
Peripheral Nervous System Adverse Events after the Administration of mRNA Vaccines: A Systematic Review and Meta-Analysis of Large-Scale Studies

Abstract
:1. Introduction
2. Materials and Methods
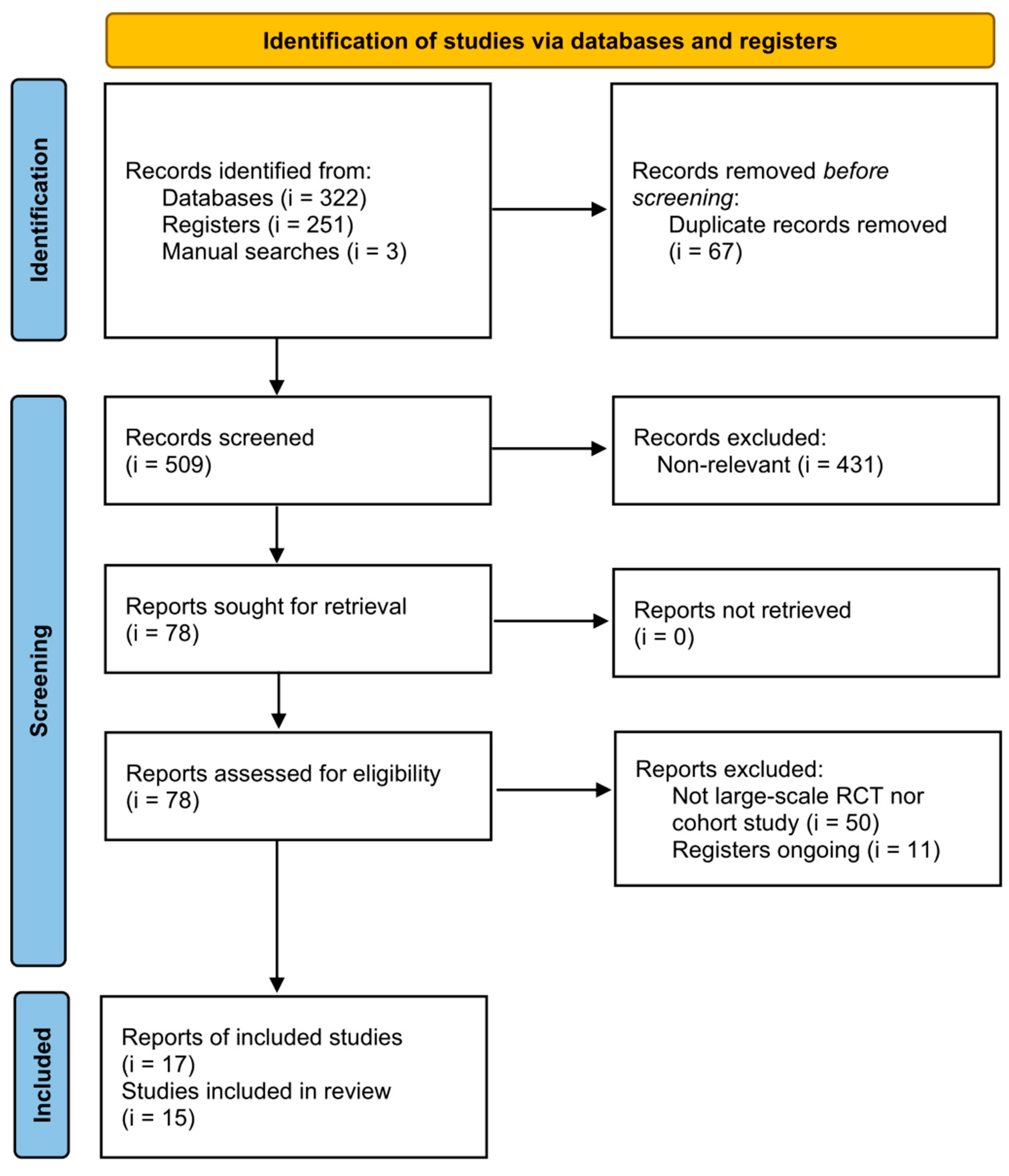
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection (Outcomes)
2.4. Quality Assessment
2.5. Statistical Methods
3. Results
3.1. Characteristics of the Included Studies
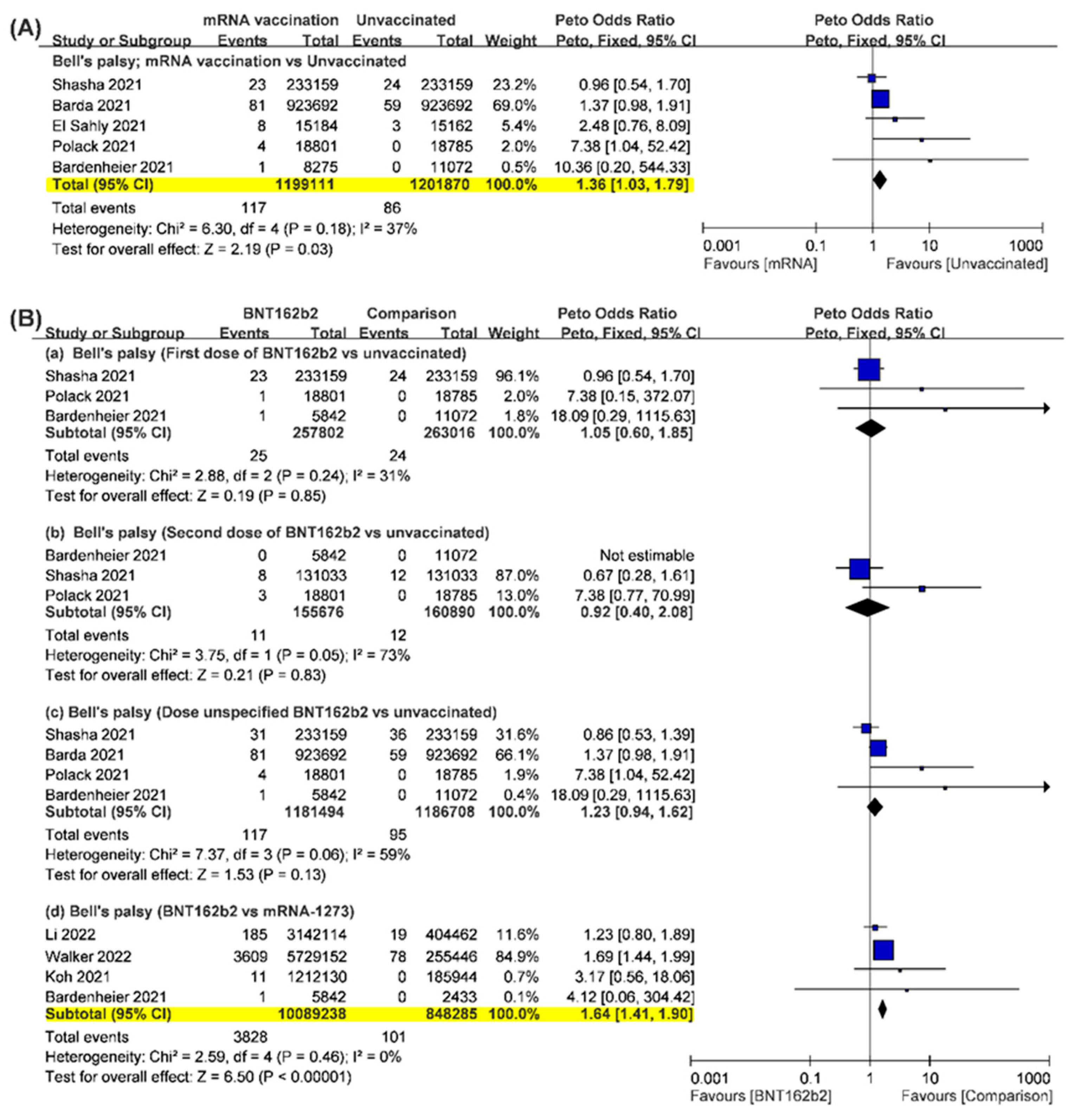
