
Severe Acute Myocarditis after the Third (Booster) Dose of mRNA COVID-19 Vaccination

 ,
,
Abstract
:1. Patient Presentation
2. Hospital Course
3. Follow-Up Course
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mevorach, D.; Anis, E.; Cedar, N.; Bromberg, M.; Haas, E.J.; Nadir, E.; Olsha-Castell, S.; Arad, D.; Hasin, T.; Levi, N.; et al. Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 2140–2149. [Google Scholar] [CrossRef] [PubMed]
- Witberg, G.; Barda, N.; Hoss, S.; Richter, I.; Wiessman, M.; Aviv, Y.; Grinberg, T.; Auster, O.; Dagan, N.; Balicer, R.D.; et al. Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. N. Engl. J. Med. 2021, 385, 2132–2139. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Jenista, E.R.; Wendell, D.C.; Azevedo, C.F.; Campbell, M.J.; Darty, S.N.; Parker, M.A.; Kim, R.J. Patients with Acute Myocarditis Following mRNA COVID-19 Vaccination. JAMA Cardiol. 2021, 6, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Diaz, G.A.; Parsons, G.T.; Gering, S.K.; Meier, A.R.; Hutchinson, I.V.; Robicsek, A. Myocarditis and Pericarditis after Vaccination for COVID-19. JAMA 2021, 326, 1210–1212. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, J.; Ryan, M.; Engler, R.; Hoffman, D.; McClenathan, B.; Collins, L.; Loran, D.; Hrncir, D.; Herring, K.; Platzer, M.; et al. Myocarditis Following Immunization with mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiol. 2021, 6, 1202. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Corona in Israel-Snapshot, Israeli Ministry of Health. Available online: https://datadashboard.health.gov.il/COVID-19/general (accessed on 1 March 2022).
- Hajjo, R.; Sabbah, D.A.; Bardaweel, S.K.; Tropsha, A. Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients. Vaccines 2021, 9, 1186. [Google Scholar] [CrossRef] [PubMed]
