
Improved SARS-CoV-2 Neutralization of Delta and Omicron BA.1 Variants of Concern after Fourth Vaccination in Hemodialysis Patients

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Hepatitis B Vaccination
2.4. SARS-CoV-2 Infection
2.5. Sample Collection
2.6. SARS-CoV-2 IgG Assay
2.7. SARS-CoV-2 Infection-Neutralization Assay
2.8. Statistical Analysis
3. Results
3.1. COVID-19 and Vaccinations
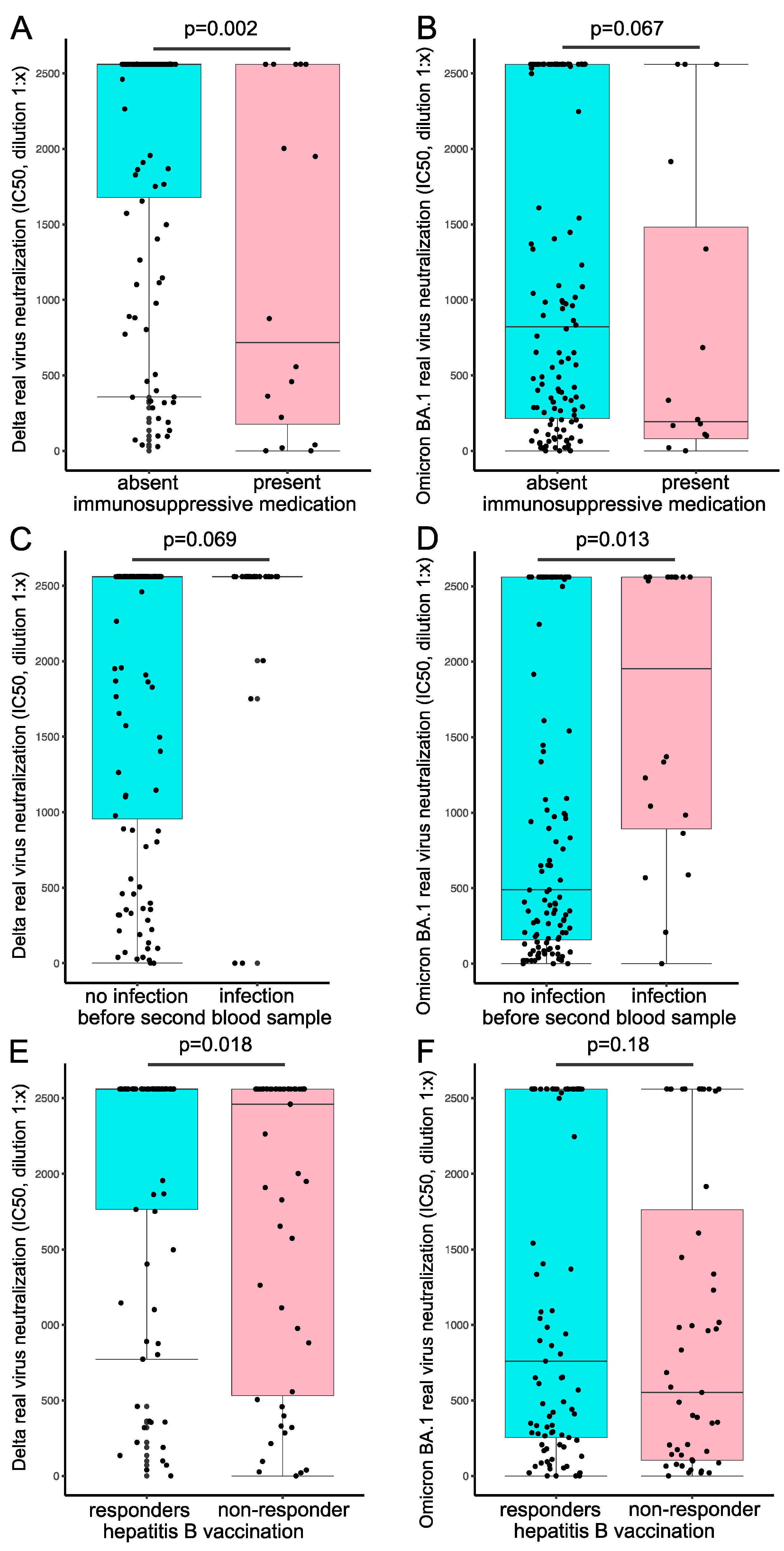
3.2. Immunosuppression
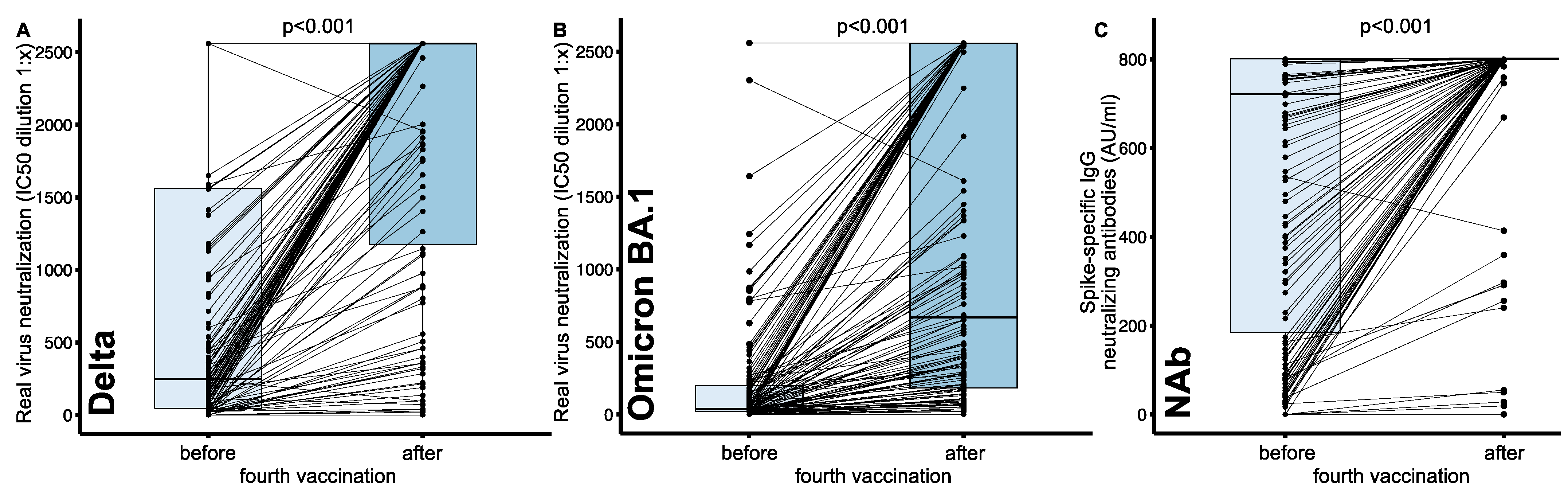
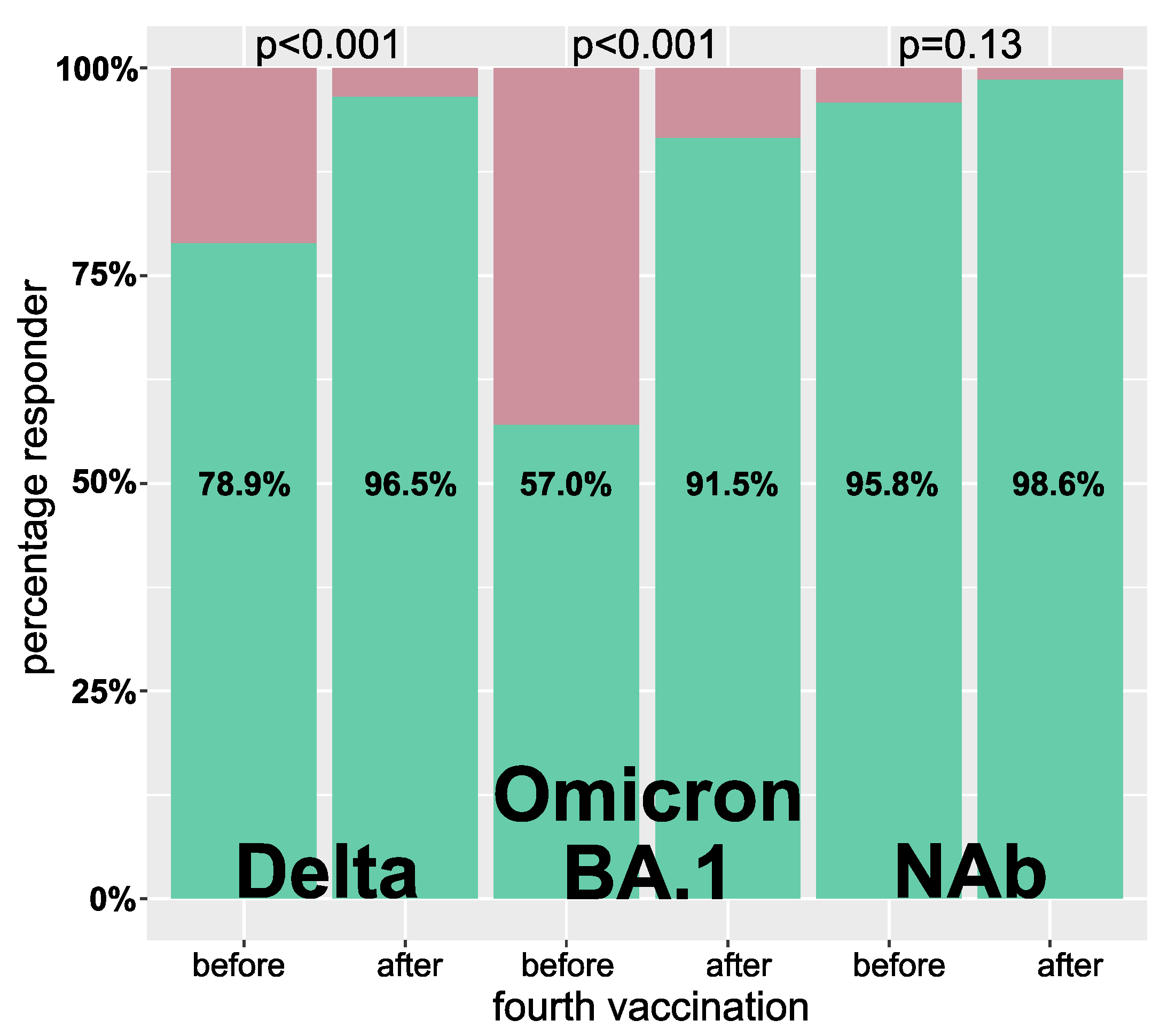
3.3. Impact of Four Vaccinations on Neutralization Capacity and NAbs
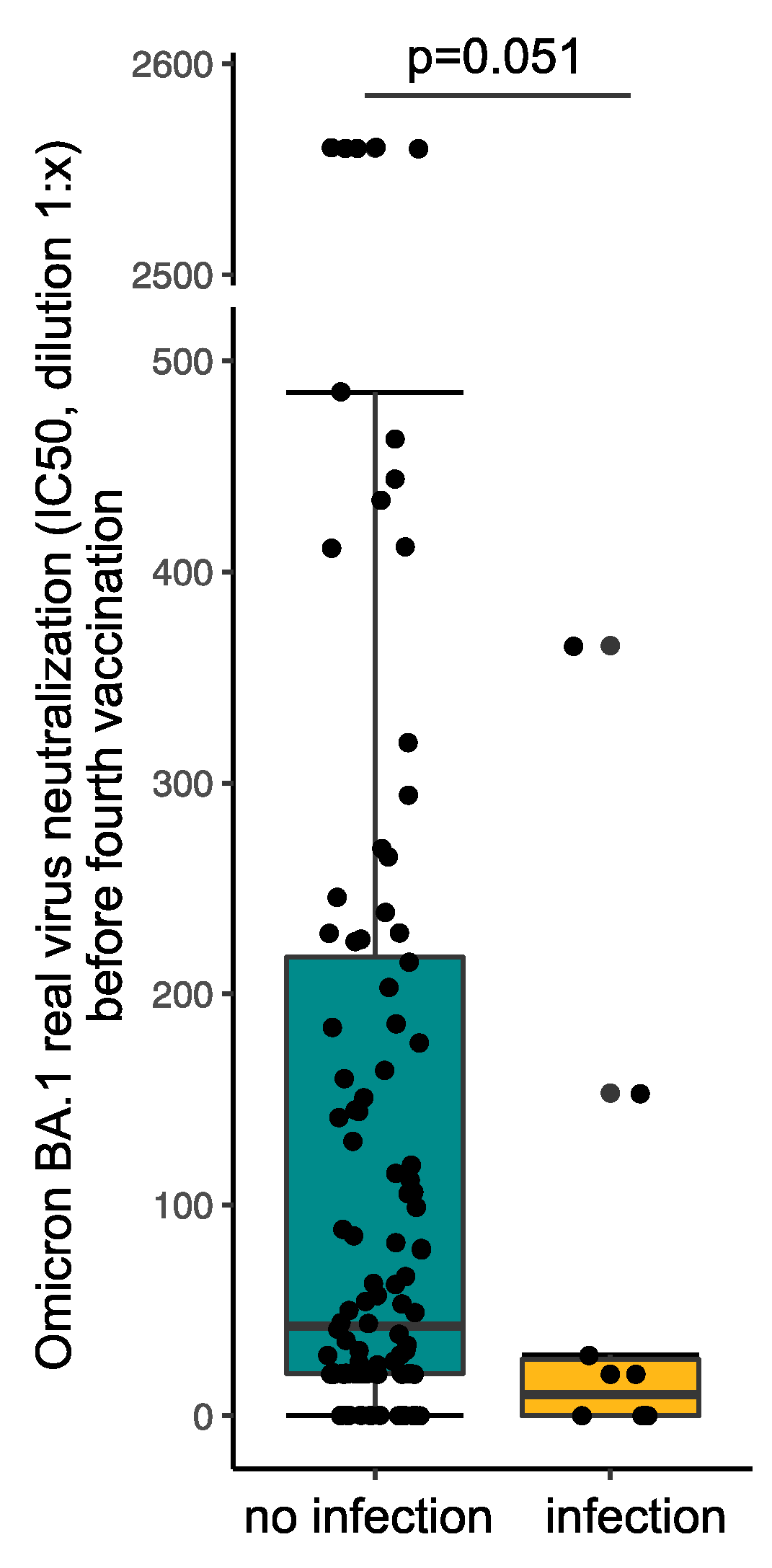
3.4. Impact of NAb and Infection Neutralization Capacity on Breakthrough Infections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- El Karoui, K.; Hourmant, M.; Ayav, C.; Glowacki, F.; Couchoud, C.; Lapidus, N. Vaccination and COVID-19 Dynamics in Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2022, 17, 395–402. [Google Scholar] [CrossRef]
- Ahmed, N.; Khderat, A.H.; Sarsour, A.; Taher, A.; Hammoudi, A.; Hamdan, Z.; Nazzal, Z. The vulnerability of maintenance dialysis patients with COVID-19: Mortality and risk factors from a developing country. Ann. Med. 2022, 54, 1511–1519. [Google Scholar] [CrossRef]
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M.; Noordzij, M.; Pena, M.J.; Vries, H.; et al. COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Nephrol. Dial. Transplant. 2020, 35, 1973–1983. [Google Scholar] [CrossRef] [PubMed]