3.2. Bell’s Palsy
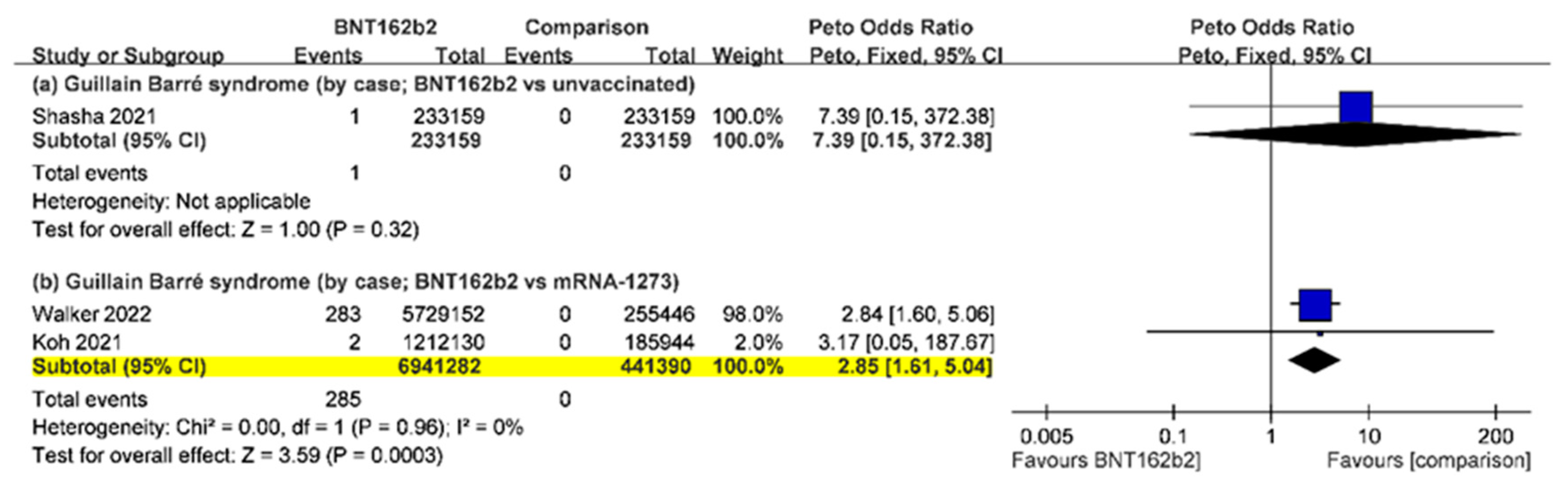
3.3. Guillain-Barré Syndrome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adam, D. The pandemic’s true death toll: Millions more than official counts. Nature 2022, 601, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- A McNamara, L.; E Wiegand, R.; Burke, R.M.; Sharma, A.J.; Sheppard, M.; Adjemian, J.; Ahmad, F.B.; Anderson, R.N.; E Barbour, K.; Binder, A.M.; et al. Estimating the early impact of the US COVID-19 vaccination programme on COVID-19 cases, emergency department visits, hospital admissions, and deaths among adults aged 65 years and older: An ecological analysis of national surveillance data. Lancet 2022, 399, 152–160. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. FDA Approves First COVID-19 Vaccine; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2021.