- Heymans, S.; Cooper, L.T. Myocarditis after COVID-19 mRNA Vaccination: Clinical Observations and Potential Mechanisms. Nat. Rev. Cardiol. 2022, 19, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Tartof, S.Y.; Qian, L.; Hong, V.; Wei, R.; Nadjafi, R.F.; Fischer, H.; Li, Z.; Shaw, S.F.; Caparosa, S.L.; Nau, C.L.; et al. Obesity and Mortality among Patients Diagnosed With COVID-19: Results from an Integrated Health Care Organization. Ann. Intern. Med. 2020, 173, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Kipshidze, N.; Kipshidze, N.; Fried, M. COVID-19 Vaccines: Special Considerations for the Obese Population. Obes. Surg. 2021, 31, 3854–3856. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Balena, A.; Tuccinardi, D.; Tozzi, R.; Risi, R.; Masi, D.; Caputi, A.; Rossetti, R.; Spoltore, M.E.; Filippi, V.; et al. Central obesity, smoking habit, and hypertension are associated with lower antibody titres in response to COVID-19 mRNA vaccine. Diabetes Metab. Res. Rev. 2022, 38, e3465. [Google Scholar] [CrossRef] [PubMed]
- Iguacel, I.; Maldonado, A.L.; Ruiz-Cabello, A.L.; Casaus, M.; Moreno, L.A.; Martínez-Jarreta, B. Association between COVID-19 Vaccine Side Effects and Body Mass Index in Spain. Vaccines 2021, 9, 1321. [Google Scholar] [CrossRef] [PubMed]
- Vermes, E.; Carbone, I.; Friedrich, M.G.; Merchant, N. Patterns of myocardial late enhancement: Typical and atypical features. Arch. Cardiovasc. Dis. 2012, 105, 300–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehrlich, P.; Klingel, K.; Ohlmann-Knafo, S.; Hüttinger, S.; Sood, N.; Pickuth, D.; Kindermann, M. Biopsy-proven lymphocytic myocarditis following first mRNA COVID-19 vaccination in a 40-year-old male: Case report. Clin. Res. Cardiol. 2021, 110, 1855–1859. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.R.; Tashjian, R.; Duncanson, E. Autopsy Histopathologic Cardiac Findings in Two Adolescents Following the Second COVID-19 Vaccine Dose. Arch. Pathol. Lab. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Lee, S.; Seo, J.-W.; Kim, M.; Jeon, Y.H.; Park, J.H.; Lee, J.K.; Yeo, N.S. Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings. J. Korean Med. Sci. 2021, 36, e286. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.K.; Lavine, K.J.; Lin, C.-Y. Myocarditis after Covid-19 mRNA Vaccination. N. Engl. J. Med. 2021, 385, 1332–1334. [Google Scholar] [CrossRef] [PubMed]
