
Long-Term Effects of Human Papillomavirus Vaccination in Clinical Trials and Real-World Data: A Systematic Review

 , , , , ,
, , , , ,
Abstract
:1. Introduction
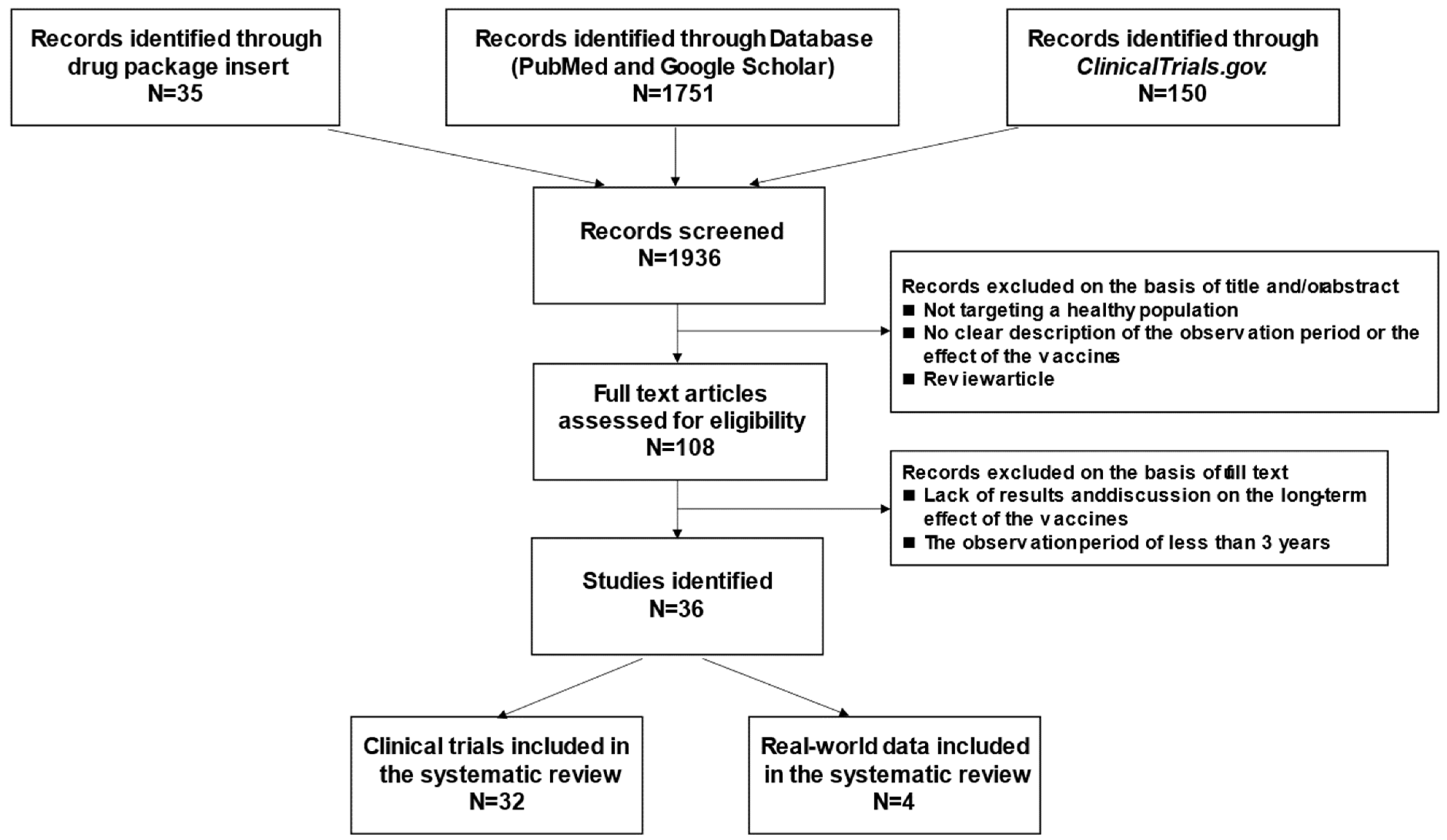
2. Methods
3. Available Vaccines
4. Long-Term Efficacy: Clinical Trials
4.1. Bivalent Vaccine
4.1.1. Young Women
4.1.2. Adult Women
4.1.3. Men
4.2. 4-Valent Vaccine
4.2.1. Young Women
4.2.2. Adult Women
4.2.3. Men
4.3. 9-Valent Vaccine
4.3.1. Young Women
4.3.2. Adult Women
4.3.3. Men
5. Long-Term Effectiveness: Real-World Data
5.1. Young Women
5.2. Adult Women
6. Long-Term Persistence of HPV Vaccine-Induced Seropositivity
6.1. Bivalent Vaccine
6.2. 4-Valent Vaccine
6.3. 9-Valent Vaccine
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tognon, M.; Tagliapietra, A.; Magagnoli, F.; Mazziotta, C.; Otòn-Gonzalez, L.; Lanzillotti, C.; Vesce, F.; Contini, C.; Rotondo, J.C.; Martini, F. Investigation on spontaneous abortion and human papillomavirus infection. Vaccines 2020, 8, 473. [Google Scholar] [CrossRef]
- Sarkola, M.E.; Grénman, S.E.; Rintala, M.A.; Syrjänen, K.J.; Syrjänen, S.M. Human papillomavirus in the placenta and umbilical cord blood. Acta Obs. Gynecol Scand. 2008, 87, 1181–1188. [Google Scholar] [CrossRef]
- Dilley, S.; Miller, K.M.; Huh, W.K. Human papillomavirus vaccination: Ongoing challenges and future directions. Gynecol. Oncol. 2020, 156, 498–502. [Google Scholar] [CrossRef]
- Szymonowicz, K.A.; Chen, J. Biological and clinical aspects of HPV-related cancers. Cancer Biol. Med. 2020, 17, 864–878. [Google Scholar] [CrossRef]
- Brianti, P.; De Flammineis, E.; Mercuri, S.R. Review of HPV-related diseases and cancers. New Microbiol. 2017, 40, 80–85. [Google Scholar]
- Centers for Disease Control and Prevention. Human Papillomavirus (HPV). Reasons to Get HPV Vaccine. Available online: https://www.cdc.gov/hpv/parents/vaccine/six-reasons.html#:~:text=HPV%20vaccination%20is%20cancer%20prevention,attendance%20for%20a%20baseball%20game (accessed on 30 September 2021).
- Paavonen, J.; Naud, P.; Salmerón, J.; Wheeler, C.M.; Chow, S.-N.; Apter, D.; Kitchener, H.; Castellsague, X.; Teixeira, J.C.; Skinner, S.R.; et al. Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): Final analysis of a double-blind, randomised study in young women. Lancet 2009, 374, 301–314. [Google Scholar] [CrossRef]
