
Adult-Onset Familial Hemophagocytic Lymphohistiocytosis Presenting with Annular Erythema following COVID-19 Vaccination

1
Department of Dermatology, Jinling Hospital, Nanjing Medical University, Nanjing 210002, China
2
Department of Dermatology, Jinling Hospital, Nanjing University, Nanjing 210002, China
*
Authors to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Vaccines 2022, 10(9), 1436; https://doi.org/10.3390/vaccines10091436
Submission received: 22 July 2022
/
Revised: 22 August 2022
/
Accepted: 22 August 2022
/
Published: 31 August 2022
(This article belongs to the Special Issue Adverse Events of COVID-19 Vaccines)
Abstract
:Familial hemophagocytic lymphohistiocytosis (HLH) is a rare genetic and life-threatening immunodeficiency disease. Here, we present a 38-year-old male who initially developed multiple annular to irregular erythema accompanied by a fever after COVID-19 vaccination. He was diagnosed with HLH with evidence of leukocytopenia in a full blood test, elevations of ferritin and sCD25, decreased NK cell function, and hemophagocytosis of a bone marrow biopsy specimen. A genetic examination revealed two probable disease-causing heterozygous mutations on UNC13D associated with type 3 familial HLH. A review of the case reports relevant to HLH following COVID-19 vaccination and the cutaneous manifestations of HLH with genetic defects suggests the necessity that individuals with preexisting immune dysregulation or diseases not classified should be cautious about COVID-19 vaccination and reminds clinicians that various recalcitrant skin lesions may be a sign of HLH.
1. Introduction
Hemophagocytic lymphohistiocytosis (HLH) is a rare and life-threatening immune-mediated syndrome characterized by uncontrolled and persistent activation of cytotoxic T lymphocytes and natural killer (NK) cells, leading to overwhelming systemic inflammation [1]. According to the etiologies, HLH is often categorized as primary and secondary/reactive HLH. Primary HLH is caused by genetic defects affecting the cytotoxic function of T lymphocytes and NK cells and normally presents in young children [1,2]. Primary HLH, including familial HLH and related immune disorders associated with an HLH phenotype, have been defined as autosomal recessive diseases. Most pediatric patients have identifiable genetic defects inherited in a Mendelian fashion as homozygous or compound heterozygous lesions [1,3]. Secondary HLH, generally affecting adolescents and adults, is always associated with diseases causing immune dysregulation in the absence of an identifiable underlying genetic mutation, such as infection, malignancy (particularly lymphoma), autoimmune conditions, or other circumstances [2,4].
HLH is primarily triggered by herpes and EB viruses but may be associated with other viral, bacterial, fungal, and parasitic infections or some non-infectious triggers such as drugs, vaccinations, surgery, and severe burns [5]. HLH induced by vaccination is uncommon. With the COVID-19 pandemic, the emerging SARS-CoV-2 vaccines have been widely applied in epidemic prevention and control. Although the benefits of the vaccines are undoubted, the adverse effects may be neglected and deserve more studies to elaborate on this topic.
Herein, we report a 38-year-old male with an initial presentation of widespread annular erythema on the trunk following SARS-CoV-2 vaccination, who was subsequently diagnosed with familial HLH. This is the first case of HLH triggered by COVID-19 vaccination immunostimulation on a genetic defect of a UNC13D background.
2. Case Report
