
A Simple Non-Invasive Score Based on Baseline Parameters Can Predict Outcome in Patients with COVID-19
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
- -
- Unit of Infectious Diseases. University Hospital Federico II, Naples.
- -
- Hospital “D. Cotugno”. AORN “Dei Colli”, Naples.
- -
- Hospital “G. Rummo”, Benevento.
- -
- Hospital “Sant’Anna e San Sebastiano”, Caserta.
- -
- Absence of respiratory symptoms related to COVID-19.
- -
- No serum CRP performed at admission (within 48 h).
- -
- No serum LDH performed at admission (within 48 h).
- -
- No arterial blood gas (ABG) test performed at admission (within 48 h).
- -
- History of a previous SARS-CoV-2 infection or presence of positive SARS-CoV-2 molecular test antecedent 2 weeks from hospitalization.
- -
- History of SARS-CoV-2 vaccination.
- -
- Other hospitalizations in the previous 30 days.
- -
- To analyse the correlation between serum LDH at hospital admission and the worst P/F ratio observed during hospitalization.
- -
- To analyse the correlation between blood lymphocyte count at admission and the worst P/F ratio observed during hospitalization.
- -
- To analyse the presence of risk factors for the worst P/F ratio < 200 during hospitalization.
- -
- To elaborate a scoring system for prediction of respiratory function deterioration.
- -
- To investigate the presence of risk factors for intensive care need during hospitalization.
- -
- To investigate the presence of risk factors for death during hospitalization.
2.2. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID19) Dashboard. Available online: https://covid19.who.int (accessed on 17 October 2022).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Sobieszczyk, M.E.; Hirsch, I.; Sproule, S.; Robb, M.L.; Corey, L.; Neuzil, K.M.; Hahn, W.; Hunt, J.; Mulligan, M.J.; et al. Phase 3 Safety and Efficacy of AZD1222 (ChAdOx1 nCoV-19) COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 2348–2360. [Google Scholar] [CrossRef] [PubMed]
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitzpatrick, M.C.; et al. The impact of vaccination on Coronavirus Disease 2019 (COVID-19) outbreaks in the United States. Clin. Inf. Dis. 2021, 73, 2257–2264. [Google Scholar] [CrossRef] [PubMed]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv, T.; Shorer Arbel, Y.; Scarfò, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef]
