
Cutaneous Adverse Reactions to SARS-CoV-2 Vaccines: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Registration of the Protocol
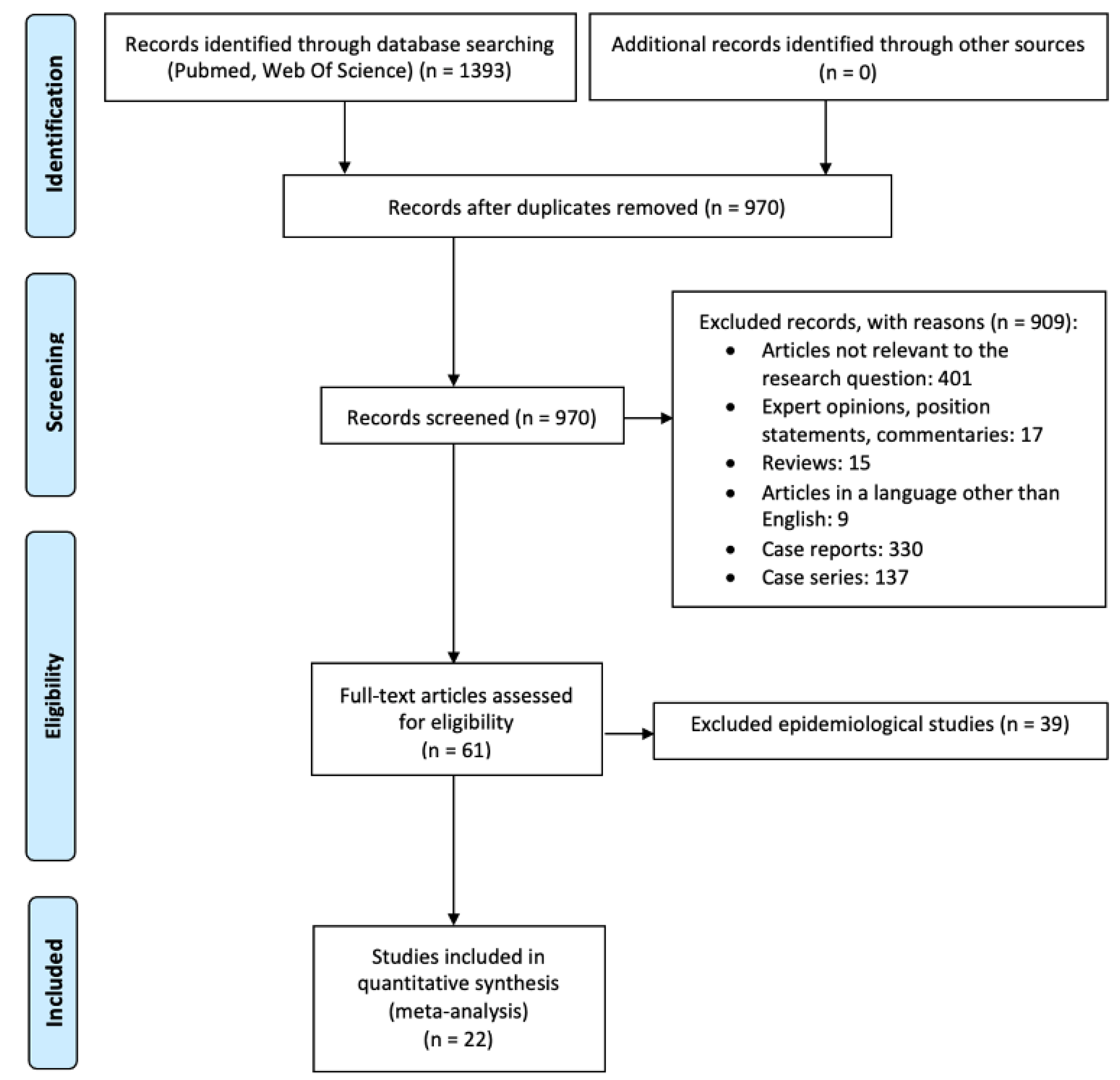
2.2. Search Strategy
2.3. Study Selection Criteria
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Statistical Analysis and Synthesis
3. Results
3.1. Characteristics of the Included Articles
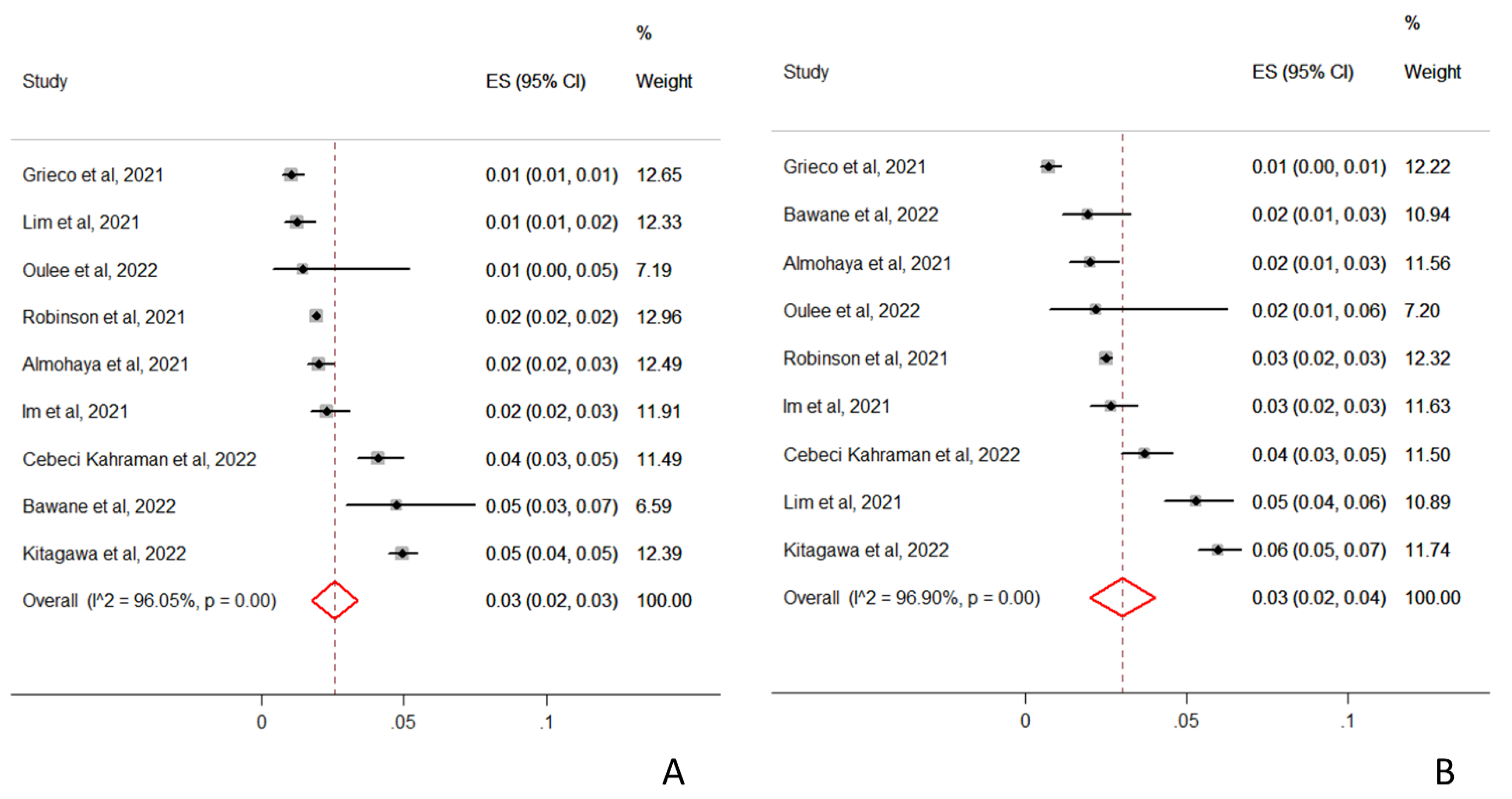
3.2. Incidence of Cutaneous Adverse Reactions
3.3. Risk of Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ledford, H.; Cyranoski, D.; Van Noorden, R. The UK has approved a COVID vaccine-here’s what scientists now want to know. Nature 2020, 588, 205–206. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/vaccines-covid-19/covid-19-vaccines-authorised (accessed on 1 August 2022).