- Kjaer, S.K.; Sigurdsson, K.; Iversen, O.E.; Hernandez-Avila, M.; Wheeler, C.M.; Perez, G.; Brown, D.R.; Koutsky, L.A.; Tay, E.H.; García, P.; et al. A pooled analysis of continued prophylactic efficacy of quadrivalent human papillomavirus (Types 6/11/16/18) vaccine against high-grade cervical and external genital lesions. Cancer Prev. Res. 2009, 2, 868–878. [Google Scholar] [CrossRef] [Green Version]
- Brotherton, J.M.; Fridman, M.; May, C.L.; Chappell, G.; Saville, A.M.; Gertig, D.M. Early effect of the HPV vaccination programme on cervical abnormalities in Victoria, Australia: An ecological study. Lancet 2011, 377, 2085–2092. [Google Scholar] [CrossRef]
- Markowitz, L.E.; Hariri, S.; Lin, C.; Dunne, E.F.; Steinau, M.; McQuillan, G.; Unger, E.R. Reduction in human papillomavirus (HPV) prevalence among young women following HPV vaccine introduction in the United States, national health and nutrition examination surveys. 2003–2010. J. Infect. Dis. 2013, 208, 385–393. [Google Scholar] [CrossRef] [Green Version]
- Tabrizi, S.N.; Brotherton, J.M.; Kaldor, J.M.; Skinner, S.R.; Liu, B.; Bateson, D.; McNamee, K.; Garefalakis, M.; Phillips, S.; Cummins, E.; et al. Assessment of herd immunity and cross-protection after a human papillomavirus vaccination programme in Australia: A repeat cross-sectional study. Lancet Infect. Dis. 2014, 14, 958–966. [Google Scholar] [CrossRef]
- Pollock, K.G.; Kavanagh, K.; Potts, A.; Love, J.; Cuschieri, K.; Cubie, H.; Robertson, C.; Cruickshank, M.; Palmer, T.J.; Nicoll, S.; et al. Reduction of low- and high-grade cervical abnormalities associated with high uptake of the HPV bivalent vaccine in Scotland. Br. J. Cancer 2014, 111, 1824–1830. [Google Scholar] [CrossRef] [Green Version]
- Garland, S.M.; Kjaer, S.K.; Muñoz, N.; Block, S.L.; Brown, D.R.; DiNubile, M.J.; Lindsay, B.R.; Kuter, B.J.; Perez, G.; Dominiak-Felden, G.; et al. Impact and effectiveness of the quadrivalent human papillomavirus vaccine: A systematic review of 10 years of real-world experience. Clin. Infect. Dis. 2016, 63, 519–527. [Google Scholar] [CrossRef]
- Baldur-Felskov, B.; Dehlendorff, C.; Munk, C.; Kjaer, S.K. Early impact of human papillomavirus vaccination on cervical neoplasia—Nationwide follow-up of young Danish women. J. Natl. Cancer. Inst. 2014, 106, djt460. [Google Scholar] [CrossRef] [Green Version]
- Oliver, S.E.; Unger, E.R.; Lewis, R.; McDaniel, D.; Gargano, J.W.; Steinau, M.; Markowitz, L.E. Prevalence of human papillomavirus among females after vaccine introduction-national health and nutrition examination survey, United States, 2003–2014. J. Infect. Dis. 2017, 216, 594–603. [Google Scholar] [CrossRef]
