

Parental Willingness for COVID-19 Vaccination among Children Aged 5 to 11 Years in Riyadh City, Saudi Arabia: A Cross-Sectional Study

 , , , ,
, , , ,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Methodology
2.1. Study Setting and Design
2.2. Sampling Technique, Sample Size and Distribution of Study Tool
2.3. Development of Study Tool and Validation
2.4. Sections of the Study Tool
2.4.1. Demographic Details
2.4.2. Parental Behavior about COVID-19 and Immunization History of Child
2.4.3. Measuring Vaccine Hesitancy-Parents’ Willingness to Vaccinate Their Children against COVID-19
2.4.4. Parental Attitude and Vaccine Hesitancy Score (VHS) towards COVID-19 Vaccination in Children
2.4.5. Source of Information and Reasons Influencing Parents’ Intention to Vaccinate Their Children
2.5. Data Processing and Statistical Analysis
3. Results
3.1. Parents’ Willingness to Vaccinate Their Children against COVID-19
3.2. Vaccine Hesitancy Scale (VHS) and Attitude Regarding the Importance of Vaccinating Children against COVID-19
3.3. Parental Behavior towards COVID-19 Vaccination, Precautionary Measures, and Childhood Vaccination
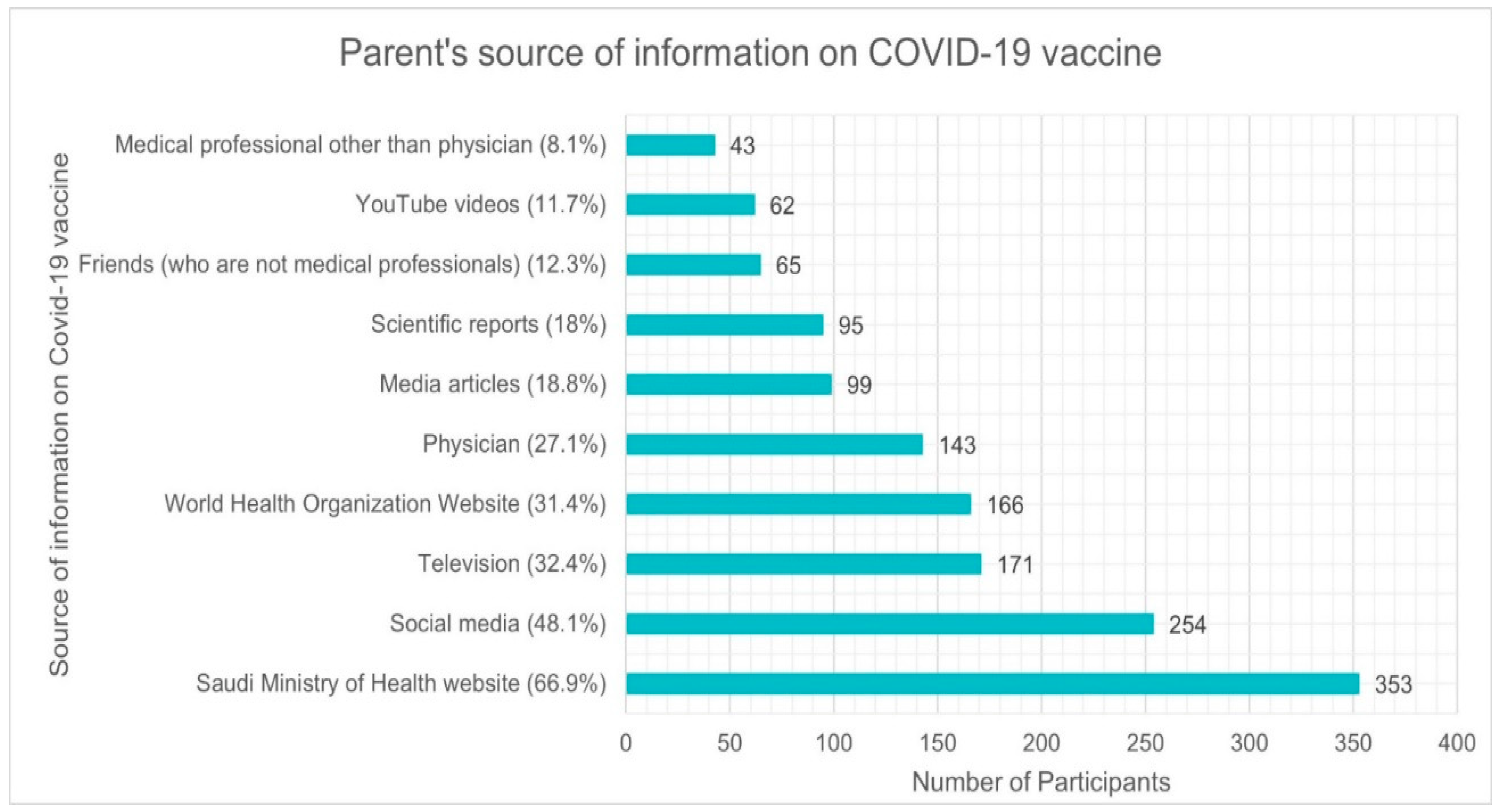
3.4. Parental Source of Information about COVID-19 Vaccine
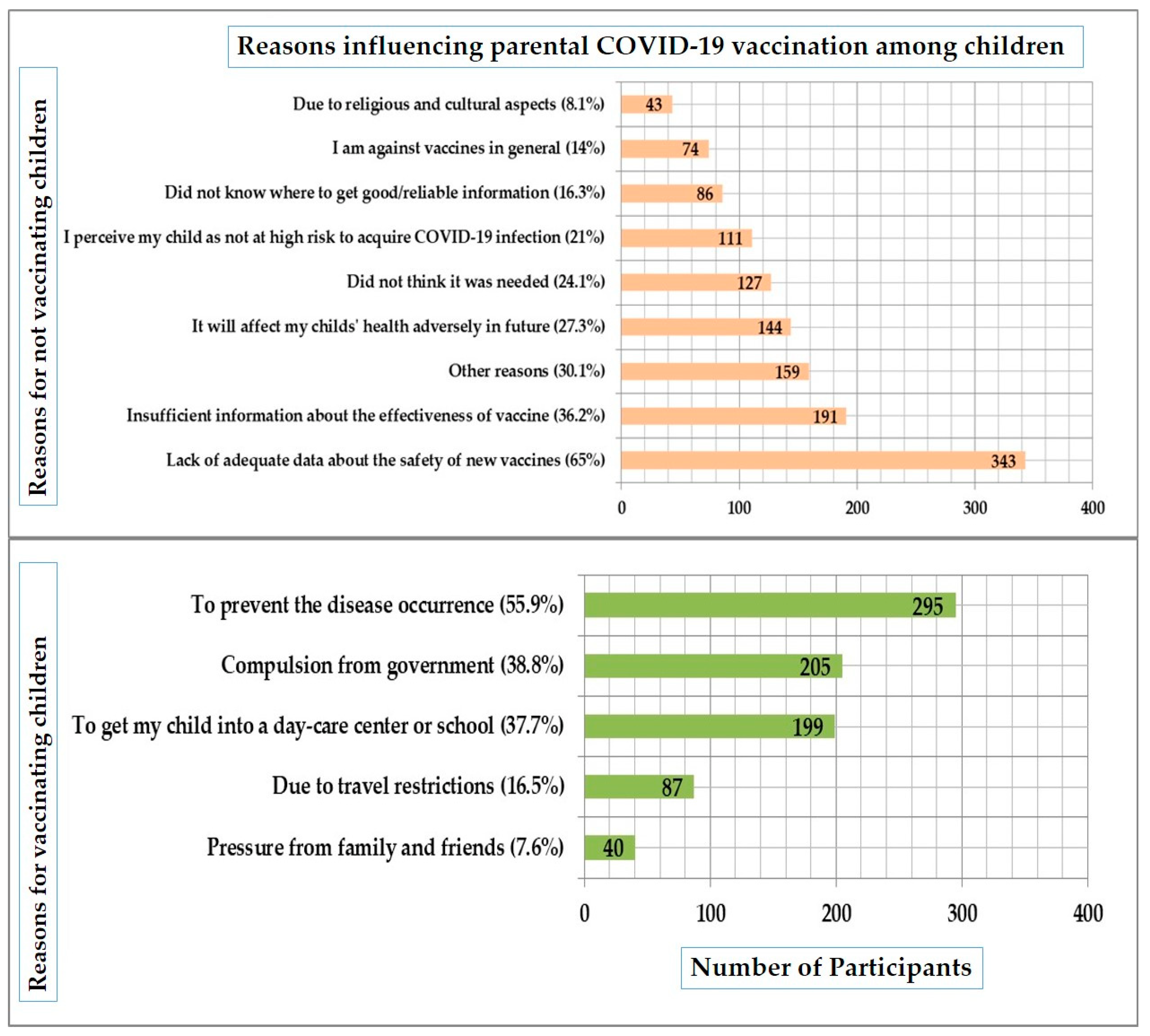
3.5. Reasons Influencing the Parent’s Decision to Vaccinate Their Children against COVID-19
3.6. Drivers of Parental COVID-19 Vaccine Hesitancy for Their Children
3.7. Binary Logistic Regression Analysis to Identify the Factors Associated with Parental COVID-19 Vaccine Hesitancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 10 September 2022).