A 38-year-old man was presented to our department with multiple pruritic annular to irregular erythema on the trunk for 2 months. He had received the COVID-19 vaccination approximately 4 weeks before the appearance of skin rashes. The patient suffered from severe interstitial pneumonia of unknown causes 3 years ago and was in stable condition in recent years. He was suspected of urticarial vasculitis (UV), erythema annulare centrifugum (EAC), or eosinophilic annular erythema (EAE). However, the histopathology indicated perivascular and periappendage infiltration comprising histocytes and atypical lymphocytes, with an obvious involvement of nerves (Figure 1). Meanwhile, complete blood count, immune serum globulin, complement and complete autoimmune antibody tests, including anti-nuclear antibody (ANA) spectrum, antibodies to double-stranded DNA (anti-dsDNA) antibody, anti-neutrophil cytoplasmic antibodies (ANCA), anti-cardiolipin antibody (ACA), rheumatoid factor (RF), etc., were all at normal levels. Thus, the diagnoses of UV, EAC, and EAE were excluded. Given the involvement of nerves in the pathologic findings, the possibility of leprosy was taken into account. However, immunofluorescence, acid-fast staining, enzyme-linked immunospot assay (ELISPOT), and next-generation sequencing (NGS) all showed no evidence of mycobacterium leprae infection. He was then treated with antihistamines, glucocorticosteroid, and thalidomide, with mild alleviation of the lesions.
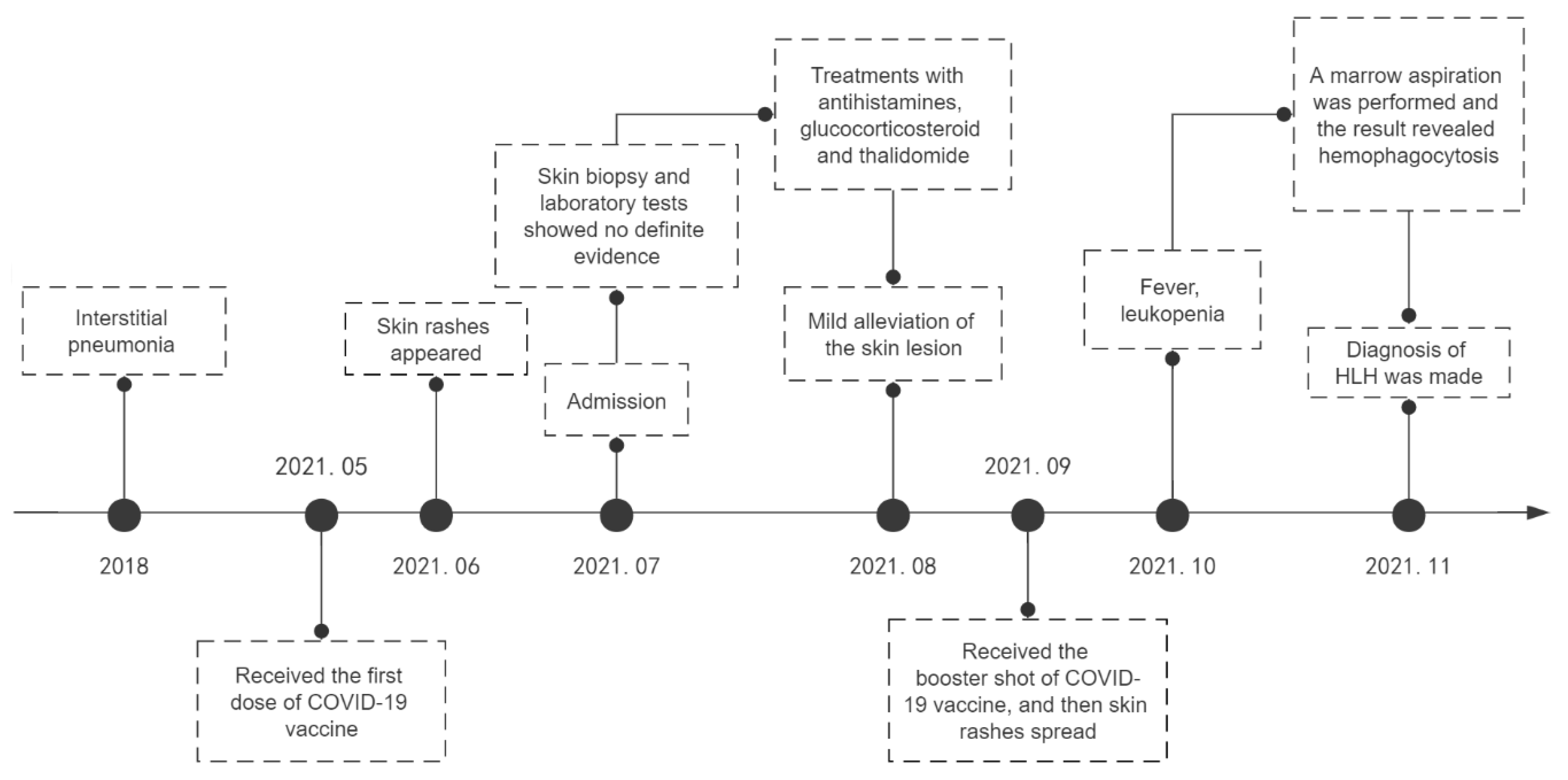
However, the lesions spread rapidly shortly after the patient received the booster shot of the COVID-19 vaccine, presenting with generalized pruritic annular to irregular erythema, accompanied by edema on his left face (Figure 2). Almost one month later, new accompanying symptoms, including a high fever and fatigue, appeared. A whole-blood test indicated leukocytopenia (WBC 2.09 × 109/L). Marrow aspiration was performed, and the result revealed the phagocytosis of platelets, erythrocytes, granulocytes, and other granular fragments by a number of hemophagocytes in the bone marrow smears. Meanwhile, he had dramatically elevated levels of ferritin and sCD25 and decreased NK cell function. The results of the laboratory tests are summarized in Table 1. Based on the HLH-2004 diagnostic criteria, a diagnosis of hemophagocytic lymphohistiocytosis was confirmed. A coherent timeline indicating the date of this case is presented in Figure 3.
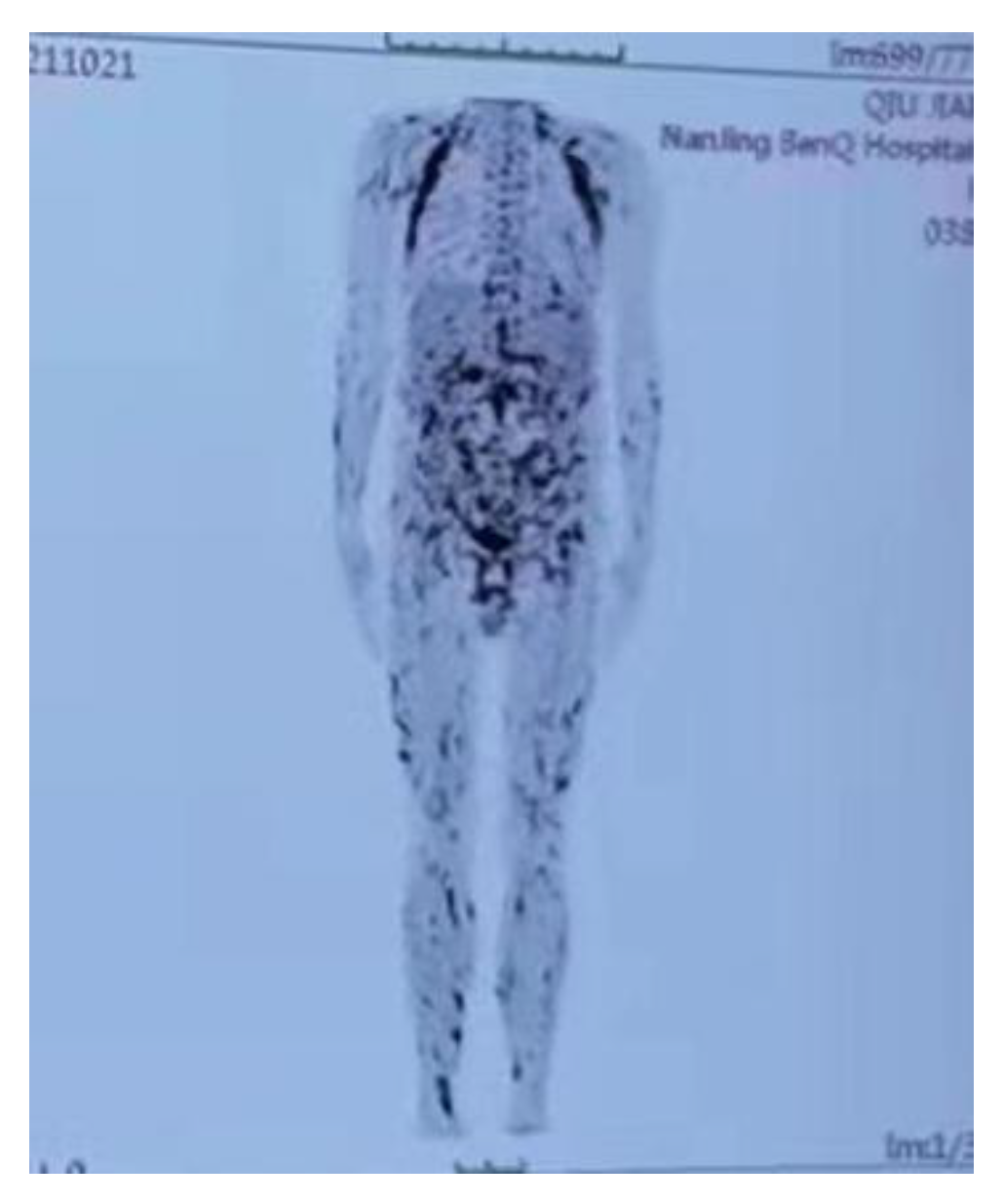
It is known that infection, malignancy (especially lymphoma), autoimmune disease, and gene deficiency are common etiologies of HLH. Therefore, a series of examinations were carried out to explore the underlying causes. Hepatitis B and C virus (HBV and HCV) screening, HIV screening, and a syphilis serum test were all negative, and NGS detected no pathogenic microorganisms in skin and blood specimens. Positron emission tomography/computed tomography (PET/CT) revealed widespread increased metabolic activity (Figure 4). A repeated skin biopsy was performed to exclude the diagnosis of lymphoma. The histopathology revealed lymphohistiocytic infiltration in the dermis as well as reactive hyperplasia of lymphoid tissue dominated by cytotoxic T-cells. Immunohistochemistry showed that these cells were positive for CD3, CD2, CD5, CD7, CD4, CD43, TIA, GrB, and perforin, weak-positive for CD8, P53, C-myc, Ki-67 (20–30%), and negative for CD21, CD23, CD20, CD56, MUM1, cyclinD1, CD10, Bc16, PAX5, CD30, PD1, CD38, kappa, lambda, and EBER. Lymphoma was also excluded based on the existing evidence, while genetic examination revealed two probable disease-causing heterozygous mutations on UNC13D, c.817C > T (p.R273*) and c.2588G > A (p.G863D), respectively. Therefore, the gene mutation was considered the cause of HLH. Furthermore, his mother was found to be a carrier of the UNC13D (p.R273*) mutation, and his father was found to be a carrier of the UNC13D (p.G863D) mutation. Finally, this patient was diagnosed as familial HLH type 3, with a mutation of UNC13D triggered by COVID-19 vaccination. The patient was given the therapy of an allogeneic bone marrow transplant.
