
Hospitalization and Mortality by Vaccination Status among COVID-19 Patients Aged ≥ 25 Years in Bangladesh: Results from a Multicenter Cross-Sectional Study

 ,
,  ,
,  ,
,
Abstract
:1. Background
2. Methods
2.1. Study Setting
2.2. Study Design and Population
2.3. Sampling Technique
2.4. Data Collection
2.5. Statistical Analysis
2.6. Ethical Consideration
3. Results
3.1. Key Characteristics of Study Participants by Hospitals
3.2. Key Characteristics of Study Participants by Vaccination Status
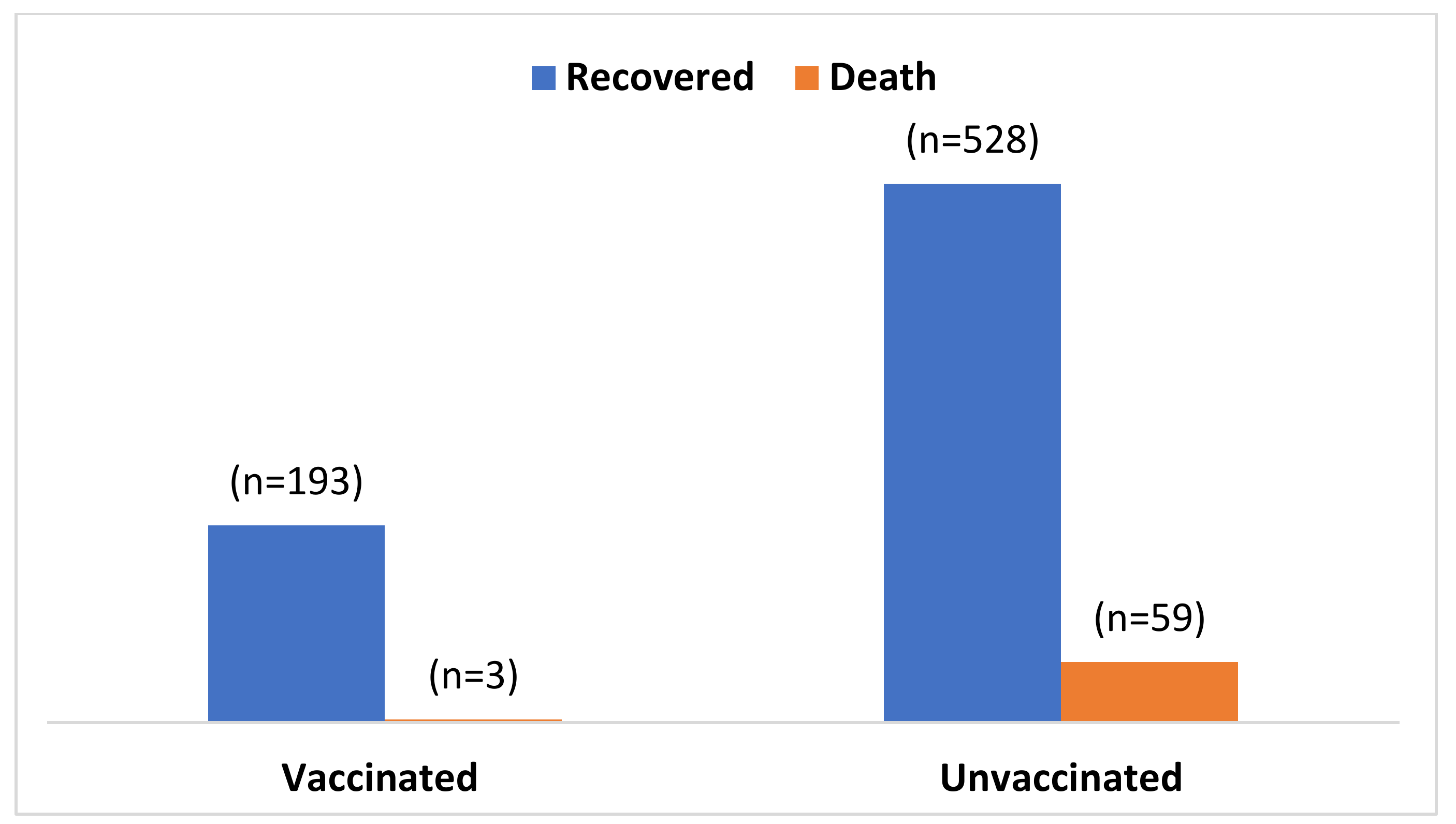
3.3. Factors Associated with COVID-19 Mortality of Enrolled Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fauci, A.S.; Lane, H.C.; Redfield, R.R. COVID-19—Navigating the Uncharted. N. Engl. J. Med. 2020, 382, 1268–1269. [Google Scholar] [CrossRef]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Qu, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Chi, H.; Chiu, N.-C.; Tai, Y.-L.; Chang, H.-Y.; Lin, C.-H.; Sung, Y.-H.; Tseng, C.-Y.; Liu, L.Y.-M.; Lin, C.-Y. Clinical features of neonates born to mothers with coronavirus disease-2019: A systematic review of 105 neonates. J. Microbiol. Immunol. Infect. 2021, 54, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Chi, H.; Chiu, N.-C.; Peng, C.-C.; Lin, C.-H.; Tai, Y.-L.; Lee, M.-D.; Cheng, Y.-J.; Tan, B.F.; Lin, C.-Y. One-Seventh of Patients with COVID-19 Had Olfactory and Gustatory Abnormalities as Their Initial Symptoms: A Systematic Review and Meta-Analysis. Life 2020, 10, 158. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Advice on the Use of Masks in the Context of COVID-19: Interim Guidance, 5 June 2020; WHO: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/332293 (accessed on 15 October 2022).
- Walker, P.G.T.; Whittaker, C.; Watson, O.J.; Baguelin, M.; Winskill, P.; Hamlet, A.; Djafaara, B.A.; Cucunubá, Z.; Mesa, D.O.; Green, W.; et al. The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries. Science 2020, 369, 413–422. [Google Scholar] [CrossRef]
- Schroter, R.C. Social distancing for COVID-19: Is 2 metres far enough? BMJ 2020, 369, m2010. [Google Scholar] [CrossRef]
- Cui, X.; Wang, P.; Wei, Z. Emergency use of COVID-19 vaccines recommended by the World Health Organization (WHO) as of June 2021. Drug Discov. Ther. 2021, 15, 222–224. [Google Scholar] [CrossRef]
- Centers for Disease Control Prevention. Updated Healthcare Infection Prevention and Control Recommendations in Response to COVID-19 Vaccination; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021. [Google Scholar]
