
Adverse Events and Safety Profile of the COVID-19 Vaccines in Adolescents: Safety Monitoring for Adverse Events Using Real-World Data

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
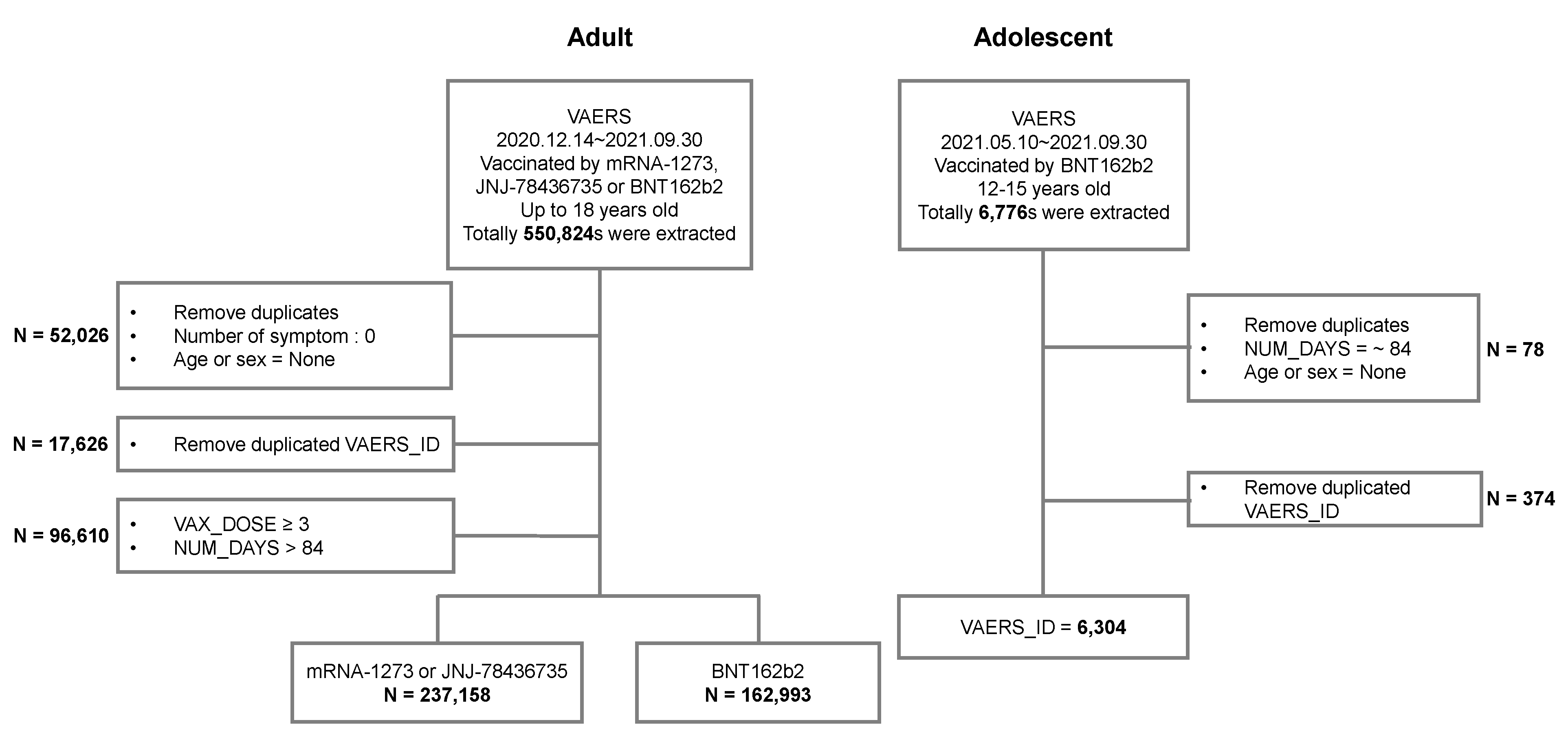