- Mahroum, N.; Lavine, N.; Ohayon, A.; Seida, R.; Alwani, A.; Alrais, M.; Zoubi, M.; Bragazzi, N.L. COVID-19 Vaccination and the Rate of Immune and Autoimmune Adverse Events Following Immunization: Insights from a Narrative Literature Review. Front. Immunol. 2022, 13, 72683. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Bellinato, F.; Maurelli, M.; Gisondi, P.; Girolomoni, G. Cutaneous Adverse Reactions Associated with SARS-CoV-2 Vaccines. J. Clin. Med. 2021, 10, 5344. [Google Scholar] [CrossRef]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid.-Based Healthc. Sept. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Available online: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Prevalence_Studies2017_0.pdf (accessed on 1 August 2022).
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Al Bahrani, S.; Albarrak, A.; Alghamdi, O.A.; Alghamdi, M.A.; Hakami, F.H.; Al Abaadi, A.K.; Alkhrashi, S.A.; Alghamdi, M.Y.; Almershad, M.M.; Alenazi, M.M.; et al. Safety and Reactogenicity of the ChAdOx1 (AZD1222) COVID-19 Vaccine in Saudi Arabia. Int. J. Infect. Dis. 2021, 110, 359–362. [Google Scholar] [CrossRef]
- Almohaya, A.M.; Qari, F.; Zubaidi, G.A.; Alnajim, N.; Moustafa, K.; Alshabi, M.M.; Alsubaie, F.M.; Almutairi, I.; Alwazna, Q.; Al-Tawfiq, J.A.; et al. Early solicited adverse events following the BNT162b2 mRNA vaccination, a population survey from Saudi Arabia. Prev. Med. Rep. 2021, 24, 101595. [Google Scholar] [CrossRef]
- Bawane, J.; Kataria, R.; Mohite, A.; Verma, K.; Shukla, U. Cutaneous adverse effects of the available COVID-19 vaccines in India: A questionnaire-based study. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e619–e622. [Google Scholar] [CrossRef] [PubMed]
- Bostan, E.; Yel, B.; Karaduman, A. Cutaneous adverse events following 771 doses of the inactivated and mRNA COVID-19 vaccines: A survey study among health care providers. J. Cosmet. Dermatol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, A.E.; Almutlq, M.M.; Bin Dakhil, A.A.; Alhetheli, G.I.; Alfouzan, S.K.; Alqahtani, M.A.; Aljalfan, A.A.; Almutawa, M.A.; Alsubaie, F.S.; Madani, A.N. Cutaneous adverse reactions to coronavirus vaccines: A Saudi nationwide study. Dermatol. Ther. 2022, 35, e15452. [Google Scholar] [CrossRef]
- Cebeci Kahraman, F.; Savaş Erdoğan, S.; Aktaş, N.D.; Albayrak, H.; Türkmen, D.; Borlu, M.; Arıca, D.A.; Demirbaş, A.; Akbayrak, A.; Polat Ekinci, A.; et al. Cutaneous reactions after COVID-19 vaccination in Turkey: A multicenter study. J. Cosmet. Dermatol. 2022. [Google Scholar] [CrossRef]
- Das, P.; Arora, S.; Singh, G.K.; Bellad, P.; Rahman, R.; Bahuguna, A.; Sapra, D.; Shrivastav, R.; Gupta, A. A study of COVID-19 vaccine (Covishield) induced dermatological adverse effects from India. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e402–e404. [Google Scholar] [CrossRef]
- Durmaz, K.; Aykut Temiz, S.; Metin, Z.; Dursun, R.; Abdelmaksoud, A. Allergic and cutaneous reactions following inactivated SARS-CoV-2 vaccine (CoronaVac®) in healthcare workers. Clin. Exp. Dermatol. 2022, 47, 171–173. [Google Scholar] [CrossRef]
- Farinazzo, E.; Ponis, G.; Zelin, E.; Errichetti, E.; Stinco, G.; Pinzani, C.; Gambelli, A.; De Manzini, N.; Toffoli, L.; Moret, A.; et al. Cutaneous adverse reactions after m-RNA COVID-19 vaccine: Early reports from Northeast Italy. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e548–e551. [Google Scholar] [CrossRef]
