
A Randomized Clinical Trial of a Fractional Low Dose of BNT162b2 Booster in Adults Following AZD1222

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Procedures
2.3. Immunogenicity Outcomes
2.3.1. Quantitative Spike Receptor Binding Domain IgG (Anti-S-RBD IgG) ELISA
2.3.2. Surrogate Virus Neutralization Test (sVNT)
2.3.3. Enzyme-Linked Immunospot (ELISpot) Assay
2.4. Reactogenicity
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
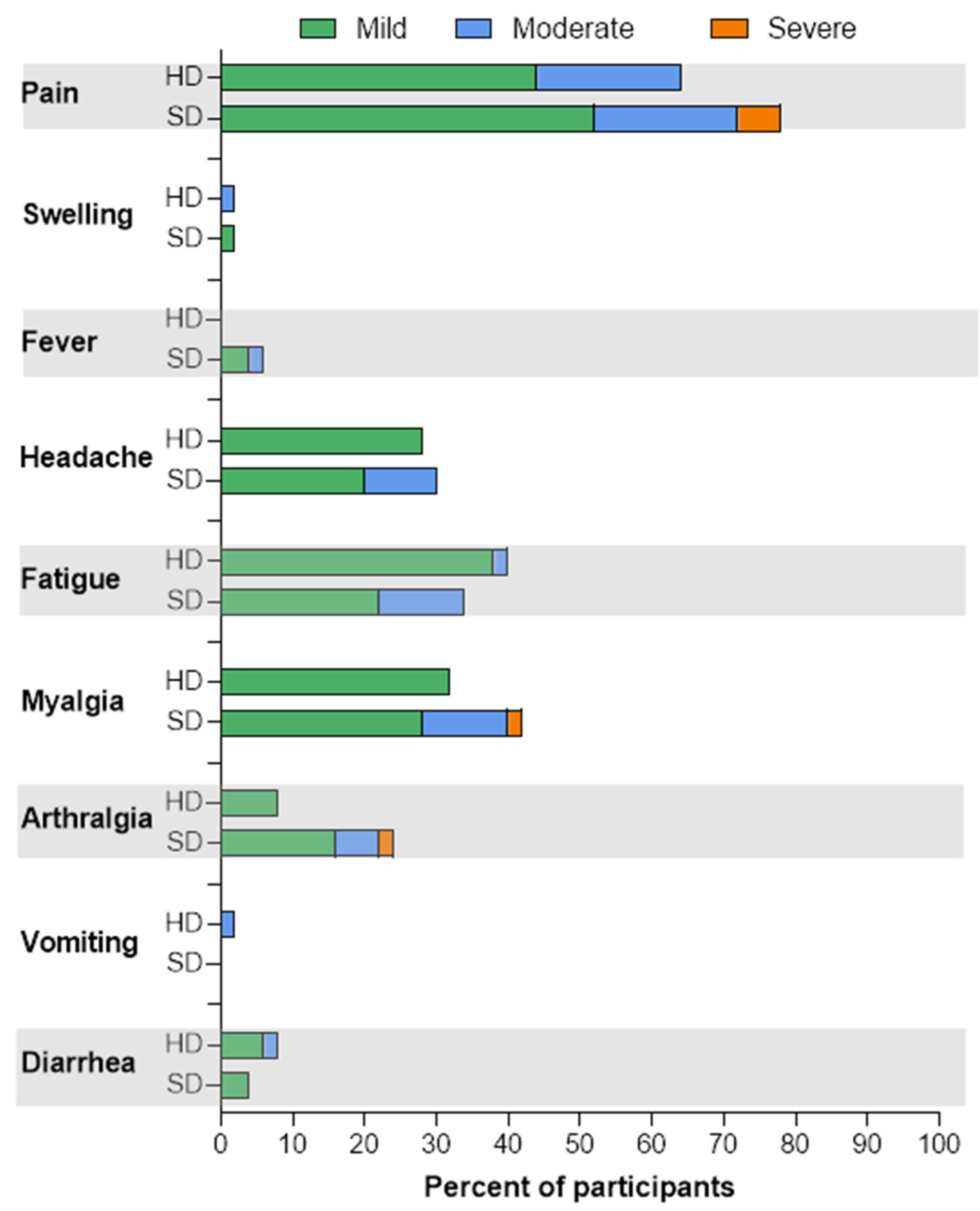
3.2. Reactogenicity
3.3. Immunogenicity