2.2. Setting and Study Population
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
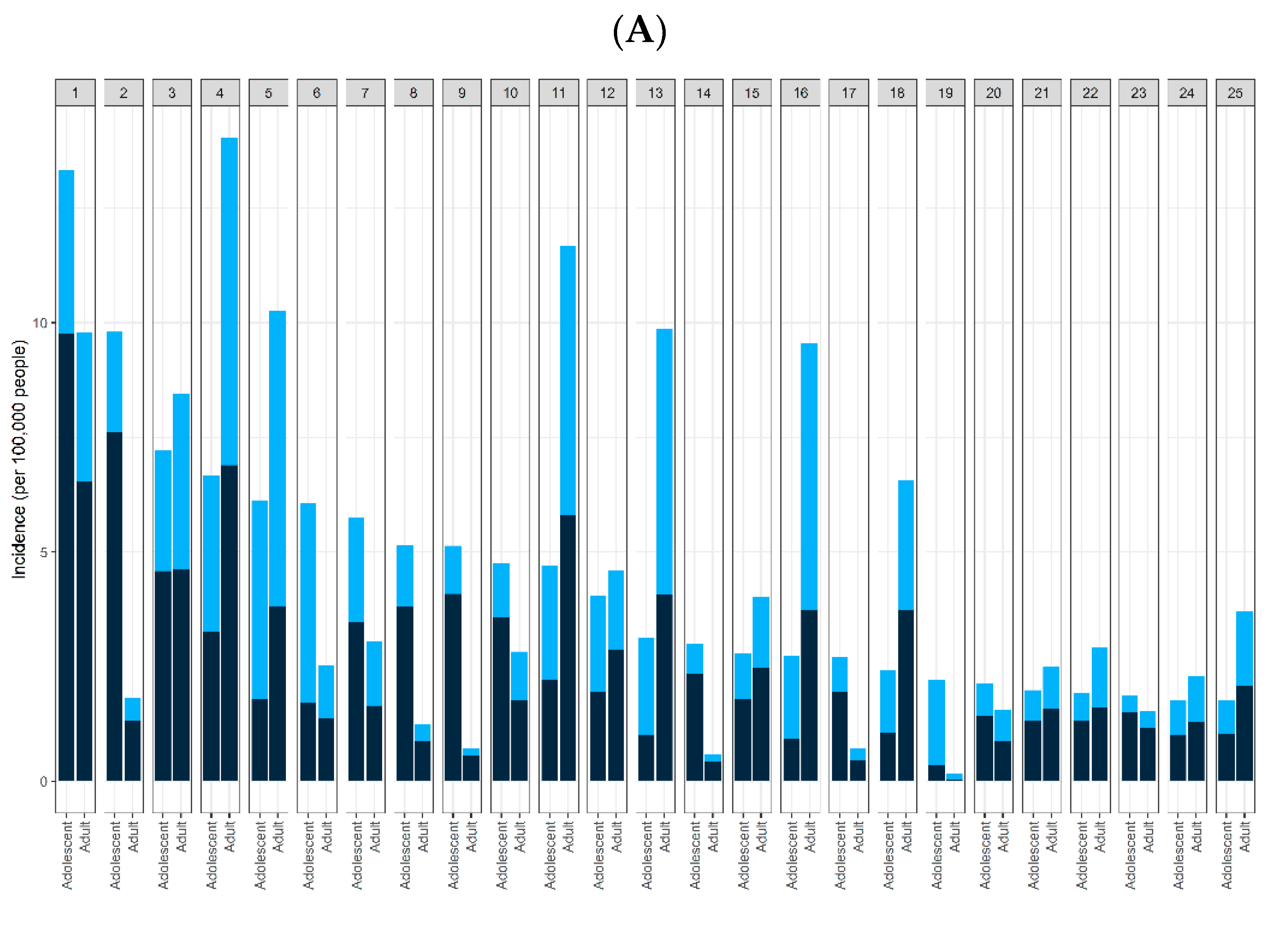
3.2. Common AEs
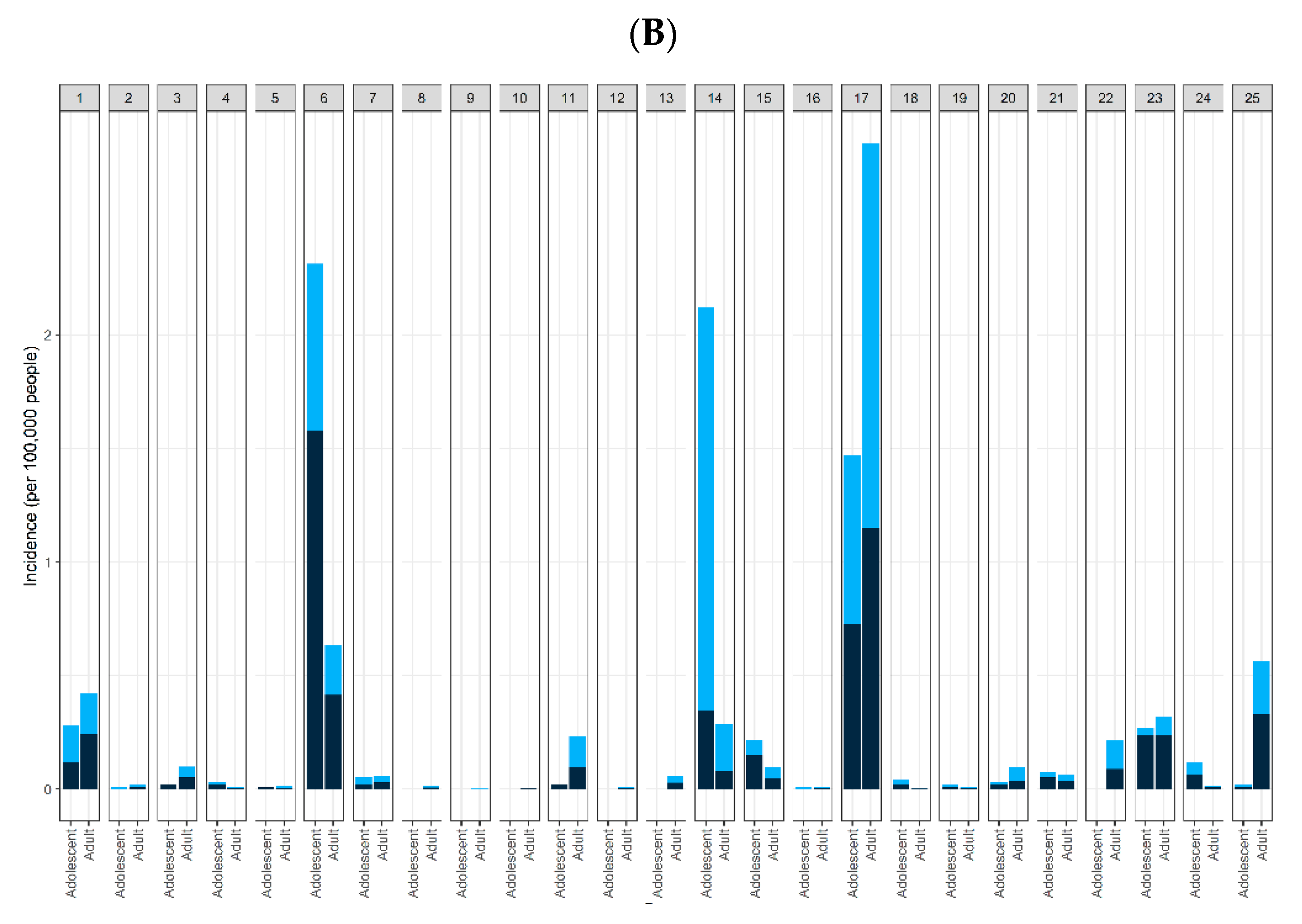
3.3. Severe AEs
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight Against Pandemic. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-pfizer-biontech-covid-19-vaccine-emergency-use (accessed on 25 October 2021).