- Tenforde, M.W.; Patel, M.M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; Gaglani, M.; McNeal, T.; et al. Effectiveness of SARS-CoV-2 mRNA Vaccines for Preventing COVID-19 Hospitalizations in the United States. medRxiv 2021. [Google Scholar] [CrossRef]
- Vasileiou, E.; Simpson, C.R.; Shi, T.; Kerr, S.; Agrawal, U.; Akbari, A.; Bedston, S.; Beggs, J.; Bradley, D.; Chuter, A.; et al. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: A national prospective cohort study. Lancet 2021, 397, 1646–1657. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Saadat, S.; Tehrani, Z.R.; Logue, J.; Newman, M.; Frieman, M.B.; Harris, A.D.; Sajadi, M.M. Binding and Neutralization Antibody Titers After a Single Vaccine Dose in Health Care Workers Previously Infected With SARS-CoV-2. JAMA 2021, 325, 1467. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, I.; Nauman, A.; Paul, P.; Ganesan, S.; Chen, K.-H.; Jalil, S.M.S.; Jaouni, S.H.; Kawas, H.; Khan, W.A.; Vattoth, A.L.; et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: A systematic review. Hum. Vaccines Immunother. 2022, 18, 2027160. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Olson, S.M.; Self, W.H.; Talbot, H.K.; Lindsell, C.J.; Steingrub, J.S.; Shapiro, N.I.; Ginde, A.A.; Douin, D.J.; Prekker, M.E.; et al. Effectiveness of Pfizer-BioNTech and Moderna Vaccines Against COVID-19 Among Hospitalized Adults Aged ≥65 Years—United States, January–March 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 674–679. [Google Scholar] [CrossRef]
- Griffin, J.B.; Haddix, M.; Danza, P.; Fisher, R.; Koo, T.H.; Traub, E.; Gounder, P.; Jarashow, C.; Balter, S. SARS-CoV-2 Infections and Hospitalizations Among Persons Aged ≥16 Years, by Vaccination Status—Los Angeles County, California, May 1–July 25, 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1170–1176. [Google Scholar] [CrossRef]
- Rinott, E.; Youngster, I.; Lewis, Y.E. Reduction in COVID-19 Patients Requiring Mechanical Ventilation Following Implementation of a National COVID-19 Vaccination Program—Israel, December 2020–February 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 326–328. [Google Scholar] [CrossRef]
- Bernal, J.L.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- Taib, N.A.A.; Raja, D.B.; Teo, A.K.J.; Kamarulzaman, A.; William, T.; Hs, A.-S.; Mokhtar, S.A.; Ting, C.-Y.; Yap, W.A.; Kim, M.C.Y.; et al. Characterisation of COVID-19 deaths by vaccination types and status in Malaysia between February and September 2021. Lancet Reg. Health-West. Pac. 2022, 18, 100354. [Google Scholar] [CrossRef]