- Erber, J.; Kappler, V.; Haller, B.; Mijočević, H.; Galhoz, A.; Prazeres da Costa, C.; Gebhardt, F.; Graf, N.; Hoffmann, D.; Thaler, M.; et al. Infection Control Measures and Prevalence of SARS-CoV-2 IgG among 4,554 University Hospital Employees, Munich, Germany. Emerg. Infect. Dis. 2022, 28, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Espi, M.; Charmetant, X.; Barba, T.; Mathieu, C.; Pelletier, C.; Koppe, L.; Chalencon, E.; Kalbacher, E.; Mathias, V.; Ovize, A.; et al. A prospective observational study for justification, safety, and efficacy of a third dose of mRNA vaccine in patients receiving maintenance hemodialysis. Kidney Int. 2022, 101, 390–402. [Google Scholar] [CrossRef] [PubMed]
- Wand, O.; Nacasch, N.; Fadeela, A.; Shashar, M.; Grupper, A.; Benchetrit, S.; Erez, D.; Shitrit, P.; Cohen-Hagai, K. Humoral response and breakthrough infections with SARS-CoV-2 B.1.617.2 variant in vaccinated maintenance hemodialysis patients. J. Nephrol. 2022, 35, 1479–1487. [Google Scholar] [CrossRef]
- Garcia-Beltran, W.F.; St Denis, K.J.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Hauser, B.M.; et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 2022, 185, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Wratil, P.R.; Stern, M.; Priller, A.; Willmann, A.; Almanzar, G.; Vogel, E.; Feuerherd, M.; Cheng, C.C.; Yazici, S.; Christa, C.; et al. Three exposures to the spike protein of SARS-CoV-2 by either infection or vaccination elicit superior neutralizing immunity to all variants of concern. Nat. Med. 2022, 28, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Verdier, J.F.; Boyer, S.; Chalmin, F.; Jeribi, A.; Egasse, C.; Maggi, M.F.; Auvray, P.; Yalaoui, T. Response to three doses of the Pfizer/BioNTech BNT162b2 COVID-19 vaccine: A retrospective study of a cohort of haemodialysis patients in France. BMC Nephrol. 