- Umei, T.C.; Kishino, Y.; Watanabe, K.; Shiraishi, Y.; Inohara, T.; Yuasa, S.; Fukuda, K. Recurrence of myopericarditis following mRNA COVID-19 vaccination in a male adolescent. CJC Open 2021, 4, 350–352. [Google Scholar] [CrossRef] [PubMed]
- Das, B.B.; Kohli, U.; Ramachandran, P.; Nguyen, H.H.; Greil, G.; Hussain, T.; Tandon, A.; Kane, C.; Avula, S.; Duru, C.; et al. Myopericarditis after messenger RNA Coronavirus Disease 2019 Vaccination in Adolescents 12 to 18 Years of Age. J. Pediatr. 2021, 238, 26–32.e1. [Google Scholar] [CrossRef] [PubMed]
- Epidemiology Working Group for NCIP Epidemic Response; Chinese Center for Disease Control and Prevention. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Article in Chinese. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145–151. [Google Scholar]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef] [PubMed]
- CDC. COVID-19 Response Team Coronavirus disease 2019 in children—United States, 12 February–2 April 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 422–426. [Google Scholar] [CrossRef]
- COVID-19 National Incident Room Surveillance Team. COVID-19, Australia: Epidemiology report 13 (reporting week to 23:59 AEST 26 April 2020). Commun. Dis. Intell. 2020, 44. [Google Scholar] [CrossRef]
- Mania, A.; Mazur-Melewska, K.; Lubarski, K.; Kuczma-Napierała, J.; Mazurek, J.; Jończyk-Potoczna, K.; Służewski, W.; Figlerowicz, M. Wide spectrum of clinical picture of COVID-19 in children—From mild to severe disease. J. Infect. Public Health 2021, 14, 374–379. [Google Scholar] [CrossRef]
- Ladhani, S.N.; Amin-Chowdhury, Z.; Davies, H.G.; Aiano, F.; Hayden, I.; Lacy, J.; Sinnathamby, M.; de Lusignan, S.; Demirjian, A.; Whittaker, H.; et al. COVID-19 in children: Analysis of the first pandemic peak in England. Arch. Dis. Child. 2020, 105, 1180–1185. [Google Scholar] [CrossRef]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Calò Carducci, F.I.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. Ptbnet COVID-19 Study Group. COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. Lancet Child Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- Jain, S.; Nolan, S.M.; Singh, A.R.; Lovig, L.; Biller, R.; Kamat, A.; Brennan, M.H.; Erb, M.; Rescoe, E.; Tatz, G.; et al. Myocarditis in Multisystem Inflammatory Syndrome in Children Associated With Coronavirus Disease 2019. Cardiol. Rev. 2020, 28, 308–311. [Google Scholar] [CrossRef]
- Arizaga-Ballesteros, V.; Gutierrez-Mendoza, M.A.; Villanueva-Sugishima, K.R.; Santos-Guzmán, J. Pediatric Inflammatory Multisystem Syndrome or Multisystem Inflammatory Syndrome in Children: A New Thread in Pandemic Era. Glob. Pediatr. Health 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.H.; Lee, S.Y.; Choi, J.W.; Korean Society of Kawasaki Disease. Clinical features, diagnosis, and outcomes of multisystem inflammatory syndrome in children associated with coronavirus disease 2019. Clin. Exp. Pediatr. 2021, 64, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, Immunogenicity, and Efficacy of the BNT162b2 COVID-19 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef]
- Vaccine Adverse Event Reporting System (VAERS) Data. Available online: https://vaers.hhs.gov/data.html (accessed on 25 October 2021).