- Muthukrishnan, J.; Vardhan, V.; Mangalesh, S.; Koley, M.; Shankar, S.; Yadav, A.K.; Khera, A. Vaccination status and COVID-19 related mortality: A hospital based cross sectional study. Med. J. Armed Forces India 2021, 77, S278–S282. [Google Scholar] [CrossRef]
- Word Health Organization. Bangladesh—WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/region/searo/country/bd (accessed on 26 September 2022).
- Abedin, M.; Islam, M.A.; Rahman, F.N.; Reza, H.M.; Hossain, M.Z.; Arefin, A.; Hossain, A. Willingness to vaccinate against COVID-19 among Bangladeshi adults: Understanding the strategies to optimize vaccination coverage. PLoS ONE 2021, 16, e0250495. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.M.A.; Rahman, M.L.; Hossian, M.; Matin, K.F.; Nabi, M.H.; Saha, S.; Hasan, M.; Manna, R.M.; Barsha, S.Y.; Hasan, S.; et al. Acceptance of COVID-19 vaccine and its determinants: Evidence from a large sample study in Bangladesh. Heliyon 2021, 7, e07376. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations?country=BGD (accessed on 26 September 2022).
- Islam, S.; Kamal, A.-H.M.; Kabir, A.; Southern, D.L.; Khan, S.H.; Hasan, S.M.M.; Sarkar, T.; Sharmin, S.; Das, S.; Roy, T.; et al. COVID-19 vaccine rumors and conspiracy theories: The need for cognitive inoculation against misinformation to improve vaccine adherence. PLoS ONE 2021, 16, e0251605. [Google Scholar] [CrossRef] [PubMed]
- John, B.V.; Deng, Y.; Scheinberg, A.; Mahmud, N.; Taddei, T.H.; Kaplan, D.; Labrada, M.; Baracco, G.; Dahman, B. Association of BNT162b2 mRNA and mRNA-1273 Vaccines With COVID-19 Infection and Hospitalization Among Patients With Cirrhosis. JAMA Intern. Med. 2021, 181, 1306–1314. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.M.; Newhams, M.M.; Halasa, N.B.; Price, A.M.; Boom, J.A.; Sahni, L.C.; Pannaraj, P.S.; Irby, K.; Walker, T.C.; Schwartz, S.P.; et al. Effectiveness of BNT162b2 Vaccine against Critical COVID-19 in Adolescents. N. Engl. J. Med. 2022, 386, 713–723. [Google Scholar] [CrossRef]
- Pálinkás, A.; Sándor, J. Effectiveness of COVID-19 Vaccination in Preventing All-Cause Mortality among Adults during the Third Wave of the Epidemic in Hungary: Nationwide Retrospective Cohort Study. Vaccines 2022, 10, 1009. [Google Scholar] [CrossRef]
- Singh, A.K.; Gillies, C.L.; Singh, R.; Singh, A.; Chudasama, Y.; Coles, B.; Seidu, S.; Zaccardi, F.; Davies, M.J.; Khunti, K. Prevalence of co-morbidities and their association with mortality in patients with COVID-19: A systematic review and meta-analysis. Diabetes Obes. Metab. 2020, 22, 1915–1924. [Google Scholar] [CrossRef]