3. Literature Review
3.1. HLH following COVID-19 Vaccination
English language cases of HLH following COVID-19 vaccination were reviewed and analyzed using the PubMed database from the date of database inception until 20 June 2022; “(COVID-19 OR SARS-CoV-2) AND (vaccine OR vaccination) AND (hemophagocytic lymphohistiocytosis OR hemophagocytic syndrome)” was used as a search filter.
A total of 12 pieces of literature with 20 HLH cases are included and summarized in Table 2, of which 12 cases were males (60.0%) with a mean age of onset of 48.10 years (14–85 years); 6/20 (30.0%) cases were accompanied by skin manifestations, including maculopapules, pruritus, jaundice, and facial swelling. Our case is the only one that presented with isolated skin lesions initially. The mean interval between onset symptoms and vaccination was 9.31 days (1–28 days); 10/20 (50.0%) patients had underlying medical conditions such as interstitial lung disease, HIV, adult-onset Still’s disease, diabetes mellitus, malignancy, heart failure; 4/20 (20.0%) patients were positive for EBV infection. Only one case explored the predisposing gene mutation without a positive result, and our patient is the first one who has tested positive for genetic mutations. The main therapy was corticosteroid in 17 out of 19 patients (89.47%). The common combination treatments included intravenous immunoglobulins (IVIG) (6/19, 31.58%), etoposide (4/19, 21.05%), anakinra (4/19, 21.05%), rituximab (1/19, 5.26%), infliximab (1/19, 5.26%) and emapalumab-lzsg (1/19, 5.26%). The conditions of 15/19 (78.95%) patients improved after multiple treatments, but two of them relapsed and got worse after discharge; 3/19 (15.79%) patients died of HLH or complications. The patients with other systemic conditions had worse prognoses. Only one improved spontaneously with no therapy due to clinical stability and improvement of HLH parameters.
3.2. Cutaneous Manifestations of HLH with Genetic Defects
English language cases of cutaneous manifestations of HLH with genetic defects were identified and analyzed using the PubMed database from the date of database inception until 20 June2022; “(skin OR cutaneous) AND (hemophagocytic lymphohistiocytosis OR hemophagocytic syndrome)” was used as a search filter.
A total of 19 case reports are shown in Table 3, of which 11 cases were males (57.89%) with ages of onset ranging from 6 days to 30 years old; 3/19 (15.80%) patients presented with initially isolated skin lesions. The subtypes of Griscelli syndrome type 2 and Chediak–Higashi syndrome were characterized by cutaneous hypopigmentation, while cutaneous manifestations were nonspecific to other subtypes. The nonspecific skin manifestations included edema (3/19, 15.80%), widespread maculopapular rash (2/19, 10.53%), papulopustules (2/19, 10.53%), granuloma (2/19, 10.53%), erythema nodosum (1/19, 5.26%), panniculitis (2/19, 10.53%), violaceous nodules (1/19, 5.26%), ecchymosis (1/19, 5.26%), and hemorrhagic skin eruptions (1/19, 5.26%). The histologic appearances were nonspecific and rarely demonstrated cutaneous hemophagocytosis. The main treatments were induction therapy, including corticosteroid (13/15, 86.67%), etoposide (7/15, 46.67%), and cyclosporine (8/15, 53.33%); 7/15 (46.67%) patients underwent or had planned to undergo hematopoietic stem cell transplantation (HSCT). Additionally, other treatments, including IVIG (1/15, 6.67%), mycophenolate mofetil (1/15, 6.67%), and 13-cis retinoic acid (1/15, 6.67%), were applied to patients. The conditions of 6 (31.58%) cases improved after multiple treatments, 7 (36.84%) cases died of HLH or complications, and 6 cases did not provide the outcomes.
4. Discussion
Hemophagocytic lymphohistiocytosis (HLH) is a rare, life-threatening hyperinflammatory syndrome characterized by an uncontrollable immune response, resulting in increased secretion of inflammatory cytokines and macrophage activation [1]. Primary HLH occurs in the presence of an underlying predisposing genetic defect damaging the immune function. The genetic defects causing primary HLH are listed in Table 4. Two probable disease-causing heterozygous mutations on UNC13D were identified in the present case, which confirmed the diagnosis of F-HLH type 3 (FH3). It is known that UNC13D encodes the protein Munc13-4, which participates in the regulation of cytolytic granule maturation and exocytosis. The absence of Munc13-4 often causes the impairment of cytotoxic activity in T lymphocytes, leading to sequential reactions of inability to clear antigenic stimulus, the exuberant production of cytokines, and infiltration with hyperactivated macrophages and histiocytes in organ systems [1,37].
Notably, the patient provided an important fact that the lesions were stirred up after the first dose of the COVID-19 vaccine; he deteriorated significantly after the booster shot. Therefore, vaccination was considered the trigger of the present HLH patient’s underlying genetic defect by excluding other precipitating factors relevant to HLH. The mechanisms of COVID-19-vaccine-related HLH have not been illuminated. We hypothesize that increases in proinflammatory cytokines resulting from the vaccination provide an initial stimulus for the activation of cytotoxic T lymphocytes and NK cells; the impaired cytotoxic function in T lymphocytes, due to the genetic defect, leads to an inability to eliminate the antigenic stimulus, which then eventually results in a persistent and amplifying immune response [1,38].