- Shimabukuro, T.T.; Nguyen, M.; Martin, D.; DeStefano, F. Safety monitoring in the Vaccine Adverse Event Reporting System (VAERS). Vaccine 2015, 33, 4398–4405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 vaccine in a nationwide setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef] [PubMed]
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for adverse events after COVID-19 mRNA vaccination. JAMA 2021, 326, 1390–1399. [Google Scholar] [CrossRef]
- Diaz, G.A.; Parsons, G.T.; Gering, S.K.; Meier, A.R.; Hutchinson, I.V.; Robicsek, A. Myocarditis and Pericarditis After Vaccination for COVID-19. JAMA 2021, 326, 1210–1212. [Google Scholar] [CrossRef]
- Kim, H.W.; Jenista, E.R.; Wendell, D.C.; Azevedo, C.F.; Campbell, M.J.; Darty, S.N.; Parker, M.A.; Kim, R.J. Patients With Acute Myocarditis Following mRNA COVID-19 Vaccination. JAMA Cardiol. 2021, 6, 1196–1201. [Google Scholar] [CrossRef]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat. Med. 2022, 28, 410–422. [Google Scholar] [CrossRef]
- Hajjo, R.; Sabbah, D.A.; Bardaweel, S.K.; Tropsha, A. Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients. Vaccines 2021, 9, 1186. [Google Scholar] [CrossRef]
- Abu Mouch, S.; Roguin, A.; Hellou, E.; Ishai, A.; Shoshan, U.; Mahamid, L.; Zoabi, M.; Aisman, M.; Goldschmid, N.; Yanay, N.B. Myocarditis following COVID-19 mRNA vaccination. Vaccine 2021, 39, 3790–3793. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.S.; Steele, J.M.; Fonseca, B.; Huang, S.; Shah, S.; Maskatia, S.A.; Buddhe, S.; Misra, N.; Ramachandran, P.; Gaur, L.; et al. COVID-19 Vaccination-Associated Myocarditis in Adolescents. Pediatrics 2021, 148, e2021053427. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Yuan, J.; Lv, G.; Brown, J.; Jiang, X.; Lu, Z.K. Myocarditis and Pericarditis following COVID-19 Vaccination: Inequalities in Age and Vaccine Types. J. Pers. Med. 2021, 11, 1106. [Google Scholar] [CrossRef] [PubMed]
- Starekova, J.; Bluemke, D.A.; Bradham, W.S.; Grist, T.M.; Schiebler, M.L.; Reeder, S.B. Myocarditis Associated with mRNA COVID-19 Vaccination. Radiology 2021, 301, E409–E411. [Google Scholar] [CrossRef]
- Engler, R.J.M.; Nelson, M.R.; Collin, L.C., Jr.; Spooner, C.; Hemann, B.A.; Gibbs, B.T.; Atwood, J.E.; Howard, R.S.; Chang, A.S.; Cruser, D.L.; et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS ONE 2015, 10, e0118283. [Google Scholar] [CrossRef] [Green Version]
- Morgan, J.; Roper, M.H.; Sperling, L.; Schieber, R.A.; Heffelfinger, J.D.; Casey, C.G.; Miller, J.W.; Santibanez, S.; Herwaldt, B.; Hightower, P.; et al. Myocarditis, pericarditis, and dilated cardiomyopathy after smallpox vaccination among civilians in the United States, January-October 2003. Clin. Infect. Dis. 2008, 46 (Suppl. S3), S242–S250. [Google Scholar] [CrossRef]
- Hu, H.; Ma, F.; Wei, X.; Fang, Y. Coronavirus fulminant myocarditis treated with glucocorticoid and human immunoglobulin. Eur. Heart J. 2021, 42, 206. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Zhou, Y.; Wang, D.W. SARS-CoV-2: A potential novel etiology of fulminant myocarditis. Herz 2020, 45, 230–232. [Google Scholar] [CrossRef] [Green Version]
- Zeng, J.H.; Liu, Y.X.; Yuan, J.; Wang, F.X.; Wu, W.B.; Li, J.X.; Wang, L.F.; Gao, H.; Wang, Y.; Dong, C.F.; et al. First case of COVID-19 complicated with fulminant myocarditis: A case report and insights. Infection 2020, 48, 773–777. [Google Scholar] [CrossRef] [Green Version]
- Heymans, S.; Cooper, L.T. Myocarditis after COVID-19 mRNA vaccination: Clinical observations and potential mechanisms. Nat. Rev. Cardiol. 2022, 19, 75–77. [Google Scholar] [CrossRef]
- Ilonze, O.J.; Guglin, M.E. Myocarditis following COVID-19 vaccination in adolescents and adults: A cumulative experience of 2021. Heart Fail. Rev. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Israel Ministry of Health. Surveillance of Myocarditis (Inflammation of the Heart Muscle) Cases between December 2020 and May 2021 (Including). Available online: https://www.gov.il/en/departments/news/01062021-03 (accessed on 17 March 2022).
