
Dynamic Changes in Hepatitis A Immunity in Regions with Different Vaccination Strategies and Different Vaccination Coverage
 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
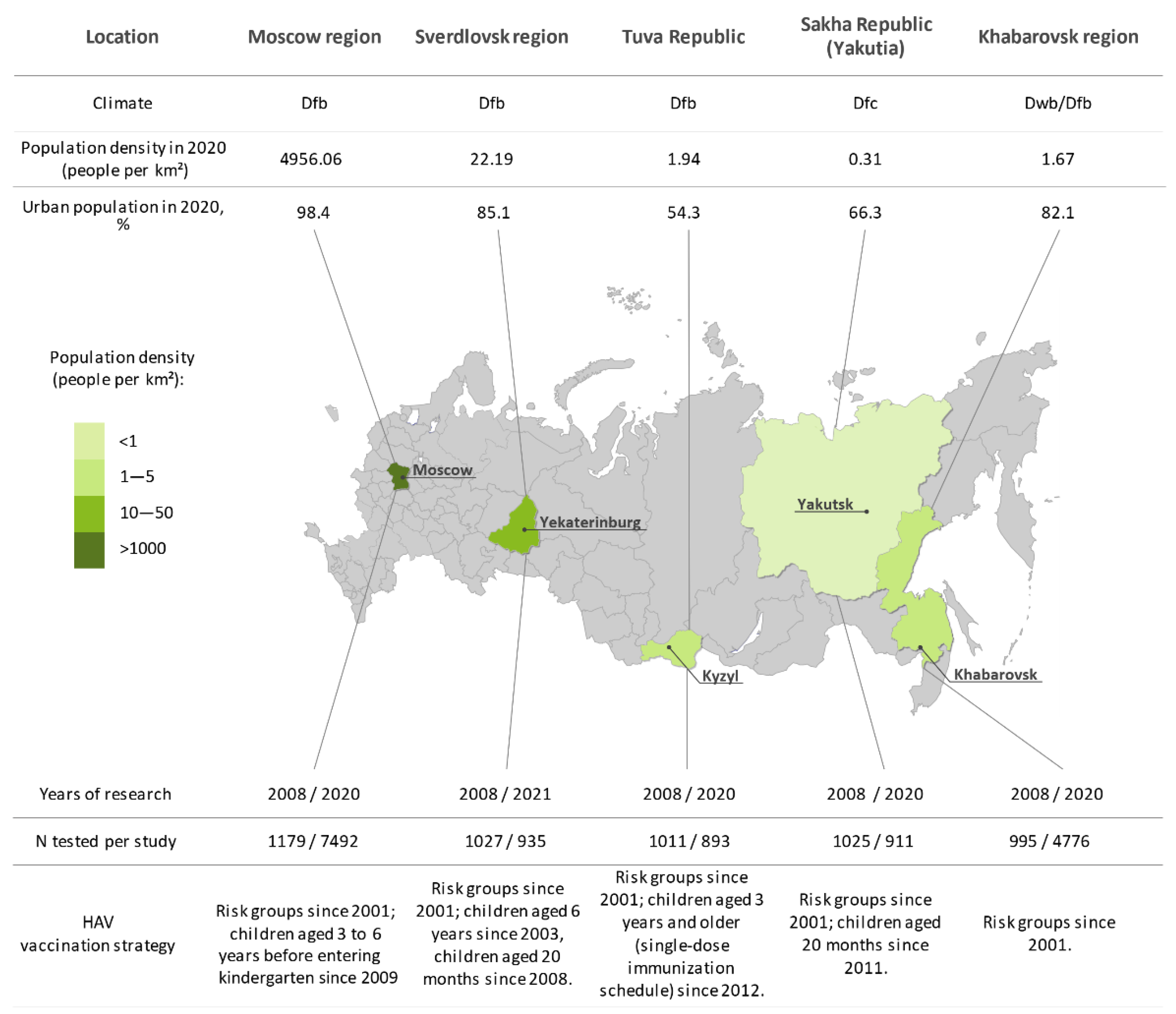
2.1. Study Cohorts