Only 1 of the 20 HLH patients (following COVID-19 vaccination) from the reviewed literature explored the predisposing gene mutation but without positive results. The present patient was the first reported case with underlying genetic defects. Some scholars have proposed that the screening sequencing of HLH-associated genes is unnecessary in adult HLH cases as genetic predisposition plays a primary role in pediatric settings [39]. However, 42.9% (48/112) of patients harbored pathogenic gene mutations or rare variants in adults with HLH in Miao’s research (Miao et al. [40]). With the widespread availability of genetic testing, HLH has been described to occur throughout life, from in utero to the seventh decade [41]. Miao et al. found nonsense and frame-shift mutations were prevalent in pediatric cases, while almost all the variants were missense mutations in adult cases. Hence, he speculated that most gene mutations in adult HLH may partly impair rather than eliminate the function of the involved proteins [40]. HLH is susceptible in individuals with gene mutations after the stimulation of various triggers or predisposing disorders. Therefore, the COVID-19 vaccine may have played a stimulating role in the present HLH patient with genetic defects of UNC13D. The present case had a history of severe interstitial pneumonia of unknown causes, and the skin lesions had not been classified. Therefore, individuals with preexisting immune dysregulation or diseases not classified should be cautious about vaccination. Gene sequencing may be considered to exclude the underlying predisposing genetic defect before vaccination in some circumstances.
The initial symptoms of HLH are variable and nonspecific, leading to difficulty in early diagnosis. The clinical presentations include a continuous high fever (>38.5 °C) of unknown origin, hepatosplenomegaly, cytopenias, skin rashes, acute liver failure, bleeding, and inflammatory central nervous system disease [42]. Cutaneous manifestations are variable and nonspecific, with an estimated prevalence of 24–40% in primary HLH and 6–65% in secondary HLH, which can be easily neglected by clinicians [43]. The current case was suspected of HLH until he presented manifestations of fever and leukocytopenia and was misdiagnosed with several diseases such as urticarial vasculitis, erythema annulare centrifugum, and leprosy for the nonspecific symptoms at the earlier disease stage. Therefore, the characteristic of cutaneous manifestations of HLH represents a diagnostic challenge for clinicians, which may provide a clue for earlier diagnosis. Fardet et al. [44] summarized that the cutaneous manifestations of reactive HLH mainly fell into three types: (i) specific to the underlying malignancy (e.g., cutaneous lymphoma, systemic disease), (ii) reflecting biological consequences of HLH (e.g., conjunctival jaundice, thrombogenic purpura), and (iii) a generalized, transient, nonpruriginous maculopapular rash. In addition, generalized erythroderma, edema, nonhealing ulcers, panniculitis, and Kawasaki-like abnormalities have also been reported to occur in HLH [43].
To explore the characteristics of cutaneous manifestations in HLH with genetic defects, we have summarized previous HLH cases caused by genetic defects accompanied by skin involvement. Hyperpigmentation, edema, erythema nodosum, maculopapular rashes, annular erythema, jaundice, and pustules are unusual skin manifestations of genetic defects related to HLH. Grisccelli syndrome type 2 and Chediak–Higashi syndrome are specific subtypes characterized by cutaneous hyperpigmentation, while cutaneous manifestations are nonspecific to other subtypes. In addition, the histologic appearances were nonspecific and rarely demonstrated cutaneous hemophagocytosis. The typical histological features are described as a lymphohistiocytic perivascular infiltrate in the reticular dermis, without evidence of epidermal changes or vasculitis, which is consistent with the skin biopsy in our case [45]. Hence, it is necessary to perform a marrow aspiration to exclude the possibility of HLH when various skin manifestations are incurable with routine treatments.
5. Conclusions
This study presents the first HLH case with stirred-up isolated skin lesions following COVID-19 vaccination with the background of a genetic defect of UNC13D. Without suggestive tests, the nonspecific and isolated lesions made it dramatically difficult to direct the diagnosis of HLH at an early stage. Clinicians should be aware of the possibility of HLH when unclassified skin lesions cannot be cured with routine treatments, and a marrow aspiration may be necessary to make a definite diagnosis. The adverse effects of COVID-19 vaccination should be made known, and full knowledge of the side effects caused by the vaccine should be analyzed and summarized. Individuals with preexisting systemic conditions should be cautious about vaccination and be closely followed up for any suspicious symptoms after vaccination. In the future, more cases should be included in multicentric trials to establish a formal clinical pathway, as in this thesis.
Author Contributions
H.S. and F.L. conceptualized the study. Y.W. performed the literature search. Y.H. (Yifan He) and Y.H. (Yun Hui) prepared the first draft. H.L. and F.L. reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by The Open Project of Jiangsu Biobank of Clinical Resources, No. TC2021B018.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
We thank Hao Chen from the Institute of Dermatology, Chinese Academy of Medical Sciences, for his help with the dermatopathology diagnosis and Yi Miao in the Department of Hematology, The First Affiliated Hospital of Nanjing Medical University, for his help and guidance on genetic detection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Al-Samkari, H.; Berliner, N. Hemophagocytic Lymphohistiocytosis. Annu. Rev. Pathol. 2018, 13, 27–49. [Google Scholar] [CrossRef] [PubMed]
- Schram, A.; Berliner, N. How I treat hemophagocytic lymphohistiocytosis in the adult patient. Blood 2015, 125, 2908–2914. [Google Scholar] [CrossRef] [PubMed]
