
Disease History, Pathogenesis, Diagnostics, and Therapeutics for Human Monkeypox Disease: A Comprehensive Review
 , , , , and
, , , , and
Abstract
:1. Background
2. History of Monkeypox
3. The 2017–2018 Outbreak in Nigeria
4. The 2022 MPXV Outbreak in Africa
5. The 2022 Monkeypox Outbreak Outside Africa
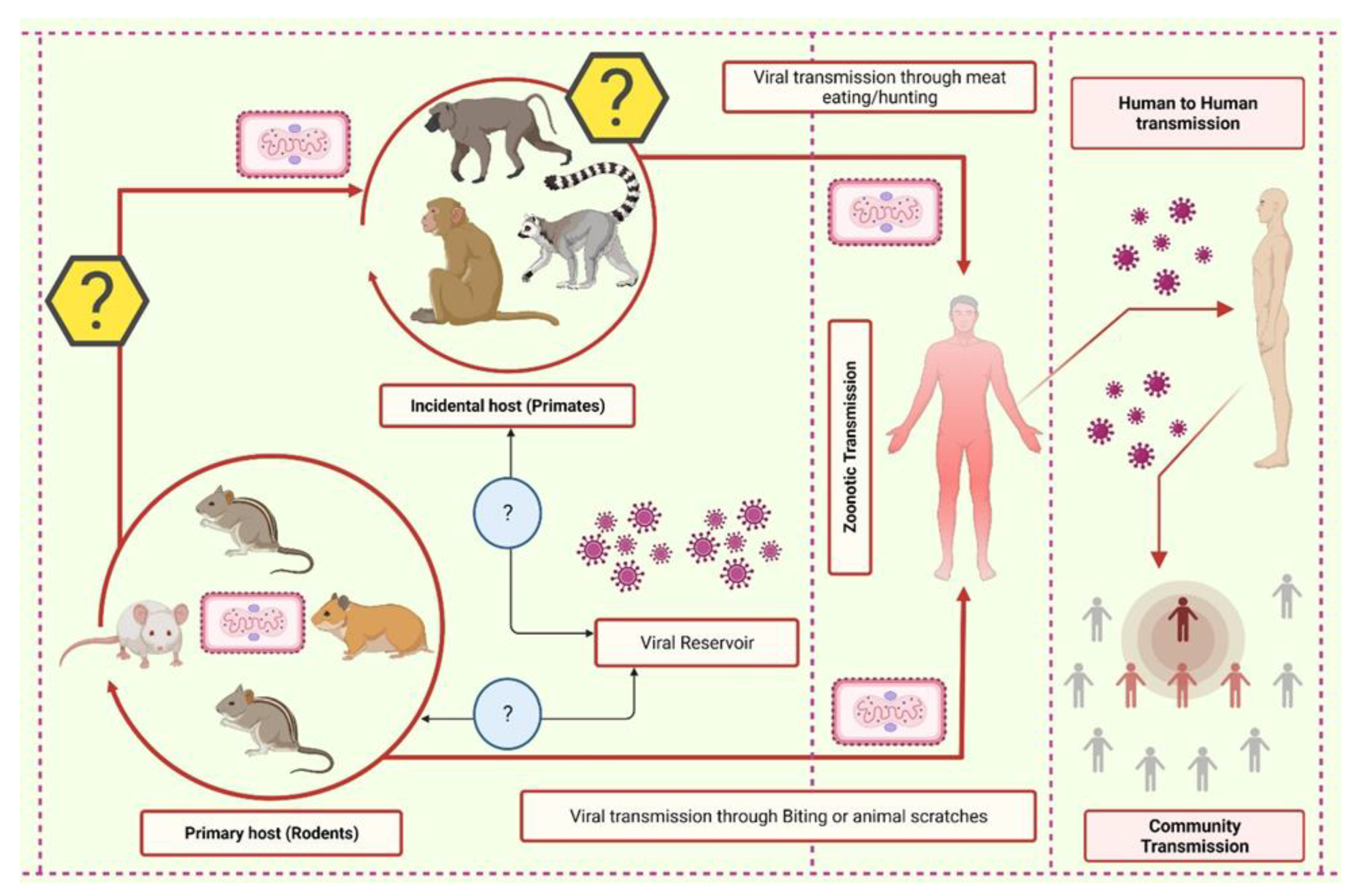
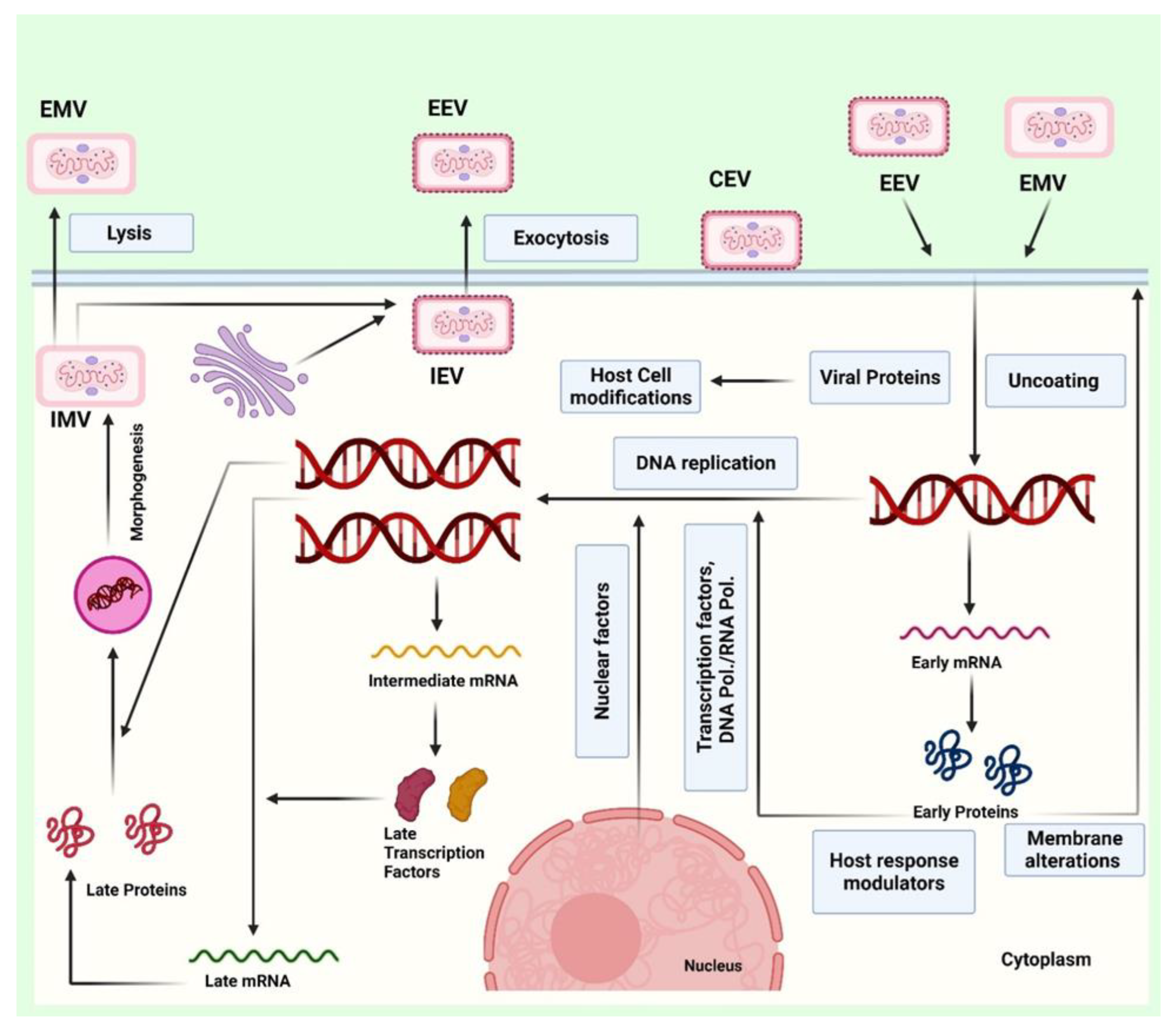
6. Pathogenesis and Infection Mechanism
7. Clinical Features and Risks for Infection
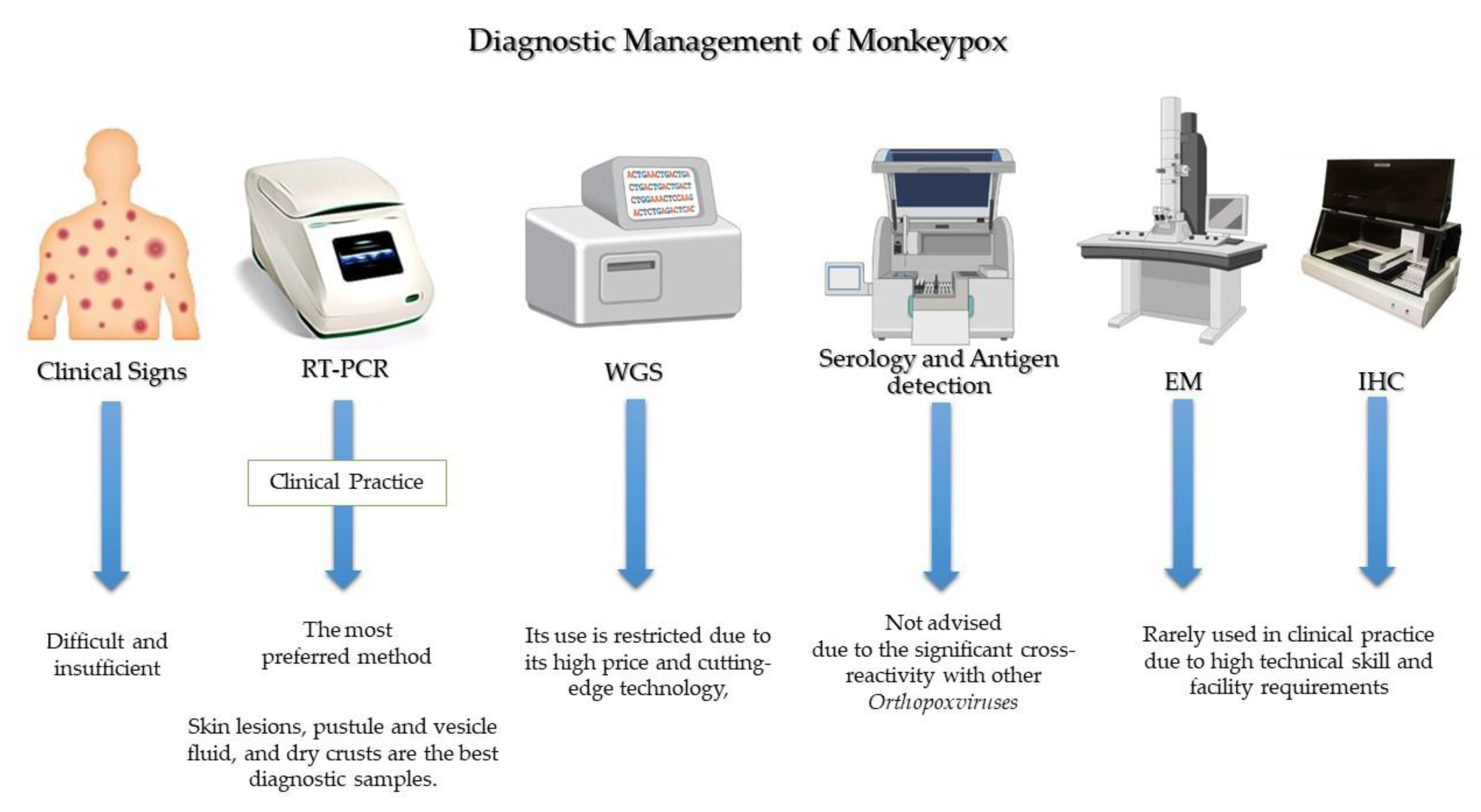
8. Diagnostic Management
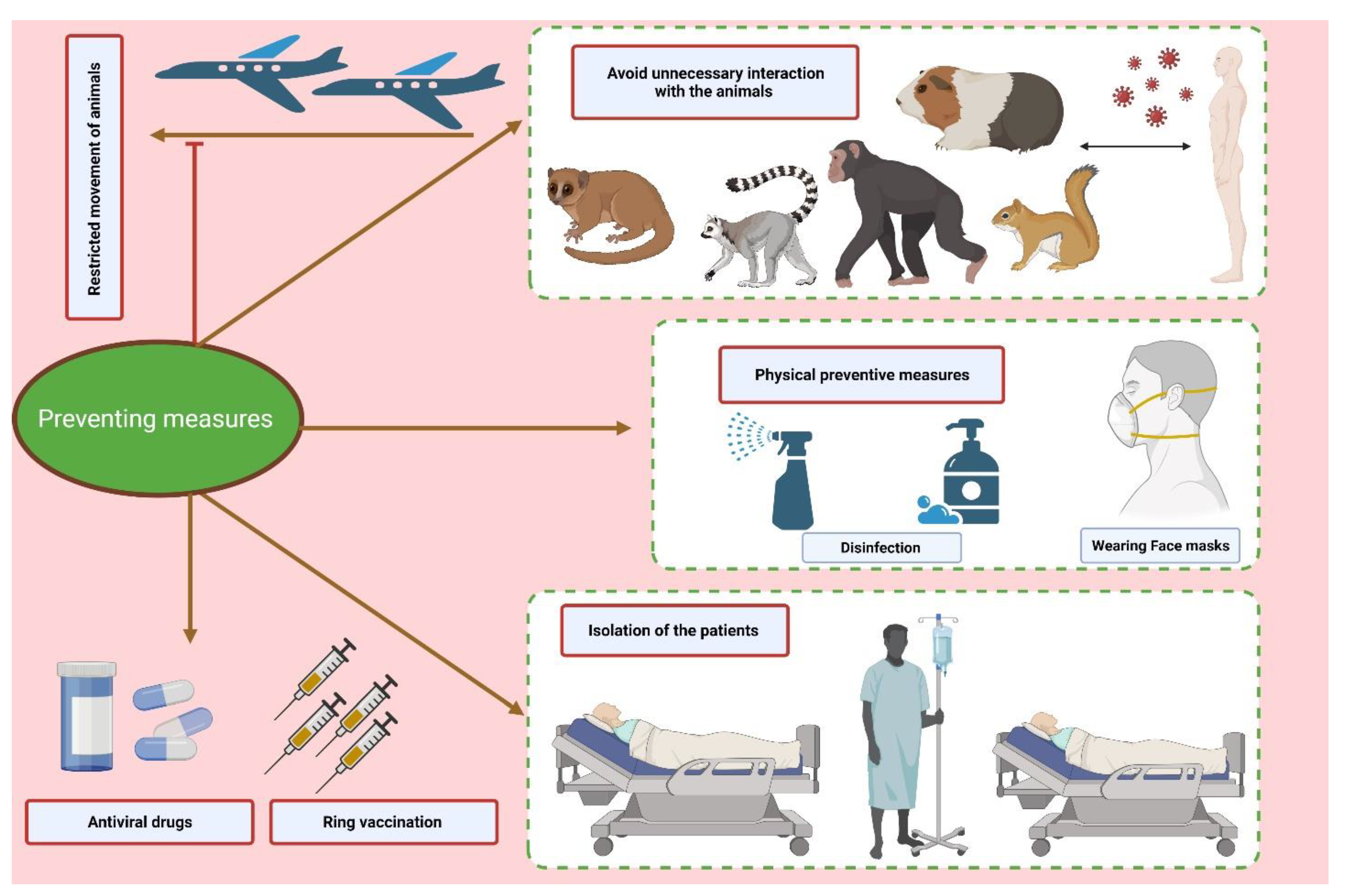
9. Preventive Measures
10. Therapeutics and Vaccination
11. Challenges
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| EEV | extracellular enveloped virus |
| IMV | intracellular mature virus |
| IL | interleukin |
| MPX | monkeypox |
| MPXV | monkeypox virus |
| NSAIDs | non-steroidal anti-inflammatory drugs |
| RT-PCR | real-time polymerase chain reaction |
| STIs | sexually transmitted infections |
| WGS | whole-genome sequencing |
| VIGIV | vaccinia immune globulin intravenous |
| WHO | World Health Organization |
References
- Alakunle, E.; Moens, U.; Nchinda, G.; Okeke, M.I. Monkeypox virus in Nigeria: Infection biology, epidemiology, and evolution. Viruses 2020, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox—A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef] [PubMed]
- Di Giulio, D.B.; Eckburg, P.B. Human monkeypox: An emerging zoonosis. Lancet Infect. Dis. 2004, 4, 15–25. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Multi-Country Monkeypox Outbreak in Non-Endemic Countries: Update. Available online: Https://WwwWhoInt/Emergencies/Disease-Outbreak-News/Item/2022-DON3882022 (accessed on 13 November 2022).
- Sharma, A.; Priyanka Fahrni, M.L.; Choudhary, O.P. Monkeypox outbreak: New zoonotic alert after the COVID-19 pandemic. Int. J. Surg. 2022, 104, 106812. [Google Scholar] [CrossRef] [PubMed]
- Happi, C.; Adetifa, I.; Mbala, P.; Njouom, R.; Nakoune, E.; Happi, A.; Ndodo, N.; Ayansola, O.; Mboowa, G.; Bedford, T.; et al. Urgent need for a non-discriminatory and non-stigmatizing nomenclature for monkeypox virus. Virol. Org. 2022, 20, e3001769. [Google Scholar] [CrossRef]
- Von Magnus, P.; Andersen, E.K.; Petersen, K.B.; Birch-Andersen, A. A pox-like disease in cynomolgus monkeys. Acta Pathol. Microbiol. Scand. 1959, 46, 156–176. [Google Scholar] [CrossRef]