- Freund, O.; Tau, L.; Weiss, T.E.; Zornitzki, L.; Frydman, S.; Jacob, G.; Bornstein, G. Associations of vaccine status with characteristics and outcomes of hospitalized severe COVID-19 patients in the booster era. PLoS ONE 2022, 17, e0268050. [Google Scholar] [CrossRef]
- Thompson, M.G.; Stenehjem, E.; Grannis, S.; Ball, S.W.; Naleway, A.L.; Ong, T.C.; DeSilva, M.B.; Natarajan, K.; Bozio, C.H.; Lewis, N.; et al. Effectiveness of COVID-19 Vaccines in Ambulatory and Inpatient Care Settings. N. Engl. J. Med. 2021, 385, 1355–1371. [Google Scholar] [CrossRef]
- Landi, F.; Barillaro, C.; Bellieni, A.; Brandi, V.; Carfì, A.; D’Angelo, M.; Fusco, D.; Landi, G.; Monaco, R.L.; Martone, A.M.; et al. The New Challenge of Geriatrics: Saving Frail Older People from the SARS-COV-2 Pandemic Infection. J. Nutr. Health Aging 2020, 24, 466–470. [Google Scholar] [CrossRef]
- Barek, A.; Aziz, A.; Islam, M.S. Impact of age, sex, comorbidities and clinical symptoms on the severity of COVID-19 cases: A meta-analysis with 55 studies and 10014 cases. Heliyon 2020, 6, e05684. [Google Scholar] [CrossRef] [PubMed]
- Saelee, R.; Zell, E.; Murthy, B.P.; Castro-Roman, P.; Fast, H.; Meng, L.; Shaw, L.; Gibbs-Scharf, L.; Chorba, T.; Harris, L.Q.; et al. Disparities in COVID-19 Vaccination Coverage Between Urban and Rural Counties—United States, December 14, 2020–January 31, 2022. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 335–340. [Google Scholar] [CrossRef]
- Roy, D.N.; Huda, N.; Azam, S. Factors influencing COVID-19 vaccine acceptance and hesitancy among rural community in Bangladesh: A cross-sectional survey based study. Hum. Vaccines Immunother. 2022, 18, 2064685. [Google Scholar] [CrossRef]
- Harun, G.D.; Anwar, M.U.; Sumon, S.A.; Hassan, Z.; Haque, T.; Mah-E-Muneer, S.; Rahman, A.; Abdullah, S.A.H.M.; Islam, S.; Styczynski, A.R.; et al. Infection prevention and control in tertiary care hospitals of Bangladesh: Results from WHO infection prevention and control assessment framework (IPCAF). Antimicrob. Resist. Infect. Control. 2022, 11, 125. [Google Scholar] [CrossRef] [PubMed]
- Harun, G.D.; Anwar, M.U.; Sumon, S.A.; Hassan, Z.; Mohona, T.M.; Rahman, A.; Abdullah, S.A.H.M.; Islam, S.; Kaydos-Daniels, S.C.; Styczynski, A.R. Rationale and guidance for strengthening infection prevention and control measures and antimicrobial stewardship programs in Bangladesh: A study protocol. BMC Health Serv. Res. 2022, 22, 1239. [Google Scholar] [CrossRef] [PubMed]