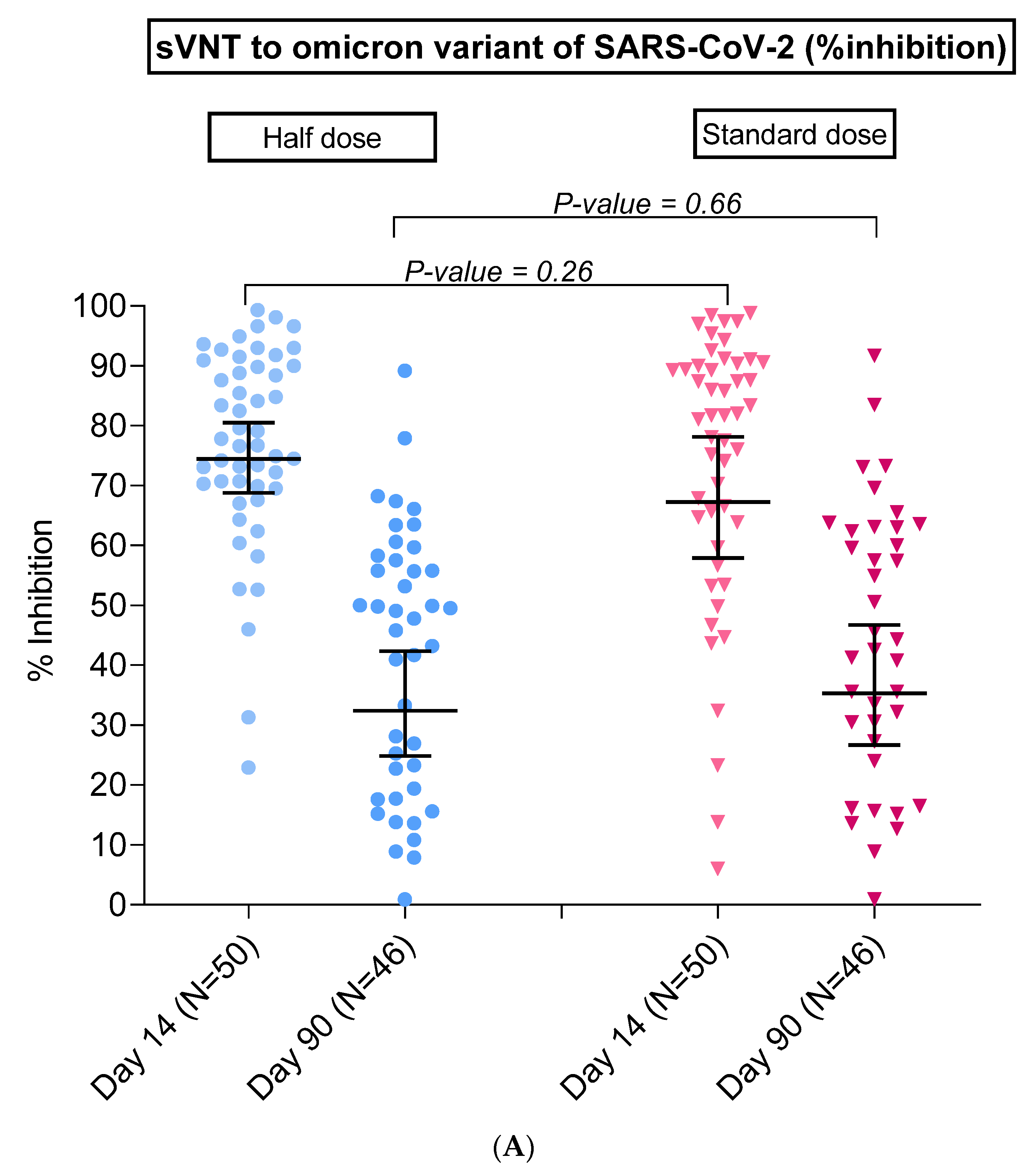
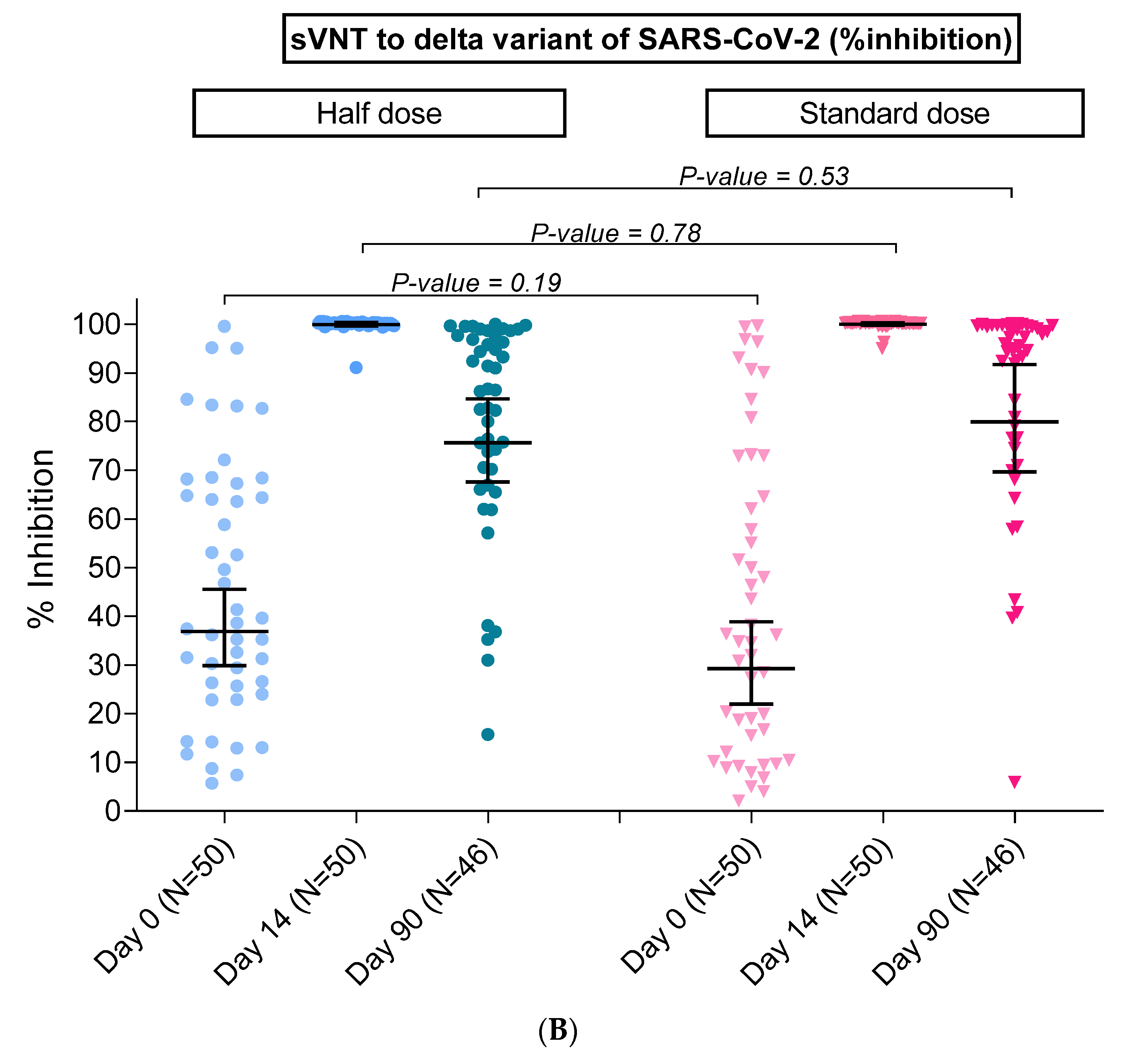
3.3.1. SARS-CoV-2-Neutralizing Antibody by Surrogate Virus Neutralization Test (sVNT)
3.3.2. SARS-CoV-2 Binding Antibody by Anti-S-RBD IgG
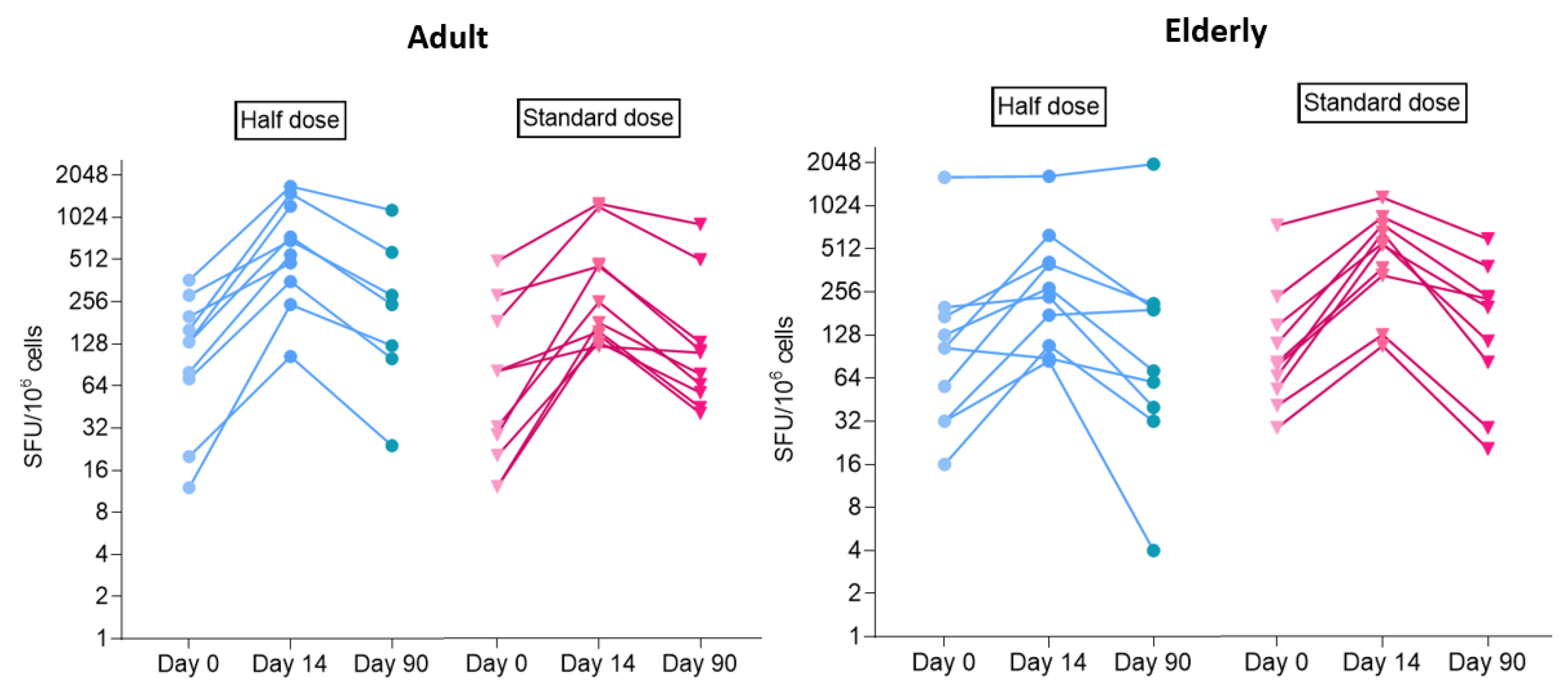
3.3.3. Cell-Mediated Immune Response by ELISpot Assay
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. COVID-19 Weekly Epidemiological Update Edition 42, Published 1 June 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---1-june-2021 (accessed on 14 March 2022).