- Nakazawa, Y.; Emerson, G.L.; Carroll, D.S.; Zhao, H.; Li, Y.; Reynolds, M.; Karem, K.L.; Olson, V.A.; Lash, R.R.; Davidson, W.B.; et al. Phylogenetic and ecologic perspectives of a monkeypox outbreak, southern Sudan, 2005. Emerg. Infect. Dis. 2013, 19, 237. [Google Scholar] [CrossRef]
- Saied, A.A. Is monkeypox virus (MPXV) older than we think? Transbound. Emerg. Dis. 2022, 69, 2407–2408. [Google Scholar] [CrossRef] [PubMed]
- Saied, A.A.; Metwally, A.A.; Aiash, H. Paleovirology of monkeypox virus: Egyptian animal mummies should be in focus. Lancet Microbe 2022, 3, e900. [Google Scholar] [CrossRef]
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A human infection caused by monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull. World Health Organ. 1972, 46, 593–597. [Google Scholar]
- Lourie, B.; Bingham, P.G.; Evans, H.H.; Foster, S.O.; Nakano, J.H.; Herrmann, K.L. Human infection with monkeypox virus: Laboratory investigation of six cases in West Africa. Bull. World Health Organ. 1972, 46, 633. [Google Scholar] [PubMed]
- Marennikova, S.S.; Šeluhina, E.M.; Mal’Ceva, N.N.; Čimiškjan, K.L.; Macevič, G.R. Isolation and properties of the causal agent of a new variola-like disease (monkeypox) in man. Bull. World Health Organ. 1972, 46, 599. [Google Scholar] [PubMed]
- Heymann, D.L.; Szczeniowski, M.; Esteves, K. Re-emergence of monkeypox in Africa: A review of the past six years. Br. Med. Bull. 1998, 54, 693–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yinka-Ogunleye, A.; Aruna, O.; Dalhat, M.; Ogoina, D.; McCollum, A.; Disu, Y.; Mamadu, I.; Akinpelu, A.; Ahmad, A.; Burga, J.; et al. Outbreak of human monkeypox in Nigeria in 2017–18: A clinical and epidemiological report. Lancet Infect. Dis. 2019, 19, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Hutin, Y.J.; Williams, R.J.; Malfait, P.; Pebody, R.; Loparev, V.N.; Ropp, S.L.; Rodriguez, M.; Knight, J.C.; Tshioko, F.K.; Khan, A.S.; et al. Outbreak of human monkeypox, Democratic Republic of Congo, 1996 to 1997. Emerg. Infect. Dis. 2001, 7, 434. [Google Scholar] [CrossRef]
- Guarner, J.; Johnson, B.J.; Paddock, C.D.; Shieh, W.-J.; Goldsmith, C.S.; Reynolds, M.; Damon, I.K.; Regnery, R.L.; Zaki, S.R. Monkeypox transmission and pathogenesis in prairie dogs. Emerg. Infect. Dis. 2004, 10, 426. [Google Scholar] [CrossRef]
- Babkin, I.V.; Babkina, I.N.; Tikunova, N.V. An Update of Orthopoxvirus Molecular Evolution. Viruses 2022, 14, 388. [Google Scholar] [CrossRef]