- Edwards, K.M.; Orenstein, W.A. COVID-19: Vaccines: UpToDate; Shefner, J.M., Ed.; UpToDate: Waltham, MA, USA, 2022. [Google Scholar]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A systematic review and meta-analysis of acceptability and its predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef]
- Patone, M.; Handunnetthi, L.; Saatci, D.; Pan, J.; Katikireddi, S.V.; Razvi, S.; Hunt, D.; Mei, X.W.; Dixon, S.; Zaccardi, F.; et al. Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. Nat. Med. 2021, 27, 2144–2153. [Google Scholar] [CrossRef]
- Sato, K.; Mano, T.; Niimi, Y.; Toda, T.; Iwata, A.; Iwatsubo, T. Facial nerve palsy following the administration of COVID-19 mRNA vaccines: Analysis of a self-reporting database. Int. J. Infect. Dis. 2021, 111, 310–312. [Google Scholar] [CrossRef]
- Matarneh, A.S.; Al-Battah, A.H.; Farooqui, K.; Ghamoodi, M.; Alhatou, M. COVID-19 vaccine causing Guillain-Barre syndrome, a rare potential side effect. Clin. Case Rep. 2021, 9, e04756. [Google Scholar] [CrossRef]
- Osowicki, J.; Morgan, H.; Harris, A.; Crawford, N.W.; Buttery, J.P.; Kiers, L. Guillain-Barré Syndrome in an Australian State Using Both mRNA and Adenovirus-Vector SARS-CoV-2 Vaccines. Ann. Neurol. 2021, 90, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Nagalli, S.; Shankar Kikkeri, N. Sub-acute Onset of Guillain-Barré Syndrome Post-mRNA-1273 Vaccination: A Case Report. SN Compr. Clin. Med. 2022, 4, 41. [Google Scholar] [CrossRef]
- Ozonoff, A.; Nanishi, E.; Levy, O. Bell’s palsy and SARS-CoV-2 vaccines. Lancet Infect. Dis. 2021, 21, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for Adverse Events After COVID-19 mRNA Vaccination. JAMA 2021, 326, 1390. [Google Scholar] [CrossRef]
- Shasha, D.; Bareket, R.; Sikron, F.H.; Gertel, O.; Tsamir, J.; Dvir, D.; Mossinson, D.; Heymann, A.D.; Zacay, G. Real-world safety data for the Pfizer BNT162b2 SARS-CoV-2 vaccine: Historical cohort study. Clin. Microbiol. Infect. 2022, 28, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Andalib, S.; Biller, J.; Di Napoli, M.; Moghimi, N.; McCullough, L.D.; Rubinos, C.A.; Nobleza, C.O.; Azarpazhooh, M.R.; Catanese, L.; Elicer, I.; et al. Peripheral Nervous System Manifestations Associated with COVID-19. Curr. Neurol. Neurosci. Rep. 2021, 21, 9. [Google Scholar] [CrossRef]
- Renoud, L.; Khouri, C.; Revol, B.; Lepelley, M.; Perez, J.; Roustit, M.; Cracowski, J.L. Association of Facial Paralysis with mRNA COVID-19 Vaccines: A Disproportionality Analysis Using the World Health Organization Pharmacovigilance Database. JAMA Intern. Med. 2021, 181, 1243–1245. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef] [PubMed]
- McMurry, R.; Lenehan, P.; Awasthi, S.; Silvert, E.; Puranik, A.; Pawlowski, C.; Venkatakrishnan, A.; Anand, P.; Agarwal, V.; O’Horo, J.C.; et al. Real-time analysis of a mass vaccination effort confirms the safety of FDA-authorized mRNA COVID-19 vaccines. Med (New York) 2021, 2, 965.e5–978.e5. [Google Scholar] [CrossRef] [PubMed]