- Steen, E.A.; Hermiston, M.L.; Nichols, K.E.; Meyer, L.K. Digenic Inheritance: Evidence and Gaps in Hemophagocytic Lym-phohistiocytosis. Front. Immunol. 2021, 12, 777851. [Google Scholar] [CrossRef]
- Hayden, A.; Park, S.; Giustini, D.; Lee, A.Y.; Chen, L.Y. Hemophagocytic syndromes (HPSs) including hemophagocytic lym-phohistiocytosis (HLH) in adults: A systematic scoping review. Blood Rev. 2016, 30, 411–420. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brito-Zerón, P.; López-Guillermo, A.; Khamashta, M.A.; Bosch, X. Adult haemophagocytic syndrome. Lancet 2014, 383, 1503–1516. [Google Scholar] [CrossRef]
- Tang, L.V.; Hu, Y. Hemophagocytic lymphohistiocytosis after COVID-19 vaccination. J. Hematol. Oncol. 2021, 14, 1–5. [Google Scholar] [CrossRef]
- Hieber, M.L.; Sprute, R.; Eichenauer, D.A.; Hallek, M.; Jachimowicz, R.D. Hemophagocytic lymphohistiocytosis after SARS-CoV-2 vaccination. Infection 2022, 1–6. [Google Scholar] [CrossRef]
- Ai, S.; Awford, A.; Roncolato, F. Hemophagocytic lymphohistiocytosis following ChAdOx1 nCov-19 vaccination. J. Med. Virol. 2021, 94, 14–16. [Google Scholar] [CrossRef]
- Nasir, S.; Khan, S.R.; Iqbal, R.; Hashmi, A.P.; Moosajee, M.; Nasir, N. Inactivated COVID-19 vaccine triggering hemophagocytic lymphohistiocytosis in an immunocompetent adult—A case report. J. Clin. Transl. Res. 2022, 8, 152–155. [Google Scholar]
- Caocci, G.; Fanni, D.; Porru, M.; Greco, M.; Nemolato, S.; Firinu, D.; Faa, G.; Scuteri, A.; La Nasa, G. Kikuchi-Fujimoto disease associated with hemophagocytic lymphohistiocytosis following the BNT162b2 mRNA COVID-19 vaccination. Haematologica 2021, 107, 1222–1225. [Google Scholar] [CrossRef]
- Baek, D.W.; Hwang, S.; Kim, J.; Lee, J.M.; Cho, H.J.; Moon, J.-H.; Hwang, N.; Jeong, J.Y.; Lee, S.-W.; Sohn, S.K. Patients presenting high fever with lymphadenopathy after COVID-19 vaccination were diagnosed with hemophagocytic lymphohistiocytosis. Infect. Dis. 2021, 54, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Sassi, M.; Khefacha, L.; Merzigui, R.; Rakez, R.; Boukhriss, S.; Laatiri, M.A. Haemophagocytosis and atypical vacuolated lymphocytes in bone marrow and blood films after SARS-CoV-2 vaccination. Br. J. Haematol. 2021, 195, 649. [Google Scholar] [CrossRef] [PubMed]
- Rocco, J.M.; Mallarino-Haeger, C.; Randolph, A.H.; Ray, S.M.; Schechter, M.C.; Zerbe, C.S.; Holland, S.M.; Sereti, I. Hyperinflammatory Syndromes After Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Messenger RNA vaccination in Individuals With Underlying Immune Dysregulation. Clin. Infect. Dis. 2022, 75, e912–e915. [Google Scholar] [CrossRef]
- Attwell, L.; Zaw, T.; McCormick, J.; Marks, J.; McCarthy, H. Haemophagocytic lymphohistiocytosis after ChAdOx1 nCoV-19 vac-cination. J. Clin. Pathol. 2022, 75, 282–284. [Google Scholar] [CrossRef]
- Wu, V.; Lopez, C.A.; Hines, A.M.; Barrientos, J.C. Haemophagocytic lymphohistiocytosis following COVID-19 mRNA vaccina-tion. BMJ Case Rep. 2022, 15, e247022. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.Y.; Yeh, Y.H.; Chen, L.W.; Cheng, C.-N.; Chang, C.; Roan, J.-N.; Shen, C.-F. Hemophagocytic Lymphohistiocytosis Following BNT162b2 mRNA COVID-19 Vaccina-tion. Vaccines 2022, 10, 573. [Google Scholar] [CrossRef]
- Cory, P.; Lawrence, H.; Abdulrahim, H.; Mahmood-Rao, H.; Hussein, A.; Gane, J. Lessons of the month 3: Haemophagocytic lym-phohistiocytosis following COVID-19 vaccination (ChAdOx1 nCoV-19). Clin. Med. 2021, 21, e677–e679. [Google Scholar] [CrossRef]
- Minocha, P.; Choudhary, R.; Agrawal, A.; Sitaraman, S. Griscelli syndrome subtype 2 with hemophagocytic lympho-histiocytosis: A case report and review of literature. Intractable Rare Dis. Res. 2017, 6, 76–79. [Google Scholar] [CrossRef]
- Mishra, K.; Singla, S.; Sharma, S.; Saxena, R.; Batra, V.V. Griscelli syndrome type 2: A novel mutation in RAB27A gene with different clinical features in 2 siblings: A diagnostic conundrum. Korean J. Pediatr. 2014, 57, 91–95. [Google Scholar] [CrossRef]
- Tewari, N.; Rajwar, A.; Mathur, V.; Chaudhari, P.K. Oral features of Griscelli syndrome type II: A rare case report. Spéc. Care Dent. 2018, 38, 421–425. [Google Scholar] [CrossRef]
- Panigrahi, I.; Suthar, R.; Rawat, A.; Behera, B. Seizure as the Presenting Manifestation in Griscelli Syndrome Type 2. Pediatr. Neurol. 2015, 52, 535–538. [Google Scholar] [CrossRef] [PubMed]
- Meschede, I.; Santos, T.; Izidoro-Toledo, T.; Gurgel-Gianetti, J.; Espreafico, E. Griscelli syndrome-type 2 in twin siblings: Case report and update on RAB27A human mutations and gene structure. Braz. J. Med. Biol. Res. 2008, 41, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Gotesman, R.; Ramien, M.; Armour, C.M.; Pham-Huy, A.; Kirshen, C. Cutaneous granulomas as the presenting manifestation of Griscelli syndrome type 2. Pediatr. Dermatol. 2020, 38, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Li, Q.; Gao, J. Langerhans cell histiocytosis complicated with hemophagocytic lymphohistiocytosis in a boy with a novel XIAP mutation: A case report. Medicine 2018, 97, e13019. [Google Scholar] [CrossRef]
- Kaya, Z.; Ehl, S.; Albayrak, M.; Maul-Pavicic, A.; Schwarz, K.; Kocak, U.; Ergun, M.A.; Gursel, T. A novel single point mutation of the LYST gene in two siblings with different phenotypic features of Chediak Higashi syndrome. Pediatr. Blood Cancer 2011, 56, 1136–1139. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, C.; Agergaard, C.N.; Jakobsen, M.A.; Møller, M.B.; Fisker, N.; Barington, T. Infantile hemophagocytic lymphohistiocytosis in a case of chediak-higashi syndrome caused by a mutation in the LYST/CHS1 gene presenting with delayed umbilical cord de-tachment and diarrhea. J. Pediatr. Hematol. Oncol. 2015, 37, e73–e79. [Google Scholar] [CrossRef]
- Wu, X.; Zhao, X.; Zhang, B.; Xuan, F.; Guo, H.; Ma, F. A novel frameshift mutation of Chediak-Higashi syndrome and treatment in the accelerated phase. Braz. J. Med. Biol. Res. 2017, 50, e5727. [Google Scholar] [CrossRef]
- Morrone, K.; Wang, Y.; Huizing, M.; Sutton, E.; White, J.G.; Gahl, W.A.; Moody, K. Two Novel Mutations Identified in an African-American Child with Chediak-Higashi Syndrome. Case Rep. Med. 2010, 2010, 967535. [Google Scholar] [CrossRef]