- Coronavirus Disease (COVID-19): Vaccines. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-(covid-19)-vaccines?adgroupsurvey={adgroupsurvey}&gclid=CjwKCAjw1ICZBhAzEiwAFfvFhO0EZ608IAHK9hjXjSkZj7YATHPSbw3-uvQFScW3CRRIIsDaSnS6MBoC3dwQAvD_BwE (accessed on 10 September 2022).
- MacDonald, N.E. SAGE Working Group on Vaccine Hesitancy Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Ten Health Issues WHO Will Tackle This Year. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 10 September 2022).
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and Guardians’ Views on the Acceptability of a Future COVID-19 Vaccine: A Multi-Methods Study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Xiu, S.; Zhao, S.; Wang, J.; Han, Y.; Dong, S.; Huang, J.; Cui, T.; Yang, L.; Shi, N.; et al. Vaccine Hesitancy: COVID-19 and Influenza Vaccine Willingness among Parents in Wuxi, China-A Cross-Sectional Study. Vaccines 2021, 9, 342. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, M.; Sahin, M.K. Parents’ Willingness and Attitudes Concerning the COVID-19 Vaccine: A Cross-Sectional Study. Int. J. Clin. Pract. 2021, 75, e14364. [Google Scholar] [CrossRef] [PubMed]
- van Riel, D.; de Wit, E. Next-Generation Vaccine Platforms for COVID-19. Nat. Mater. 2020, 19, 810–812. [Google Scholar] [CrossRef]
- Caserotti, M.; Girardi, P.; Rubaltelli, E.; Tasso, A.; Lotto, L.; Gavaruzzi, T. Associations of COVID-19 Risk Perception with Vaccine Hesitancy over Time for Italian Residents. Soc. Sci. Med. 2021, 272, 113688. [Google Scholar] [CrossRef]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 Pathophysiology: A Review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef] [PubMed]
- Bonam, S.R.; Kotla, N.G.; Bohara, R.A.; Rochev, Y.; Webster, T.J.; Bayry, J. Potential Immuno-Nanomedicine Strategies to Fight COVID-19 like Pulmonary Infections. Nano Today 2021, 36, 101051. [Google Scholar] [CrossRef]
- Saudi Arabia: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/region/emro/country/sa (accessed on 10 September 2022).
- CDC COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker/ (accessed on 10 September 2022).
- Saudi Arabia Starts Giving Covid-19 Vaccines to Children Aged 5–11. Available online: https://saudigazette.com.sa/article/614992 (accessed on 10 September 2022).
- Ministry of Health Saudi Arabia. Available online: https://www.moh.gov.sa/en/CCC/Pages/default.aspx (accessed on 10 September 2022).
- Saudi Arabia Approves COVID-19 Vaccine for Kids Ages 5 to 11. Available online: https://www.arabnews.com/node/1961956/saudi-arabia (accessed on 12 November 2022).
- Brewer, N.T.; Chapman, G.B.; Rothman, A.J.; Leask, J.; Kempe, A. Increasing Vaccination: Putting Psychological Science into Action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef] [Green Version]
- Hussain, S.F.; Boyle, P.; Patel, P.; Sullivan, R. Eradicating Polio in Pakistan: An Analysis of the Challenges and Solutions to This Security and Health Issue. Global. Health 2016, 12, 63. [Google Scholar] [CrossRef]
- Riyadh Population 2022. Available online: https://worldpopulationreview.com/world-cities/riyadh-population (accessed on 10 January 2022).