- Bardenheier, B.H.; Gravenstein, S.; Blackman, C.; Gutman, R.; Sarkar, I.N.; Feifer, R.A.; White, E.M.; McConeghy, K.; Nanda, A.; Mor, V. Adverse events following mRNA SARS-CoV-2 vaccination among U.S. nursing home residents. Vaccine 2021, 39, 3844–3851. [Google Scholar] [CrossRef] [PubMed]
- García-Grimshaw, M.; Ceballos-Liceaga, S.E.; Hernández-Vanegas, L.E.; Núñez, I.; Hernández-Valdivia, N.; Carrillo-García, D.A.; Michel-Chávez, A.; Galnares-Olalde, J.A.; Carbajal-Sandoval, G.; Saniger-Alba, M.D.M.; et al. Neurologic adverse events among 704,003 first-dose recipients of the BNT162b2 mRNA COVID-19 vaccine in Mexico: A nationwide descriptive study. Clin. Immunol. 2021, 229, 108786. [Google Scholar] [CrossRef]
- Hanson, K.E.; Goddard, K.; Lewis, N.; Fireman, B.; Myers, T.R.; Bakshi, N.; Weintraub, E.; Donahue, J.G.; Nelson, J.C.; Xu, S.; et al. Incidence of Guillain-Barré Syndrome After COVID-19 Vaccination in the Vaccine Safety Datalink. JAMA Netw. Open 2022, 5, e228879. [Google Scholar] [CrossRef] [PubMed]
- Keh, R.Y.S.; Scanlon, S.; Datta-Nemdharry, P.; Donegan, K.; Cavanagh, S.; Foster, M.; Skelland, D.; Palmer, J.; Machado, P.M.; Keddie, S.; et al. COVID-19 vaccination and Guillain-Barré syndrome: Analyses using the National Immunoglobulin Database. Brain 2022. Online ahead of print. [Google Scholar]
- Koh, J.S.; Hoe, R.H.M.; Yong, M.H.; Chiew, H.J.; Goh, Y.; Yong, K.P.; Tu, T.M.; Chan, D.W.S.; Tan, B.Y.-Q.; Yeo, L.L.L.; et al. Hospital-based observational study of neurological disorders in patients recently vaccinated with COVID-19 mRNA vaccines. J. Neurol. Sci. 2021, 430, 120030. [Google Scholar] [CrossRef]
- Li, X.; Raventós, B.; Roel, E.; Pistillo, A.; Martinez-Hernandez, E.; Delmestri, A.; Reyes, C.; Strauss, V.; Prieto-Alhambra, D.; Burn, E.; et al. Association between covid-19 vaccination, SARS-CoV-2 infection, and risk of immune mediated neurological events: Population based cohort and self-controlled case series analysis. Bmj 2022, 376, e068373. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Rosenblum, H.G.; Gee, J.; Liu, R.; Marquez, P.L.; Zhang, B.; Strid, P.; E Abara, W.; McNeil, M.M.; Myers, T.R.; Hause, A.M.; et al. Safety of mRNA vaccines administered during the initial 6 months of the US COVID-19 vaccination programme: An observational study of reports to the Vaccine Adverse Event Reporting System and v-safe. Lancet Infect. Dis. 2022, 22, 802–812. [Google Scholar] [CrossRef]
- Walker, J.L.; Schultze, A.; Tazare, J.; Tamborska, A.; Singh, B.; Donegan, K.; Stowe, J.; E Morton, C.; Hulme, W.J.; Curtis, H.J.; et al. Safety of COVID-19 vaccination and acute neurological events: A self-controlled case series in England using the OpenSAFELY platform. Vaccine 2022, 40, 4479–4487. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Xu, L.; Luo, T.; Wu, F.; Zhao, B.; Li, X. The etiology of Bell’s palsy: A review. J. Neurol. 2020, 267, 1896–1905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, E.Y.F.; Chui, C.S.L.; Lai, F.T.T.; Chan, E.W.Y.; Li, X.; Yan, V.K.C.; Gao, L.; Yu, Q.; Lam, I.C.H.; Chun, R.K.C.; et al. Bell’s palsy following vaccination with mRNA (BNT162b2) and inactivated (CoronaVac) SARS-CoV-2 vaccines: A case series and nested case-control study. Lancet Infect. Dis. 2022, 22, 64–72. [Google Scholar] [CrossRef] [PubMed]