- Sheng, L.; Zhang, W.; Gu, J.; Shen, K.; Luo, H.; Yang, Y. Novel mutations of STXBP2 and LYST associated with adult haemophagocytic lymphohistiocytosis with Epstein-Barr virus infection: A case report. BMC Med. Genet. 2019, 20, 34. [Google Scholar] [CrossRef]
- Larson, K.N.; Gaitan, S.R.; Stahr, B.J.; Morrell, D.S. Hemophagocytic Lymphohistiocytosis in a Newborn Presenting as “Blueberry Muffin Baby”. Pediatr. Dermatol. 2017, 34, e150–e151. [Google Scholar] [CrossRef]
- Viñas-Giménez, L.; Rincón, R.; Colobran, R.; de la Cruz, X.; Celis, V.P.; Dapena, J.L.; Alsina, L.; Sayós, J.; Martínez-Gallo, M. Case Report: Characterizing the Role of the STXBP2-R190C Monoallelic Muta-tion Found in a Patient With Hemophagocytic Syndrome and Langerhans Cell Histiocytosis. Front. Immunol. 2021, 12, 723836. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Guo, X.; Li, Q.; Huang, Z. Familial hemophagocytic lymphohistiocytosis type 5 in a Chinese Tibetan patient caused by a novel compound heterozygous mutation in STXBP2. Medicine 2019, 98, e17674. [Google Scholar] [CrossRef] [PubMed]
- Pasqualini, C.; Jorini, M.; Carloni, I.; Giangiacomi, M.; Cetica, V.; Aricò, M.; de Benedictis, F.M. Cytophagic histiocytic panniculitis, hemophagocytic lymphohistiocytosis and unde-termined autoimmune disorder: Reconciling the puzzle. Ital. J. Pediatr. 2014, 40, 17. [Google Scholar] [CrossRef]
- Chen, R.-L.; Hsu, Y.-H.; Ueda, I.; Imashuku, S.; Takeuchi, K.; Tu, B.P.-H.; Chuang, S.-S. Cytophagic histiocytic panniculitis with fatal haemophagocytic lymphohistiocytosis in a paediatric patient with perforin gene mutation. J. Clin. Pathol. 2007, 60, 1168–1169. [Google Scholar] [CrossRef]
- Akyol, S.; Ozcan, A.; Sekine, T.; Chiang, S.C.C.; Yilmaz, E.; Karakurkcu, M.; Patiroglu, T.; Bryceson, Y.; Unal, E. Different Clinical Presentation of 3 Children With Familial Hemophagocytic Lymphohisti-ocytosis With 2 Novel Mutations. J. Pediatr. Hematol. Oncol. 2020, 42, e627–e629. [Google Scholar] [CrossRef] [PubMed]
- Zengin, H.B.; Reyes-Barron, C.; Cusick, E.; Cordisco, M.; Katzman, P.J.; Burack, W.R.; Scott, G.A. Young Boy With Hemophagocytic Lymphohistiocytosis Presenting With Vac-cine-Related Granulomatous Dermatitis: A Case Report and Literature Review. Am. J. Dermatopathol. 2021, 43, e267–e272. [Google Scholar] [CrossRef]
- Wysocki, C.A. Comparing hemophagocytic lymphohistiocytosis in pediatric and adult patients. Curr. Opin. Allergy Clin. Immunol. 2017, 17, 405–413. [Google Scholar] [CrossRef]
- Mascellino, M.T.; Di Timoteo, F.; De Angelis, M.; Oliva, A. Overview of the Main Anti-SARS-CoV-2 Vaccines: Mechanism of Action, Efficacy and Safety. Infect. Drug Resist. 2021, 14, 3459–3476. [Google Scholar] [CrossRef]
- Sprute, R.; Hieber, M.L.; Jachimowicz, R.D. Correspondence to: Hemophagocytic lymphohistiocytosis after SARS-CoV-2 vaccination. Infection 2022, 1–2. [Google Scholar] [CrossRef]
- Miao, Y.; Zhu, H.-Y.; Qiao, C.; Xia, Y.; Kong, Y.; Zou, Y.-X.; Miao, Y.-Q.; Chen, X.; Cao, L.; Wu, W.; et al. Pathogenic Gene Mutations or Variants Identified by Targeted Gene Sequencing in Adults With Hemophagocytic Lymphohistiocytosis. Front. Immunol. 2019, 10, 395. [Google Scholar] [CrossRef]
- Usmani, G.N.; Woda, B.A.; Newburger, P.E. Advances in understanding the pathogenesis of HLH. Br. J. Haematol. 2013, 161, 609–622. [Google Scholar] [CrossRef] [PubMed]
- Risma, K.A.; Marsh, R.A. Hemophagocytic Lymphohistiocytosis: Clinical Presentations and Diagnosis. J. Allergy Clin. Immunol. Pract. 2018, 7, 824–832. [Google Scholar] [CrossRef]
- Zerah, M.L.; DeWitt, C.A. Cutaneous Findings in Hemophagocytic Lymphohistiocytosis. Dermatology 2015, 230, 234–243. [Google Scholar] [CrossRef]
- Fardet, L.; Galicier, L.; Vignon-Pennamen, M.D.; Regnier, S.; Noguera, M.E.; de Labarthe, A.; Raffoux, E.; Martinez, V.; Buyse, S.; Viguier, M.; et al. Frequency, clinical features and prognosis of cutaneous manifestations in adult patients with re-active haemophagocytic syndrome. Br. J. Dermatol. 2010, 162, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Morrell, D.S.; Pepping, M.A.; Scott, J.P.; Esterly, N.B.; Drolet, B.A. Cutaneous manifestations of hemophagocytic lymphohistio-cytosis. Arch. Dermatol. 2002, 138, 1208–1212. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Skin biopsy revealed perivascular and periadnexal infiltration comprising histocytes and lymphocytes in the dermis, with the obvious involvement of nerves.
Figure 1.
Skin biopsy revealed perivascular and periadnexal infiltration comprising histocytes and lymphocytes in the dermis, with the obvious involvement of nerves.

Figure 2.
Generalized pruritic annular to irregular erythema, accompanied by edema on the left side of the face.
Figure 2.
Generalized pruritic annular to irregular erythema, accompanied by edema on the left side of the face.

Figure 3.
A coherent timeline indicating the date of this case.

Figure 4.
PET/CT revealed widespread increased metabolic activity.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Laboratory tests on the second admission.
| Tests on Admission | Results | Normal Ranges | Tests on Admission | Results | Normal Ranges |
|---|---|---|---|---|---|
| Complete blood count | Hepatic and renal function | ||||
| White blood cell (109/L) | 2.09 | 3.5–9.5 | ALT (U/L) | 27.8 | 5–46 |
| Neutrophil count (109/L) | 1.50 | 1.8–6.3 | AST (U/L) | 66.7 | 8–40 |
| Lymphocyte count (109/L) | 0.43 | 1.1–3.2 | Lactate dehydrogenase (U/L) | 668 | 100–245 |
| Hemoglobin (g/L) | 147.0 | 130–175 | Serum creatinine (umol/L) | 69.3 | 35–115 |
| Platelet (109/L) | 111 | 125–350 | Blood urea nitrogen (mmol/L) | 4.97 | 2.9–8.2 |
| Coagulation | Fasting triglycerides (mg/dL) | 1.96 | 0.46–2.25 | ||
| APTT (s) | 34.00 | 25–37 | Ferritin (ng/mL) | 18,669.00 | 24.00–336.2 |
| PT (s) | 11.80 | 9–13.5 | Soluble IL-2 receptor (U/mL) | 103,915 | <6400 |
| Thrombin time (s) | 18.80 | 10.3–16.6 | NK cell (%) | 11.54 | ≥15.11 |
| Fibrinogen (g/L) | 1.83 | 2–4 | |||
| D-Dimer (mg/mL) | 322.00 | 0–550 |
Abnormal results are shown in BOLD. APTT: activated partial thromboplastin time; PT: prothrombin time.