- Li, H.; Zhang, H.; Ding, K.; Wang, X.-H.; Sun, G.-Y.; Liu, Z.-X.; Luo, Y. The evolving epidemiology of monkeypox virus. Cytokine Growth Factor Rev. 2022, 68, 1–12. [Google Scholar] [CrossRef]
- Tiee, M.S.; Harrigan, R.J.; Thomassen, H.A.; Smith, T.B. Ghosts of infections past: Using archival samples to understand a century of monkeypox virus prevalence among host communities across space and time. R. Soc. Open Sci. 2018, 5, 171089. [Google Scholar] [CrossRef] [Green Version]
- Parker, S.; Buller, R.M. A review of experimental and natural infections of animals with monkeypox virus between 1958 and 2012. Future Virol. 2013, 8, 129–157. [Google Scholar] [CrossRef] [Green Version]
- Antunes, F.; Cordeiro, R.; Virgolino, A. Monkeypox: From A Neglected Tropical Disease to a Public Health Threat. Infect. Dis. Rep. 2022, 14, 772–783. [Google Scholar] [CrossRef]
- Fenner, F. Smallpox: Emergence, Global Spread, and Eradication. Hist. Philos. Life Sci. 1993, 15, 397–420, JSTOR. Available online: http://www.jstor.org/stable/23331731 (accessed on 7 July 2022). [PubMed]
- Simpson, K.; Heymann, D.; Brown, C.S.; Edmunds, W.J.; Elsgaard, J.; Fine, P.; Hochrein, H.; Hoff, N.A.; Green, A.; Ihekweazu, C.; et al. Human monkeypox–After 40 years, an unintended consequence of smallpox eradication. Vaccine 2020, 38, 5077–5081. [Google Scholar] [CrossRef]
- Reynolds, M.G.; Davidson, W.B.; Curns, A.T.; Conover, C.S.; Huhn, G.; Davis, J.P.; Wegner, M.; Croft, D.R.; Newman, A.; Obiesie, N.N.; et al. Spectrum of infection and risk factors for human monkeypox, United States, 2003. Emerg. Infect. Dis. 2007, 13, 1332. [Google Scholar] [CrossRef] [PubMed]
- Yinka-Ogunleye, A.; Aruna, O.; Ogoina, D.; Aworabhi, N.; Eteng, W.; Badaru, S.; Mohammed, A.; Agenyi, J.; Etebu, E.N.; Numbere, T.-W.; et al. Reemergence of human monkeypox in Nigeria, 2017. Emerg. Infect. Dis. 2018, 24, 1149. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, A.; Aarons, E.; Astbury, J.; Balasegaram, S.; Beadsworth, M.; Beck, C.R.; Chand, M.; O’Connor, C.; Dunning, J.; Ghebrehewet, S.; et al. Two cases of monkeypox imported to the United Kingdom, September 2018. Eurosurveillance 2018, 23, 1800509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erez, N.; Achdout, H.; Milrot, E.; Schwartz, Y.; Wiener-Well, Y.; Paran, N.; Politi, B.; Tamir, H.; Israely, T.; Weiss, S.; et al. Diagnosis of imported monkeypox, Israel, 2018. Emerg. Infect. Dis. 2019, 25, 980. [Google Scholar] [CrossRef] [Green Version]