- Luostarinen, T.; Apter, D.; Dillner, J.; Eriksson, T.; Harjula, K.; Natunen, K.; Paavonen, J.; Pukkala, E.; Lehtinen, M. Vaccination protects against invasive HPV-associated cancers. Int. J. Cancer 2018, 142, 2186–2187. [Google Scholar] [CrossRef] [Green Version]
- Lei, J.; Ploner, A.; Elfström, K.M.; Wang, J.; Roth, A.; Fang, F.; Sundström, K.; Dillner, J.; Sparén, P. HPV vaccination and the risk of invasive cervical cancer. New Engl. J. Med. 2020, 383, 1340–1348. [Google Scholar] [CrossRef]
- Kjaer, S.K.; Dehlendorff, C.; Belmonte, F.; Baandrup, L. Real-world effectiveness of human papillomavirus vaccination against cervical cancer. J. Natl. Cancer Inst. 2021, 113, 1329–1335. [Google Scholar] [CrossRef]
- Falcaro, M.; Castañon, A.; Ndlela, B.; Checchi, M.; Soldan, K.; Lopez-Bernal, J.; Elliss-Brookes, L.; Sasieni, P. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: A register-based observational study. Lancet 2021, 398, 2084–2092. [Google Scholar] [CrossRef]
- WHOEa. Human papillomavirus vaccines: WHO position paper, May 2017—Recommendations. Vaccine 2017, 35, 5753–5755. [Google Scholar] [CrossRef]
- WHO Immunization, Vaccines and Biologicals. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals (accessed on 20 August 2021).
- Schiller, J.T.; Castellsagué, X.; Garland, S.M. A review of clinical trials of human papillomavirus prophylactic vaccines. Vaccine 2012, 30, F123–F138. [Google Scholar] [CrossRef] [Green Version]
- De Vincenzo, R.; Conte, C.; Ricci, C.; Scambia, G.; Capelli, G. Long-term efficacy and safety of human papillomavirus vaccination. Int. J. Women’s Health 2014, 6, 999–1010. [Google Scholar] [CrossRef] [Green Version]
- Jacot-Guillarmod, M.; Pasquier, J.; Greub, G.; Bongiovanni, M.; Achtari, C.; Sahli, R. Impact of HPV vaccination with Gardasil® in Switzerland. BMC Infect. Dis. 2017, 17, 790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GlaxoSmithKline Biologicals. Cervarix. Available online: https://gskpro.com/content/dam/global/hcpportal/ja_JP/products-info/cervarix/cervarix.pdf (accessed on 31 August 2021).
- GlaxoSmithKline Biologicals. Gardasil. Available online: https://pins.japic.or.jp/pdf/newPINS/00059715.pdf (accessed on 31 August 2021).
- GlaxoSmithKline Biologicals. Gardasil9. Available online: https://www.msdconnect.jp/static/mcijapan/images/pi_silgard9_injnsr.pdf (accessed on 31 August 2021).