- De Beuckelaer, A.; Grooten, J.; De Koker, S. Type I Interferons Modulate CD8(+) T Cell Immunity to mRNA Vaccines. Trends Mol. Med. 2017, 23, 216–226. [Google Scholar] [CrossRef]
- Jonsson, L.; Alm, G.; Thomander, L. Elevated serum interferon levels in patients with Bell’s palsy. Arch. Otolaryngol. Head Neck Surg. 1989, 115, 37–40. [Google Scholar] [CrossRef]
- Hoare, M.; Woodall, T.; Alexander, G.J. Bell’s palsy associated with IFN-alpha and ribavirin therapy for hepatitis C virus infection. J. Interferon Cytokine Res. 2005, 25, 174–176. [Google Scholar] [CrossRef]
- Hwang, I.; Calvit, T.B.; Cash, B.D.; Holtzmuller, K.C. Bell’s palsy: A rare complication of interferon therapy for hepatitis C. Dig. Dis. Sci. 2004, 49, 619–620. [Google Scholar] [CrossRef]
- Ogundipe, O.; Smith, M. Bell’s palsy during interferon therapy for chronic hepatitis C infection in patients with haemorrhagic disorders. Haemophilia 2000, 6, 110–112. [Google Scholar] [CrossRef]
- Li, X.; Ostropolets, A.; Makadia, R.; Shoaibi, A.; Rao, G.; Sena, A.G.; Martinez-Hernandez, E.; Delmestri, A.; Verhamme, K.; Rijnbeek, P.R.; et al. Characterising the background incidence rates of adverse events of special interest for covid-19 vaccines in eight countries: Multinational network cohort study. BMJ 2021, 373, n1435. [Google Scholar] [CrossRef]
- Yılmaz, M.; Tarakcıoǧlu, M.; Bayazıt, N.; Bayazıt, Y.A.; Namıduru, M.; Kanlıkama, M. Serum cytokine levels in bell’s palsy. J. Neurol. Sci. 2002, 197, 69–72. [Google Scholar] [CrossRef]
- Lin, C.F.; Huang, Y.H.; Cheng, C.Y.; Wu, K.H.; Tang, K.S.; Chiu, I.M. Public Health Interventions for the COVID-19 Pandemic Reduce Respiratory Tract Infection-Related Visits at Pediatric Emergency Departments in Taiwan. Front. Public Health 2020, 8, 604089. [Google Scholar] [CrossRef] [PubMed]
- Rotulo, G.A.; Percivale, B.; Molteni, M.; Naim, A.; Brisca, G.; Piccotti, E.; Castagnola, E. The impact of COVID-19 lockdown on infectious diseases epidemiology: The experience of a tertiary Italian Pediatric Emergency Department. Am. J. Emerg. Med. 2021, 43, 115–117. [Google Scholar] [CrossRef]
- Tamaki, A.; Cabrera, C.I.; Li, S.; Rabbani, C.; Thuener, J.E.; Rezaee, R.P.; Fowler, N. Incidence of Bell Palsy in Patients with COVID-19. JAMA Otolaryngol.–Head Neck Surg. 2021, 147, 767–768. [Google Scholar] [CrossRef] [PubMed]
- Kline, L.B.; Kates, M.M.; Tavakoli, M. Bell Palsy. JAMA 2021, 326, 1983. [Google Scholar] [CrossRef]
- Reich, S.G. Bell’s Palsy. Continuum (Minneap Minn) 2017, 23, 447–466. [Google Scholar] [CrossRef] [PubMed]
- Shibli, R.; Barnett, O.; Abu-Full, Z.; Gronich, N.; Najjar-Debbiny, R.; Doweck, I.; Rennert, G.; Saliba, W. Association between vaccination with the BNT162b2 mRNA COVID-19 vaccine and Bell’s palsy: A population-based study. Lancet Reg. Health Eur. 2021, 11, 100236. [Google Scholar] [CrossRef] [PubMed]
- Shahrizaila, N.; Lehmann, H.C.; Kuwabara, S. Guillain-Barré syndrome. Lancet 2021, 397, 1214–1228. [Google Scholar] [CrossRef]