- Yong, S.E.F.; Ng, O.T.; Ho, Z.J.M.; Mak, T.M.; Marimuthu, K.; Vasoo, S.; Yeo, T.W.; Ng, Y.K.; Cui, L.; Ferdous, Z.; et al. Imported Monkeypox, Singapore. Emerg. Infect. Dis. 2020, 26, 1826. [Google Scholar] [CrossRef]
- Costello, V.; Sowash, M.; Gaur, A.; Cardis, M.; Pasieka, H.; Wortmann, G.; Ramdeen, S. Imported Monkeypox from International Traveler, Maryland, USA, 2021. Emerg. Infect. Dis. 2022, 28, 1002. [Google Scholar] [CrossRef]
- WHO. Monkeypox-United Kingdom of Great Britain and Northern Ireland. Available online: Https://WwwWhoInt/Emergencies/Disease-Outbreak-News/Item/2022-DON3812022 (accessed on 13 November 2022).
- Centers for Disease Control and Prevention. What Clinicians Need to Know About Monkeypox in the United States and Other Countries. Available online: Https://EmergencyCdcGov/Coca/Calls/2022/Callinfo_052422Aspn.d (accessed on 13 November 2022).
- Ogoina, D.; Izibewule, J.H.; Ogunleye, A.; Ederiane, E.; Anebonam, U.; Neni, A.; Oyeyemi, A.; Etebu, E.N.; Ihekweazu, C. The 2017 human monkeypox outbreak in Nigeria—report of outbreak experience and response in the Niger Delta University Teaching Hospital, Bayelsa State, Nigeria. PLoS ONE 2019, 14, e0214229. [Google Scholar] [CrossRef] [Green Version]
- Ogoina, D.; Iroezindu, M.; James, H.I.; Oladokun, R.; Yinka-Ogunleye, A.; Wakama, P.; Otike-odibi, B.; Usman, L.M.; Obazee, E.; Aruna, O.; et al. Clinical course and outcome of human monkeypox in Nigeria. Clin. Infect. Dis. 2020, 71. [Google Scholar] [CrossRef] [PubMed]
- Rimoin, A.W.; Mulembakani, P.M.; Johnston, S.C.; Smith, J.O.L.; Kisalu, N.K.; Kinkela, T.L.; Blumberg, S.; Thomassen, H.A.; Pike, B.L.; Fair, J.N.; et al. Major increase in human monkeypox incidence 30 years after smallpox vaccination campaigns cease in the Democratic Republic of Congo. Proc. Natl. Acad. Sci. USA 2010, 107, 16262–16267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilder-Smith, A.; Osman, S. Public health emergencies of international concern: A historic overview. J. Travel. Med. 2020, 27, taaa227. [Google Scholar] [CrossRef] [PubMed]
- Kozlov, M. Monkeypox in Africa: The science the world ignored. Nature 2022, 607, 17–18. [Google Scholar] [CrossRef] [PubMed]
- Fahrni, M.L.; Sharma, A.; Choudhary, O.P. Monkeypox: Prioritizing public health through early intervention and treatment. Int. J. Surg. 2022, 104, 106774. [Google Scholar] [CrossRef] [PubMed]
- BBC News. Monkeypox, Two More Confirmed Cases of Viral Infection. Available online: Https://WwwBbcCom/News/Uk-England-London-614492142022 (accessed on 13 November 2022).