2022, 23, 189. [Google Scholar] [CrossRef] [PubMed]
- Robert-Koch-Institute. Wöchentlicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19), Kalenderwoche 11, 24 March 2022. 2022. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Gesamt.html (accessed on 12 August 2022).
- Koerber, N.; Priller, A.; Yazici, S.; Bauer, T.; Cheng, C.C.; Mijočević, H.; Wintersteller, H.; Jeske, S.; Vogel, E.; Feuerherd, M.; et al. Dynamics of spike-and nucleocapsid specific immunity during long-term follow-up and vaccination of SARS-CoV-2 convalescents. Nat. Commun. 2022, 13, 153. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.H.; Leung, K.Y.; Zhang, R.R.; Liu, D.; Fan, Y.; Chen, H.; Yuen, K.Y.; Hung, I.F. Performance of a Surrogate SARS-CoV-2-Neutralizing Antibody Assay in Natural Infection and Vaccination Samples. Diagnostics 2021, 11, 1757. [Google Scholar] [CrossRef] [PubMed]
- Espi, M.; Koppe, L.; Fouque, D.; Thaunat, O. Chronic Kidney Disease-Associated Immune Dysfunctions: Impact of Protein-Bound Uremic Retention Solutes on Immune Cells. Toxins 2020, 12, 300. [Google Scholar] [CrossRef] [PubMed]
- Housset, P.; Kubab, S.; Hanafi, L.; Pardon, A.; Vittoz, N.; Bozman, D.F.; Caudwell, V.; Faucon, A.L. Humoral response after a fourth “booster” dose of a coronavirus disease 2019 vaccine following a 3-dose regimen of mRNA-based vaccination in dialysis patients. Kidney Int. 2022. [Google Scholar] [CrossRef] [PubMed]