- World Health Organization. COVID-19 Weekly Epidemiological Update Edition 74, Published 11 January 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---11-january-2022 (accessed on 14 March 2022).
- Ford, C.T.; Jacob Machado, D.; Janies, D.A. Predictions of the SARS-CoV-2 Omicron Variant (B.1.1.529) Spike Protein Receptor-Binding Domain Structure and Neutralizing Antibody Interactions. Front. Virol. 2022, 2, 830202. [Google Scholar] [CrossRef]
- Cele, S.; Jackson, L.; Khoury, D.S.; Khan, K.; Moyo-Gwete, T.; Tegally, H.; San, J.E.; Cromer, D.; Scheepers, C.; Amoako, D.G.; et al. Omicron extensively but incompletely escapes Pfizer BNT162b2 neutralization. Nature 2022, 602, 654–656. [Google Scholar] [CrossRef] [PubMed]
- Dejnirattisai, W.; Shaw, R.H.; Supasa, P.; Liu, C.; Stuart, A.S.; Pollard, A.J.; Liu, X.; Lambe, T.; Crook, D.; Stuart, D.I.; et al. Reduced neutralisation of SARS-CoV-2 omicron B.1.1.529 variant by post-immunisation serum. Lancet 2022, 399, 234–236. [Google Scholar] [CrossRef]
- Altarawneh, H.N.; Chemaitelly, H.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; AlMukdad, S.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Benslimane, F.M.; et al. Protection against the Omicron Variant from Previous SARS-CoV-2 Infection. N. Engl. J. Med. 2022, 386, 1288–1290. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Fast, H.E.; Zell, E.; Murthy, B.P.; Murthy, N.; Meng, L.; Scharf, L.G.; Black, C.L.; Shaw, L.; Chorba, T.; Harris, L.Q. Booster and Additional Primary Dose COVID-19 Vaccinations Among Adults Aged ≥ 65 Years—United States, August 13, 2021–November 19, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1735–1739. [Google Scholar] [CrossRef]
- Ferdinands, J.M.; Rao, S.; Dixon, B.E.; Mitchell, P.K.; DeSilva, M.B.; Irving, S.A.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.J.; et al. Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19-Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 255–263. [Google Scholar] [CrossRef]
- Liu, X.; Shaw, R.H.; Stuart, A.S.V.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, A.E.; Collins, A.M.; et al. Safety and immunogenicity of heterologous versus homologous prime-boost schedules with an adenoviral vectored and mRNA COVID-19 vaccine (Com-COV): A single-blind, randomised, non-inferiority trial. Lancet 2021, 398, 856–869. [Google Scholar] [CrossRef]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Mbaeyi, S.; Oliver, S.E.; Collins, J.P.; Godfrey, M.; Goswami, N.D.; Hadler, S.C.; Jones, J.; Moline, H.; Moulia, D.; Reddy, S.; et al. The Advisory Committee on Immunization Practices’ Interim Recommendations for Additional Primary and Booster Doses of COVID-19 Vaccines—United States, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.; Vrbicky, K.; Montefiori, D.; Huang, W.; Nestorova, B.; Chang, Y.; Carfi, A.; Edwards, D.K.; Oestreicher, J.; Legault, H.; et al. Immune response to SARS-CoV-2 after a booster of mRNA-1273: An open-label phase 2 trial. Nat. Med. 2022, 28, 1042–1049. [Google Scholar] [CrossRef]
- Angkasekwinai, N.; Niyomnaitham, S.; Sewatanon, J.; Phumiamorn, S.; Sukapirom, K.; Senawong, S.; Mahasirimongkol, S.; Umrod, P.; Sompornet, T.; Chumpol, S.; et al. The immunogenicity and safety of different COVID-19 booster vaccination following CoronaVac or ChAdOx1 nCoV-19 primary series. medRxiv 2021. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Więcek, W.; Ahuja, A.; Chaudhuri, E.; Kremer, M.; Gomes, A.S.; Snyder, C.M.; Tabarrok, A.; Tan, B.J. Testing fractional doses of COVID-19 vaccines. Proc. Natl. Acad. Sci. USA 2022, 119, e2116932119. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent Immune Response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Amanat, F.; Stadlbauer, D.; Strohmeier, S.; Nguyen, T.H.O.; Chromikova, V.; McMahon, M.; Jiang, K.; Arunkumar, G.A.; Jurczyszak, D.; Polanco, J.; et al. A serological assay to detect SARS-CoV-2 seroconversion in humans. Nat. Med. 2020, 26, 1033–1036. [Google Scholar] [CrossRef]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.-C.; Tiu, C.; Hu, Z.; Chen, V.C.-W.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services FDA (CBER). Guidance for Industry Toxicity Grading Scale for Healthy Adult and Adolescent Volunteers Enrolled in Preventive Vaccine Clinical Trials September 2007. Available online: https://www.fda.gov/media/73679/download (accessed on 30 November 2021).