- Leonhard, S.E.; Mandarakas, M.R.; Gondim, F.A.A.; Bateman, K.; Ferreira, M.L.B.; Cornblath, D.R.; van Doorn, P.A.; Dourado, M.E.; Hughes, R.A.C.; Islam, B.; et al. Diagnosis and management of Guillain-Barré syndrome in ten steps. Nat. Rev. Neurol. 2019, 15, 671–683. [Google Scholar] [CrossRef]
- Maramattom, B.V.; Krishnan, P.; Paul, R.; Padmanabhan, S.; Cherukudal Vishnu Nampoothiri, S.; Syed, A.A.; Mangat, H.S. Guillain-Barré Syndrome following ChAdOx1-S/nCoV-19 Vaccine. Ann. Neurol. 2021, 90, 312–314. [Google Scholar] [CrossRef]
- Willison, H.J.; Jacobs, B.C.; van Doorn, P.A. Guillain-Barré syndrome. Lancet 2016, 388, 717–727. [Google Scholar] [CrossRef] [Green Version]
- Palaiodimou, L.; Stefanou, M.I.; Katsanos, A.H.; Fragkou, P.C.; Papadopoulou, M.; Moschovos, C.; Michopoulos, I.; Kokotis, P.; Bakirtzis, C.; Naska, A.; et al. Prevalence, clinical characteristics and outcomes of Guillain-Barré syndrome spectrum associated with COVID-19: A systematic review and meta-analysis. Eur. J. Neurol. 2021, 28, 3517–3529. [Google Scholar] [CrossRef] [PubMed]
- Keddie, S.; Pakpoor, J.; Mousele, C.; Pipis, M.; Machado, P.M.; Foster, M.; Record, C.J.; Keh, R.Y.S.; Fehmi, J.; Paterson, R.W.; et al. Epidemiological and cohort study finds no association between COVID-19 and Guillain-Barré syndrome. Brain 2021, 144, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Dickerman, B.A.; Madenci, A.L.; Gerlovin, H.; Kurgansky, K.E.; Wise, J.K.; Muñiz, M.J.F.; Ferolito, B.R.; Gagnon, D.R.; Gaziano, J.M.; Cho, K.; et al. Comparative Safety of BNT162b2 and mRNA-1273 Vaccines in a Nationwide Cohort of US Veterans. JAMA Intern. Med. 2022, 182, 739–746. [Google Scholar] [CrossRef]
- Richards, N.E.; Keshavarz, B.; Workman, L.J.; Nelson, M.R.; Platts-Mills, T.A.E.; Wilson, J.M. Comparison of SARS-CoV-2 Antibody Response by Age Among Recipients of the BNT162b2 vs the mRNA-1273 Vaccine. JAMA Netw. Open 2021, 4, e2124331. [Google Scholar] [CrossRef]
- Morris, A.M.; Deeks, S.L.; Hill, M.D.; Midroni, G.; Goldstein, W.C.; Mazzulli, T.; Davidson, R.; Squires, S.G.; Marrie, T.; McGeer, A.; et al. Annualized incidence and spectrum of illness from an outbreak investigation of Bell’s palsy. Neuroepidemiology 2002, 21, 255–261. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Trial/Author | Location | Period | Treatment | Dose | Sex (Male/Female) | Mean Age (Years) |
|---|---|---|---|---|---|---|
| NCT04470427 | United States | 2020/07/27 to | mRNA-M | 1, 2 (but mixed) | 7917/7263 | 51.4 |
| (Baden, El Sahly) | 2020/10/23 | Unvaccinated | Nil | 8057/7109 | 51.3 | |
| NCT04368728 | 152 sites | 2020/07/27 to | mRNA-B | 1, 2 (but mixed) | 9639/9221 | 52 |
| (Polack, Stephen) | worldwide | 2020/11/14 | Unvaccinated | Nil | 9436/9410 | 52 |
| Barda et al. | Israel | 2020/12/20 to | mRNA-B | 1, 2 (but mixed) | 461,590/423,238 | 38 |
| 2021/05/24 | Unvaccinated | Nil | 461,590/423,238 | 38 | ||
| Bardenheier et al. | United States | 2020/12/18 to | mRNA-B/M | 1, 2 (separated) | 1st 3191/5301, 2nd 3072/5161 | >65 (without mean age) |
| 2021/03/07 | Unvaccinated | 1, 2 (separated) | 4128/6731 | >65 (without mean age) | ||