Table 2.
Reported cases of HLH following COVID-19 vaccination.
| Case | Sex, Age | Symptoms Onset after Vaccination | Clinical Manifestations | Medical History | Other Cause of HLH | Gene Mutations | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| Our case | M, 38 y | 4 weeks | Annular erythema, fever, fatigue | Interstitial lung disease | None | UNC13D | Methylprednisolone, etoposide, doxorubicin, HSCT | Improved and under follow-up |
| Tang et al., J Hematol Oncol, 2021 [6] | M, 43 y | Shortly after vaccination | Fever, vomiting, malaise | None | EBV infection | Absent | Dexamethasone | Discharged |
| Hieber et al., Infection, 2022 [7] | F, 24 y | 10 days | Fatigue, fever, chills, nausea | None | None | Not tested | IVIG, dexamethasone, Anakinra | Discharged |
| Ai et al., J Med Virol, 2022 [8] | M, 68 y | 10 days | Fevers, rigors, lethargy, night sweats | Hypertension, gout, Bowen’s disease | None | Not tested | No therapy | Spontaneous improvement |
| Nasir et al., J Clin Transl Res, 2022 [9] | M, 46 y | 3 weeks | Fever, fatigue, disturbed sleep, reduced appetite, skin rashes, oral ulcers | None | None | Not tested | Dexamethasone | Improved |
| Caocci et al., Haematologica, 2021 [10] | M, 38 y | 21 days | Fever, chills, fatigue, erythematous papules | None | None | Not tested | Methylprednisolone | Fully recovered |
| Baek et al., Infect Dis (Lond), 2021 [11] | M, 20 y | 2 days | Fever, myalgia, nausea, skin rashes | None | Not provided | Not tested | Dexamethasone | Immediate improvement |
| F, 71 y | 7 days | Fever, neurologic symptoms | Hypertension | Not provided | Not tested | Dexamethasone, etoposide | Discharged | |
| Sassi et al., Br J Haematol, 2021 [12] | M, 85 y | Shortly after vaccination | Anorexia, asthenia, pruritus | None | Not provided | Not tested | Not provided | Not provided |
| Rocco et al., Clin Infect Dis, 2021 [13] | M, 52 y | 1 day | Fever, abdominal pain | A viral syndrome | T-cell lymphoma, EBV viremia | Not tested | Dexamethasone, etoposide | Death |
| M, 53 y | 4 days | Fever, worsening hypoxia | Interstitial lung disease | EBV viremia | Not tested | Dexamethasone, Anakinra, IVIG, rituximab | Discharged to rehab facility | |
| M, 57 y | 12 days | Malaise, nausea | Heart failure, HIV infection, Mycobacterium avium, KSHV viremia | Kaposi sarcoma herpesvirus viremia | Not tested | Methylprednisolone | Death | |
| F, 55 y | 3 days | Fever | Adult-onset Still’s disease, pulmonary aspergillosis, GATA2 deficiency | Not found | Not tested | Anakinra | Slowly recovered | |
| F, 48 y | 4 days | Fever, cough, pleuritic chest pain | HIV | Not found | Not tested | Prednisone, infliximab | Improvement within 72 h | |
| Attwell et al., J Clin Pathol, 2022 [14] | M, 65 y | 5 days | Breathlessness, fever, myalgia | Type 2 diabetes mellitus | Not found | Not tested | Methylprednisolone, IVIG, Anakinra | Deteriorated |
| F, 75 y | 7 days | Night sweats, breathlessness, myalgia, fever, cough | JAK2-mutation positive essential thrombocythaemia, breast cancer | Not found | Not tested | Methylprednisolone, IVIG, Anakinra | Death | |
| M, 35 y | 8 days | Fever, diarrhea, sore throat, pruritic rash, breathlessness | Ankylosing spondylitis | Not found | Not tested | Methylprednisolone | Responded well | |
| Wu et al., BMJ Case Rep,2022 [15] | M, 60 y | 6 days | Fevers, night sweats, loss of appetite, delirium, non-ambulatory | Barrett’s esophagus | Not found | Not tested | Dexamethasone, etoposide | Discharged, but relapsed and deteriorated |
| F, 32 y | 4 weeks | Fever | None | Not found | Not provided | Dexamethasone, etoposide, emapalumab-lzsg | Discharged, but deteriorated | |
| Lin et al., Vaccines, 2022 [16] | F, 14 y | 15 days | Fever, headache, nausea, tachypnea, drowsy consciousness, mottling skin, jaundice | None | EBV viremia | Not tested | Methylprednisolone, IVIG | Discharged |
| Cory et al., Clin Med (Lond), 2021 [17] | F, 36 y | 9 days | Fever, myalgia, sore throat, mild facial swelling | None | Not found | Not tested | Methylprednisolone, IVIG | Improvement |
M, male; F, female; y, years; IVIG, intravenous immunoglobulin; HSCT, hematopoietic stem cell transplantation.
Table 3.
Primary HLH with cutaneous manifestations.