2.2. Anti-HAV Antibody Testing
2.3. Incidence and Vaccination Coverage Analysis
2.4. Statistical Analysis
3. Results
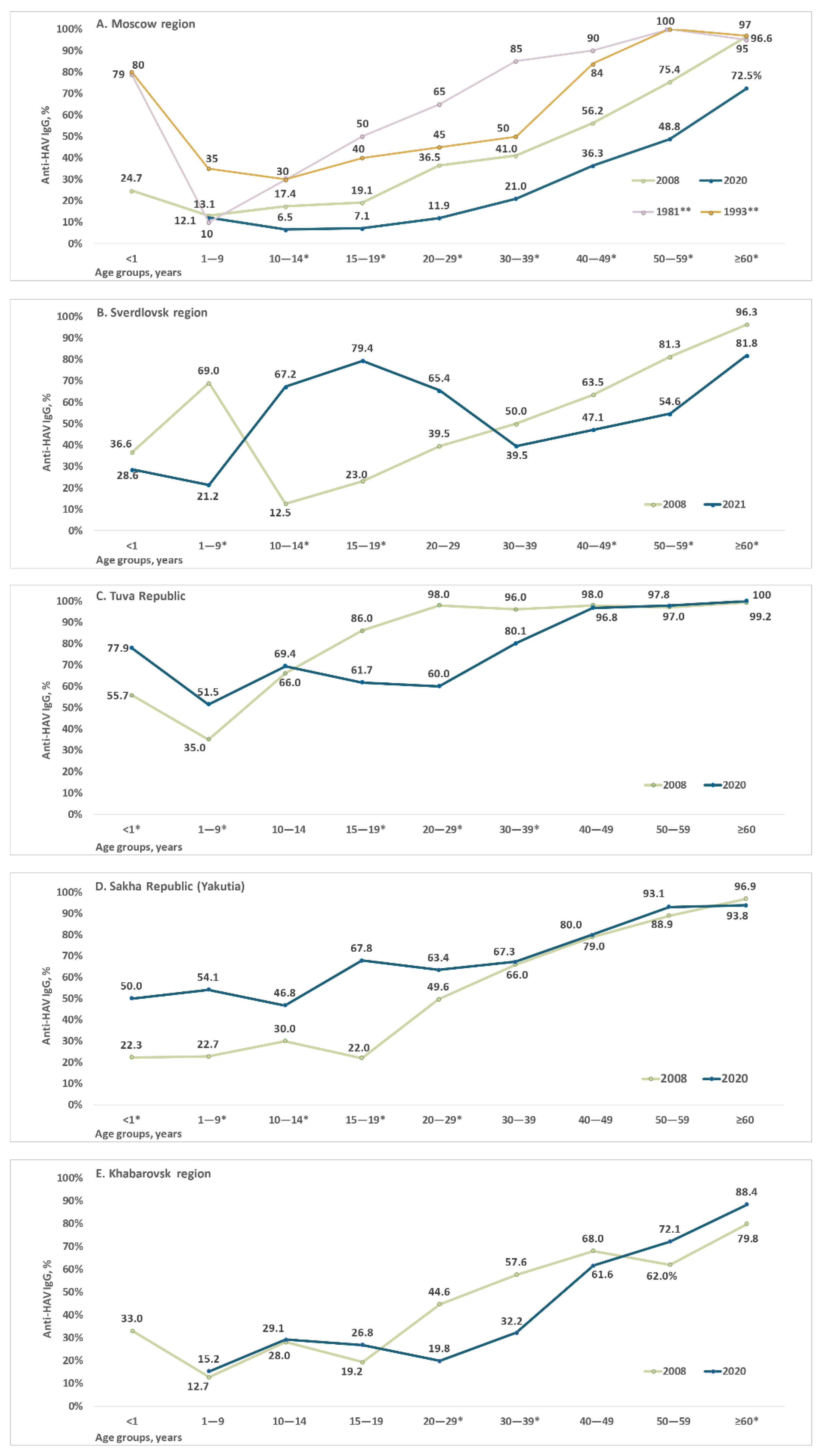
3.1. Hepatitis A Seroprevalence
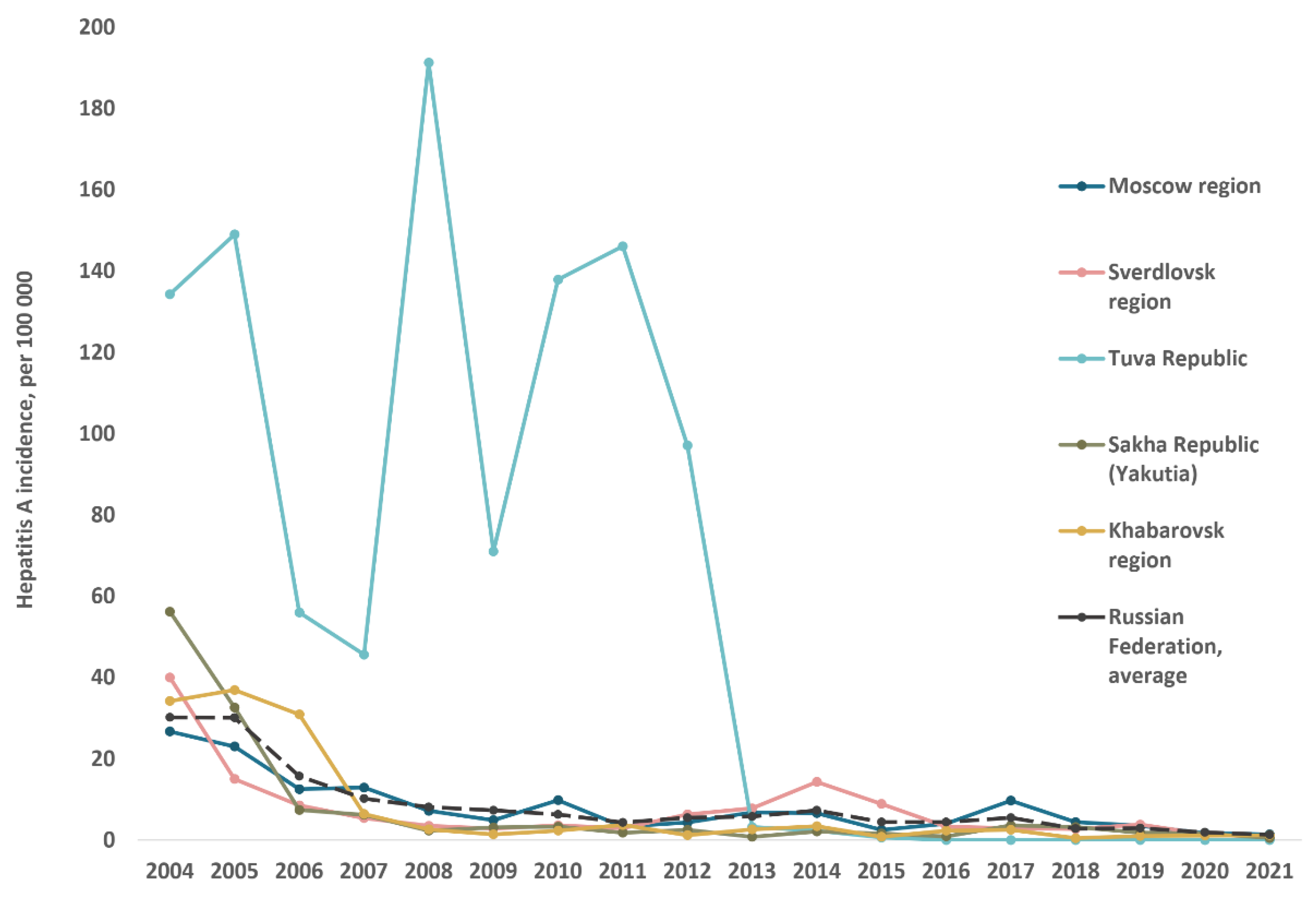