- Cinkilic, O.; Anft, M.; Blazquez-Navarro, A.; Meister, T.L.; Roch, T.; Stervbo, U.; Pfaender, S.; Westhoff, T.H.; Babel, N. Inferior humoral and sustained cellular immunity against wild-type and omicron variant of concern in hemodialysis patients immunized with 3 SARS-CoV-2 vaccine doses compared with 4 doses. Kidney Int. 2022, 101, 1287–1289. [Google Scholar] [CrossRef] [PubMed]
- Anft, M.; Blazquez-Navarro, A.; Frahnert, M.; Fricke, L.; Meister, T.L.; Roch, T.; Stervbo, U.; Pfaender, S.; Westhoff, T.H.; Babel, N. Inferior cellular and humoral immunity against Omicron and Delta variants of concern compared with SARS-CoV-2 wild type in hemodialysis patients immunized with 4 SARS-CoV-2 vaccine doses. Kidney Int. 2022. [Google Scholar] [CrossRef] [PubMed]
- Carr, E.J.; Wu, M.; Harvey, R.; Billany, R.E.; Wall, E.C.; Kelly, G.; Howell, M.; Kassiotis, G.; Swanton, C.; Gandhi, S.; et al. Omicron neutralising antibodies after COVID-19 vaccination in haemodialysis patients. Lancet 2022, 399, 800–802. [Google Scholar] [CrossRef]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Orero, E.; Tejedor, S.; Mantecon, C.J.J.; Gomez Perez, V.O.; Marin Franco, A.J.; Alfaro Sanchez, C.; Puerta Carretero, M.; et al. Humoral Response to Third Dose of SARS-CoV-2 Vaccines in the CKD Spectrum. Clin. J. Am. Soc. Nephrol. 2022, 17, 872–876. [Google Scholar] [CrossRef] [PubMed]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Vaquera, S.M.; Mantecón, C.J.J.; Useche, G.; Márquez, M.G.S.; Carnerero, M.; Rodríguez, M.T.J.; Ramos, P.M.; et al. Safety and immediate humoral response of COVID-19 vaccines in chronic kidney disease patients: The SENCOVAC study. Nephrol. Dial. Transplant. 2021, gfab313. [Google Scholar] [CrossRef] [PubMed]