- Truong, D.T.; Dionne, A.; Muniz, J.C.; McHugh, K.E.; Portman, M.A.; Lambert, L.M.; Thacker, D.; Elias, M.D.; Li, J.S.; Toro-Salazar, O.H.; et al. Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults: Suspected Myocarditis after COVID-19 Vaccination. Circulation 2022, 145, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis with COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A: Clinical Characteristics and Laboratory Findings General Characteristics | |
|---|---|
| Age | 43 |
| Sex | Female |
| Race | White, Arab Israeli |
| Medical history | Obesity |
| Medications prior to illness | None |
| Admission vital signs | |
| Heart rate (bpm) | 116 |
| Respiratory rate (per minute) | 20 |
| Blood pressure (mmHg) | 102/86 |
| Temperature (°C) | 37.3 |
| Pulse oximeter saturation (%) | 96 |
| Body Mass Index (kg/m2) | 33.5 |
| Laboratory findings | |
| Admission Laboratories | |
| WBC (×103/µL) | 8.8 |
| Neutrophils (%) | 69.1 |
| Lymphocytes (%) | 21.9 |
| Eosinophils (%) | 2.5 |
| Hemoglobin (g/dL) | 12.8 |
| Hematocrit (%) | 40.3 |
| Platelets (×103/µL) | 315 |
| Sodium (mmol/L) | 136 |
| Potassium (mmol/L) | 3.6 |
| BUN (mg/dL) | 21 |
| Creatinine (mg/dL) | 0.8 |
| AST (U/L) | 42 (reference: 8–48 ng/L) |
| ALT (U/L) | 51 (reference: 7–55 ng/L) |
| Alkaline phosphatase (U/L) | 57 (reference: 40–129 ng/L) |
| Total bilirubin (mg/dL) | 7.5 (reference: 0.1–1.2 mg/dL) |
| Troponin I (high-sensitive) (ng/L) | 630 (reference: 0–34 ng/L) |
| Creatinine phosphokinase (U/L) | 97 (reference: 26–192 U/L) |
| Other labs | |
| Peak troponin I (high-sensitive) (ng/L) | 2082 (reference: 0–34 ng/L) |
| Lactate | 2.2 (reference: 0.5–2.2 mmol/L) |
| TSH (mIU/L) | 2.1 (reference: 0.3–4.2 mIU/L) |
| C-reactive protein (mg/dL) | 6.8 (reference: <0.5 mg/dL) |
| Ferritin (ng/mL) | 105 (reference: 10–291 ng/mL) |
| NT-proBNP (pg/mL) | 257 (reference: 0–125 pg/mL) |