- Collier, D.A.; Ferreira, I.A.T.M.; Kotagiri, P.; Datir, R.P.; Lim, E.Y.; Touizer, E.; Meng, B.; Abdullahi, A.; Baker, S.; Dougan, G.; et al. Age-related immune response heterogeneity to SARS-CoV-2 vaccine BNT162b2. Nature 2021, 596, 417–422. [Google Scholar] [CrossRef]
- Yelin, I.; Katz, R.; Herzel, E.; Berman-Zilberstein, T.; Ben-Tov, A.; Kuint, J.; Gazit, S.; Patalon, T.; Chodick, G.; Kishony, R. Associations of the BNT162b2 COVID-19 vaccine effectiveness with patient age and comorbidities. medRxiv 2021. preprint. [Google Scholar] [CrossRef]
- Tamuzi, J.L.; Muyaya, L.M.; Mitra, A.; Nyasulu, P.S. Systematic review and meta-analysis of COVID-19 vaccines safety, tolerability, and efficacy among HIV-infected patients. medRxiv 2022. preprint. [Google Scholar] [CrossRef]
- Gao, Y.-d.; Ding, M.; Dong, X.; Zhang, J.-j.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.-l.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 illness in native and immunosuppressed states: A clinical–therapeutic staging proposal. J. Heart Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.a.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacciapuoti, S.; De Rosa, A.; Gelzo, M.; Megna, M.; Raia, M.; Pinchera, B.; Pontarelli, A.; Scotto, R.; Scala, E.; Scarano, F.; et al. Immunocytometric analysis of COVID patients: A contribution to personalized therapy? Life Sci. 2020, 261, 118355. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.L.; Hou, Y.L.; Li, D.T.; Li, F.Z. Laboratory findings of COVID-19: A systematic review and meta-analysis. Scand. J. Clin. Lab. Investig. 2020, 80, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Sokolowska, M.; Lukasik, Z.M.; Agache, I.; Akdis, C.A.; Akdis, D.; Akdis, M.; Barcik, W.; Brough, H.A.; Eiwegger, T.; Eljaszewicz, A.; et al. Immunology of COVID-19: Mechanisms, clinical outcome, diagnostics, and perspectives-A report of the European Academy of Allergy and Clinical Immunology (EAACI). Allergy 2020, 75, 2445–2476. [Google Scholar] [CrossRef]
- Zhang, J.J.; Cao, Y.Y.; Tan, G.; Dong, X.; Wang, B.C.; Lin, J.; Yan, Y.Q.; Liu, G.H.; Akdis, M.; Akdis, C.A.; et al. Clinical, radiological, and laboratory characteristics and risk factors for severity and mortality of 289 hospitalized COVID-19 patients. Allergy 2021, 76, 533–550. [Google Scholar] [CrossRef]