- Wieske, L.; van Dam, K.P.J.; Steenhuis, M.; Stalman, E.W.; Kummer, L.Y.L.; van Kempen, Z.L.E.; Killestein, J.; Volkers, A.G.; Tas, S.W.; Boekel, L.; et al. Humoral responses after second and third SARS-CoV-2 vaccination in patients with immune-mediated inflammatory disorders on immunosuppressants: A cohort study. Lancet Rheumatol. 2022, 4, e338–e350. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Omicron BA.1 Neutralization after Fourth Vaccination | ||||
|---|---|---|---|---|
| Total n = 142 | Low/Non-Responder n = 12 | Responder n = 130 | p | |
| Age (years) | 72.6 (61.5–80.6) | 77.1 (67.0–79.7) | 72.2 (60.5–80.6) | 0.47 |
| Female | 48 (33.8%) | 7 (58.3%) | 41 (31.5%) | 0.11 |
| Dialysis vintage (months) | 48.9 (21.3–83.7) | 38.7 (13.4–63.6) | 49.3 (21.9–84.0) | 0.34 |
| Vaccines | 1.0 | |||
| mRNA and vector | 8 (5.6%) | 0 (0.0%) | 8 (6.2%) | |
| only mRNA | 134 (94.4%) | 12 (100.0%) | 122 (93.8%) | |
| COVID-19 infection before second blood examination | 22 (15.5%) | 2 (16.7%) | 20 (15.4%) | 1.0 |
| Time lap between infection and second blood examination (days) | 215.7 ± 223.3 | 157.5 ± 222.7 | 224.6 ± 231.1 | 0.71 |
| Charlson Comorbidity Index | 5.0 (4.0–7.0) | 5.5 (4.0–6.2) | 5.0 (4.0–7.0) | 0.95 |
| History of kidney transplantation | 16 (11.3%) | 1 (8.1%) | 15 (11.5%) | 1.00 |
| Immunosuppressive medication | 16 (11.3%) | 4 (33.3%) | 12 (9.2%) | 0.031 |