| PT (%) | 100 (reference: 63.8–127.7) |
| aPTT (sec) | 28.7 (reference: 22.4–36.3) |
| INR | 1.0 (reference: 0.9–1.2) |
| D-dimer (mg/L) | 1.3 (reference: 0–0.4 mg/L) |
| Autoimmune evaluation | |
| p-ANCA | Negative |
| c-ANCA | Negative |
| ANA | Negative |
| IgA (mg/dL) | 190.8 (reference: 70–400 mg/dL) |
| IgM (mg/dL) | 160.8 (reference: 40–230 mg/dL) |
| IgG (mg/dL) | 596 (reference: 700–1700 mg/dL) |
| C3 (mg/dL) | 207.6 (reference: 90–180 mg/dL) |
| C4 (mg/dL) | 41.8 (reference: 10–40 mg/dL) |
| Anti-Titin autoantibodies | Negative |
| Viral evaluation in nasopharyngeal swab specimens (PCR) | |
| SARS-CoV-2 PCR | Negative |
| Respiratory viral panel (PCR): | |
| Adenovirus | Negative |
| Human Metapneumovirus | Negative |
| Rhinovirus/Enterovirus | Negative |
| Influenza virus type A (non H1N1) | Negative |
| Influenza virus type A (H1N1) | Negative |
| Influenza virus type B | Negative |
| Parainfluenza virus types 1/2/3 | Negative |
| Respiratory Syncytial Virus (RSV) | Negative |
| Viral serology (antibodies in serum) | |
| COVID-19 (IgM) * | Negative |
| COVID-19 (Anti S IgG) * | Positive (14,135 AU/mL), (reference: <50 AU/mL) |
| COVID-19 (Anti N IgG) * | Negative |
| Adenovirus | Negative |
| CMV | Negative |
| EBV | Negative |
| Enterovirus | Negative |
| HHV-6 | Negative |
| HSV-1 | Negative |
| HSV-2 | Negative |
| Myocardial tissue specimens (PCR) | |
| Enterovirus | Negative |
| Adenovirus | Negative |
| Human Metapneumovirus | Negative |
| Parvovirus | Negative |
| HHV-6 | Negative |
| Influenza virus type A (non H1N1) | Negative |
| Influenza virus type A (H1N1) | Negative |
| Influenza virus type B | Negative |
| Parainfluenza virus types 1/2/3 | Negative |
| Respiratory Syncytial Virus (RSV) | Negative |
| SARS-Cov-2 | Negative |
| B: Cardiac Diagnostic Testing and Medical Treatment | |
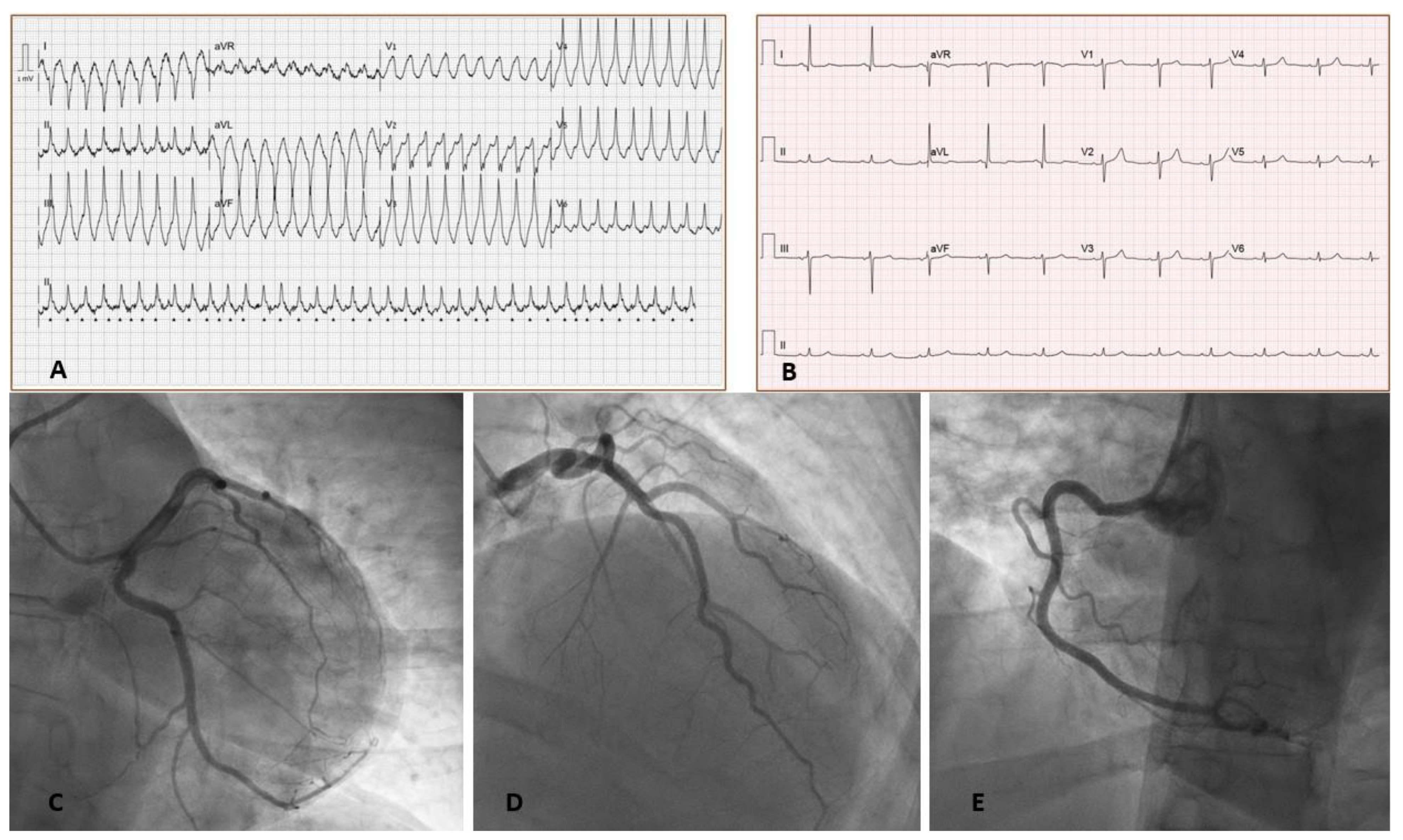
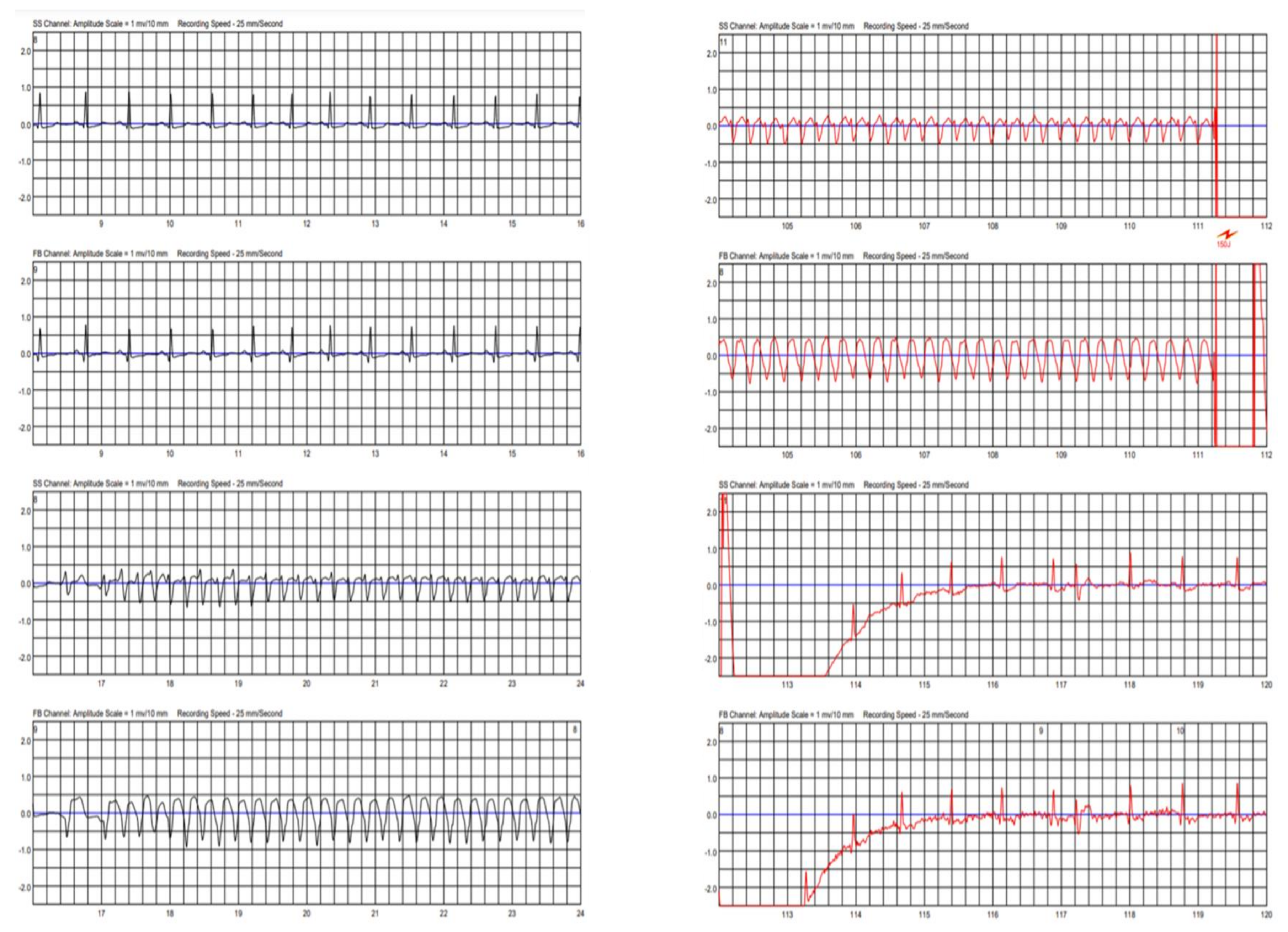
| ECG | Initial presentation: Rapid monomorphic ventricular tachycardia with ventricular rate of 120 bpm. |