- Halim, M.; Halim, A.; Tjhin, Y. COVID-19 vaccination efficacy and safety literature review. J. Clin. Med. Res. 2021, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tagoe, E.T.; Sheikh, N.; Morton, A.; Nonvignon, J.; Sarker, A.R.; Williams, L.; Megiddo, I. COVID-19 Vaccination in Lower-Middle Income Countries: National Stakeholder Views on Challenges, Barriers, and Potential Solutions. Front. Public Health 2021, 9, 709127. [Google Scholar] [CrossRef]
- Galanakis, E.; Jansen, A.; Lopalco, P.L.; Giesecke, J. Ethics of mandatory vaccination for healthcare workers. Euro. Surveill. 2013, 18, 20627. [Google Scholar] [CrossRef] [Green Version]
- Maltezou, H.C.; Poland, G.A. Immunization of Health-Care Providers: Necessity and Public Health Policies. Healthcare 2016, 4, 47. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total [N = 783] | Hospital 1 [N = 344] | Hospital 2 [N = 322] | Hospital 3 [N = 117] |
|---|---|---|---|---|
| n/N (%) | ||||
| Age (in years) | ||||
| Median (IQR) | 56.0 [47.0–66.0] | 58.5 [50.0–58.5] | 54.0 [44.0–66.0] | 60.0 [50.0–68.0] |
| 25–40 | 109 (13.9) | 47 (13.7) | 57 (17.7) | 5 (4.3) |
| 41–50 | 157 (20.0) | 69 (20.1) | 58 (18.0) | 30 (25.6) |
| 51–60 | 208 (26.6) | 82 (23.8) | 90 (27.9) | 36 (30.8) |
| 61–70 | 173 (22.1) | 92 (26.7) | 55 (17.1) | 26 (22.2) |
| >70 | 136 (17.4) | 54 (15.7) | 62 (19.3) | 20 (17.1) |
| Sex: Male | 391 (50.0) | 179 (52.0) | 147 (45.6) | 65 (55.6) |
| Religion: Muslim | 726 (92.7) | 321 (93.3) | 296 (91.9) | 109 (93.2) |
| Profession | ||||
| Day labor | 24 (3.1) | 15 (4.4) | 3 (1.0) | 6 (5.1) |
| Business | 170 (21.7) | 82 (23.8) | 34 (10.5) | 54 (46.1) |
| Service | 153 (19.5) | 84 (24.4) | 38 (11.8) | 31 (26.5) |
| Housewife | 291 (37.2) | 118 (34.3) | 169 (52.5) | 4 (3.4) |
| Agriculture | 40 (5.1) | 9 (2.6) | 12 (3.7) | 19 (16.2) |
| No employment | 105 (13.4) | 30 (8.7) | 66 (20.5) | 3 (2.6) |
| Living place | ||||
| Rural | 400 (51.1) | 197 (57.3) | 148 (46.0) | 55 (47.0) |
| Urban | 383 (48.9) | 147 (42.7) | 174 (54.0) | 62 (53.0) |
| Had comorbidities | 652 (71.8) | 216 (62.8) | 256 (79.5) | 90 (76.9) |
| Hospitalization status, by vaccine | ||||
| Unvaccinated | 587 (75.0) | 255 (74.1) | 301 (93.5) | 31 (26.5) |
| Vaccinated (any dose) | 196 (25.0) | 89 (25.9) | 21 (6.5) | 86 (73.5) |
| COVID-19 Vaccination status | ||||
| Double doses | 124 (15.8) | 37 (10.8) | 19 (5.9) | 68 (58.1) |
| Single doses | 72 (9.2) | 52 (15.1) | 2 (0.6) | 18 (15.4) |
| Final Outcome | ||||
| Recovered and discharged | 721 (92.1) | 313 (91.0) | 294 (91.3) | 112 (95.7) |
| Died | 62 (7.9) | 29 (8.4) | 28 (8.7) | 5 (4.3) |
| Hospitalized Patients, by Vaccine | |||
|---|---|---|---|
| Total (N) | Unvaccinated n (%) | Vaccinated n (%) | |
| Gender | |||