- World Health Organization. Guidelines on Clinical Evaluation of Vaccines: Regulatory Expectations, WHO Technical Report Series 1004, Annex 9. 2017. Available online: https://www.who.int/publications/m/item/WHO-TRS-1004-web-annex-9 (accessed on 12 December 2021).
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Hause, A.M.; Baggs, J.; Marquez, P.; Myers, T.R.; Su, J.R.; Blanc, P.G.; Baumblatt, J.A.G.; Woo, E.J.; Gee, J.; Shimabukuro, T.T.; et al. Safety Monitoring of COVID-19 Vaccine Booster Doses Among Adults—United States, September 22, 2021–February 6, 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Joint Committee on Vaccination and Immunisation (JCVI). JCVI Statement on the Adult COVID-19 Booster Vaccination Programme and the Omicron Variant: 7 January 2022. Available online: https://www.gov.uk/government/publications/jcvi-statement-on-the-adult-covid-19-booster-vaccination-programme-and-the-omicron-variant/jcvi-statement-on-the-adult-covid-19-booster-vaccination-programme-and-the-omicron-variant-7-january-2022 (accessed on 12 April 2022).
- World Health Organization Africa. Africa’s COVID-19 Vaccine Uptake Increases by 15% 2022; updated 17 March 2022. Available online: https://www.afro.who.int/news/africas-covid-19-vaccine-uptake-increases-15 (accessed on 13 April 2022).
- Kanokudom, S.; Assawakosri, S.; Suntronwong, N.; Chansaenroj, J.; Auphimai, C.; Nilyanimit, P.; Vichaiwattana, P.; Thongmee, T.; Yorsaeng, R.; Duangchinda, T.; et al. Comparison of the reactogenicity and immunogenicity of a reduced and standard booster dose of the mRNA COVID-19 vaccine in healthy adults after two doses of inactivated vaccine. medRxiv 2022. [Google Scholar] [CrossRef]
- Moss, P. The T cell immune response against SARS-CoV-2. Nat. Immunol. 2022, 23, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Naranbhai, V.; Nathan, A.; Kaseke, C.; Berrios, C.; Khatri, A.; Choi, S.; Getz, M.A.; Tano-Menka, R.; Ofoman, O.; Gayton, A.; et al. T cell reactivity to the SARS-CoV-2 Omicron variant is preserved in most but not all individuals. Cell 2022, 185, 1041–1051.e6. [Google Scholar] [CrossRef]
- Tarke, A.; Coelho, C.H.; Zhang, Z.; Dan, J.M.; Yu, E.D.; Methot, N.; Bloom, N.I.; Goodwin, B.; Phillips, E.; Mallal, S.; et al. SARS-CoV-2 vaccination induces immunological T cell memory able to cross-recognize variants from Alpha to Omicron. Cell 2022, 185, 847–859.e11. [Google Scholar] [CrossRef]
- World Health Organization. Interim Statement on COVID-19 Vaccines in the Context of the Circulation of the Omicron SARS-CoV-2 Variant from the WHO Technical Advisory Group on COVID-19 Vaccine Composition (TAG-CO-VAC). 8 March 2022. Available online: https://www.who.int/news/item/08-03-2022-interim-statement-on-covid-19-vaccines-in-the-context-of-the-circulation-of-the-omicron-sars-cov-2-variant-from-the-who-technical-advisory-group-on-covid-19-vaccine-composition-(tag-co-vac)-08-march-2022 (accessed on 28 March 2022).