- Harper, D.M.; Franco, E.L.; Wheeler, C.; Ferris, D.G.; Jenkins, D.; Schuind, A.; Zahaf, T.; Innis, B.; Naud, P.; De Carvalho, N.S.; et al. Efficacy of a bivalent L1 virus-like particle vaccine in prevention of infection with human papillomavirus types 16 and 18 in young women: A randomised controlled trial. Lancet 2004, 364, 1757–1765. [Google Scholar] [CrossRef]
- Schwarz, T.F.; Spaczynski, M.; Schneider, A.; Wysocki, J.; Galaj, A.; Perona, P.; Poncelet, S.; Zahaf, T.; Hardt, K.; Descamps, D.; et al. Immunogenicity and tolerability of an HPV-16/18 AS04-adjuvanted prophylactic cervical cancer vaccine in women aged 15–55 years. Vaccine 2009, 27, 581–587. [Google Scholar] [CrossRef]
- Schwarz, T.F.; Spaczynski, M.; Schneider, A.; Wysocki, J.; Galaj, A.; Schulze, K.; Poncelet, S.M.; Catteau, G.; Thomas, F.; Descamps, D. Persistence of immune response to HPV-16/18 AS04-adjuvanted cervical cancer vaccine in women aged 15–55 years. Hum. Vaccin. 2011, 7, 958–965. [Google Scholar] [CrossRef]
- GlaxoSmithKline Vaccine HPV-007 Study Group. Sustained efficacy and immunogenicity of the human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine: Analysis of a randomised placebo-controlled trial up to 6.4 years. Lancet 2009, 374, 1975–1985. [Google Scholar] [CrossRef]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.; Fu, H.; et al. Efficacy, safety, and immunogenicity of the human papillomavirus 16/18 AS04-adjuvanted vaccine in women older than 25 years: 7-year follow-up of the phase 3, double-blind, randomised controlled VIVIANE study. Lancet Infect. Dis. 2016, 16, 1154–1168. [Google Scholar] [CrossRef]
- Roteli-Martins, C.M.; Naud, P.; De Borba, P.; Teixeira, J.C.; De Carvalho, N.S.; Zahaf, T.; Sanchez, N.; Geeraerts, B.; Descamps, D. Sustained immunogenicity and efficacy of the HPV-16/18 AS04-adjuvanted vaccine: Up to 8.4 years of follow-up. Hum. Vaccines Immunother. 2012, 8, 390–397. [Google Scholar] [CrossRef]
- Naud, P.S.; Roteli-Martins, C.M.; De Carvalho, N.S.; Teixeira, J.C.; de Borba, P.C.; Sanchez, N.; Zahaf, T.; Catteau, G.; Geeraerts, B.; Descamps, D. Sustained efficacy, immunogenicity, and safety of the HPV-16/18 AS04-adjuvanted vaccine: Final analysis of a long-term follow-up study up to 9.4 years post-vaccination. Hum. Vaccines Immunother. 2014, 10, 2147–2162. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, T.F.; Galaj, A.; Spaczynski, M.; Wysocki, J.; Kaufmann, A.M.; Poncelet, S.; Suryakiran, P.V.; Folschweiller, N.; Thomas, F.; Lin, L.; et al. Ten-year immune persistence and safety of the HPV-16/18 AS04-adjuvanted vaccine in females vaccinated at 15–55 years of age. Cancer Med. 2017, 6, 2723–2731. [Google Scholar] [CrossRef] [Green Version]
- Porras, C.; Tsang, S.H.; Herrero, R.; Guillén, D.; Darragh, T.M.; Stoler, M.H.; Hildesheim, A.; Wagner, S.; Boland, J.; Lowy, D.R.; et al. Efficacy of the bivalent HPV vaccine against HPV 16/18-associated precancer: Long-term follow-up results from the Costa Rica vaccine trial. Lancet Oncol. 2020, 21, 1643–1652. [Google Scholar] [CrossRef]
- Petäjä, T.; Keränen, H.; Karppa, T.; Kawa, A.; Lantela, S.; Siitari-Mattila, M.; Levänen, H.; Tocklin, T.; Godeaux, O.; Lehtinen, M.; et al. Immunogenicity and safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine in healthy boys aged 10–18 years. J. Adolesc. Health 2009, 44, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Kurosawa, M.; Sekine, M.; Yamaguchi, M.; Kudo, R.; Hanley, S.; Hara, M.; Adachi, S.; Ueda, Y.; Miyagi, E.; Ikeda, S.; et al. Long-term effectiveness of HPV vaccination against HPV infection in young Japanese women: Real-world data. Cancer Sci. 2022. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.M.; Hernandez-Avila, M.; Wheeler, C.M.; Perez, G.; Harper, D.M.; Leodolter, S.; Tang, G.W.; Ferris, D.G.; Steben, M.; Bryan, J.; et al. Quadrivalent vaccine against human papillomavirus to prevent anogenital diseases. N. Engl. J. Med. 2007, 356, 1928–1943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villa, L.L.; Ault, K.A.; Giuliano, A.R.; Costa, R.L.; Petta, C.A.; Andrade, R.P.; Brown, D.R.; Ferenczy, A.; Harper, D.M.; Koutsky, L.A.; et al. Immunologic responses following administration of a vaccine targeting human papillomavirus Types 6, 11, 16, and 18. Vaccine 2006, 24, 5571–5583. [Google Scholar] [CrossRef]