| Male | 391 | 283 (72.4) | 108 (27.6) |
| Female | 392 | 303 (77.3) | 89 (22.7) |
| Living area | |||
| Urban | 383 | 269 (70.2) | 114 (29.8) |
| Rural | 400 | 317 (79.2) | 83 (20.8) |
| Had comorbidities | 562 | 414 (73.7) | 148 (26.3) |
| O2 required | 634 | 477 (75.2) | 157 (24.8) |
| ICU required | 244 | 184 (75.4) | 60 (24.6) |
| Severity | 187 | 138 (73.8) | 49 (26.2) |
| Died | 62 | 59 (95.2) | 3 (4.8) |
| UOR (95%CI) | p-Value | AOR (95%CI) | p-Value | |
|---|---|---|---|---|
| Age | ||||
| 25–40 | ref | ref | ||
| 41–50 | 1.29 (0.46–3.61) | 0.623 | 1.61 (0.55–4.73) | 0.388 |
| 51–60 | 0.69 (0.23–2.03) | 0.497 | 0.67 (0.22–2.11) | 0.512 |
| 61–70 | 1.63 (0.61–4.34) | 0.328 | 1.44 (0.51–4.02) | 0.488 |
| >70 | 3.31 (1.29–8.49) | 0.013 | 3.16 (1.16–8.58) | 0.024 |
| Hospitalization by vaccine | ||||
| Vaccinated | ref | ref | ||
| Unvaccinated | 7.19 (2.28–23.20) | 0.001 | 7.17 (2.21–23.27) | 0.001 |
| Had Comorbidities | ||||
| Vaccinated | ref | |||
| Unvaccinated | 10.72 (2.57–44.55) | 0.001 | 9.98 (2.39–41.68) | 0.002 |
| O2 required | ||||
| Vaccinated | ref | ref | ||
| Unvaccinated | 10.31 (2.49–42.75) | 0.001 | 10.25 (2.46–42.69) | 0.001 |
| ICU required | ||||
| Vaccinated | ref | ref | ||
| Unvaccinated | 6.81 (1.59–29.24) | 0.010 | 7.74 (1.78–33.74) | 0.006 |
| Severity | ||||
| Vaccinated | ref | ref | ||
| Unvaccinated | 6.53 (1.50–28.4) | 0.012 | 6.98 (1.57–30.92) | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, M.S.; Harun, M.G.D.; Sumon, S.A.; Mohona, T.M.; Abdullah, S.A.H.M.; Khan, M.N.H.; Gazi, M.I.; Islam, M.S.; Anwar, M.M.U. Hospitalization and Mortality by Vaccination Status among COVID-19 Patients Aged ≥ 25 Years in Bangladesh: Results from a Multicenter Cross-Sectional Study. Vaccines 2022, 10, 1987. https://doi.org/10.3390/vaccines10121987
Rahman MS, Harun MGD, Sumon SA, Mohona TM, Abdullah SAHM, Khan MNH, Gazi MI, Islam MS, Anwar MMU. Hospitalization and Mortality by Vaccination Status among COVID-19 Patients Aged ≥ 25 Years in Bangladesh: Results from a Multicenter Cross-Sectional Study. Vaccines. 2022; 10(12):1987. https://doi.org/10.3390/vaccines10121987
Chicago/Turabian StyleRahman, Md. Saydur, Md. Golam Dostogir Harun, Shariful Amin Sumon, Tahrima Mohsin Mohona, Syed Abul Hassan Md Abdullah, Md. Nazuml Huda Khan, Md. Ismail Gazi, Md. Saiful Islam, and Md. Mahabub Ul Anwar. 2022. "Hospitalization and Mortality by Vaccination Status among COVID-19 Patients Aged ≥ 25 Years in Bangladesh: Results from a Multicenter Cross-Sectional Study" Vaccines 10, no. 12: 1987. https://doi.org/10.3390/vaccines10121987