia | Approved |
| NCV-COV2373 | Serum Institute of India, Pune | Novovax | Emergency authorisation |
| HGCO 19 m-RNA based vaccine | Genova, Pune, India | HDT-Bio, US DBT | Approved |
| Recombinant protein-based Vaccine (Corbevax) | Biological E, Hyderabad, India | Baylor College, US | Approved |
| Codon-deoptimised live attenuated COVID-19 Vaccine | Indian Immunologicals Limited, India | Griffith University, Australia | Pre-clinical |
| Warm COVID-19 Vaccine | Mynvax, Indian institute of Science, Bengaluru, India | BIRAC |
| Positively Contributing Factors | Negatively Affecting Factors | |
|---|---|---|
| Strengths (S) | Weaknesses (W) | |
| Internal factors | 1. Young and aspiring workforce 2. Cost competitiveness 3. High efficacy, low cost and akin safety level; growing demand in healthcare 4. Affordable, low-cost biosimilars make medication cost-effective in a price-sensitive Indian market 5. Reduced cycle in synthesis and regulatory compliance compared to innovator molecule 6. Innovation, R&D focus in innovative therapeutics as key player at global scale 7. Government regulatory assistance to produce biosimilars 8. Government initiatives to foster confidence and encourage investment | 1. Poor Industry-Academia alliance 2. Low government funding to industry 3. Complex regulatory compliance process; lack of confidence in regulatory bodies and policy makers leading to high corporate cost in approval 4. Physicians not prescribing biosimilars; low awareness among the doctor and patient 5. Higher price compared to conventional generic drugs 6. Pharmacovigilance to monitor efficacy and safety needed for possible immunogenicity 7. Altered production process may alter biosimilars’ property 8. Batch-wise uniform production is a challenge; needs skilled manpower, and validated and verifiable SOP |
| Opportunities (O) | Threats (T) | |
| External factors | 1. Green-field, favourable emerging global biosimilars market 2. Fast-growing biopharma trade; US $300 million Indian biosimilar market anticipated to be worth US $40 billion by 2030 3. Over next few years, patent protection of many biologics expire 4. Vast prospect for cost-effective Indian biosimilars; biologics company start-ups booming 5. Biosimilar to cost 20–30% less than biologicals; low cost makes it affordable and accessible as demand grows 6. Government pledges to fund up to US $1.3 billion on API-based pharma business 7. Making APIs locally appear doable in next couple of years; to drive developing biotech-based medicines in India for the world 8. Efforts of DBT and BIRAC to support Indian biotech industry would benefit biologics industry 9. Government strategies focus on globally-acceptable legislation, entrepreneurship, industry-academia and public-private partnerships, and investment avenues for business house, investor and other agencies | 1. Stronger Chinese and Korean influence 2. Bargaining power of Indian companies with international patent litigations; patent litigation stifles smaller company from getting into biosimilars business 3. Lack of a comprehensive regulatory framework for biosimilars development 4. Tough approval process for pharama companies to enter global market 5. Delay in clinical trials approval, new pharma pricing policy, uniform code for sales and marketing practises, compulsory licencing, product quality, regularity uncertainty, reluctant to prescribe, and production complexity 6. Substantial competition from branded biologics than the tough competition as posed by small-molecule generics |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panda, S.; Singh, P.K.; Mishra, S.; Mitra, S.; Pattnaik, P.; Adhikary, S.D.; Mohapatra, R.K. Indian Biosimilars and Vaccines at Crossroads–Replicating the Success of Pharmagenerics. Vaccines 2023, 11, 110. https://doi.org/10.3390/vaccines11010110
Panda S, Singh PK, Mishra S, Mitra S, Pattnaik P, Adhikary SD, Mohapatra RK. Indian Biosimilars and Vaccines at Crossroads–Replicating the Success of Pharmagenerics. Vaccines. 2023; 11(1):110. https://doi.org/10.3390/vaccines11010110
Chicago/Turabian StylePanda, Sunita, Puneet Kumar Singh, Snehasish Mishra, Sagnik Mitra, Priyabrata Pattnaik, Sanjib Das Adhikary, and Ranjan K. Mohapatra. 2023. "Indian Biosimilars and Vaccines at Crossroads–Replicating the Success of Pharmagenerics" Vaccines 11, no. 1: 110. https://doi.org/10.3390/vaccines11010110