- Wolff, D.; Nee, S.; Hickey, N.S.; Marschollek, M. Risk factors for COVID-19 severity and fatality: A structured literature review. Infection 2021, 49, 15–28. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, X.; Jia, X.; Li, J.; Hu, K.; Chen, G.; Wei, J.; Gong, Z.; Zhou, C.; Yu, H.; et al. Risk factors for disease severity, unimprovement, and mortality in COVID-19 patients in Wuhan, China. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2020, 26, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Ebinger, J.E.; Achamallah, N.; Ji, H.; Claggett, B.L.; Sun, N.; Botting, P.; Nguyen, T.T.; Luong, E.; Kim, E.H.; Park, E.; et al. Pre-existing traits associated with COVID-19 illness severity. PLoS ONE 2020, 15, e0236240. [Google Scholar] [CrossRef]
- Bousquet, J.; Anto, J.M.; Czarlewski, W.; Haahtela, T.; Fonseca, S.C.; Iaccarino, G.; Blain, H.; Vidal, A.; Sheikh, A.; Akdis, C.A.; et al. Cabbage and fermented vegetables: From death rate heterogeneity in countries to candidates for mitigation strategies of severe COVID-19. Allergy 2021, 76, 735–750. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Anto, J.M.; Iaccarino, G.; Czarlewski, W.; Haahtela, T.; Anto, A.; Akdis, C.A.; Blain, H.; Canonica, G.W.; Cardona, V.; et al. Is diet partly responsible for differences in COVID-19 death rates between and within countries? Clin. Transl. Allergy 2020, 10, 16. [Google Scholar] [CrossRef]
- Li, R.; Tian, J.; Yang, F.; Lv, L.; Yu, J.; Sun, G.; Ma, Y.; Yang, X.; Ding, J. Clinical characteristics of 225 patients with COVID-19 in a tertiary Hospital near Wuhan, China. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2020, 127, 104363. [Google Scholar] [CrossRef]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in Patients Younger Than 60 Years Is a Risk Factor for COVID-19 Hospital Admission. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 896–897. [Google Scholar] [CrossRef] [Green Version]
- Attaway, A.A.; Zein, J.; Hatipoğlu, U.S. SARS-CoV-2 infection in the COPD population is associated with increased healthcare utilization: An analysis of Cleveland clinic’s COVID-19 registry. eClinicalMedicine 2020, 26, 100515. [Google Scholar] [CrossRef]
- Esposito, A.J.; Menon, A.A.; Ghosh, A.J.; Putman, R.K.; Fredenburgh, L.E.; El-Chemaly, S.Y.; Goldberg, H.J.; Baron, R.M.; Hunninghake, G.M.; Doyle, T.J. Increased Odds of Death for Patients with Interstitial Lung Disease and COVID-19: A Case-Control Study. Am. J. Respir. Crit. Care Med. 2020, 202, 1710–1713. [Google Scholar] [CrossRef]
- Singh, S.; Khan, A. Clinical Characteristics and Outcomes of Coronavirus Disease 2019 Among Patients With Preexisting Liver Disease in the United States: A Multicenter Research Network Study. Gastroenterology 2020, 159, 768–771.e763. [Google Scholar] [CrossRef]