| Case | Sex, Age | Gene Defects | HLH Type | Initial Symptoms | Cutaneous Manifestations | Skin Histologic Findings | Treatments | Outcome |
|---|---|---|---|---|---|---|---|---|
| Minocha et al., Intractable Rare Dis Res, 2017 [18] | M, 20 m | RAB27A | Griscelli syndrome type 2 | Fever, jaundice, pallor, weight loss | Icterus, silvery-gray hair, and hypopigmented skin | Not provided | Mycophenolate mofetil, HSCT | Improved and under follow-up |
| Mishra et al., Korean J Pediatr, 2014 [19] | M, 5 y | RAB27A | Griscelli syndrome type 2 | Fever, skin lesion | A generalized hypopigmented skin and multiple erythematous to hyperpigmented, nodular lesions, extending from midthighs to feet | Widening of septae in the subcutaneous tissue, infiltration of the periphery of the fat lobule by chronic inflammatory cells | Prednisolone, HSCT | Not provided |
| Tewari et al., Spec Care Dentist, 2018 [20] | M, 4 y | RAB27A | Griscelli syndrome type 2 | Pain in the oral cavity and tooth decay | Silvery white hair and white skin | Not provided | Not provided | Not provided |
| Panigrahi et al., Pediatr Neurol, 2015 [21] | F, 1 y | RAB27A | Griscelli syndrome type 2 | Fever | Silvery white hairs, silvery eyelashes | Not provided | Methylprednisolone | Died |
| Meschede et al., Braz J Med Biol Res, 2008 [22] | M, 3 y | RAB27A | Griscelli syndrome type 2 | Fever | Light silvery-gray colored scalp hair and eyebrows | Not provided | Corticoid, cyclosporine | Died |
| Gotesman et al., Pediatr Dermatol, 2020 [23] | F, 18 m | RAB27A | Griscelli syndrome type 2 | Skin lesion | Non-pruritic, erythematous-violaceous papules, and dry, coarse, silvery-gray hair | A granulomatous inflammatory process | HSCT | Improvement |
| Guo et al., Medicine, 2018 [24] | M, 13 m | XIAP | X-linked lymphoproliferative syndrome | Fever, skin lesion, recurrent ear discharge | Widespread hemorrhagic skin eruptions | Langerhans cell histiocytosis (LCH) | HLH-2004- directed chemotherapy | Died |
| Kaya et al., Pediatr Blood Cancer, 2011 [25] | F, 4 y | LYST | Chediak–Higashi syndrome | Fever, pallor, lethargy, poor appetite | Speckled hypopigmented areas | Not provided | HLH-2004 therapy | Complete remission |
| Nielsen et al., J Pediatr Hematol Oncol, 2015 [26] | F, 2 m | LYST | Chediak–Higashi syndrome | Coryza, coughing, skin eruption | A pustule skin eruption, fair hair, pale and wax-like skin | Numerous large inclusion bodies in mast cells, and an epidermis virtually absent of melanin in both melanocytes and keratinocytes | Etoposide, dexamethasone, cyclosporine, IVIG | Died |
| Wu et al., Braz J Med Biol Res, 2017 [27] | M, 9 m | LYST | Chediak–Higashi syndrome | Fever | Mild pallor, gray hair, patchy hypopigmentation of the skin, red rashes on the trunk | Not provided | Cyclosporine A, dexamethasone, etoposide; HSCT has been planned | Temporary remission |
| Morrone et al., Case Rep Med, 2010 [28] | F, 16 m | CHD1 | Chediak–Higashi syndrome | Fever, decreased activity, increased sleepiness, irritability | Silvery hair, pale skin, edematous eyelids | Not provided | Etoposide, dexamethasone, cyclosporine | Died |
| Sheng et al., BMC Med Genet, 2019 [29] | F, 30 y | STXBP2, LYST | Not provided | Fever, fatigue | Oedematose swelling of the face and coexistent skin lesions | Not provided | Etoposide, dexamethasone, currently waiting for HSCT | Well-controlled for a month |
| Larson et al., Pediatr Dermatol, 2017 [30] | M, 6 d | PRF1 | F-HLH type 2 | Skin lesion | Multiple blue–purple violaceous nodules | An intact epidermis and an underlying dermal infiltrate of mononuclear cells | Not provided | Not provided |
| Viñas et al., Front Immunol, 2021 [31] | M, 16 m | STXBP2 | F-HLH type 5 | Skin lesion, fever, vomit, diarrhea, edema | An exacerbation of cutaneous Langerhans cell histiocytosis, edema | Not provided | Not provided | Not provided |
| Tang et al., Medicine, 2019 [32] | F, 9 y | STXBP2 | F-HLH type 5 | Fever | Ecchymosis and edema of the lower extremities | Not provided | HLH-2004-directed chemotherapy, HSCT | Died |
| Pasqualin et al., Ital J Pediatr, 2014 [33] | M, 11 y | STX11 | F-HLH type 4 | Fever, dyspnea | A warm, painful, indurated plaque with a brownish, hyperpigmented over the right thigh | Mixed septal and lobular inflammatory infiltrate of benign-appearing histiocytes, plasma cells and lymphocytes, and diffuse fat necrosis | Methylprednisolone, cyclosporine | Remission was sustained at 6-month follow-up |
| Chen et al., J Clin Pathol, 2007 [34] | F, 11 y | PRF1 | F-HLH type 2 | Fever, skin lesion | Indurated skin nodules over the left thigh | Lobular panniculitis with lymphocytic infiltration with occasional benign histiocytes showing hemophagocytosis | 13-cis retinoic acid, prednisolone | Died |
| Akyol et al., J Pediatr Hematol Oncol, 2020 [35] | F, 21 m | UNC13D | F-HLH type 3 | Fever, skin lesion | Widespread maculopapular rash | Not provided | Not provided | Not provided |
| Zengin et al., Am J Dermatopathol, 2021 [36] | M, 4 y | UNC13D | F-HLH type 3 | Skin lesion | A widespread popular–pustular rash | A cup-shaped depression of the epidermis, which exhibited perforation with necrobiotic collagen. Necrobiosis with palisading histiocytes and lymphoplasmacytic inflammatory cell infiltration in the dermis | Dexamethasone, HSCT | Not provided |
| our case | M, 36 y | UNC13D | F-HLH type 3 | Skin lesion | Widespread annular erythema, facial edema | Lymphohistiocytic infiltration in the dermis, as well as reactive hyperplasias of lymphoid tissue dominated by cytotoxic T-cells | Methylprednisolone, etoposide, doxorubicin, HSCT | Improved and under follow-up |
y, years; m, months; d, days; HSCT, hematopoietic stem cell transplantation; IVIG, intravenous immunoglobulin.
Table 4.
Genetic defects associated with primary HLH.
| Type of HLH | Defective Gene | |
|---|---|---|
| Familial HLH (F-HLH) | F-HLH type 2 | PRF1 |
| F-HLH type 3 | UNC13D | |
| F-HLH type 4 | STX11 | |
| F-HLH type 5 | STXBP2 | |
| Immuno-deficiency syndromes | Griscelli syndrome type 2 | RAB27A |
| Chediak–Higashi syndrome | LYST | |
| Hermansky–Pudlak syndrome type 2 | AP3B1 | |
| EBV-driven | X-linked lymphoproliferative disorder type 1 (XLP-1) | SH2D1A |
| X-linked lymphoproliferative disorder type 2 (XLP-2) | BIRC4 | |
| IL2-inducible T-cell kinase deficiency | ITK | |
| CD27 deficiency | CD27 | |
| X-linked immunodeficiency with magnesium defect (XMEN) | MAGT1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
He, Y.; Hui, Y.; Liu, H.; Wu, Y.; Sang, H.; Liu, F. Adult-Onset Familial Hemophagocytic Lymphohistiocytosis Presenting with Annular Erythema following COVID-19 Vaccination. Vaccines 2022, 10, 1436. https://doi.org/10.3390/vaccines10091436
AMA Style
He Y, Hui Y, Liu H, Wu Y, Sang H, Liu F. Adult-Onset Familial Hemophagocytic Lymphohistiocytosis Presenting with Annular Erythema following COVID-19 Vaccination. Vaccines. 2022; 10(9):1436. https://doi.org/10.3390/vaccines10091436
Chicago/Turabian StyleHe, Yifan, Yun Hui, Haibo Liu, Yifan Wu, Hong Sang, and Fang Liu. 2022. "Adult-Onset Familial Hemophagocytic Lymphohistiocytosis Presenting with Annular Erythema following COVID-19 Vaccination" Vaccines 10, no. 9: 1436. https://doi.org/10.3390/vaccines10091436
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.