| Garcia-Grimshaw et al. | Mexico | 2020/12/24 to | mRNA-B | Non-specific | All (dose): 16,646,623 | >18 (without mean age) |
| 2021/10/29 | mRNA-M | Non-specific | All (dose): 2318,057 | >18 (without mean age) | ||
| Hanson et al. | United States | 2020/12/13 to | mRNA-B | 1, 2 (but mixed) | Overall: 14,637,020 | >12 (without mean age) |
| 2021/11/13 | mRNA-M | 1, 2 (but mixed) | >12 (without mean age) | |||
| Keh et al. | England | 2021/01/01 | mRNA-B | Non-specific | Overall (national database) > 10,000 but unclear | NR |
| 2021/11/07 | mRNA-M | Non-specific | NR | |||
| Koh et al. | Singapore | 2020/12/30 to | mRNA-B | 1, 2 (but mixed) | Overall (estimated from percentage and total cases): | Overall: |
| 2021/04/20 | mRNA-M | 1, 2 (but mixed) | 761,950/636,124 | 59 | ||
| Li (Xintong) et al. | United Kingdom | 2020/09/01 | mRNA-B | 1, 2 (separated) | Overall: 8330,497 | >18 (without mean age) |
| and Spain | 2021/06/23 | mRNA-M | 1, 2 (separated) | >18 (without mean age) | ||
| McMurry et al. | United States | 2020/12/01 to | mRNA-B | 1, 2 (separated) | 20,695/31,099 | 53.83 |
| 2021/04/20 | mRNA-M | 1, 2 (separated) | 7713/8758 | 63 | ||
| Unvaccinated | Nil | 28,408/39,857 | 55.61 | |||
| Renoud et al. | Worldwide | Before | mRNA-B | 1, 2 (but mixed) | Overall >10,000 but unclear | NR |
| 2021/03/09 | mRNA-M | 1, 2 (but mixed) | NR | |||
| Rosenblum et al. | United States | 2020/12/14 to | mRNA-B | 1, 2 (but mixed) | 45,157/116,587 (other 2925 were unknown) | Unclear |
| 2021/06/14 | mRNA-M | 1, 2 (but mixed) | 43,140/129,475 (other 3201 were unknown) | Unclear | ||
| Sato et al. | United States | Before | mRNA-B | 1, 2 (but mixed) | Overall >10,000 but unclear | NR |
| 2021/04/30 | mRNA-M | 1, 2 (but mixed) | NR | |||
| Shasha et al. | Israel | 2020/12/19 to | mRNA-B | 1, 2 (separated) | 1st 114,634/118,525; 2nd 64,580/66,453 | Unclear |
| 2021/02/12 | Unvaccinated | Nil | 1st 121,453/111,706; 2nd 64,580/66,453 | Unclear | ||
| Walker et al. | England | 2020/07/01 to | mRNA-B | 1, 2 separately | All: 5,729,152 | >18 (without mean age) |
| 2021/07/07 | mRNA-M | 1, 2 separately | All: 255,446 | >18 (without mean age) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-H.; Chen, H.-Y.; Chiu, H.-H.; Kang, Y.-N.; Wong, S.-B. Peripheral Nervous System Adverse Events after the Administration of mRNA Vaccines: A Systematic Review and Meta-Analysis of Large-Scale Studies. Vaccines 2022, 10, 2174. https://doi.org/10.3390/vaccines10122174
Lai Y-H, Chen H-Y, Chiu H-H, Kang Y-N, Wong S-B. Peripheral Nervous System Adverse Events after the Administration of mRNA Vaccines: A Systematic Review and Meta-Analysis of Large-Scale Studies. Vaccines. 2022; 10(12):2174. https://doi.org/10.3390/vaccines10122174
Chicago/Turabian StyleLai, Yu-Hsin, Hong-Yu Chen, Hsin-Hui Chiu, Yi-No Kang, and Shi-Bing Wong. 2022. "Peripheral Nervous System Adverse Events after the Administration of mRNA Vaccines: A Systematic Review and Meta-Analysis of Large-Scale Studies" Vaccines 10, no. 12: 2174. https://doi.org/10.3390/vaccines10122174