
Availability of the HPV Vaccine in Regional Pharmacies and Provider Perceptions Regarding HPV Vaccination in the Pharmacy Setting

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Pharmacy Data Collection
2.2. Family Medicine and Obstetrics–Gynecology Provider Surveys
2.3. Statistical Analysis
3. Results
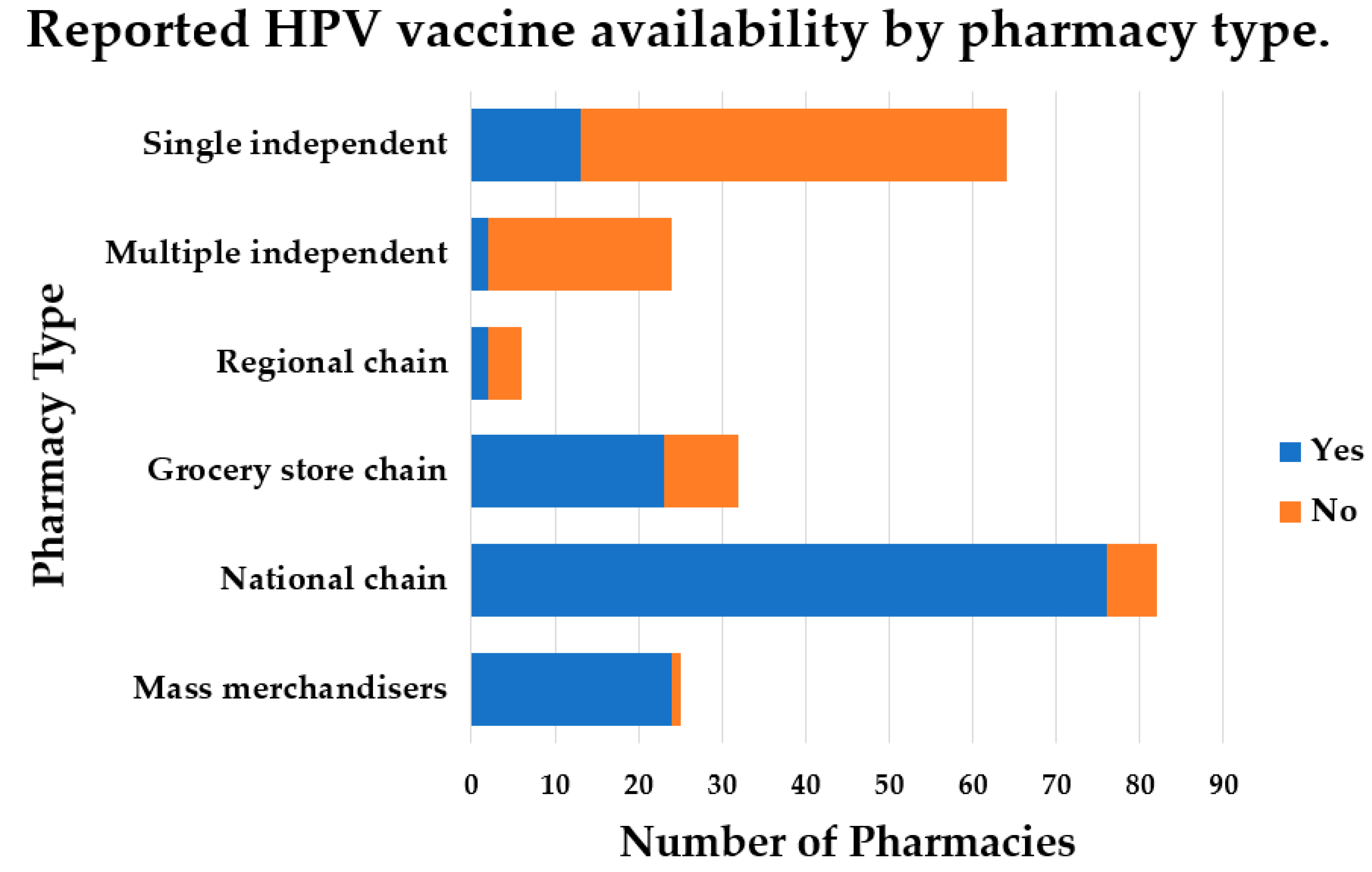
3.1. Pharmacy Data Collection
3.2. Family Medicine and Obstetrics–Gynecology Providers
3.2.1. Provider Characteristics
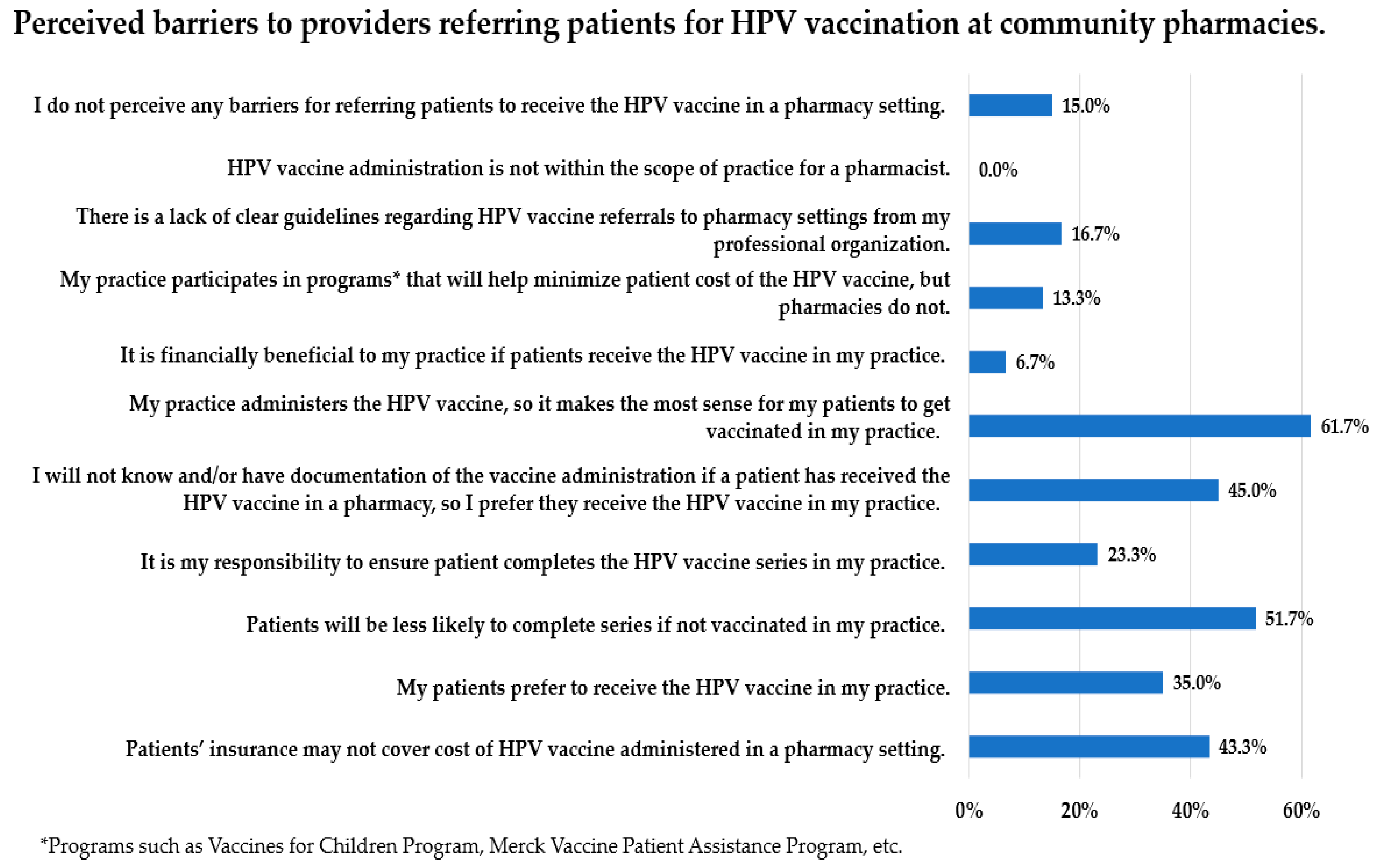
3.2.2. HPV Vaccination Availability and Referral Practices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Senkomago, V.; Henley, S.J.; Thomas, C.C.; Mix, J.M.; Markowitz, L.E.; Saraiya, M. Human papillomavirus-attributable cancers-united states, 2012–2016. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 724–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dyne, E.A.; Henley, S.J.; Saraiya, M.; Thomas, C.C.; Markowitz, L.E.; Benard, V.B. Trends in human papillomavirus-associated cancers-united states, 1999–2015. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 918–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viens, L.J.; Henley, S.J.; Watson, M.; Markowitz, L.E.; Thomas, C.C.; Thompson, T.D.; Razzaghi, H.; Saraiya, M. Human papillomavirus-associated cancers-united states, 2008–2012. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Pingali, C.; Yankey, D.; Elam-Evans, L.D.; Markowitz, L.E.; Williams, C.L.; Fredua, B.; McNamara, L.A.; Stokley, S.; Singleton, J.A. National, regional, state, and selected local area vaccination coverage among adolescents aged 13–17 years-united states, 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.J.; Hung, M.C.; Srivastav, A.; Grohskopf, L.A.; Kobayashi, M.; Harris, A.M.; Dooling, K.L.; Markowitz, L.E.; Rodriguez-Lainz, A.; Williams, W.W. Surveillance of vaccination coverage among adult populations -united states, 2018. MMWR Surveill. Summ. 2021, 70, 1–26. [Google Scholar] [CrossRef]
- Damgacioglu, H.; Sonawane, K.; Zhu, Y.; Li, R.; Balasubramanian, B.A.; Lairson, D.R.; Giuliano, A.R.; Deshmukh, A.A. Oropharyngeal cancer incidence and mortality trends in all 50 states in the US, 2001–2017. JAMA Otolaryngol. Head Neck Surg. 2021, 148, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; McGrath, C.J.; Berenson, A.B. Geographic variation in human papillomavirus vaccination uptake among 13–17 year old adolescent girls in the united states. Vaccine 2014, 32, 2394–2398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahnd, W.E.; Rodriguez, C.; Jenkins, W.D. Rural-urban differences in human papillomavirus-associated cancer trends and rates. J. Rural Health 2019, 35, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Hpv Vaccination for Cancer Prevention: Progress, Opportunities, and a Renewed Call to Action. Available online: https://prescancerpanel.cancer.gov/report/hpvupdate/pdf/PresCancerPanel_HPVUpdate_Nov2018.pdf (accessed on 1 December 2021).