| Hepatitis B vaccination non-response | 51 (36.4%) | 5 (41.7%) | 46 (35.4%) | 0.94 |
| Renal diagnosis | ||||
| Glomerulopathy | 22 (16.1%) | |||
| Diabetic nephropathy | 24 (17.5%) | |||
| Hypertensive nephropathy | 17 (12.4%) | |||
| Congenital or cystic renal disease | 13 (9.5%) | |||
| Tubulointerstitial disease | 2 (1.5%) | |||
| Reflux nephropathy | 3 (2.2%) | |||
| Other | 18 (13.1%) | |||
| Nephropathy of unknown origin | 43 (30.3%) | |||
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Predictor | b (95% CI) | p | b (95% CI) | p |
| ||||
| (Intercept) | - | - | 1918.2 (985.5, 2850.9) | <0.001 |
| Age (1 year) | −2.1 (−14.1, 10.0) | 0.74 | 2.6 (−14.5, 19.6) | 0.77 |
| Dialysis vintage (1 month) | 2.1 (−0.4, 4.6) | 0.10 | 0.05 (−0.04, 0.13) | 0.27 |
| Charlson comorbidity index | −28.4 (−102.6, 45.7) | 0.45 | −17.3 (−120.8, 86.1) | 0.74 |
| Immunosuppressive medication | −814.7 (−1293.8, −355.9) | 0.001 | −867.3 (−1356.7, −377.9) | <0.001 |
| Hepatitis B vaccination non-response | −331.9 (−658.1, −5.6) | 0.046 | −290.8 (−605.3, 23.7) | 0.070 |
| ||||
| (Intercept) | - | - | 1167.7 (91.6, 2243.8) | 0.034 |
| Age (1 year) | −0.5 (−13.9, 12.9) | 0.94 | 0.2 (−19.4, 19.9) | 0.98 |
| Dialysis vintage (1 month) | 1.0 (−1.9, 3.8) | 0.50 | 0.02 (−0.07, 0.12) | 0.62 |
| Charlson comorbidity index | −7.9 (−90.5, 74.8) | 0.85 | −0.6 (119.9, 118.7) | 0.99 |
| Immunosuppressive medication | −382.7 (−933.3, 167.9) | 0.17 | −457.6 (−1031.3, 116.0) | 0.12 |
| Hepatitis B vaccination non-response | −228.1 (−590.7, 134.4) | 0.22 | −180.7 (−568.3, 206.8) | 0.36 |
| ||||