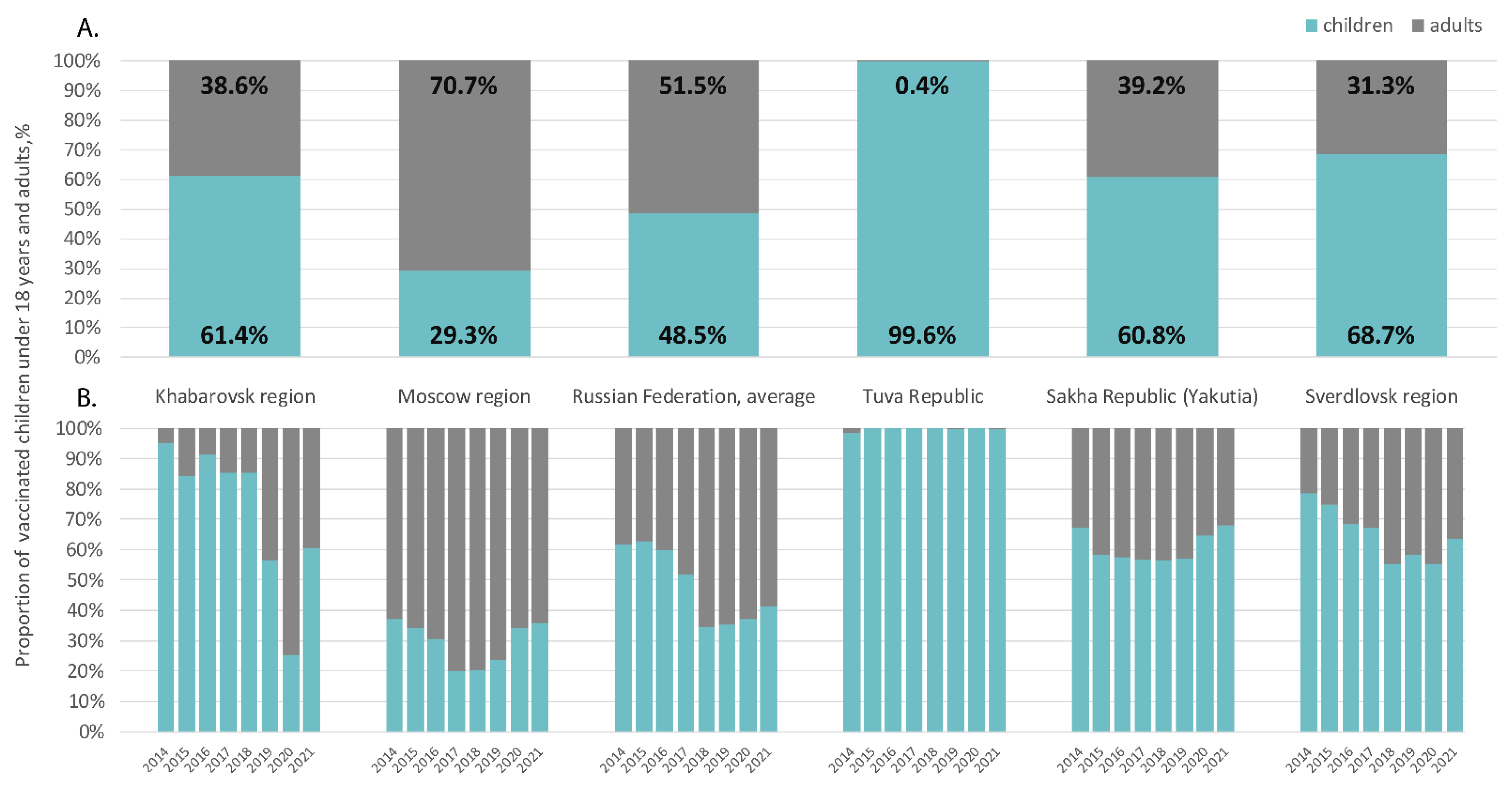
3.2. Hepatitis A Incidence and Vaccination Coverage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Migueres, M.; Lhomme, S.; Izopet, J. Hepatitis A: Epidemiology, High-Risk Groups, Prevention and Research on Antiviral Treatment. Viruses 2021, 13, 1900. [Google Scholar] [CrossRef] [PubMed]
- WHO Position Paper on Hepatitis A Vaccines. 2012. Available online: https://www.who.int/publications/i/item/who-wer8728-29-261-276 (accessed on 29 July 2022).