- GOVUK. Monkeypox Cases Confirmed in England–Latest Updates. Available online: Https://WwwGovUk/Government/News/Monkeypox-Cases-Confirmed-in-England-Latest-Updates2022 (accessed on 13 November 2022).
- CDC. C for DC and P. 2022 U.S. Monkeypox Outbreak. Available online: Https://WwwCdcGov/Poxvirus/Monkeypox/Response/2022/IndexHtml2022 (accessed on 13 November 2022).
- Fahrni, M.L.; Priyanka; Choudhary, O.P. Possibility of vertical transmission of the human monkeypox virus. Int. J. Surg. 2022, 105, 106832. [Google Scholar] [CrossRef] [PubMed]
- Bížová, B.; Veselý, D.; Trojánek, M.; Rob, F. Coinfection of syphilis and monkeypox in HIV positive man in Prague, Czech Republic. Travel Med. Infect. Dis. 2022, 49, 102368. [Google Scholar] [CrossRef]
- Au, N.H.; Portillo, M.T.; Marwah, A.; Thomas-Bachli, A.; Demarsh, P.A.; Khan, K.; I Bogoch, I. Potential for monkeypox exportation from west and Central Africa through global travel networks. J. Travel Med. 2022, 29. [Google Scholar] [CrossRef]
- Vivancos, R.; Anderson, C.; Blomquist, P.; Balasegaram, S.; Bell, A.; Bishop, L.; Brown, C.S.; Chow, Y.; Edeghere, O.; Florence, I.; et al. Community transmission of monkeypox in the United Kingdom, April to May 2022. Eurosurveillance 2022, 27, 2200422. [Google Scholar] [CrossRef]
- WHO. Multi-Country Monkeypox Outbreak: Situation Update. 4 June 2022. Available online: Https//www.WhoInt/Emergencies/Disease-Outbreak-News/Item/2022-Don3902022 (accessed on 7 June 2022).
- Yang, Z. Monkeypox: A potential global threat? J. Med. Virol. 2022, 94, 4034–4036. [Google Scholar] [CrossRef]
- Reynolds, M.G.; Yorita, K.L.; Kuehnert, M.J.; Davidson, W.B.; Huhn, G.D.; Holman, R.C.; Damon, I.K. Clinical manifestations of human monkeypox influenced by route of infection. J. Infect. Dis. 2006, 194, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Duque, M.P.; Ribeiro, S.; Martins, J.V.; Casaca, P.; Leite, P.P.; Tavares, M.; Mansinho, K.; Duque, L.M.; Fernandes, C.; Cordeiro, R.; et al. Ongoing monkeypox virus outbreak, Portugal, 29 April to 23 May 2022. Eurosurveillance 2022, 27, 2200424. [Google Scholar] [CrossRef]
- Saied, A.A.; Metwally, A.A.; Choudhary, O.P. Monkeypox: An extra burden on global health. Int. J. Surg. 2022, 104, 106745. [Google Scholar] [CrossRef]
- Sklenovska, N.; Van Ranst, M. Emergence of monkeypox as the most important orthopoxvirus infection in humans. Front. Public Health 2018, 6, 241. [Google Scholar] [CrossRef] [Green Version]
- Quarleri, J.; Delpino, M.; Galvan, V. Monkeypox: Considerations for the understanding and containment of the current outbreak in non-endemic countries. GeroScience 2022, 44, 2095–2103. [Google Scholar] [CrossRef]
- Saied, A.A. Should not airborne transmission be ignored in the 2022 monkeypox outbreak? Int. J. Surg. 2022, 104, 106762. [Google Scholar] [CrossRef] [PubMed]
- Seang, S.; Burrel, S.; Todesco, E.; Leducq, V.; Monsel, G.; Le Pluart, D.; Cordevant, C.; Pourcher, V.; Palich, R. Evidence of human-to-dog transmission of monkeypox virus. Lancet 2022, 400, 658–659. [Google Scholar] [CrossRef]
- Mbala, P.K.; Huggins, J.W.; Riu-Rovira, T.; Ahuka, S.M.; Mulembakani, P.; Rimoin, A.W.; Martin, J.W.; Muyembe, J.-J.T. Maternal and fetal outcomes among pregnant women with human monkeypox infection in the Democratic Republic of Congo. J. Infect. Dis. 2017, 216, 824–828. [Google Scholar] [CrossRef] [PubMed]
- De Baetselier, I.; Van Dijck, C.; Kenyon, C.; Coppens, J.; Van den Bossche, D.; Smet, H.; Vanroye, F.; Liesenborghs, L.; Ramadan, K.; Platteau, T.; et al. Asymptomatic monkeypox virus infections among male sexual health clinic attendees in Belgium 2022. MedRxiv 2022, 11, 2288–2292. [Google Scholar] [CrossRef]
- Kugelman, J.R.; Johnston, S.C.; Mulembakani, P.M.; Kisalu, N.; Lee, M.S.; Koroleva, G.; McCarthy, S.E.; Gestole, M.c.; Wolfe, N.D.; Fair, J.N.; et al. Genomic variability of monkeypox virus among humans, Democratic Republic of the Congo. Emerg. Infect. Dis. 2014, 20, 232–239. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, F.I.; Bleck, C.K.E.; Mercer, J. Poxvirus host cell entry. Curr. Opin. Virol. 2012, 2, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.L.; Smith, G.L. Vaccinia virus morphogenesis and dissemination. Trends Microbiol. 2008, 16, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.L.; Law, M. The exit of vaccinia virus from infected cells. Virus Res. 2004, 106, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Velavan, T.P.; Meyer, C.G. Monkeypox 2022 outbreak: An update. Trop Med. Int. Health 2022. [CrossRef]