- Grieco, T.; Maddalena, P.; Sernicola, A.; Muharremi, R.; Basili, S.; Alvaro, D.; Cangemi, R.; Rossi, A.; Pellacani, G. Cutaneous adverse reactions after COVID-19 vaccines in a cohort of 2740 Italian subjects: An observational study. Dermatol. Ther. 2021, 34, e15153. [Google Scholar] [CrossRef]
- Im, J.H.; Kim, E.; Lee, E.; Seo, Y.; Lee, Y.; Jang, Y.; Yu, S.; Maeng, Y.; Park, S.; Park, S.; et al. Adverse Events with the Pfizer-BioNTech COVID-19 Vaccine among Korean Healthcare Workers. Yonsei Med. J. 2021, 62, 1162–1168. [Google Scholar] [CrossRef]
- Kitagawa, H.; Kaiki, Y.; Sugiyama, A.; Nagashima, S.; Kurisu, A.; Nomura, T.; Omori, K.; Akita, T.; Shigemoto, N.; Tanaka, J.; et al. Adverse reactions to the BNT162b2 and mRNA-1273 mRNA COVID-19 vaccines in Japan. J. Infect. Chemother. 2022, 28, 576–581. [Google Scholar] [CrossRef]
- Klugar, M.; Riad, A.; Mekhemar, M.; Conrad, J.; Buchbender, M.; Howaldt, H.P.; Attia, S. Side Effects of mRNA-Based and Viral Vector-Based COVID-19 Vaccines among German Healthcare Workers. Biology 2021, 10, 752. [Google Scholar] [CrossRef]
- Lim, S.M.; Chan, H.C.; Santosa, A.; Quek, S.C.; Liu, E.H.C.; Somani, J. Safety and side effect profile of Pfizer-BioNTech COVID-19 vaccination among healthcare workers: A tertiary hospital experience in Singapore. Ann. Acad. Med. Singap. 2021, 50, 703–711. [Google Scholar] [CrossRef]
- Oulee, A.; Salem, S.; Yahia, R.; Yang, K.; Garcia, D.; Holmes, A.; Furukawa, B. Cutaneous reactions due to Pfizer’s BNT162b2 mRNA and Moderna’s mRNA-1273 vaccines. J. Eur. Acad. Dermatol Venereol. 2022, 36, e332–e334. [Google Scholar] [CrossRef]
- Pourani, M.R.; Shahidi Dadras, M.; Salari, M.; Diab, R.; Namazi, N.; Abdollahimajd, F. Cutaneous adverse events related to COVID-19 vaccines: A cross-sectional questionnaire-based study of 867 patients. Dermatol. Ther. 2022, 35, e15223. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Mekhemar, M.; Conrad, J.; Klugarová, J.; Koščík, M.; Klugar, M.; Attia, S. Safety of ChAdOx1 nCoV-19 Vaccine: Independent Evidence from Two EU States. Vaccines 2021, 9, 673. [Google Scholar] [CrossRef]
- Riad, A.; Hocková, B.; Kantorová, L.; Slávik, R.; Spurná, L.; Stebel, A.; Havriľak, M.; Klugar, M. Side Effects of mRNA-Based COVID-19 Vaccine: Nationwide Phase IV Study among Healthcare Workers in Slovakia. Pharmaceuticals 2021, 14, 873. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Klugarová, J.; Antalová, N.; Kantorová, L.; Koščík, M.; Klugar, M. Side Effects of mRNA-Based COVID-19 Vaccines among Young Adults (18-30 Years Old): An Independent Post-Marketing Study. Pharmaceuticals 2021, 14, 1049. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 Vaccine Side Effects among Healthcare Workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef]
- Robinson, L.B.; Fu, X.; Hashimoto, D.; Wickner, P.; Shenoy, E.S.; Landman, A.B.; Blumenthal, K.G. Incidence of Cutaneous Reactions After Messenger RNA COVID-19 Vaccines. JAMA Dermatol. 2021, 157, 1000–1002. [Google Scholar] [CrossRef]
- Ruiz-Villaverde, R.; Rivera-Izquierdo, M.; Gil-Villalba, A.; Pegalajar-García, M.D.; Pérez-Rojas, J.; Soler-Iborte, E.; Valero-Ubierna, M.C. Dermatological adverse reactions after vaccination with BNT162b2 in a cohort of healthcare workers. Int. J. Dermatol. 2022. [Google Scholar] [CrossRef]
- Available online: https://cioms.ch/publications/product/cioms-cumulative-pharmacovigilance-glossary/ (accessed on 1 August 2022).