- Olsson, S.E.; Villa, L.L.; Costa, R.L.; Petta, C.A.; Andrade, R.P.; Malm, C.; Iversen, O.E.; Høye, J.; Steinwall, M.; Riis-Johannessen, G.; et al. Induction of immune memory following administration of a prophylactic quadrivalent human papillomavirus (HPV) types 6/11/16/18 L1 virus-like particle (VLP) vaccine. Vaccine 2007, 25, 4931–4939. [Google Scholar] [CrossRef]
- Luna, J.; Plata, M.; Gonzalez, M.; Correa, A.; Maldonado, I.; Nossa, C.; Radley, D.; Vuocolo, S.; Haupt, R.M.; Saah, A. Long-term follow-up observation of the safety, immunogenicity, and effectiveness of Gardasil™ in adult women. PLoS ONE 2013, 8, e83431. [Google Scholar] [CrossRef]
- Nygard, M. Long-term effectiveness and immunogenicity of GardasilTM in the Nordic countries. In Proceedings of the European Research Organisation On Genital Infection & Neoplasia Congress, Eurogin, Florence, Italy, 3–6 November 2013. [Google Scholar]
- Ferris, D.G.; Samakoses, R.; Block, S.L.; Lazcano-Ponce, E.; Restrepo, J.A.; Mehlsen, J.; Chatterjee, A.; Iversen, O.E.; Joshi, A.; Chu, J.; et al. 4-valent human papillomavirus (4vHPV) vaccine in preadolescents and adolescents after 10 years. Pediatrics 2017, 140. [Google Scholar] [CrossRef] [Green Version]
- Kjaer, S.K.; Nygård, M.; Sundström, K.; Dillner, J.; Tryggvadottir, L.; Munk, C.; Berger, S.; Enerly, E.; Hortlund, M.; Ágústsson, Á.I.; et al. Final analysis of a 14-year long-term follow-up study of the effectiveness and immunogenicity of the quadrivalent human papillomavirus vaccine in women from four nordic countries. EClinicalMedicine 2020, 23, 100401. [Google Scholar] [CrossRef]
- Palefsky, J.M.; Giuliano, A.R.; Goldstone, S.; Moreira, E.D., Jr.; Aranda, C.; Jessen, H.; Hillman, R.; Ferris, D.; Coutlee, F.; Stoler, M.; et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N. Engl. J. Med. 2011, 365, 1576–1585. [Google Scholar] [CrossRef]
- Goldstone, S.E.; Giuliano, A.R.; Palefsky, J.M.; Lazcano-Ponce, E.; Penny, M.E.; Cabello, R.E.; Moreira, E.D., Jr.; Baraldi, E.; Jessen, H.; Ferenczy, A.; et al. Efficacy, immunogenicity, and safety of a quadrivalent HPV vaccine in men: Results of an open-label, long-term extension of a randomised, placebo-controlled, phase 3 trial. Lancet Infect. Dis. 2021, in press. [Google Scholar] [CrossRef]
- Stephen, G. Long-term effectiveness and immunogenicity of quadrivalent HPV vaccine in young men: 10-year end-of study analysis. J. Clin. Oncol. 2018, 36, 1553. [Google Scholar]
- Machalek, D.A.; Garland, S.M.; Brotherton, J.; Bateson, D.; McNamee, K.; Stewart, M.; Rachel Skinner, S.; Liu, B.; Cornall, A.M.; Kaldor, J.M.; et al. Very low prevalence of vaccine human papillomavirus types among 18- to 35-year old Australian women 9 years following implementation of vaccination. J. Infect. Dis. 2018, 217, 1590–1600. [Google Scholar] [CrossRef] [PubMed]
- Thamsborg, L.H.; Napolitano, G.; Larsen, L.G.; Lynge, E. High-grade cervical lesions after vaccination against human papillomavirus: A Danish cohort study. Acta Obstet. Et. Gynecol. Scand. 2020, 99, 1290–1296. [Google Scholar] [CrossRef] [PubMed]