- Cifuentes-Munoz, N.; El Najjar, F.; Dutch, R.E. Viral cell-to-cell spread: Conventional and non-conventional ways. Adv. Virus Res. 2020, 108, 85–125. [Google Scholar] [CrossRef]
- Kumar, N.; Acharya, A.; Gendelman, H.E.; Byrareddy, S.N. The 2022 outbreak and the pathobiology of the monkeypox virus. J. Autoimmun. 2022, 131, 102855. [Google Scholar] [CrossRef]
- Johnston, S.C.; Johnson, J.C.; Stonier, S.W.; Lin, K.L.; Kisalu, N.K.; Hensley, L.E.; Rimoin, A.W. Cytokine modulation correlates with severity of monkeypox disease in humans. J. Clin. Virol. 2015, 63, 42–45. [Google Scholar] [CrossRef]
- Weinstein, R.A.; Nalca, A.; Rimoin, A.W.; Bavari, S.; Whitehouse, C.A. Reemergence of monkeypox: Prevalence, diagnostics, and countermeasures. Clin. Infect. Dis. 2005, 41, 1765–1771. [Google Scholar] [CrossRef]
- Weaver, J.R.; Isaacs, S.N. Monkeypox virus and insights into its immunomodulatory proteins. Immunol. Rev. 2008, 225, 96–113. [Google Scholar] [CrossRef] [Green Version]
- Fenner, F.; Henderson, D.A.; Arita, I.; Jezek, Z.; Ladnyi, I.D. Smallpox and Its Eradication; World Health Organization Geneva: Geneva, Switzerland, 1988; Volume 6. [Google Scholar]
- Dhawan, M.; Choudhary, O. Emergence of monkeypox: Risk assessment and containment measures. Travel. Med. Infect. Dis. 2022, 49, 102392. [Google Scholar] [CrossRef]
- Moore, M.; Zahra, F. Monkeypox. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2021. [Google Scholar]
- Adalja, A.; Inglesby, T. A Novel International Monkeypox Outbreak. Ann. Intern. Med. 2022, 175, 1175–1176. [Google Scholar] [CrossRef] [PubMed]
- Diseases, T.L.I. Monkeypox: A neglected old foe. Lancet Infect. Dis. 2022, 22, 913. [Google Scholar] [CrossRef]
- Dashraath, P.; Nielsen-Saines, K.; Mattar, C.; Musso, D.; Tambyah, P.; Baud, D. Guidelines for pregnant individuals with monkeypox virus exposure. Lancet 2022, 400, 21–22. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, O.P.; Saied, A.A.; Priyanka; Ali, R.K.; Maulud, S.Q. Russo-Ukrainian war: An unexpected event during the COVID-19 pandemic. Travel Med. Infect. Dis. 2022, 48, 102346. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, P.G.; Acosta-España, J.D.; Mosquera Moyano, F.; Altamirano Jara, M.B. Sexually or intimately transmitted infections: A look at the current outbreak of monkeypox in 2022. Travel Med. Infect. Dis. 2022, 49, 102383. [Google Scholar] [CrossRef]
- Griffiths-Acha, J.; Vela-Ganuza, M.; Sarró-Fuente, C.; López-Estebaranz, J.L. Monkeypox: A new differential diagnosis when addressing genital ulcer disease. Br. J. Dermatol. 2022, 187, 1050–1052. [Google Scholar] [CrossRef]
- de Sousa, D.; Patrocínio, J.; Frade, J.; Brazão, C.; Mancha, D.; Correia, C.; Borges-Costa, J.; Filipe, P. Monkeypox Diagnosis by Cutaneous and Mucosal Findings. Infect. Dis. Rep. 2022, 14, 759–764. [Google Scholar] [CrossRef]
- Durski, K.N.; McCollum, A.M.; Nakazawa, Y.; Petersen, B.W.; Reynolds, M.G.; Briand, S. Emergence of monkeypox in West Africa and Central Africa, 1970-2017/Emergence de l’orthopoxvirose simienne en Afrique de l’Ouest et en Afrique centrale, 1970–2017. Wkly Epidemiol. Rec. 2018, 93, 125–133. [Google Scholar]
- Li, Y.; Olson, V.A.; Laue, T.; Laker, M.T.; Damon, I.K. Detection of monkeypox virus with real-time PCR assays. J. Clin. Virol. 2006, 36, 194–203. [Google Scholar] [CrossRef]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, L.; Habibi, M.S.; et al. Monkeypox virus infection in humans across 16 countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef]
- Huhn, G.D.; Bauer, A.M.; Yorita, K.; Graham, M.B.; Sejvar, J.; Likos, A.; Damon, I.K.; Reynolds, M.; Kuehnert, M.J. Clinical characteristics of human monkeypox, and risk factors for severe disease. Clin. Infect. Dis. 2005, 41, 1742–1751. [Google Scholar] [CrossRef] [PubMed]
- CDC. C for DC and P. Preparation and Collection of Specimens. Centers for Disease Control and Prevention. Available online: Https://WwwCdcGov/Poxvirus/Monkeypox/Clinicians/Prep-Collection-SpecimensHtml2022 (accessed on 13 November 2022).
- Aden, T.A.; Blevins, P.; York, S.W.; Rager, S.; Balachandran, D.; Hutson, C.L.; Lowe, D.; Mangal, C.N.; Wolford, T.; Matheny, A.; et al. Rapid diagnostic testing for response to the monkeypox outbreak—Laboratory Response Network, United States, 17 May–30 June 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 904. [Google Scholar] [CrossRef] [PubMed]
- FDA. FDA Says to Test for Monkeypox You Must Swab the Lesion-Blood, Saliva May Give False Results. Available online: Https://WwwFdaGov/Medical-Devices/Safety-Communications/Monkeypox-Testing-Use-Lesion-Swab-Samples-Avoid-False-Results-Fda-Safety-Communication2022 (accessed on 13 November 2022).