- Herzog, C.; Van Herck, K.; Van Damme, P. Hepatitis A Vaccination and Its Immunological and Epidemiological Long-Term Effects—A Review of the Evidence. Hum. Vaccines Immunother. 2021, 17, 1496–1519. [Google Scholar] [CrossRef] [PubMed]
- Shliakhtenko, L.; Plotnikova, V.; Levakova, I.; Rubis, L.; Solovieva, E.; Mukomolov, S. Modern Epidemiology of Hepatitis A in the North-Western Region of the Russian Federation. J. Viral Hepat. 2008, 15 (Suppl. 2), 38–42. [Google Scholar] [CrossRef] [PubMed]
- Federal Center of Hygiene and Epidemiology. Infectious and Parasitic Diseases Morbidity in Russian Federation. In Federal Statistical Form 1; Federal Center of Hygiene and Epidemiology: Moscow, Russia, 2019. (In Russian) [Google Scholar]
- Michaylov, M.; Kyuregyan, K. Contemporary Strategy to Control Viral Hepatitis A in the Russian Federation. Zhurnal. Mikrobiol. Epidemiol. Immunobiol. 2021, 98, 190–197. [Google Scholar] [CrossRef]
- Mikhailov, M.I.; Shakhgildyan, I.V. Enteral. Viral Hepatitis; VUNMC Rozdrav Press: Moscow, Russia, 2007. (In Russian) [Google Scholar]
- Romanenko, V.V.; Ankudinova, A.V.; Yurovskikh, A.I.; Osipova, S.N. Strategies and tactics of immunization against hepatitis A in the Sverdlovsk region. Bull. Ural State Med. Acad. 2012, 24, 133–134. (In Russian) [Google Scholar]
- Briko, N.I.; Mindlina, A.Y.; Polibin, R.V. Peculiarities of epidemic process manifestations and implementation of the program of hepatitis a prevention in the framework of the Moscow regional vaccination schedule. Epidemiol. Vaccine 2012, 7, 23–27. (In Russian) [Google Scholar]
- Semenova, V.K.; Ivanova, V.V. Epidemiological situation on hepatitis A and its specific prevention in the Republic of Saha (Yakutia). Bull. North-East. Fed. Univ. M.K. Ammosov. Ser. Med. Sci. 2018, 2, 55–59. (In Russian) [Google Scholar]
- Mikhailov, M.I.; Lopatukhina, M.A.; Asadi Mobarhan, F.A.; Ilchenko, L.Y.; Kozhanova, T.V.; Isaeva, O.V.; Karlsen, A.A.; Potemkin, I.A.; Kichatova, V.S.; Saryglar, A.A.; et al. Universal Single-Dose Vaccination against Hepatitis A in Children in a Region of High Endemicity. Vaccines 2020, 8, 780. [Google Scholar] [CrossRef]
- Van Herck, K.; Van Damme, P. Prevention of Hepatitis A by Havrix: A Review. Expert. Rev. Vaccines 2005, 4, 459–471. [Google Scholar] [CrossRef]
- World Health Organization. Hepatitis A. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-a (accessed on 29 July 2022).
- Lemon, S.M.; Ott, J.J.; Van Damme, P.; Shouval, D. Type A Viral Hepatitis: A Summary and Update on the Molecular Virology, Epidemiology, Pathogenesis and Prevention. J. Hepatol. 2017, 68, 167–184. [Google Scholar] [CrossRef]
- Theeten, H.; Van Herck, K.; Van Der Meeren, O.; Crasta, P.; Van Damme, P.; Hens, N. Long-Term Antibody Persistence after Vaccination with a 2-Dose Havrix (Inactivated Hepatitis A Vaccine): 20 Years of Observed Data, and Long-Term Model-Based Predictions. Vaccine 2015, 33, 5723–5727. [Google Scholar] [CrossRef]
- Federal State Statistics Service. Russia Demography Report. Available online: https://rosstat.gov.ru/folder/12781 (accessed on 29 July 2022). (In Russian)
- Hajian-Tilaki, K. Sample Size Estimation in Epidemiologic Studies. Caspian. J. Intern. Med. 2011, 2, 289–298. [Google Scholar]
- Jacobsen, K.H.; Wiersma, S.T. Hepatitis A Virus Seroprevalence by Age and World Region, 1990 and 2005. Vaccine 2010, 28, 6653–6657. [Google Scholar] [CrossRef]