- Ng, J.H.; Hirsch, J.S.; Wanchoo, R.; Sachdeva, M.; Sakhiya, V.; Hong, S.; Jhaveri, K.D.; Fishbane, S.; Abate, M.; Andrade, H.P.; et al. Outcomes of patients with end-stage kidney disease hospitalized with COVID-19. Kidney Int. 2020, 98, 1530–1539. [Google Scholar] [CrossRef]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Nadkarni, G.N.; Lala, A.; Bagiella, E.; Chang, H.L.; Moreno, P.R.; Pujadas, E.; Arvind, V.; Bose, S.; Charney, A.W.; Chen, M.D.; et al. Anticoagulation, Bleeding, Mortality, and Pathology in Hospitalized Patients With COVID-19. J. Am. Coll. Cardiol. 2020, 76, 1815–1826. [Google Scholar] [CrossRef] [PubMed]
- Bompard, F.; Monnier, H.; Saab, I.; Tordjman, M.; Abdoul, H.; Fournier, L.; Sanchez, O.; Lorut, C.; Chassagnon, G.; Revel, M.P. Pulmonary embolism in patients with COVID-19 pneumonia. Eur. Respir. J. 2020, 56, 2001365. [Google Scholar] [CrossRef]
- Liu, J.; Li, S.; Liu, J.; Liang, B.; Wang, X.; Wang, H.; Li, W.; Tong, Q.; Yi, J.; Zhao, L.; et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. eBioMedicine 2020, 55, 102763. [Google Scholar] [CrossRef]
- Huang, G.; Kovalic, A.J.; Graber, C.J. Prognostic Value of Leukocytosis and Lymphopenia for Coronavirus Disease Severity. Emerg. Infect. Dis. 2020, 26, 1839–1841. [Google Scholar] [CrossRef]
- Yu, H.H.; Qin, C.; Chen, M.; Wang, W.; Tian, D.S. D-dimer level is associated with the severity of COVID-19. Thromb. Res. 2020, 195, 219–225. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M. Procalcitonin in patients with severe coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chim. Acta 2020, 505, 190–191. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef]
- Lei, F.; Liu, Y.M.; Zhou, F.; Qin, J.J.; Zhang, P.; Zhu, L.; Zhang, X.J.; Cai, J.; Lin, L.; Ouyang, S.; et al. Longitudinal Association Between Markers of Liver Injury and Mortality in COVID-19 in China. Hepatology 2020, 72, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Jin, Y.; Li, R.; Zhang, Z.; Sun, R.; Chen, D. Prevalence and impact of acute renal impairment on COVID-19: A systematic review and meta-analysis. Crit. Care 2020, 24, 356. [Google Scholar] [CrossRef] [PubMed]
- Hadjadj, J.; Yatim, N.; Barnabei, L.; Corneau, A.; Boussier, J.; Smith, N.; Péré, H.; Charbit, B.; Bondet, V.; Chenevier-Gobeaux, C.; et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 2020, 369, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Scotto, R.; Pinchera, B.; Perna, F.; Atripaldi, L.; Giaccone, A.; Sequino, D.; Zappulo, E.; Sardanelli, A.; Schiano Moriello, N.; Stanziola, A.; et al. Serum KL-6 Could Represent a Reliable Indicator of Unfavourable Outcome in Patients with COVID-19 Pneumonia. Int. J. Environ. Res. Public Health 2021, 18, 2078. [Google Scholar] [CrossRef]