- Altindis, M.; Puca, E.; Shapo, L. Diagnosis of monkeypox virus–An overview. Travel Med. Infect. Dis. 2022, 50, 102459. [Google Scholar] [CrossRef] [PubMed]
- Karem, K.L.; Reynolds, M.; Braden, Z.; Lou, G.; Bernard, N.; Patton, J.; Damon, I.K. Characterization of acute-phase humoral immunity to monkeypox: Use of immunoglobulin M enzyme-linked immunosorbent assay for detection of monkeypox infection during the 2003 North American outbreak. Clin. Vaccine Immunol. 2005, 12, 867–872. [Google Scholar] [CrossRef] [Green Version]
- Soheili, M.; Nasseri, S.; Afraie, M.; Khateri, S.; Moradi, Y.; Mortazavi, S.M.M.; Gilzad-Kohan, H. Monkeypox: Virology, Pathophysiology, Clinical Characteristics, Epidemiology, Vaccines, Diagnosis, and Treatments. J. Pharm. Pharm. Sci. 2022, 25, 297–322. [Google Scholar] [CrossRef]
- McCollum, A.M.; Damon, I.K. Human monkeypox. Clin. Infect. Dis. 2014, 58, 260–267. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Zhao, H.; Wilkins, K.; Hughes, C.; Damon, I.K. Real-time PCR assays for the specific detection of monkeypox virus West African and Congo Basin strain DNA. J. Virol. Methods 2010, 169, 223–227. [Google Scholar] [CrossRef]
- Li, D.; Wilkins, K.; McCollum, A.M.; Osadebe, L.; Kabamba, J.; Nguete, B.; Likafi, T.; Balilo, M.P.; Lushima, R.S.; Malekani, J.; et al. Evaluation of the GeneXpert for human monkeypox diagnosis. Am. J. Trop. Med. Hyg. 2016, 96, 405. [Google Scholar] [CrossRef] [Green Version]
- Chelsky, Z.L.; Dittmann, D.; Blanke, T.; Chang, M.; Vormittag-Nocito, E.; Jennings, L.J. Validation Study of a Direct Real-Time PCR Protocol for Detection of Monkeypox Virus. J. Mol. Diagn. 2022, 24, 1155–1159. [Google Scholar] [CrossRef]
- Brown, K.; Leggat, P.A. Human monkeypox: Current state of knowledge and implications for the future. Trop. Med. Infect. Dis. 2016, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Morales, A.J.; Ortiz-Martínez, Y.; Bonilla-Aldana, D.K. What has been researched about monkeypox? A bibliometric analysis of an old zoonotic virus causing global concern. New Microbes New Infect. 2022, 47, 100993. [Google Scholar] [CrossRef] [PubMed]
- Bosworth, A.; Wakerley, D.; Houlihan, C.F.; Atabani, S.F. Monkeypox: An old foe, with new challenges. Infect. Prev. Pr. 2022, 4, 100229. [Google Scholar] [CrossRef] [PubMed]
- Parvin, R.; Ali, A.; Nagy, A.; Zhu, Z.; Zhao, S.; Paul, A.K.; Hafez, H.M.; Shehata, A.A. Monkeypox virus: A comprehensive review of taxonomy, evolution, epidemiology, diagnosis, prevention, and control regiments so far. Ger. J. Microbiol. 2022, 2, 1–15. [Google Scholar] [CrossRef]
- Reynolds, M.G.; McCollum, A.M.; Nguete, B.; Shongo Lushima, R.; Petersen, B.W. Improving the care and treatment of monkeypox patients in low-resource settings: Applying evidence from contemporary biomedical and smallpox biodefense research. Viruses 2017, 9, 380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koenig, K.L.; Beÿ, C.K.; Marty, A.M. Monkeypox 2022 identify-isolate-inform (3I): A tool for frontline clinicians for a zoonosis with escalating human community transmission. One Health 2022, 15, 100410. [Google Scholar] [CrossRef] [PubMed]
- Okyay, R.A.; Bayrak, E.; Kaya, E.; Şahin, A.R.; Koçyiğit, B.F.; Taşdoğan, A.M.; Avcı, A.; Sümbül, H.E. Another Epidemic in the Shadow of Covid 19 Pandemic: A Review of Monkeypox. Proteins 2022, 7, 10. [Google Scholar] [CrossRef]
- Rizk, J.G.; Lippi, G.; Henry, B.M.; Forthal, D.N.; Rizk, Y. Prevention and Treatment of Monkeypox. Drugs 2022, 82, 957–963. [Google Scholar] [CrossRef]
- Wittek, R. Vaccinia immune globulin: Current policies, preparedness, and product safety and efficacy. Int. J. Infect. Dis. 2006, 10, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Whitehouse, E.R.; Rao, A.K.; Yon, C.Y.; Patricia, A.Y.; Griffin, M.; Gorman, S.; Angel, K.A.; McDonald, E.C.; Manlutac, A.L.; de Perio, M.A.; et al. Novel treatment of a vaccinia virus infection from an occupational needlestick—San Diego, California, 2019. Morb. Mortal. Wkly Rep. 2019, 68, 943. [Google Scholar] [CrossRef] [Green Version]
- Lindholm, D.A.; Fisher, R.D.; Montgomery, J.R.; Davidson, W.; Yu, P.A.; Yu, Y.C.; Burgado, J.; Wilkins, K.; Petersen , B.W.; Okulicz, J.F. Preemptive Tecovirimat Use in an Active Duty Service Member Who Presented With Acute Myeloid Leukemia After Smallpox Vaccination. Clin. Infect. Dis. 2019, 69, 2205–2207. [Google Scholar] [CrossRef]
- Huang, Y.; Mu, L.; Wang, W. Monkeypox: Epidemiology, pathogenesis, treatment and prevention. Signal. Transduct. Target Ther. 2022, 7, 1–22. [Google Scholar] [CrossRef]
- Russo, A.T.; Grosenbach, D.W.; Chinsangaram, J.; Honeychurch, K.M.; Long, P.G.; Lovejoy, C.; Maiti, B.; Meara, I.; Hruby, D.E. An overview of tecovirimat for smallpox treatment and expanded anti-orthopoxvirus applications. Expert Rev. Anti- infect. Ther. 2020, 19, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Grosenbach, D.W.; Honeychurch, K.; Rose, E.A.; Chinsangaram, J.; Frimm, A.; Maiti, B.; Lovejoy, C.; Meara, I.; Long, P.; Hruby, D.E. Oral tecovirimat for the treatment of smallpox. N. Engl. J. Med. 2018, 379, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Quenelle, D.C.; Buller, R.M.L.; Parker, S.; Keith, K.A.; Hruby, D.E.; Jordan, R.; Kern, E.R. Efficacy of delayed treatment with ST-246 given orally against systemic orthopoxvirus infections in mice. Antimicrob. Agents Chemother. 2007, 51, 689–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huggins, J.W.; Zwiers, S.H.; Baker, R.O.; Hensley, L.E.; Larsen, T.; Martinez, M.J.; Jahrling, P.B. Cidofovir treatment of variola (smallpox) in the hemorrhagic smallpox primate model and the IV monkeypox primate model. Antivir. Res. 2003, 57, A78. [Google Scholar]
- Chittick, G.; Morrison, M.; Brundage, T.; Nichols, W.G. Short-term clinical safety profile of brincidofovir: A favorable benefit–risk proposition in the treatment of smallpox. Antivir. Res. 2017, 143, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Lanier, R.; Trost, L.; Tippin, T.; Lampert, B.; Robertson, A.; Foster, S.; Rose, M.; Painter, W.; O’Mahony, R.; Almond, M.; et al. Development of CMX001 for the treatment of poxvirus infections. Viruses 2010, 2, 2740–2762. [Google Scholar] [CrossRef] [PubMed]
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.; Duncan, C.J.; et al. Clinical features management of human monkeypox: A retrospective observational study in the UK. Lancet Infect. Dis. 2022, 22, 1153–1162. [Google Scholar] [CrossRef]