- Gripenberg, M.; Aloysia D’Cor, N.; L’Azou, M.; Marsh, G.; Druelles, S.; Nealon, J. Changing Sero-Epidemiology of Hepatitis A in Asia Pacific Countries: A Systematic Review. Int. J. Infect. Dis. 2018, 68, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Carrillo-Santisteve, P.; Tavoschi, L.; Severi, E.; Bonfigli, S.; Edelstein, M.; Byström, E.; Lopalco, P. ECDC HAV Expert Panel Seroprevalence and Susceptibility to Hepatitis A in the European Union and European Economic Area: A Systematic Review. Lancet Infect. Dis. 2017, 17, e306–e319. [Google Scholar] [CrossRef]
- World Health Organization. WHO Immunological Basis for Immunization Series: Module 18: Hepatitis A; World Health Organization: Geneva, Switzerland, 2019; ISBN 978-92-4-151632-7. [Google Scholar]
- David, A.M.; Steering Committee for Prevention and Control of Infectious Diseases. Hepatitis A Outbreaks—Methods of Intervention in South-East Asian Countries. Int. J. Infect. Dis. 2004, 8, 201–209. [Google Scholar] [CrossRef]
- Wooten, D.A. Forgotten but Not Gone: Learning from the Hepatitis A Outbreak and Public Health Response in San Diego. Top. Antivir. Med. 2019, 26, 117–121. [Google Scholar]
- Domínguez, A.; Varela, C.; Soldevila, N.; Izquierdo, C.; Guerrero, M.; Peñuelas, M.; Martínez, A.; Godoy, P.; Borràs, E.; Rius, C.; et al. Hepatitis A Outbreak Characteristics: A Comparison of Regions with Different Vaccination Strategies, Spain 2010–2018. Vaccines 2021, 9, 1214. [Google Scholar] [CrossRef]
- Resolution No. 9 dated 03.11.2013 of the Chief Sanitary Doctor of the Russian Federation. Available online: https://www.rospotrebnadzor.ru/documents/details.php?ELEMENT_ID=227 (accessed on 29 July 2022). (In Russian).
- Estripeaut, D.; Contreras, R.; Tinajeros, O.; Castrejón, M.M.; Shafi, F.; Ortega-Barria, E.; DeAntonio, R. Impact of Hepatitis A Vaccination with a Two-Dose Schedule in Panama: Results of Epidemiological Surveillance and Time Trend Analysis. Vaccine 2015, 33, 3200–3207. [Google Scholar] [CrossRef]
- Guturu, P.; Cicalese, L.; Duchini, A. Hepatitis A Vaccination in Healthcare Personnel. Ann. Hepatol. 2012, 11, 326–329. [Google Scholar] [CrossRef]
- Shet, A.; Carr, K.; Danovaro-Holliday, M.C.; Sodha, S.V.; Prosperi, C.; Wunderlich, J.; Wonodi, C.; Reynolds, H.W.; Mirza, I.; Gacic-Dobo, M.; et al. Impact of the SARS-CoV-2 pandemic on routine immunisation services: Evidence of disruption and recovery from 170 countries and territories. Lancet Glob. Health 2022, 10, e186–e194. [Google Scholar] [CrossRef]
- Dankwa, E.A.; Donnelly, C.A.; Brouwer, A.F.; Zhao, R.; Montgomery, M.P.; Weng, M.K.; Martin, N.K. Estimating Vaccination Threshold and Impact in the 2017–2019 Hepatitis A Virus Outbreak among Persons Experiencing Homelessness or Who Use Drugs in Louisville, Kentucky, United States. Vaccine 2021, 39, 7182–7190. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-S.; Charlett, A. Bayesian Modelling of a Hepatitis A Outbreak in Men Who Have Sex with Men in Sydney, Australia, 1991/1992. Epidemiol. Infect. 2019, 147, e226. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Region | Year of Study | Average Number of Samples per Age Group (Min.–Max.) | Male/Female Ratio | Urban/Rural Population Ratio |
|---|---|---|---|---|