- Dickens, B.S.L.; Lim, J.T.; Low, J.W.; Lee, C.K.; Sun, Y.; Nasir, H.B.M.; Akramullah, F.A.B.M.; Yan, G.; Oon, J.; Yan, B.; et al. Simple “Rule-of-6” Predicts Severe Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2020, 72, 1861–1862. [Google Scholar] [CrossRef]
- Ye, W.; Chen, G.; Li, X.; Lan, X.; Ji, C.; Hou, M.; Zhang, D.; Zeng, G.; Wang, Y.; Xu, C.; et al. Dynamic changes of D-dimer and neutrophil-lymphocyte count ratio as prognostic biomarkers in COVID-19. Respir. Res. 2020, 21, 169. [Google Scholar] [CrossRef]
- Wang, D.; Yin, Y.; Hu, C.; Liu, X.; Zhang, X.; Zhou, S.; Jian, M.; Xu, H.; Prowle, J.; Hu, B.; et al. Clinical course and outcome of 107 patients infected with the novel coronavirus, SARS-CoV-2, discharged from two hospitals in Wuhan, China. Crit. Care 2020, 24, 188. [Google Scholar] [CrossRef]
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and outcomes of COVID-19 hospitalisations: Systematic review and meta-analysis. BMJ Evid. -Based Med. 2021, 26, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-j.; Ni, Z.-y.; Hu, Y.; Liang, W.-h.; Ou, C.-q.; He, J.-x.; Liu, L.; Shan, H.; Lei, C.-l.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Wang, F.; Nie, J.; Wang, H.; Zhao, Q.; Xiong, Y.; Deng, L.; Song, S.; Ma, Z.; Mo, P.; Zhang, Y. Characteristics of Peripheral Lymphocyte Subset Alteration in COVID-19 Pneumonia. J. Infect. Dis. 2020, 221, 1762–1769. [Google Scholar] [CrossRef]
- Mori, S.; Ai, T.; Otomo, Y. Characteristics, laboratories, and prognosis of severe COVID-19 in the Tokyo metropolitan area: A retrospective case series. PLoS ONE 2020, 15, e0239644. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.; Li, C.; Zhang, K.; Kang, H.; Chen, W.; Gu, B. Comparative analysis of laboratory indexes of severe and non-severe patients infected with COVID-19. Clin. Chim. Acta 2020, 509, 180–194. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, Y.; Zhang, C.; Huang, F.; Wang, F.; Yuan, J.; Wang, Z.; Li, J.; Li, J.; Feng, C.; et al. Clinical and biochemical indexes from 2019-nCoV infected patients linked to viral loads and lung injury. Sci. China Life Sci. 2020, 63, 364–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; van de Veen, W.; Brüggen, M.C.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef] [PubMed]