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Dey, S.K. Efficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 714170. [Google Scholar] [CrossRef] [PubMed]
- Washrawirul, C.; Triwatcharikorn, J.; Phannajit, J.; Ullman, M.; Susantitaphong, P.; Rerknimitr, P. Global prevalence and clinical manifestations of cutaneous adverse reactions following COVID-19 vaccination: A systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Bonetto, C.; Trotta, F.; Felicetti, P.; Alarcón, G.S.; Santuccio, C.; Bachtiar, N.S.; Pernus, Y.B.; Chandler, R.; Girolomoni, G.; Hadden, R.D.; et al. Vasculitis as an adverse event following immunization-Systematic literature review. Vaccine 2016, 34, 6641–6651. [Google Scholar] [CrossRef] [PubMed]
- Nikkels, A.F.; Nikkels-Tassoudji, N.; Piérard, G.E. Cutaneous adverse reactions following anti-infective vaccinations. Am. J. Clin. Dermatol. 2005, 6, 79–87. [Google Scholar] [CrossRef]
- Rosenblatt, A.E.; Stein, S.L. Cutaneous reactions to vaccinations. Clin. Dermatol. 2015, 33, 327–332. [Google Scholar] [CrossRef]
- Kounis, N.G.; Koniari, I.; de Gregorio, C.; Velissaris, D.; Petalas, K.; Brinia, A.; Assimakopoulos, S.F.; Gogos, C.; Kouni, S.N.; Kounis, G.N.; et al. Allergic reactions to current available COVID-19 vaccinations: Pathophysiology, causality, and therapeutic considerations. Vaccines 2021, 9, 211. [Google Scholar] [CrossRef]
- Freeman, E.E.; Sun, Q.; McMahon, D.E.; Singh, R.; Fathy, R.; Tyagi, A.; Blumenthal, K.; Hruza, G.J.; French, L.E.; Fox, L.P. Skin reactions to COVID-19 vaccines: An American Academy of Dermatology/International League of Dermatological Societies registry update on reaction location and COVID vaccine type. J. Am. Acad. Dermatol. 2022, 86, e165–e167. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| First Author | Study Population | Sample Size | Country | Age, Mean (SD) | Female (%) | Time-Frame | Vaccine Producer | General Incidence of CARs (%) |
|---|---|---|---|---|---|---|---|---|
| Al Bahrani et al. | General population | 1592 | Saudi Arabia | 37.4 (9.6) | 19 | 10 April–20 May 2021 | Astra Zeneca | NR |
| Almohaya et al. | General population | 3639 | Saudi Arabia | 37.0 (28.0–48.0) * | 63.3 | 29 May–8 June 2021 | Pfizer-BioNTech | 73/3639 (2.00%) |
| Bawane et al. | Healthcare workers | 1029 | India | NR | NR | 16 January–16 August 2021 | Covishield-Astra Zeneca, Covaxin | 30/1029 (2.92%) |
| Bostan et al. | Healthcare workers | 234 | Turkey | 31.51 (9.25) | 67.1 | NR | CoronaVac, Pfizer-BioNTech | 2/234 (0.85%) |
| Bukhari et al. | General population | 1021 | Saudi Arabia | NR | 70.7 | 1 June–30 September 2021 | Astra Zeneca, Pfizer-BioNTech | 51/1021 (5.00%) |
| Cebeci Kahraman et al. | General population | 2189 | Turkey | 50,4 (17.9) | 56.4 | 15 April–15 July 2021 | CoronaVac, Pfizer-BioNTech | 175/2189 (7.99%) |
| Das et al. | General population | 4063 | India | 36.7 (19–86) ^ | 37 | September–November 2021 | Covishield-Astra Zeneca | 50/4063 (1.23%) |