- Nygaard, U.; Holm, M.; Bohnstedt, C.; Chai, Q.; Schmidt, L.S.; Hartling, U.B.; Petersen, J.J.H.; Thaarup, J.; Bjerre, J.; Vejlstrup, N.G.; et al. Population-based Incidence of Myopericarditis After COVID-19 Vaccination in Danish Adolescents. Pediatr. Infect. Dis. J. 2022, 41, e25–e28. [Google Scholar] [CrossRef] [PubMed]
- Switzer, C.; Loeb, M. Evaluating the relationship between myocarditis and mRNA vaccination. Expert Rev. Vaccines 2022, 21, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Hause, A.M.; Gee, J.; Baggs, J.; Abara, W.E.; Marquez, P.; Thompson, D.; Su, J.R.; Licata, C.; Rosenblum, H.G.; Myers, T.R.; et al. COVID-19 Vaccine Safety in Adolescents Aged 12–17 Years—United States, 14 December 2020–16 July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Sookaromdee, P.; Wiwanitkit, V. Acute Myocardial Injury Following COVID-19 Vaccination. J. Prim. Care Community Health 2021, 12. [Google Scholar] [CrossRef]
- Azevedo, R.B.; Botelho, B.G.; Hollanda, J.V.G.; Ferreira, L.V.L.; de Andrade, L.Z.J.; Oei, S.S.M.L.; Mello, T.S.; Muxfeldt, E.S. COVID-19 and the cardiovascular system: A comprehensive review. J. Hum. Hypertens. 2021, 35, 4–11. [Google Scholar] [CrossRef]
- Nune, A.; Iyengar, K.P.; Goddard, C.; Ahmed, A.E. Multisystem inflammatory syndrome in an adult following the SARS-CoV-2 vaccine (MIS-V). BMJ Case Rep. 2021, 14, e243888. [Google Scholar] [CrossRef]
- Chai, Q.; Nygaard, U.; Schmidt, R.C.; Zaremba, T.; Møller, A.M.; Thorvig, C.M. Multisystem inflammatory syndrome in a male adolescent after his second Pfizer-BioNTech COVID-19 vaccine. Acta Paediatr. 2022, 111, 125–127. [Google Scholar] [CrossRef]
- Yalçinkaya, R.; Polat, M.; Cinni, R.G.; Öz, F.N.; Tanir, G.; Yazici, M.U. Crimean-Congo Hemorrhagic Fever Mimicking Multisystem Inflammatory Syndrome in Children Associated With COVID-19: A Diagnostic Challenge. Pediatr. Infect. Dis. J. 2021, 40, e524–e525. [Google Scholar] [CrossRef]
- Jiang, L.; Tang, K.; Levin, M.; Irfan, O.; Morris, S.K.; Wilson, K.; Klein, J.D.; Bhutta, Z.A. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect. Dis. 2020, 20, e276–e288. [Google Scholar] [CrossRef]