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dube, E.; Schuster, M.; MacDonald, N.E.; Wilson, R. SAGE Working Group on Vaccine Hesitancy Measuring Vaccine Hesitancy: The Development of a Survey Tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temsah, M.-H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; Alhaboob, A.; Bashiri, F.A.; Alshaer, A.; Temsah, O.; et al. Parental Attitudes and Hesitancy about COVID-19 vs. Routine Childhood Vaccinations: A National Survey. Front. Public Health 2021, 9, 752323. [Google Scholar] [CrossRef] [PubMed]
- Kempe, A.; Saville, A.W.; Albertin, C.; Zimet, G.; Breck, A.; Helmkamp, L.; Vangala, S.; Dickinson, L.M.; Rand, C.; Humiston, S.; et al. Parental Hesitancy about Routine Childhood and Influenza Vaccinations: A National Survey. Pediatrics 2020, 146, e20193852. [Google Scholar] [CrossRef] [PubMed]
- Babicki, M.; Pokorna-Kałwak, D.; Doniec, Z.; Mastalerz-Migas, A. Attitudes of Parents with Regard to Vaccination of Children against COVID-19 in Poland. A Nationwide Online Survey. Vaccines 2021, 9, 1192. [Google Scholar] [CrossRef]
- Alfieri, N.L.; Kusma, J.D.; Heard-Garris, N.; Davis, M.M.; Golbeck, E.; Barrera, L.; Macy, M.L. Parental COVID-19 Vaccine Hesitancy for Children: Vulnerability in an Urban Hotspot. BMC Public Health 2021, 21, 1662. [Google Scholar] [CrossRef]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 Vaccine Acceptance among Pregnant Women and Mothers of Young Children: Results of a Survey in 16 Countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Ennaceur, S.; Al-Mohaithef, M. Parents’ Willingness to Vaccinate Children against COVID-19 in Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 156. [Google Scholar] [CrossRef]
- Rodrigues, C.M.C.; Plotkin, S.A. Impact of Vaccines; Health, Economic and Social Perspectives. Front. Microbiol. 2020, 11, 1526. [Google Scholar] [CrossRef]
- Schaffer DeRoo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458–2459. [Google Scholar] [CrossRef]
- Almalki, O.S.; Alfayez, O.M.; Al Yami, M.S.; Asiri, Y.A.; Almohammed, O.A. Parents’ Hesitancy to Vaccinate Their 5–11-Year-Old Children against COVID-19 in Saudi Arabia: Predictors from the Health Belief Model. Front. Public Health 2022, 10, 842862. [Google Scholar] [CrossRef]
- Horiuchi, S.; Sakamoto, H.; Abe, S.K.; Shinohara, R.; Kushima, M.; Otawa, S.; Yui, H.; Akiyama, Y.; Ooka, T.; Kojima, R.; et al. Factors of Parental COVID-19 Vaccine Hesitancy: A Cross Sectional Study in Japan. PLoS ONE 2021, 16, e0261121. [Google Scholar] [CrossRef]
- Aedh, A.I. Parents’Attitudes, Their Acceptance of the COVID-19 Vaccines for Children and the Contributing Factors in Najran, Saudi Arabia: A Cross-Sectional Survey. Vaccines 2022, 10, 1264. [Google Scholar] [CrossRef]
- Ali, M.; Ahmed, S.; Bonna, A.S.; Sarkar, A.-S.; Islam, M.A.; Urmi, T.A.; Proma, T.S. Parental Coronavirus Disease Vaccine Hesitancy for Children in Bangladesh: A Cross-Sectional Study. F1000Research 2022, 11, 90. [Google Scholar] [CrossRef]
- Coronavirus: Arab Countries Struggle with High Vaccine Hesitancy. Available online: https://www.dw.com/en/middle-east-covid-vaccine-rollout-hesitancy/a-57227395 (accessed on 10 September 2022).
- COVID-19 Anti-Vaxxers Can Derail Fight against Pandemic: UAE Health Experts. Available online: https://english.alarabiya.net/coronavirus/2021/08/10/COVID-19-anti-vaxxers-can-derail-fight-against-pandemic-UAE-health-experts (accessed on 10 September 2022).