- National Vaccine Advisory Committee. Overcoming barriers to low hpv vaccine uptake in the united states: Recommendations from the national vaccine advisory committee: Approved by the national vaccine advisory committee on June 9, 2015. Public Health Rep. 2016, 131, 17–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cartmell, K.B.; Young-Pierce, J.; McGue, S.; Alberg, A.J.; Luque, J.S.; Zubizarreta, M.; Brandt, H.M. Barriers, facilitators, and potential strategies for increasing hpv vaccination: A statewide assessment to inform action. Papillomavirus Res. 2018, 5, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Face-to-Face with Community Pharmacies. Available online: https://www.nacds.org/pdfs/about/rximpact-leavebehind.pdf (accessed on 1 December 2021).
- Westrick, S.C.; Patterson, B.J.; Kader, M.S.; Rashid, S.; Buck, P.O.; Rothholz, M.C. National survey of pharmacy-based immunization services. Vaccine 2018, 36, 5657–5664. [Google Scholar] [CrossRef] [PubMed]
- Pharmacist Administered Vaccines, Updated July 2021, Based on Apha/Naspa Survey of State Iz Laws/Rules. Available online: https://aphanet.pharmacist.com/sites/default/files/files/practice/07-2020/pharmacist-administered-vaccines-june-2020.pdf (accessed on 15 September 2021).
- Campos-Outcalt, D.; Jeffcott-Pera, M.; Carter-Smith, P.; Schoof, B.K.; Young, H.F. Vaccines provided by family physicians. Ann. Fam. Med. 2010, 8, 507–510. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, S.T.; Riley, L.E.; Lindley, M.C.; Allison, M.A.; Crane, L.A.; Hurley, L.P.; Beaty, B.L.; Brtnikova, M.; Collins, M.; Albert, A.P.; et al. Vaccination practices among obstetrician/gynecologists for non-pregnant patients. Am. J. Prev. Med. 2019, 56, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Developing an Immunization Referral System. Available online: https://www.nacds.org/ceo/2018/0628/2018-Immun-Referral-TipSheet.pdf (accessed on 1 December 2021).
- Federal Office of Rural Health Policy (Forhp) Data Files. Available online: https://www.hrsa.gov/rural-health/about-us/definition/datafiles.html (accessed on 1 September 2021).
- Hurley, L.P.; Bridges, C.B.; Harpaz, R.; Allison, M.A.; O’Leary, S.T.; Crane, L.A.; Brtnikova, M.; Stokley, S.; Beaty, B.L.; Jimenez-Zambrano, A.; et al. U.S. Physicians’ perspective of adult vaccine delivery. Ann. Intern. Med. 2014, 160, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hastings, T.J.; Hohmann, L.A.; McFarland, S.J.; Teeter, B.S.; Westrick, S.C. Pharmacists’ attitudes and perceived barriers to human papillomavirus (hpv) vaccination services. Pharmacy 2017, 5, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oyedeji, O.; Maples, J.M.; Gregory, S.; Chamberlin, S.M.; Gatwood, J.D.; Wilson, A.Q.; Zite, N.B.; Kilgore, L.C. Pharmacists’ perceived barriers to human papillomavirus (hpv) vaccination: A systematic literature review. Vaccines 2021, 9, 1360. [Google Scholar] [CrossRef] [PubMed]
- Ryan, G.; Daly, E.; Askelson, N.; Pieper, F.; Seegmiller, L.; Allred, T. Exploring opportunities to leverage pharmacists in rural areas to promote administration of human papillomavirus vaccine. Prev. Chronic. Dis. 2020, 17, E23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Just How Rural or Urban are Tennessee’s 95 Counties? Finding a Measure for Policy Makers. Tennessee Advisory Commission on Intergovernmental Relations Staff Report. Available online: https://www.tn.gov/content/dam/tn/tacir/documents/2016JustHowRuralOrUrban.pdf (accessed on 16 February 2022).