- Shilling, H.; Garland, S.M.; Atchison, S.; Cornall, A.M.; Brotherton, J.; Bateson, D.; McNamee, K.; Kaldor, J.M.; Hocking, J.S.; Chen, M.Y.; et al. Human papillomavirus prevalence and risk factors among Australian women 9–12 years after vaccine program introduction. Vaccine 2021, 39, 4856–4863. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Sternberg, Á.; Moreira, E.D.; Restrepo, J.A.; Lazcano-Ponce, E.; Cabello, R.; Silva, A.; Andrade, R.; Revollo, F.; Uscanga, S.; Victoria, A.; et al. Efficacy, immunogenicity, and safety of a 9-valent human papillomavirus vaccine in Latin American girls, boys, and young women. Papillomavirus. Res. 2018, 5, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Huh, W.K.; Joura, E.A.; Giuliano, A.R.; Iversen, O.E.; de Andrade, R.P.; Ault, K.A.; Bartholomew, D.; Cestero, R.M.; Fedrizzi, E.N.; Hirschberg, A.L.; et al. Final efficacy, immunogenicity, and safety analyses of a nine-valent human papillomavirus vaccine in women aged 16–26 years: A randomised, double-blind trial. Lancet 2017, 390, 2143–2159. [Google Scholar] [CrossRef]
- Olsson, S.E.; Restrepo, J.A.; Reina, J.C.; Pitisuttithum, P.; Ulied, A.; Varman, M.; Van Damme, P.; Moreira, E.D., Jr.; Ferris, D.; Block, S.; et al. Long-term immunogenicity, effectiveness, and safety of nine-valent human papillomavirus vaccine in girls and boys 9 to 15 years of age: Interim analysis after 8 years of follow-up. Papillomavirus Res. 2020, 10, 100203. [Google Scholar] [CrossRef]
- Kjaer, S.K.; Nygård, M.; Sundström, K.; Munk, C.; Berger, S.; Dzabic, M.; Fridrich, K.E.; Waldstrøm, M.; Sørbye, S.W.; Bautista, O.; et al. Long-term effectiveness of the nine-valent human papillomavirus vaccine in Scandinavian women: Interim analysis after 8 years of follow-up. Hum. Vaccin. Immunother. 2021, 17, 943–949. [Google Scholar] [CrossRef]
- Schwarz, T.F.; Spaczynski, M.; Schneider, A.; Wysocki, J.; Galaj, A.; Schulze, K. Persistence of immune response 7 years after administration of the HPV-16/18 as04-adjuvanted vaccine to women aged 15–55 years. In Proceedings of the Asia-Oceania Research Organization in Genital Infection and Neoplasia–2011 Interim Conference (AOGIN), Bali, Indonesia, 17–19 March 2011. [Google Scholar]
- Pedersen, C.; Petaja, T.; Strauss, G.; Rumke, H.C.; Poder, A.; Richardus, J.H.; Spiessens, B.; Descamps, D.; Hardt, K.; Lehtinen, M.; et al. Immunization of early adolescent females with human papillomavirus type 16 and 18 L1 virus-like particle vaccine containing AS04 adjuvant. J. Adolesc. Health 2007, 40, 564–571. [Google Scholar] [CrossRef]
- Castellsagué, X.; Muñoz, N.; Pitisuttithum, P.; Ferris, D.; Monsonego, J.; Ault, K.; Luna, J.; Myers, E.; Mallary, S.; Bautista, O.M.; et al. End-of-study safety, immunogenicity, and efficacy of quadrivalent HPV (types 6, 11, 16, 18) recombinant vaccine in adult women 24–45 years of age. Br. J. Cancer 2011, 105, 28–37. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Palefsky, J.M.; Goldstone, S.; Moreira, E.D., Jr.; Penny, M.E.; Aranda, C.; Vardas, E.; Moi, H.; Jessen, H.; Hillman, R.; et al. Efficacy of quadrivalent HPV vaccine against HPV Infection and disease in males. N. Engl. J. Med. 2011, 364, 401–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstone, S.E.; Jessen, H.; Palefsky, J.M.; Giuliano, A.R.; Moreira, E.D., Jr.; Vardas, E.; Aranda, C.; Hillman, R.J.; Ferris, D.G.; Coutlee, F.; et al. Quadrivalent HPV vaccine efficacy against disease related to vaccine and non-vaccine HPV types in males. Vaccine 2013, 31, 3849–3855. [Google Scholar] [CrossRef]
- Joura, E.A.; Giuliano, A.R.; Iversen, O.E.; Bouchard, C.; Mao, C.; Mehlsen, J.; Moreira, E.D., Jr.; Ngan, Y.; Petersen, L.K.; Lazcano-Ponce, E.; et al. A 9-valent HPV vaccine against infection and intraepithelial neoplasia in women. N. Engl. J. Med. 2015, 372, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Van Damme, P.; Olsson, S.E.; Block, S.; Castellsague, X.; Gray, G.E.; Herrera, T.; Huang, L.M.; Kim, D.S.; Pitisuttithum, P.; Chen, J.; et al. Immunogenicity and safety of a 9-Valent HPV vaccine. Pediatrics 2015, 136, e28–e39. [Google Scholar] [CrossRef] [Green Version]