- Chouchana, L.; Blet, A.; Al-Khalaf, M.; Kafil, T.S.; Nair, G.; Robblee, J.; Drici, M.D.; Valnet-Rabier, M.B.; Micallef, J.; Salvo, F.; et al. Features of Inflammatory Heart Reactions Following mRNA COVID-19 Vaccination at a Global Level. Clin. Pharmacol. Ther. 2022, 111, 605–613. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, L.; Toledo, N.A.; Budrie, L.; Waechter, R.; Rayner, J. A Systematic Review of Severe Neurological Manifestations in Pediatric Patients with Coexisting SARS-CoV-2 Infection. Neurol. Int. 2021, 13, 410–427. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.J.; Chavarria, H.D.; Hacking, S.M. A Case of Multisystem Inflammatory Syndrome in Children Mimicking Acute Appendicitis in a COVID-19 Pandemic Area. Cureus 2020, 12, e10722. [Google Scholar] [CrossRef] [PubMed]
- Hwang, M.; Wilson, K.; Wendt, L.; Pohlman, J.; Densmore, E.; Kaeppler, C.; Arendonk, K.V.; Yale, S. The Great Gut Mimicker: A case report of MIS-C and appendicitis clinical presentation overlap in a teenage patient. BMC Pediatr. 2021, 21, 258. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Severe AEs | |||
|---|---|---|---|
| Total | Dose1 | Dose2 | |
| Female | |||
| 12 | 738 | 457 | 281 |
| 13 | 786 | 504 | 282 |
| 14 | 853 | 552 | 301 |
| 15 | 945 | 604 | 341 |
| Sum | 3322 | 2117 | 1205 |
| Male | |||
| 12 | 714 | 407 | 307 |
| 13 | 668 | 403 | 265 |
| 14 | 763 | 463 | 300 |
| 15 | 837 | 497 | 340 |
| Sum | 2982 | 1770 | 1212 |
| Total | 6304 | 3887 | 2417 |
| Lymphadenopathy | Myocarditis/Pericarditis | |||||
|---|---|---|---|---|---|---|
| OR * | 95% CI | p | OR * | 95% CI | p | |
| Sex (M/F) | 1.96 | 1.38–2.80 | <0.001 | 6.61 | 4.43–9.88 | <0.001 |
| Age (years) | 0.91 | 0.78–1.06 | 0.23 | 1.53 | 1.33–1.76 | <0.001 |
| Symptom onset (days) | 1.03 | 1.01–1.05 | 0.002 | 1.02 | 0.999–1.04 | 0.06 |
| Dose series † | 1.54 | 1.09–2.17 | 0.01 | 8.52 | 5.79–12.54 | <0.001 |
| Multisystem inflammatory syndrome in children/adults | Death | |||||
| OR * | 95% CI | p | OR * | 95% CI | p | |
| Sex (M/F) | 0.91 | 0.28–2.99 | 0.88 | NA | 0–Inf | 0.99 |
| Age (years) | 0.78 | 0.46–1.33 | 0.36 | 1.39 | 0.35–5.42 | 0.64 |
| Symptom onset (days) | 1.03 | 0.97–1.09 | 0.41 | 1.08 | 1.02–1.14 | 0.005 |
| Dose series † | 1.27 | 0.38–4.22 | 0.70 | 1.08 | 0.06–18.39 | 0.96 |
| Adolescents | Adults | |||||
|---|---|---|---|---|---|---|
| Symptom | Number | Incidence † of Events (Onset Day-Median) | Number | Incidence † of Events (Onset Day-Median) | Relative Risk * (95% CI) | Fisher’s Exact Test p |
| Bell’s palsy | 26 | 0.28 (7) | 728 | 0.32 (6) | 0.87 (0.59–1.29) | 0.57 |
| Stroke, hemorrhagic | 1 | 0.01 (51) | 22 | 0.01 (6.5) | 1.11 (0.15–8.24) | 0.60 |
| Stroke, ischemic | 2 | 0.02 (12.5) | 105 | 0.05 (5) | 0.47 (0.11–1.89) | 0.45 |
| Encephalitis/myelitis/encephalomyelitis | 2 | 0.02 (8.5) | 2 | 0 (5.5) | 24.43 (3.44–173.43) | 0.01 * |