| Moscow region | 2008 | 131 (97–237) | 1:1.1 | 1:0.09 |
| 2020 | 936 (184–2751) | 1:2.1 | 1:0.03 | |
| Sverdlovsk region | 2008 | 114 (81–200) | 1:2.4 | 1:0.02 |
| 2021 | 103 (35–204) | 1:1.6 | 1:0.01 | |
| Tuva Republic | 2008 | 112 (88–200) | 1:1.8 | 1:1.66 |
| 2020 | 99 (64–169) | 1:0.9 | 1:0.17 | |
| Sakha Republic (Yakutia) | 2008 | 114 (97–203) | 1:1.4 | 1:0.28 |
| 2020 | 101 (58–185) | 1:1.4 | 1:0.34 | |
| Khabarovsk region | 2008 | 110 (99–197) | 1:1.1 | 1:0.14 |
| 2020 | 596 (294–1255) | 1:0.9 | 1:0.05 |
| Study Region | Year of Study | Anti-HAV IgG Antibody Prevalence | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Average, % [95% CI] | p * | Men, % [95% CI] | Women, % [95% CI] | p * | Urban Population, % [95% CI] | Rural Population, % [95% CI] | p * | ||
| Moscow region | 2008 | 40.1 [37.4–42.9] | >0.0001 | 38.1 [34.1–42.2] | 41.9 [38.1–45.8] | 0.1905 | 39.4 [36.5 –42. 5] | 48.0 [38.3–57.8] | 0.1068 |
| 2020 | 23.0 [22.0–24.0] | 22.0 [20.4–23.7] | 23.5 [22.3–24.6] | 0.1679 | 22.6 [21.6–23.6] | 35.6 [21.6–23.6] | >0.0001 | ||
| Sverdlovsk region | 2008 | 54.0 [51.0–57.1] | 0.856 | 43.6 [38.1–49.2] | 58.4 [54.8–62.0] | >0.0001 | 54.0 [50.9–57.0] | 66.7 [20.2–94.4] | 1 |
| 2021 | 54.6 [51.3–57.7] | 53.3 [60.9–45.8] | 54.8 [60.9–48.7] | 0.6854 | 54.4 [51.2–57.6] | 63.6 [35.2–85.0] | 0.7625 | ||
| Tuva Republic | 2008 | 77.4 [74.7–79.8] | 0.4162 | 70.1 [65.2–74.5] | 81.5 [78.3–84.3] | >0.0001 | 70.3 [65.5–74.6] | 81.6 [78.4–84.5] | >0.0001 |
| 2020 | 75.7 [72.8–78.4] | 67.4 [63.0–71.5] | 85.0 [81.3–88.1] | >0.0001 | 76.9 [73.8–79.8] | 68.7 [60.3–76.0] | 0.0474 | ||
| Sakha Republic (Yakutia) | 2008 | 49.7 [46.6–52.7] | >0.0001 | 38.4 [33.9–43.1] | 57.6 [53.6–61.4] | >0.0001 | 52.6 [49.1–56.0] | 39.3 [33.1–45.8] | 0.0005 |
| 2020 | 67.1 [64.0–70.0] | 71.2 [66.6–75.4] | 63.8 [59.5–67.8] | 0.0193 | 67.2 [63.5–70.6] | 66.8 [60.5–72.6] | 0.9356 | ||
| Khabarovsk region | 2008 | 41.8 [38.8–44.9] | 0.0002 | 37.0 [32.7–41.4] | 46.1 [41.9–50.4] | 0.0038 | 43.1 [39.8–46.4] | 32.5 [24.8–41.3] | 0.0299 |
| 2020 | 35.5 [34.1–36.9] | 35.6 [33.7–37.4] | 35.4 [33.4–37.4] | 0.9275 | 38.1 [36.5–39.6] | 39.3 [31.8–46.8] | 0.8048 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyuregyan, K.K.; Lopatukhina, M.A.; Asadi Mobarkhan, F.A.; Kichatova, V.S.; Potemkin, I.A.; Isaeva, O.V.; Karlsen, A.A.; Malinnikova, E.Y.; Kaira, A.N.; Kozhanova, T.V.; et al. Dynamic Changes in Hepatitis A Immunity in Regions with Different Vaccination Strategies and Different Vaccination Coverage. Vaccines 2022, 10, 1423. https://doi.org/10.3390/vaccines10091423
Kyuregyan KK, Lopatukhina MA, Asadi Mobarkhan FA, Kichatova VS, Potemkin IA, Isaeva OV, Karlsen AA, Malinnikova EY, Kaira AN, Kozhanova TV, et al. Dynamic Changes in Hepatitis A Immunity in Regions with Different Vaccination Strategies and Different Vaccination Coverage. Vaccines. 2022; 10(9):1423. https://doi.org/10.3390/vaccines10091423
Chicago/Turabian StyleKyuregyan, Karen K., Maria A. Lopatukhina, Fedor A. Asadi Mobarkhan, Vera S. Kichatova, Ilya A. Potemkin, Olga V. Isaeva, Anastasia A. Karlsen, Elena Yu. Malinnikova, Alla N. Kaira, Tatyana V. Kozhanova, and et al. 2022. "Dynamic Changes in Hepatitis A Immunity in Regions with Different Vaccination Strategies and Different Vaccination Coverage" Vaccines 10, no. 9: 1423. https://doi.org/10.3390/vaccines10091423