- Choudhary, O.P.; Priyanka Fahrni, M.L.; Saied, A.A.; Chopra, H. Ring vaccination for monkeypox containment: Strategic imple-mentation and challenges. Int. J. Surg. 2022, 105, 106873. [Google Scholar] [CrossRef]
- Ahmed, M.; Naseer, H.; Arshad, M.; Ahmad, A. Monkeypox in 2022: A new threat in developing. Ann. Med. Surg. 2022, 78, 103975. [Google Scholar] [CrossRef]
- Greenberg, R.N.; Overton, E.T.; Haas, D.W.; Frank, I.; Goldman, M.; Von Krempelhuber, A.; Virgin, G.; Bädeker, N.; Vollmar, J.; Chaplin, P. Safety, immunogenicity, and surrogate markers of clinical efficacy for modified vaccinia Ankara as a smallpox vaccine in HIV-infected subjects. J. Infect. Dis. 2013, 207, 749–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatch, G.J.; Graham, V.A.; Bewley, K.R.; Tree, J.A.; Dennis, M.; Taylor, I.; Funnell, S.G.P.; Bate, S.R.; Steeds, K.; Tipton, T.; et al. Assessment of the protective effect of Imvamune and Acam2000 vaccines against aerosolized monkeypox virus in cynomolgus macaques. J. Virol. 2013, 87, 7805–7815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaughan, A.; Aarons, E.; Astbury, J.; Brooks, T.; Chand, M.; Flegg, P.; Hardman, A.; Harper, N.; Jarvis, R.; Mawdsley, S.; et al. Human-to-human transmission of monkeypox virus, United Kingdom, October 2018. Emerg. Infect. Dis. 2020, 26, 782. [Google Scholar] [CrossRef] [PubMed]
- Md Khairi, L.N.; Fahrni, M.L.; Lazzarino, A.I. The race for global equitable access to COVID-19 vaccines. Vaccines 2022, 10, 1306. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Event | References |
|---|---|---|
| 3500 years ago | Separation of MPXV within Old World Orthopoxviruses took place. | [18] |
| 600 years ago | MPXV West African subtype appeared | [18,19] |
| 1899 | Identification of MPXV in five species of African rope squirrel (Funisciurus sp.) collected across Central Africa. | [20] |
| 1958 | MPXV was first identified in Denmark following an outbreak of the pustular disease in a macaque colony (cynomolgus monkeys). The macaques had been imported from Singapore. | [7] |
| 1959–1964 | MPXV, which was reported among colonies of captive monkeys, were also described in the USA (1959 and 1962) and Rotterdam Zoo, the Netherlands (1964). | [21] |
| 1970 1972 | The first human monkeypox case was identified in the Democratic Republic of Congo (DRC, then Zaire). | [11] |
| 1970–1979 | A reported outbreak of human MPXV in Nigeria. | [1,22] |
| 1980 | Vaccination laid the basis for the eradication of Variola (genetically related to MPXV) | [23] |
| 1996–1997 | A major outbreak of human monkeypox occurred in Katako-Combe, Zaire (DRC). A total of 73% of cases reported contact with another human case while 27% had known contact with a wild animal. | [24] |
| 2003 | An outbreak of human monkeypox occurred in the USA (more than 71 infected people). It was initiated by rodents (small mammals) imported from Ghana to be sold as exotic pets and have been transmitted by pet prairie (Cynomys spp.). These infected mammals were kept near prairie dogs that were later sold as pets. | [25] |
| 2017 | The largest West-African monkeypox outbreak began in September 2017 in Nigeria following very heavy rainfall and flooding. Active surveillance confirmed human monkeypox, and as of September 2019, a total of 176 human-monkeypox cases had been confirmed from 18 states. | [15,26] |
| 2018 | Four individuals traveling from Nigeria to the United Kingdom (UK) (n = 2; travel from Nigeria, bush meat possible for one case—Secondary Exposure during healthcare), Israel (n = 1; rodent carcasses in Nigeria), and Singapore (n = 1; travel to Nigeria and attended a wedding and eat bushmeat) became the first human-monkeypox cases exported from Africa and a related nosocomial-transmission event in the UK became the first confirmed human-to-human monkeypox transmission event outside of Africa. This explains the role travelers play in the spread of infectious-disease epidemics in new regions globally. | [27,28,29] |
| 2019 | A further case of human monkeypox was confirmed in the UK, again imported from Nigeria. Contact tracing was initiated and the smallpox vaccine (Imvanex) was procured. In 2019, a Nigerian travelling to Singapore for a training course developed skin lesions shortly after arrival and was diagnosed with human monkeypox. | [24,27] |
| 2021 | Reported human-monkeypox cases in the UK. Another case was reported in a returning traveler from Nigeria to Maryland, and another case in Texas in the USA. | [30] |
| 2022 | MPXV outbreak outside Africa starting from UK in early May 2022 MPXV outbreak in Africa in endemic and non-endemic African countries | [31] |
| African Countries That Have Not Historically Reported Monkeypox | Confirmed Cases | Deaths |
| Egypt | 1 | 0 |
| Morocco | 3 | 0 |
| Sudan | 18 | 1 |
| Benin | 3 | 0 |
| Mozambique | 1 | 1 |
| South Africa | 5 | 0 |
| African Countries that Have Historically Reported Monkeypox | Confirmed Cases | Deaths |
| Liberia | 3 | 0 |
| Ghana | 107 | 4 |
| Nigeria | 624 | 7 |
| Cameroon | 16 | 2 |
| Central African Republic | 12 | 0 |
| Republic of the Congo | 5 | 0 |
| Democratic Republic of the Congo | 206 | 0 |
| Total as of 13 November 2022 | 1004 | 15 (CFR = 1.5%) |
| https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html, accessed on 13 November 2022 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saied, A.A.; Dhawan, M.; Metwally, A.A.; Fahrni, M.L.; Choudhary, P.; Choudhary, O.P. Disease History, Pathogenesis, Diagnostics, and Therapeutics for Human Monkeypox Disease: A Comprehensive Review. Vaccines 2022, 10, 2091. https://doi.org/10.3390/vaccines10122091
Saied AA, Dhawan M, Metwally AA, Fahrni ML, Choudhary P, Choudhary OP. Disease History, Pathogenesis, Diagnostics, and Therapeutics for Human Monkeypox Disease: A Comprehensive Review. Vaccines. 2022; 10(12):2091. https://doi.org/10.3390/vaccines10122091
Chicago/Turabian StyleSaied, AbdulRahman A., Manish Dhawan, Asmaa A. Metwally, Mathumalar Loganathan Fahrni, Priyanka Choudhary, and Om Prakash Choudhary. 2022. "Disease History, Pathogenesis, Diagnostics, and Therapeutics for Human Monkeypox Disease: A Comprehensive Review" Vaccines 10, no. 12: 2091. https://doi.org/10.3390/vaccines10122091