- Welch, A.C.; Ferreri, S.P.; Blalock, S.J.; Caiola, S.M. North carolina family practice physicians’ perceptions of pharmacists as vaccinators. J. Am. Pharm. Assoc. 2005, 45, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Doucette, W.R.; Kent, K.; Seegmiller, L.; McDonough, R.P.; Evans, W. Feasibility of a coordinated human papillomavirus (hpv) vaccination program between a medical clinic and a community pharmacy. Pharmacy 2019, 7, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frederick, K.D.; Gatwood, J.D.; Atchley, D.R.; Rein, L.J.; Ali, S.G.; Brookhart, A.L.; Crain, J.; Hagemann, T.M.; Ramachandran, S.; Chiu, C.Y.; et al. Exploring the early phase of implementation of a vaccine-based clinical decision support system in the community pharmacy. J. Am. Pharm. Assoc. 2020, 60, e292–e300. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Pharmacies (n = 233) | |
|---|---|
| Pharmacy Type | |
| Single independent | 64 (27.5%) |
| Multiple independent | 24 (10.3%) |
| Grocery store chain | 32 (13.7%) |
| Mass merchandiser | 25 (10.7%) |
| National chain | 82 (35.2%) |
| Regional chain | 6 (2.6%) |
| Geographic location | |
| Nonrural | 171 (73.4%) |
| Rural | 62 (26.6%) |
| HPV Vaccine Availability | |
| No | 93 (39.9%) |
| Yes | 140 (60.1%) |
| Pharmacies with HPV Vaccine Availability (n = 140) | |
| Stock HPV Vaccine | |
| No | 46 (32.9%) |
| Yes | 94 (67.1%) |
| Appointment Needed | N = 140 |
| No | 126 (90.0%) |
| Yes | 14 (10.0%) |
| Length of Time Needed for Desired HPV Vaccination | |
| Same Day | 107 (76.4%) |
| Within 24 h | 9 (6.4%) |
| 24–48 h | 6 (4.3%) |
| More than 48 h | 11 (7.9%) |
| Other | 7 (5.0%) |
| Not Willing at All | Not Really Willing | Somewhat Willing | Willing | Very Willing | |
|---|---|---|---|---|---|
| Patient Age Group | % (n) | % (n) | % (n) | % (n) | % (n) |
| 11–18 years | 0 (0) | 0 (0) | 5.2 (3) | 25.9 (15) | 68.9 (40) |
| 19–26 years | 0 (0) | 0 (0) | 8.3 (5) | 25.0 (15) | 66.7 (40) |
| 27–49 years | 0 (0) | 0 (0) | 10.0 (6) | 23.3 (14) | 66.7 (40) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maples, J.M.; Zite, N.B.; Oyedeji, O.; Chamberlin, S.M.; Mastronardi, A.M.; Gregory, S.; Gatwood, J.D.; Hohmeier, K.C.; Booker, M.E.; Perry, J.D.; et al. Availability of the HPV Vaccine in Regional Pharmacies and Provider Perceptions Regarding HPV Vaccination in the Pharmacy Setting. Vaccines 2022, 10, 351. https://doi.org/10.3390/vaccines10030351
Maples JM, Zite NB, Oyedeji O, Chamberlin SM, Mastronardi AM, Gregory S, Gatwood JD, Hohmeier KC, Booker ME, Perry JD, et al. Availability of the HPV Vaccine in Regional Pharmacies and Provider Perceptions Regarding HPV Vaccination in the Pharmacy Setting. Vaccines. 2022; 10(3):351. https://doi.org/10.3390/vaccines10030351
Chicago/Turabian StyleMaples, Jill M., Nikki B. Zite, Oluwafemifola Oyedeji, Shauntá M. Chamberlin, Alicia M. Mastronardi, Samantha Gregory, Justin D. Gatwood, Kenneth C. Hohmeier, Mary E. Booker, Jamie D. Perry, and et al. 2022. "Availability of the HPV Vaccine in Regional Pharmacies and Provider Perceptions Regarding HPV Vaccination in the Pharmacy Setting" Vaccines 10, no. 3: 351. https://doi.org/10.3390/vaccines10030351