| Cerebral venous sinus thrombosis | 1 | 0.01 (19) | 16 | 0.01 (10.5) | 1.53 (0.2–11.51) | 0.49 |
| Convulsions/seizures | 197 | 2.13 (0) | 844 | 0.37 (0) | 5.7 (4.88–6.66) | <0.001 § |
| Guillain–Barré syndrome | 6 | 0.06 (17) | 53 | 0.02 (5) | 2.77 (1.19–6.43) | 0.03 ‡ |
| Transverse myelitis | 0 | 0 | 13 | 0.01 (8) | _ | 1.00 |
| Acute disseminated encephalomyelitis | 0 | 0 | 1 | 0 (8) | _ | 1.00 |
| Narcolepsy/cataplexy | 0 | 0 | 6 | 0 (1) | _ | 1.00 |
| Pulmonary embolism | 2 | 0.02 (18) | 237 | 0.10 (11) | 0.21 (0.05–0.83) | 0.01 ‡ |
| Acute respiratory distress syndrome | 0 | 0 | 6 | 0 (13.5) | _ | 1.00 |
| Acute myocardial infarction | 0 | 0 | 59 | 0.03 (10) | _ | 0.18 |
| Myocarditis/pericarditis | 211 | 2.28 (2) | 263 | 0.12 (3) | 19.6 (16.35–23.49) | <0.001 § |
| Appendicitis | 20 | 0.22 (2) | 143 | 0.06 (6) | 3.42 (2.14–5.46) | <0.001 § |
| Anemia | 1 | 0.01 (29) | 9 | 0 (3) | 2.71 (0.34–21.42) | 0.33 |
| Lymphadenopathy | 136 | 1.47 (1) | 726 | 0.32 (1) | 4.58 (3.81–5.5) | <0.001 § |
| Lymphopenia | 4 | 0.04 (17) | 1 | 0 (9) | 97.72 (10.92–874.28) | <0.001 § |
| Neutropenia | 2 | 0.02 (13) | 8 | 0 (13.5) | 6.11 (1.3–28.76) | 0.06 |
| Other thrombosis | 3 | 0.03 (5) | 107 | 0.05 (9) | 0.68 (0.22–2.16) | 0.80 |
| Thrombocytopenia | 7 | 0.08 (13) | 75 | 0.03 (10) | 2.28 (1.05–4.95) | 0.04 ‡ |
| Deep vein thrombosis | 0 | 0 | 285 | 0.13 (8) | _ | <0.001 § |
| Anaphylaxis | 1 | 0.01 (0) | 29 | 0.01 (0) | 0.84 (0.11–6.18) | 1.00 |
| Multisystem inflammatory syndrome in children/adults | 10 | 0.11 (1) | 1 | 0 (1) | 244.3 (31.27–1908.38) | <0.001 § |
| Death | 2 | 0.02 (20) | 726 | 0.32 (5) | 0.07 (0.02–0.27) | <0.001 § |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.W.; Sa, S.; Hong, M.; Kim, J.; Shim, S.R.; Han, H.W. Adverse Events and Safety Profile of the COVID-19 Vaccines in Adolescents: Safety Monitoring for Adverse Events Using Real-World Data. Vaccines 2022, 10, 744. https://doi.org/10.3390/vaccines10050744
Lee CW, Sa S, Hong M, Kim J, Shim SR, Han HW. Adverse Events and Safety Profile of the COVID-19 Vaccines in Adolescents: Safety Monitoring for Adverse Events Using Real-World Data. Vaccines. 2022; 10(5):744. https://doi.org/10.3390/vaccines10050744
Chicago/Turabian StyleLee, Chae Won, Soonok Sa, Myunghee Hong, Jihyun Kim, Sung Ryul Shim, and Hyun Wook Han. 2022. "Adverse Events and Safety Profile of the COVID-19 Vaccines in Adolescents: Safety Monitoring for Adverse Events Using Real-World Data" Vaccines 10, no. 5: 744. https://doi.org/10.3390/vaccines10050744