| (Intercept) | - | - | 837.9 (661.4, 1014.4) | <0.001 |
| Age (1 year) | −1.2 (−3.6, 1.1) | 0.30 | −1.3 (−4.6, 1.9) | 0.41 |
| Dialysis vintage (1 month) | 0.4 (−0.1, 0.19) | 0.12 | 0.01 (−0.01, 0.02) | 0.32 |
| Charlson comorbidity index | −7.0 (−21.3, 7.4) | 0.34 | 2.8 (−16.7, 22.3) | 0.78 |
| Immunosuppressive medication | −209.6 (−302.1, −117.0) | <0.001 | −223.0 (319.9, −126.0) | <0.001 |
| Hepatitis B vaccination non-response | −228.1 (−590.7, 134.4) | 0.22 | −22.8 (−86.5, 40.9) | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, C.-C.; Platen, L.; Christa, C.; Tellenbach, M.; Kappler, V.; Bester, R.; Liao, B.-H.; Holzmann-Littig, C.; Werz, M.; Schönhals, E.; et al. Improved SARS-CoV-2 Neutralization of Delta and Omicron BA.1 Variants of Concern after Fourth Vaccination in Hemodialysis Patients. Vaccines 2022, 10, 1328. https://doi.org/10.3390/vaccines10081328
Cheng C-C, Platen L, Christa C, Tellenbach M, Kappler V, Bester R, Liao B-H, Holzmann-Littig C, Werz M, Schönhals E, et al. Improved SARS-CoV-2 Neutralization of Delta and Omicron BA.1 Variants of Concern after Fourth Vaccination in Hemodialysis Patients. Vaccines. 2022; 10(8):1328. https://doi.org/10.3390/vaccines10081328
Chicago/Turabian StyleCheng, Cho-Chin, Louise Platen, Catharina Christa, Myriam Tellenbach, Verena Kappler, Romina Bester, Bo-Hung Liao, Christopher Holzmann-Littig, Maia Werz, Emely Schönhals, and et al. 2022. "Improved SARS-CoV-2 Neutralization of Delta and Omicron BA.1 Variants of Concern after Fourth Vaccination in Hemodialysis Patients" Vaccines 10, no. 8: 1328. https://doi.org/10.3390/vaccines10081328