- Fang, Z.; Peng, L.; Filler, R.; Suzuki, K.; McNamara, A.; Lin, Q.; Renauer, P.A.; Yang, L.; Menasche, B.; Sanchez, A.; et al. Omicron-specific mRNA vaccination alone and as a heterologous booster against SARS-CoV-2. BioRxiv 2022. [Google Scholar] [CrossRef]
- Hawman, D.W.; Meade-White, K.; Clancy, C.; Archer, J.; Hinkley, T.; Leventhal, S.S.; Rao, D.; Stamper, A.; Lewis, M.; Rosenke, R.; et al. Replicating RNA platform enables rapid response to the SARS-CoV-2 Omicron variant and elicits enhanced protection in naïve hamsters compared to ancestral vaccine. BioRxiv 2022. [Google Scholar] [CrossRef]
- Lee, I.-J.; Sun, C.-P.; Wu, P.-Y.; Lan, Y.-H.; Wang, I.-H.; Liu, W.-C.; Tseng, S.-C.; Tsung, S.-I.; Chou, Y.-C.; Kumari, M.; et al. Omicron-specific mRNA vaccine induced potent neutralizing antibody against Omicron but not other SARS-CoV-2 variants. BioRxiv 2022. [Google Scholar] [CrossRef]
- Ying, B.; Scheaffer, S.M.; Whitener, B.; Liang, C.-Y.; Dmytrenko, O.; Mackin, S.; Wu, K.; Lee, D.; Avena, L.E.; Chong, Z.; et al. Boosting with Omicron-matched or historical mRNA vaccines increases neutralizing antibody responses and protection against B.1.1.529 infection in mice. BioRxiv 2022. [Google Scholar] [CrossRef]
- Gagne, M.; Moliva, J.I.; Foulds, K.E.; Andrew, S.F.; Flynn, B.J.; Werner, A.P.; Wagner, D.A.; Teng, I.T.; Lin, B.C.; Moore, C.; et al. mRNA-1273 or mRNA-Omicron boost in vaccinated macaques elicits comparable B cell expansion, neutralizing antibodies and protection against Omicron. BioRxiv 2022. [Google Scholar] [CrossRef]
- ModernaTX Inc. A Study to Evaluate the Immunogenicity and Safety of mRNA-1273.529 Vaccine for the COVID-19 Omicron Variant, B.1.1.529. Available online: https://clinicaltrials.gov/ct2/show/NCT05249829 (accessed on 28 March 2022).
- BioNTech SE. To Evaluate the Safety, Tolerability, Efficacy and Immunogenicity of BNT162b2 Boosting Strategies against COVID-19 in Participants ≥ 12 Years of Age. Available online: https://clinicaltrials.gov/ct2/show/NCT04955626 (accessed on 28 March 2022).