- Wendel Garcia, P.D.; Fumeaux, T.; Guerci, P.; Heuberger, D.M.; Montomoli, J.; Roche-Campo, F.; Schuepbach, R.A.; Hilty, M.P. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: Initial report of the international RISC-19-ICU prospective observational cohort. eClinicalMedicine 2020, 25, 100449. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2021, 27, 83–88. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex (M; n, %) | 204 (63.2) |
| Age (median, IQR) | 61 (49–70) |
| Age > 60 years (n, %) | 163 (50.5) |
| Comorbidities (n, %) | |
| Cardiovascular disease | 55 (17.0) |
| COPD | 54 (16.7) |
| CKD | 15 (4.6) |
| Malignancy | 41 (12.7) |
| Cirrhosis | 3 (0.9) |
| Diabetes | 53 (16.4) |
| N° of comorbidities (n, %) | |
| 0 | 187 (57.9) |
| 1–2 | 112 (34.7) |
| 3–5 | 24 (7.4) |
| Laboratory parameters at admission (median, IQR) | |
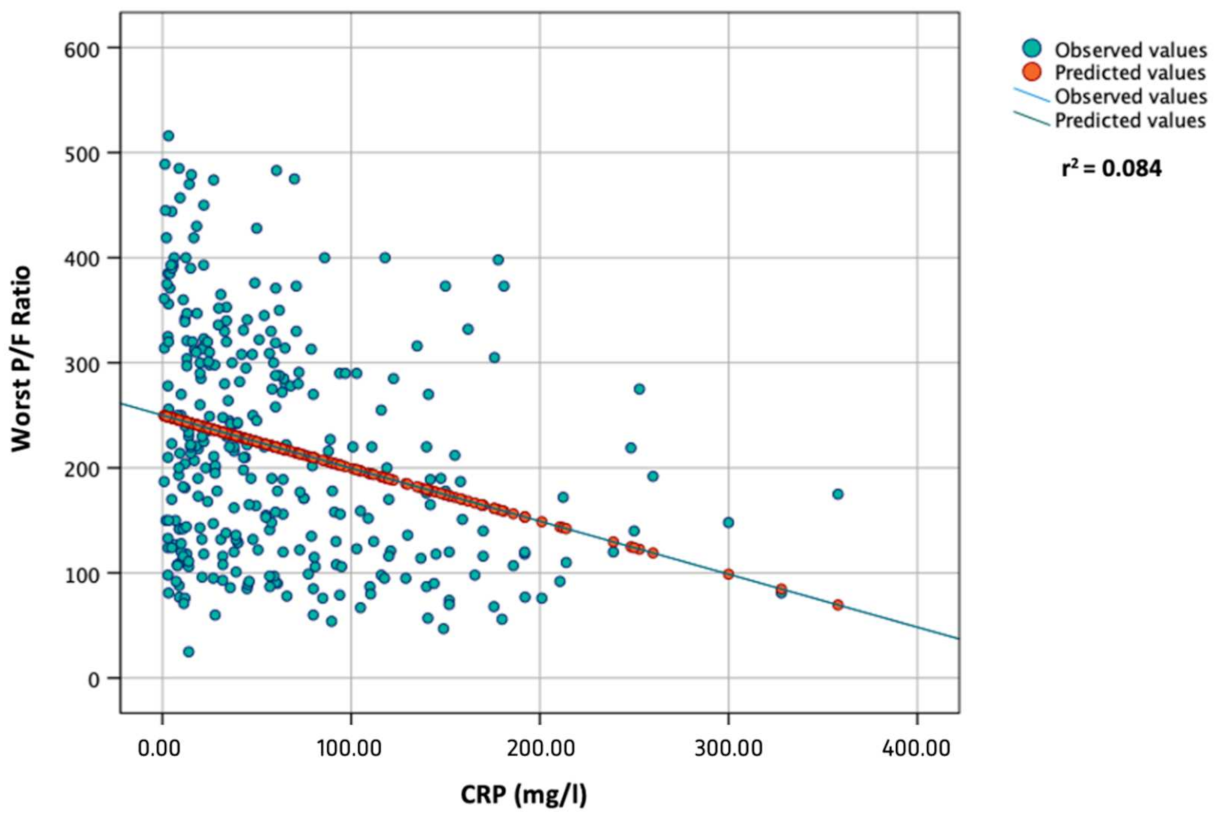
| CRP (mg/L) | 41.15 (15.10–88.75) |
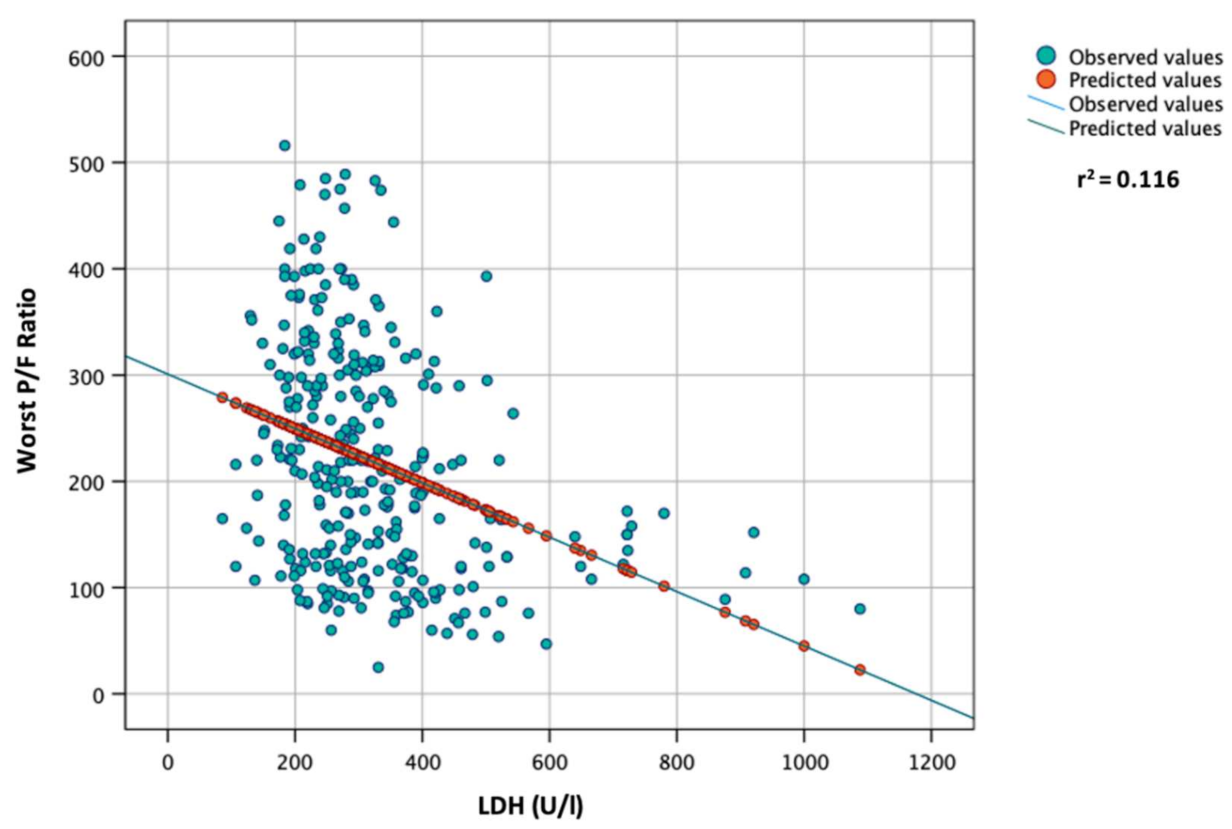
| LDH (U/L) | 288 (230–369) |
| Lymphocyte count (cell/µL) | 990 (680–1432) |
| Outcome (n, %) | |
| Worst P/F ratio < 200 | 153 (47.4) |
| ICU admission | 51 (15.8) |
| Exitus | 22 (6.8) |
| Worst P/F | ICU | Death | |||||||
|---|---|---|---|---|---|---|---|---|---|
| <200 | ≥200 | p-Value | Yes | No | p-Value | Yes | No | p-Value | |
| Male Sex (n, %) | 70.9 | 58.1 | <0.05 | 78.4 | 61.4 | <0.001 | 68.2 | 63.9 | 0.683 |
| Age (median, IQR) | 63 (54–72) | 58 (42–67) | <0.001 | 65 (52–71) | 60 (49–70) | 0.132 | 78 (71–84) | 60 (48–68) | <0.001 |
| Age > 60 years (n, %) | 56.4 | 37.7 | <0.001 | 66.0 | 49.2 | <0.05 | 90.9 | 49.0 | <0.001 |
| Comorbidities (n, %) | |||||||||
| Cardiovascular disease | 18.3 | 15.9 | 0.564 | 17.6 | 16.9 | 0.898 | 50.0 | 14.6 | <0.001 |
| COPD | 19.0 | 14.7 | 0.307 | 7.8 | 18.4 | 0.064 | 22.7 | 16.3 | 0.298 |
| CKD | 3.9 | 5.3 | 0.558 | 3.9 | 4.8 | 0.568 | 13.6 | 4.0 | <0.05 |
| Malignancy | 14.4 | 11.2 | 0.388 | 7.8 | 13.6 | 0.257 | 27.3 | 11.6 | <0.05 |
| Cirrhosis | 0.7 | 1.2 | 0.625 | 0.0 | 1.1 | 0.596 | 0.0 | 1.0 | 0.638 |
| Diabetes | 17.0 | 15.9 | 0.788 | 15.7 | 16.5 | 0.879 | 45.5 | 14.3 | <0.001 |
| N° of comorbidities (n, %) | |||||||||
| 0 | 54.9 | 60.6 | 0.301 | 62.7 | 57.0 | 0.445 | 22.7 | 60.5 | <0.001 |
| 1–2 | 37.9 | 31.8 | 0.247 | 35.3 | 34.6 | 0.919 | 54.4 | 33.2 | <0.05 |
| 3–5 | 7.2 | 7.6 | 0.876 | 2.0 | 8.5 | 0.081 | 22.7 | 6.3 | <0.01 |