- Luxembourg, A.; Moreira, E.D., Jr.; Samakoses, R.; Kim, K.H.; Sun, X.; Maansson, R.; Moeller, E.; Christiano, S.; Chen, J. Phase III, randomized controlled trial in girls 9–15 years old to evaluate lot consistency of a novel nine-valent human papillomavirus L1 virus-like particle vaccine. Hum. Vaccin. Immunother. 2015, 11, 1306–1312. [Google Scholar] [CrossRef] [Green Version]
- Konno, R.; Yoshikawa, H.; Okutani, M.; Quint, W.V.; Suryakiran, P.; Lin, L.; Struyf, F. Efficacy of the human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical intraepithelial neoplasia and cervical infection in young Japanese women. Hum. Vaccin. Immunother. 2014, 10, 1781–1794. [Google Scholar] [CrossRef]
- Guevara, A.; Cabello, R.; Woelber, L.; Moreira, E.D., Jr.; Joura, E.; Reich, O.; Shields, C.; Ellison, M.C.; Joshi, A.; Luxembourg, A.; et al. Antibody persistence and evidence of immune memory at 5years following administration of the 9-valent HPV vaccine. Vaccine 2017, 35, 5050–5057. [Google Scholar] [CrossRef]


{kind=link}
| Bivalent Vaccine Cervarix® | 4-Valent Vaccine Gardasil® | 9-Valent Vaccine Gardasil9® | |
|---|---|---|---|
| Target HPV types | HPV 16/18 (HR-HPV) | HPV 6/11 (LR-HPV) HPV 16/18 (HR-HPV) | HPV 6/11 (LR-HPV) HPV 16/18/31/33/45/52 (HR-HPV) |
| Schedule | Over 10 years 0, 1, and 6 months | Over 9 years 0, 2, and 6 months | Over 9 years 0, 2, and 6 months |
| VLP dose | L1 dose 20/20 μg | L1 dose 20/40/40/20 μg | L1 dose 30/30/60/40/20/20/20/20/20 μg |
| Adjuvant | 500 μg aluminum hydroxide, 50 μg 3-O-deacylated-4-monophosphoryl lipid A | 225 μg aluminum hydroxyphosphate sulfate | 500 μg aluminum hydroxyphosphate sulfate |
| Study | Study Design | Study Subjects | Efficacy and Effectiveness | Follow-Up Period (Seropositivity) | Follow-Up Period (Clinical Effect) |
|---|---|---|---|---|---|
| HPV 001 [28] | Clinical trial | Young women (15–25 years) | Reduced HPV 16/18 infection and HPV 16/18-related cytological abnormalities | 3.6 years | 3.6 years |
| HPV 032/063 [29] | Clinical trial | Young women (20–25 years) | No case of HPV16/18–associated CIN1+ | 4 years | 4 years |
| Extension NCT00196937 [30] | Clinical trial | Women (15–55 years) | Sustained anti-HPV-16/18 seropositivity rates | 6 years | - |
| HPV 007 [31] | Clinical trial | Young women (15–25 years) | No case of persistent infection or CIN2+ associated with HPV-16/18 | 6.4 years | 6.4 years |
| VIVIAN study [32] | Clinical trial | Adult women (> 25 years) | Reduced HPV 16/18 infection, Cytological abnormalities and CIN1+ | - | 7 years |
| HPV 023 [33] | Clinical trial | Young women (15–25 years) | No new infection or CIN2+ associated with HPV 16/18 | 8.4 years | 8.4 years |
| Extension HPV023 [34] | Clinical trial | Young women (15–25 years) | No case of HPV16/18 infection and HPV16/18–related Histropathological abnormalities | 9.4 years | 9.4 years |
| NCT 00947115 [35] | Clinical trial | Women (15–55 years) | Sustained anti-HPV-16/18 antibody titers | 10 years | - |
| Costa Rica Vaccine Tria [36] | Clinical trial | Young women (18–25 years) | Reduced HPV16/18–related CIN2/3 | - | 11.1 years |
| P011–NCT 00309166 [37] | Clinical trial | Men (10–18 years) | Higher antibody titers of HPV 16/18 | 7 months | 7 months |
| Niigata Study [38] | Real–world data | Young women (25–26 years) | Reduced HPV 16/18 and HPV31/45/52 infection | - | 9 years |
| Study | Study Design | Study Subjects | Efficacy and Effectiveness | Follow-Up Period (Seropositivity) | Follow-Up Period (Clinical Effect) |
|---|---|---|---|---|---|
| FUTURE I [39] | Clinical trial | Young women (16–24 years) | Reduced HPV-related anogenital disease | 2 years | 3.6 years |