- Coalition for Epidemic Preparedness Innovations (CEPI). CEPI, THSTI and Panacea Biotec Partner to Develop Broadly Protective Betacoronavirus Vaccines 2022. Available online: https://cepi.net/news_cepi/cepi-thsti-and-panacea-biotec-partner-to-develop-broadly-protective-betacoronavirus-vaccines/ (accessed on 29 March 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 100) | Half-Dose BNT162b2 Booster (15 µg/Dose) (n = 50) | Standard-Dose BNT162b2 Booster (30 µg/Dose) (n = 50) |
|---|---|---|---|
| Age (years), median (IQR) | 59.3 (33.4–65.5) | 59.3 (32.2–65.5) | 57.9 (33.6–65.8) |
| - Group 18–59 years | 33.4 (28.1–43.0) | 32.3 (28.1–42.1) | 33.6 (29.7–43.4) |
| - Group 60–69 years | 65.5 (63.3–67.8) | 65.5 (63.2–67.8) | 65.8 (64.0–67.8) |
| Female, n (%) | 61 (61) | 31 (62) | 30 (60) |
| BMI (kg/m2), median (IQR) | 23.3 (21.8–26.1) | 22.8 (21.1–25.3) | 23.8 (22.3–27.5) |
| Interval between 2nd dose of AZD1222 to BNT162b2 (days), median (IQR) | 98 (92–128) | 98 (92–131) | 98 (92–126) |
| sVNT to delta variant (% inhibition), GM (95% CI) | 32.8 (27.5–39.1) | 36.9 (29.9–45.6) | 29.2 (22.0–38.9) |
| sVNT to wild type (% inhibition), GM (95% CI) | 39.4 (33.5–46.5) | 42.8 (34.8–52.6) | 36.4 (28.1–47.2) |
| Anti-S-RBD IgG (BAU/mL), GM (95% CI) | 199.1 (170.1–233.0) | 193.7 (156.2–240.2) | 204.6 (161.5–259.3) |
| Immunogenicity Outcomes | Half Dose GM (95% CI) (n = 50) | Standard Dose GM (95% CI) (n = 50) | GMR (95% CI) |
|---|---|---|---|
| sVNT to omicron variant (% inhibition) | |||
| Day 14 | 74.4 (68.8–80.5) | 67.3 (57.9–78.1) | 1.11 (0.93–1.30) |
| Day 90 | 22.3 (14.9–33.4) | 20.4 (13.1–32.0) | 1.09 (0.60–1.98) |
| sVNT to delta variant (% inhibition) | |||
| Day 14 | 100.0 (99.6–100.4) | 100.0 (99.8–100.3) | 1.00 (0.99–1.00) |
| Day 90 | 75.7 (67.6–84.7) | 79.9 (69.7–91.7) | 0.95 (0.79–1.13) |
| Anti-S-RBD IgG (BAU/mL) | |||
| Day 14 | 2329.8 (2109.3–2573.4) | 2574.7 (2262.5–2929.9) | 0.90 (0.77–1.06) |
| Day 90 | 549.6 (479.1–630.5) | 676.1 (573.8–796.7) | 0.81 (0.66–1.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nantanee, R.; Jantarabenjakul, W.; Jaru-Ampornpan, P.; Sodsai, P.; Himananto, O.; Athipunjapong, J.; Sophonphan, J.; Nanthapisal, S.; Hirankarn, N.; Puthanakit, T., on behalf of the Study Team. A Randomized Clinical Trial of a Fractional Low Dose of BNT162b2 Booster in Adults Following AZD1222. Vaccines 2022, 10, 914. https://doi.org/10.3390/vaccines10060914
Nantanee R, Jantarabenjakul W, Jaru-Ampornpan P, Sodsai P, Himananto O, Athipunjapong J, Sophonphan J, Nanthapisal S, Hirankarn N, Puthanakit T on behalf of the Study Team. A Randomized Clinical Trial of a Fractional Low Dose of BNT162b2 Booster in Adults Following AZD1222. Vaccines. 2022; 10(6):914. https://doi.org/10.3390/vaccines10060914
Chicago/Turabian StyleNantanee, Rapisa, Watsamon Jantarabenjakul, Peera Jaru-Ampornpan, Pimpayao Sodsai, Orawan Himananto, Jitthiwa Athipunjapong, Jiratchaya Sophonphan, Sira Nanthapisal, Nattiya Hirankarn, and Thanyawee Puthanakit on behalf of the Study Team. 2022. "A Randomized Clinical Trial of a Fractional Low Dose of BNT162b2 Booster in Adults Following AZD1222" Vaccines 10, no. 6: 914. https://doi.org/10.3390/vaccines10060914