| Durmaz et al. | Healthcare workers | 221 | Turkey | Male: 37.03 (13.83)Female: 38.56 (13.29) | 50.2 | January–March 2021 | CoronaVac | NR |
| Farinazzo et al. | Healthcare workers | 19485 | Italy | NR | NR | January 2021 | Pfizer-BioNTech | 28/19485 (0.14%) |
| Grieco et al. | Healthcare workers | 2740 | Italy | NR | NR | January–July 2021 | Moderna, Pfizer-BioNTech, Astra Zeneca | 50/2740 (1.82%) |
| Im et al. | Healthcare workers | 2498 | South Korea | NR | NR | March–April 2021 | Pfizer-BioNTech | 93/2498 (3.72%) |
| Kitagawa et al. | Healthcare workers | 12,109 | Japan | NR | § | 15–19 July and 19–22 August 2021 | Moderna, Pfizer-BioNTech | 648/12109 (5.35%) |
| Klugar et al. | Healthcare workers | 599 | Germany | 39 * | §§ | February–April 2021 | Moderna, Pfizer-BioNTech, Astra Zeneca | 21/599 (3.51%) |
| Lim et al. | Healthcare workers | 1704 | Singapore | NR | NR | February–April 2021 | Pfizer-BioNTech | 132/1704 (7.75%) |
| Oulee et al. | Healthcare workers | 137 | USA | NR | 54.7 | 29 March–29 May 2021 | Moderna, Pfizer-BioNTech | 5/137 (3.64%) |
| Pourani et al. | Healthcare workers | 761 | Iran | 28.08 (11.94) | 70.3 | June–July 2021 | Astra Zeneca, Sinopharm, Sputnik, Bharat, Cuba-Pasteur, Pfizer-BioNTech, Moderna | 95/761 (12.48%) |
| Riad et al. 1 | Healthcare workers | 92 | Germany, Czech Republic | 35.37 (12.62) | 77.2 | February–March 2021 | Astra Zeneca | 4/92 (4.34%) |
| Riad et al. 2 | Healthcare workers | 522 | Slovakia | 37.77 (11.61) | 77 | February–March 2021 | Moderna, Pfizer-BioNTech, Astra Zeneca | 18/522 (3.45%) |
| Riad et al. 3 | General Population | 539 | Czech Republic | 22.86 (2.05) | 70.1 | April–June 2021 | Moderna, Pfizer-BioNTech | 4/539 (0.74%) |
| Riad et al. 4 | Healthcare workers | 877 | Czech Republic | 42.56 (10.5) | 88.5 | 27 January–27 February 2021 | Pfizer-BioNTech | 45/877 (5.13%) |
| Robinson et al. | Healthcare workers | 33039 | USA | NR | NR | December 2020–February 2021 | Moderna, Pfizer-BioNTech | 1541/33039 (4.66%) |
| Ruiz-Villaverde et al. | Healthcare workers | 3969 | Spain | 46.4 (13.9) | 73.1 | 27 December 20–1 September 2021 | Pfizer-BioNTech | 13/3969 (0.33%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellinato, F.; Fratton, Z.; Girolomoni, G.; Gisondi, P. Cutaneous Adverse Reactions to SARS-CoV-2 Vaccines: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1475. https://doi.org/10.3390/vaccines10091475
Bellinato F, Fratton Z, Girolomoni G, Gisondi P. Cutaneous Adverse Reactions to SARS-CoV-2 Vaccines: A Systematic Review and Meta-Analysis. Vaccines. 2022; 10(9):1475. https://doi.org/10.3390/vaccines10091475
Chicago/Turabian StyleBellinato, Francesco, Zeno Fratton, Giampiero Girolomoni, and Paolo Gisondi. 2022. "Cutaneous Adverse Reactions to SARS-CoV-2 Vaccines: A Systematic Review and Meta-Analysis" Vaccines 10, no. 9: 1475. https://doi.org/10.3390/vaccines10091475