| After cardioversion: Normal sinus rhythm, ventricular rate of 64 bpm, normal axis, no ST-T or PR changes, no QT prolongation, and normal QRS duration. | |
| Transthoracic echocardiogram | Mildly to moderately decreased LV systolic function, EF 40–45%, mildly increased LV size (mid LV diameter of 5.8 cm), normal RV size and function, normal RA and LA size, mild MR and TR, normal IVC size (<2.1 cm), no pericardial effusion |
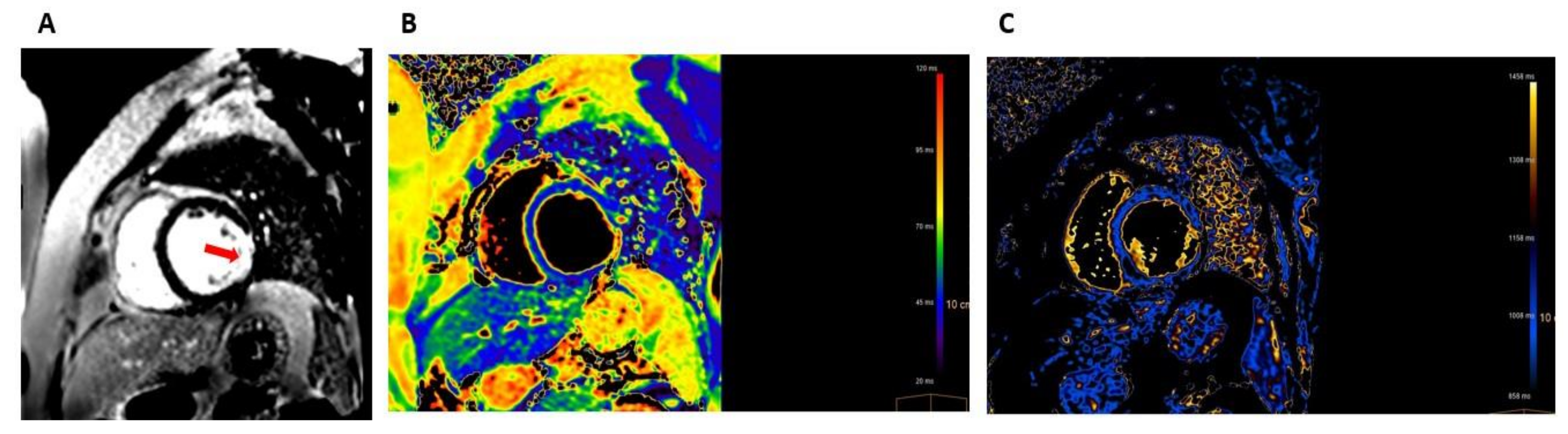
| Cardiac MRI | Mildly to moderately reduced systolic function, hypokinesia of the lateral wall and akinesia of an aneurysmatic inferolateral wall, myocardial edema in the inferolateral wall, subendocardial and transmural LGE in the lateral wall and inferolateral wall. |
| Coronary angiography | Right dominant system |
| No angiographic evidence of CAD | |
| Hemodynamics/right heart catheterization | RAP 4 mmHg |
| RVP 30/5 mmHg | |
| PAP 30/15 mmHg, mPAP 20 mmHg | |
| PCWP 14 mmHg | |
| AOP 122/70 mmHg | |
| TPG 6 | |
| PVR 1.0 | |
| CO 6.0 L/min (per Fick) | |
| CI 3.1 L/min/m2 (per Fick) | |
| Medications received during illness/hospitalization | Prednisone |
| Omeprazole | |
| Bisoprolol | |
| Ramipril | |
| Sulfamethoxazole/Trimethoprim | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mengesha, B.; Asenov, A.G.; Hirsh-Raccah, B.; Amir, O.; Pappo, O.; Asleh, R. Severe Acute Myocarditis after the Third (Booster) Dose of mRNA COVID-19 Vaccination. Vaccines 2022, 10, 575. https://doi.org/10.3390/vaccines10040575
Mengesha B, Asenov AG, Hirsh-Raccah B, Amir O, Pappo O, Asleh R. Severe Acute Myocarditis after the Third (Booster) Dose of mRNA COVID-19 Vaccination. Vaccines. 2022; 10(4):575. https://doi.org/10.3390/vaccines10040575
Chicago/Turabian StyleMengesha, Bethlehem, Asen G. Asenov, Bruria Hirsh-Raccah, Offer Amir, Orit Pappo, and Rabea Asleh. 2022. "Severe Acute Myocarditis after the Third (Booster) Dose of mRNA COVID-19 Vaccination" Vaccines 10, no. 4: 575. https://doi.org/10.3390/vaccines10040575