| HPV P007 [40] | Clinical trial | Young women (16–23 years) | No case of HPV 6/11/16/18-related CIN | 5 years | 5 years |
| Extension P007 [41] | Clinical trial | Young women (16–23 years) | Sustained serum anti-HPV 6/11/16/18 immunoglobulin levels | 5 years | – |
| Extension P019 [42] | Clinical trial | Adult women (24–45 years) | Reduced HPV 6/11/16/18-related CIN | 6 years | 6 years |
| Nordic P015 [43] | Clinical trial | Young women (16–23 years) | No case of HPV 6/11/16/18-related CIN | 9 years | 8 years |
| P019-21 [26] | Clinical trial | Adult women (24–45 years) | No case of HPV 6/11/16/18-related CIN, AIS and EGL | 10 years | 10 years |
| V501-018-11 [44] | Clinical trial | Girls and Boys (9–15 years) | No case breakthrough disease in the form of genital warts or cervical and/or genital precancers and cancers | 10.5 years | 10 years |
| FUTURE II (P015-21) [45] | Clinical trial | Young women (16–23 years) | No case of HPV16/18 related CIN2+ and cervical cancer | 14 years | 14 years |
| P020-AIN substudy [46] | Clinical trial | Men-MSM | Reduced AIN (grade 2+) | - | 3 years |
| NCT00090285 [47] (Extension P020/P020-11) | Clinical trial | Men (including MSM) (16–26 years) | No case of HPV 6/11/16/18-related EGL | - | 9.5 years in early vaccination 4.7 years in catch-up vaccination |
| P020-21 [48] | Clinical trial | Men (16–26 years) | No case of HPV 6/11-related genital warts, HPV 6/11/16/18-related EGL or AIN | 10 years | 10 years (up to 11.5 years) |
| Australian study (2015) [49] | Real-world data | Women (18–24, 25–35 years) | Reduced vaccine-targeted HPV infection | - | 9 years |
| Danich study [50] | Real-world data | Adult women (born in 1993, 1983) | Reduced high-grade CIN | - | 10 years |
| Australian study (2020) [51] | Real-world data | Women (18–35 years) | Reduced vaccine-targeted HPV infection | - | 12 years |
| Study | Study Design | Study Subjects | Efficacy and Effectiveness | Follow-Up Period (Seropositivity) | Follow-Up Period (Clinical Effect) |
|---|---|---|---|---|---|
| Latin American study [52] | Clinical trial | Young women (16–26 years) and girls and boys (9–15 years) | Prevented HPV31/33/45/52/58-related high-grade cervical, vulvar and vaginal dysplasia | 5 years | 5 years |
| Extension V503-001 [53] | Clinical trial | Young women (16–26 years) | Prevented persistent vaccine-targeted HPV infection, cytological abnormalities, high-grade lesions, and cervical procedures | 5 years | 6 years |
| LTFU extension study of V503-002 [54] | Clinical trial | Girls and boys (9–15 years) | No case of vaccine-targeted HPV infection, or high-grade CIN, AIS, VIN, VaIN, PIN, or genital warts | 7 years | 8 years |
| Scandinavian study [55] | Clinical trial | Young women (16–26 years) | No case of HPV 16/18/31/33/45/52/58-related high-grade CIN | - | 8 years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurosawa, M.; Sekine, M.; Yamaguchi, M.; Kudo, R.; Hanley, S.J.B.; Hara, M.; Adachi, S.; Ueda, Y.; Miyagi, E.; Ikeda, S.; et al. Long-Term Effects of Human Papillomavirus Vaccination in Clinical Trials and Real-World Data: A Systematic Review. Vaccines 2022, 10, 256. https://doi.org/10.3390/vaccines10020256
Kurosawa M, Sekine M, Yamaguchi M, Kudo R, Hanley SJB, Hara M, Adachi S, Ueda Y, Miyagi E, Ikeda S, et al. Long-Term Effects of Human Papillomavirus Vaccination in Clinical Trials and Real-World Data: A Systematic Review. Vaccines. 2022; 10(2):256. https://doi.org/10.3390/vaccines10020256
Chicago/Turabian StyleKurosawa, Megumi, Masayuki Sekine, Manako Yamaguchi, Risa Kudo, Sharon J. B. Hanley, Megumi Hara, Sosuke Adachi, Yutaka Ueda, Etsuko Miyagi, Sayaka Ikeda, and et al. 2022. "Long-Term Effects of Human Papillomavirus Vaccination in Clinical Trials and Real-World Data: A Systematic Review" Vaccines 10, no. 2: 256. https://doi.org/10.3390/vaccines10020256