| Baseline CRP (mg/L; median, IQR) | 60.0 (21.1–129.9) | 32.0 (14.30–60.10) | <0.001 | 77.4 (12.0–137.0) | 39.0 (16.0–75.0) | 0.059 | 87.15 (45.40–149.0) | 38.5 (15.0–80.0) | <0.001 |
| Baseline CRP > 60 mg/L (n, %) | 49.0 | 25.5 | <0.001 | 52.9 | 33.6 | <0.01 | 68.2 | 34.4 | <0.01 |
| Baseline LDH (U/L; median, IQR) | 342 (256–427) | 269 (211–321) | <0.001 | 357 (258–479) | 280 (220–351) | <0.001 | 337 (254–479) | 287 (228–360) | <0.05 |
| Baseline LDH > 600 U/L (n,%) | 10.1 | 0.0 | <0.001 | 16.0 | 2.7 | <0.001 | 13.6 | 4.1 | <0.05 |
| Baseline LDH > 300 U/L (n, %) | 59.7 | 32.3 | <0.001 | 62.0 | 42.2 | <0.05 | 59.1 | 44.3 | 0.180 |
| Baseline lymphocyte count (cell/µL; median, IQR) | 861 (605–1220) | 1100 (720–1550) | <0.001 | 880 (520–1150) | 1000 (690–1450) | <0.05 | 670 (430–920) | 1000 (690–1440) | <0.01 |
| Baseline lymphocyte count < 1000 cell/µL (n, %) | 62.2 | 43.4 | <0.001 | 64.7 | 49.8 | 0.051 | 76.2 | 50.5 | <0.05 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| B | 95CI | p-Value | B | 95CI | p-Value | |
| Worst P/F ratio # | - | - | - | - | - | - |
| Age | −2.372 | −3.073 to −1.672 | <0.001 | −2.079 | −2.724 to −1.433 | <0.001 |
| CRP | −0.504 | −0.690 to −0.319 | <0.001 | −0.323 | −0.497 to −0.149 | <0.001 |
| LDH | −0.256 | −0.335 to −0.177 | <0.001 | −0.205 | −0.279 to −0.130 | <0.001 |
| Lymphocyte | 0.000 | −0.005 to +0.006 | 0.862 | - | - | - |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95CI | p-Value | aOR | 95CI | p-Value | |
| Worst P/F ratio < 200 | ||||||
| Male sex | 1.75 | 1.10 to 2.80 | <0.05 | 1.73 | 1.03 to 2.91 | <0.05 |
| Age > 60 years | 2.14 | 1.36 to 3.56 | <0.001 | 1.80 | 1.10 to 2.94 | <0.05 |
| 1–2 comorbidities | 1.31 | 0.83 to 2.08 | 0.247 | - | - | - |
| 3–5 comorbidities | 0.94 | 0.41 to 2.15 | 0.936 | - | - | - |
| CRP > 60 mg/L | 2.81 | 1.75 to 4.52 | <0.001 | 2.33 | 1.37 to 3.94 | <0.01 |
| LDH > 300 U/L | 3.11 | 1.95 to 4.93 | <0.001 | 2.47 | 1.50 to 4.06 | <0.001 |
| Lymphocyte < 1000 cell/µL | 2.14 | 1.36 to 3.37 | <0.001 | 1.38 | 0.83 to 2.29 | 0.209 |
| ICU admission | ||||||
| Male sex | 2.28 | 1.12 to 4.65 | <0.05 | 2.31 | 1.08 to 4.92 | <0.05 |
| Age > 60 years | 2.00 | 1.06 to 3.77 | <0.05 | 1.66 | 0.86 to 3.21 | 0.130 |
| 1–2 comorbidities | 1.03 | 0.55 to 1.93 | 0.919 | - | - | - |
| 3–5 comorbidities | 0.22 | 0.03 to 1.64 | 0.214 | - | - | - |
| CRP > 60 mg/L | 2.22 | 1.21 to 4.08 | 0.01 | 2.00 | 1.03 to 3.86 | <0.05 |
| LDH > 300 U/L | 2.23 | 1.20 to 4.16 | <0.05 | 1.74 | 0.89 to 3.41 | 0.107 |
| Lymphocyte < 1000 cell/µL | 1.85 | 0.99 to 3.44 | 0.054 | 1.18 | 0.60 to 2.33 | 0.628 |
| Death | ||||||
| Male sex | 1.21 | 0.48 to 3.07 | 0.683 | 0.93 | 0.33 to 2.60 | 0.885 |
| Age > 60 years | 10.42 | 2.39 to 45,39 | <0.01 | 8.65 | 1.86 to 40.33 | <0.01 |
| 1–2 comorbidities | 2.41 | 1.01 to 5.77 | <0.05 | 2.85 | 0.92 to 8.87 | 0.07 |
| 3–5 comorbidities | 4.36 | 1.45 to 13.11 | <0.01 | 8.17 | 1.72 to 38.71 | <0.01 |
| CRP > 60 mg/L | 4.09 | 1.62 to 10.37 | <0.01 | 5.45 | 1.82 to 16.34 | <0.01 |
| LDH > 300 U/L | 1.81 | 0.75 to 4.38 | 0.185 | 1.02 | 0.36 to 2.90 | 0.969 |
| Lymphocyte < 1000 cell/µL | 3.13 | 1.12 to 8.78 | <0.05 | 2.20 | 0.71 to 6.78 | 0.169 |
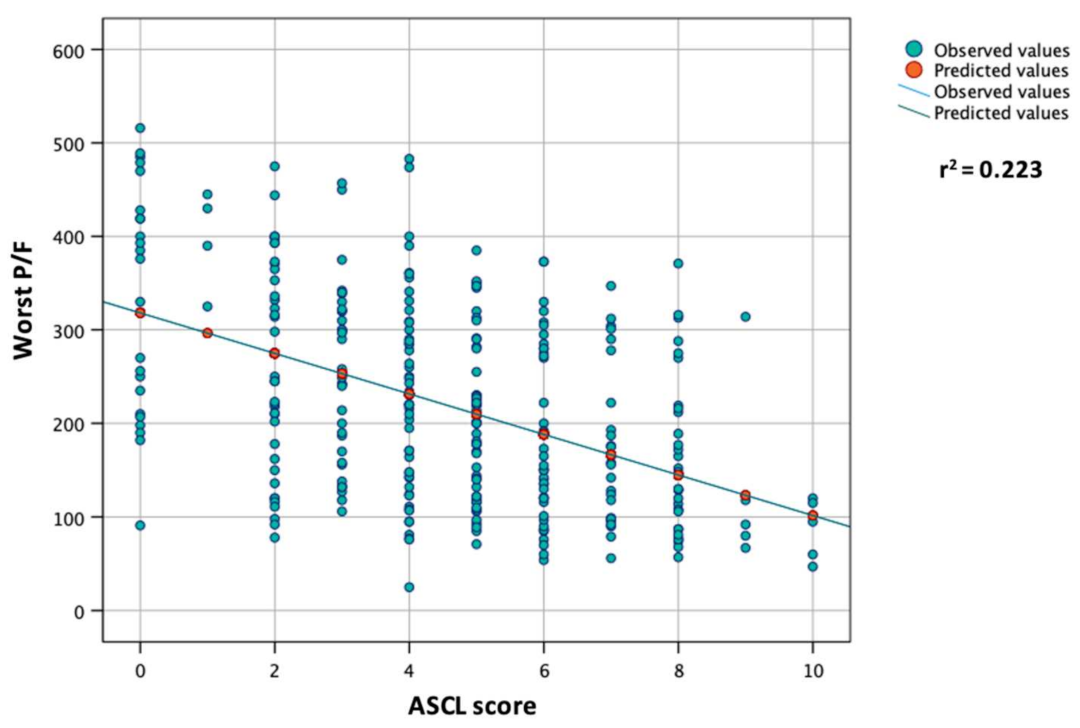
| Parameter | Points |
|---|---|
| Age | |
| <50 years | 0 |
| 50–59 years | 1 |
| 60–69 years | 2 |
| 70–79 years | 3 |
| ≥80 years | 4 |
| Sex | |
| Female | 0 |
| Male | 2 |
| CRP | |
| ≤60 mg/L | 0 |
| >60 mg/L | 2 |
| LDH | |
| ≤300 U/L | 0 |
| >300 U/L | 2 |
| P/F Ratio < 200 (n = 153) | |||
|---|---|---|---|
| ASCL Score | % * | OR | 95CI |
| 0 | 16.7 | 0.20 | 0.07 to 0.60 |
| 1 | 0.0 | # | # |
| 2 | 29.7 | 0.43 | 0.20 to 0.90 |
| 3 | 34.3 | 0.54 | 0.26 to 1.13 |
| 4 | 37.7 | 0.62 | 0.34 to 1.14 |
| 5 | 49.0 | 1.08 | 0.59 to 1.97 |
| 6 | 65.1 | 2.31 | 1.18 to 4.52 |
| 7 | 73.1 | 3.30 | 1.35 to 8.09 |
| 8 | 67.7 | 2.54 | 1.16 to 5.59 |
| 9 | 80.0 | 4.54 | 0.50 to 41.04 |
| 10 | 100.0 | ‡ | ‡ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scotto, R.; Lanzardo, A.; Buonomo, A.R.; Pinchera, B.; Cattaneo, L.; Sardanelli, A.; Mercinelli, S.; Viceconte, G.; Perrella, A.; Esposito, V.; et al. A Simple Non-Invasive Score Based on Baseline Parameters Can Predict Outcome in Patients with COVID-19. Vaccines 2022, 10, 2043. https://doi.org/10.3390/vaccines10122043
Scotto R, Lanzardo A, Buonomo AR, Pinchera B, Cattaneo L, Sardanelli A, Mercinelli S, Viceconte G, Perrella A, Esposito V, et al. A Simple Non-Invasive Score Based on Baseline Parameters Can Predict Outcome in Patients with COVID-19. Vaccines. 2022; 10(12):2043. https://doi.org/10.3390/vaccines10122043
Chicago/Turabian StyleScotto, Riccardo, Amedeo Lanzardo, Antonio Riccardo Buonomo, Biagio Pinchera, Letizia Cattaneo, Alessia Sardanelli, Simona Mercinelli, Giulio Viceconte, Alessandro Perrella, Vincenzo Esposito, and et al. 2022. "A Simple Non-Invasive Score Based on Baseline Parameters Can Predict Outcome in Patients with COVID-19" Vaccines 10, no. 12: 2043. https://doi.org/10.3390/vaccines10122043