- Doustmohammadi, S.; Cherry, J.D. The Sociology of the Antivaccine Movement. Emerg. Top. Life Sci. 2020, 4, 241–245. [Google Scholar] [CrossRef]
- Huynh, G.; Nguyen, H.T.N.; Van Tran, K.; Le An, P.; Tran, T.D. Determinants of COVID-19 Vaccine Hesitancy among Parents in Ho Chi Minh City, Vietnam. Postgrad. Med. 2022, 134, 303–308. [Google Scholar] [CrossRef]
- Li, T.; Qiu, X.; Gong, X.; Zhan, R.; Zheng, X. The Cross-Sectional Survey on COVID-19 Vaccine Hesitancy and It Predictors among Chinese Parents of 3–17 Years Aged Children in Shenzhen City. Ann. Agric. Environ. Med. 2022, 29, 120–125. [Google Scholar] [CrossRef]
- Giambi, C.; Fabiani, M.; D’Ancona, F.; Ferrara, L.; Fiacchini, D.; Gallo, T.; Martinelli, D.; Pascucci, M.G.; Prato, R.; Filia, A.; et al. Parental Vaccine Hesitancy in Italy–Results from a National Survey. Vaccine 2018, 36, 779–787. [Google Scholar] [CrossRef]
- Manolescu, L.S.C.; Zaharia, C.N.; Dumitrescu, A.I.; Prasacu, I.; Radu, M.C.; Boeru, A.C.; Boidache, L.; Nita, I.; Necsulescu, A.; Medar, C.; et al. COVID-19 Parental Vaccine Hesitancy in Romania: Nationwide Cross-Sectional Study. Vaccines 2022, 10, 493. [Google Scholar] [CrossRef]
- Saudi Arabia Requires Students to Receive Vaccinations before Start of School Year. Available online: https://english.alarabiya.net/coronavirus/2021/08/01/Saudi-Arabia-requires-students-to-receive-vaccinations-before-start-of-school-year (accessed on 8 September 2022).




{kind=link}
{kind=link}
{kind=link}
| Demographic Information- n = 528 | |||
|---|---|---|---|
| Characteristics | Category | Number (n) | Percentage (%) |
| Parent Age | 25 years and below | 41 | 7.8 |
| 26 to 40 years | 358 | 67.8 | |
| 41 years and above | 129 | 24.4 | |
| Relationship with Child | Father | 118 | 22.3 |
| Mother | 410 | 77.7 | |
| Nationality | Saudi | 508 | 96.2 |
| Non-Saudi | 20 | 3.8 | |
| Marital Status | Married | 483 | 91.5 |
| Divorced or separated | 45 | 8.5 | |
| Parents Education | High school or less | 99 | 18.8 |
| College degree | 373 | 70.6 | |
| Postgraduate or higher | 56 | 10.6 | |
| Family’s Monthly Income | Less than SAR 5000 | 28 | 5.3 |
| SAR 5000 to 10,000 | 116 | 22.0 | |
| more than SAR 10,000 | 245 | 46.4 | |
| Prefer not to answer | 139 | 26.3 | |
| Are you a Healthcare professional? | Yes | 81 | 15.3 |
| No | 447 | 84.7 | |
| Job Sector | Government | 178 | 33.7 |
| Private | 115 | 21.8 | |
| Self-Employed | 39 | 7.4 | |
| Unemployed | 16 | 3.0 | |
| Retired | 27 | 5.1 | |
| Housewife | 146 | 27.7 | |
| Student | 7 | 1.3 | |
| Number of Children | One | 61 | 11.6 |
| Two | 109 | 20.6 | |
| Three | 123 | 23.3 | |
| Four | 113 | 21.4 | |
| Five and above | 122 | 23.1 | |
| Children of 5–11 years age | Yes | 467 | 88.4 |
| No | 61 | 11.6 | |
| Gender of children | Only boys | 115 | 21.8 |
| Only girls | 114 | 21.6 | |
| Both boys and girls | 299 | 56.6 | |
| Children with chronic diseases? | Yes | 113 | 21.4 |
| No | 415 | 78.6 | |
| Willingness to Vaccinate Children Against COVID-19 | |||||||
|---|---|---|---|---|---|---|---|
| Variables | Sub-Group | Not Willing to Vaccinate (%) | Undecided (%) | Delay for a Year and Above (%) | Delay for Few Months (%) | Yes, as soon as Possible (%) | p Value |
| Parent Age | 25 years and below | 11 (26.8) | 10 (24.4) | 7 (17.1) | 3 (7.3) | 10 (24.4) | 0.206 |
| 26 to 40 years | 151 (42.2) | 86 (24) | 51 (14.2) | 22 (6.1) | 48 (13.4) | ||
| 41 years and above | 41 (31.8) | 29 (22.5) | 21 (16.3) | 10 (7.8) | 28 (21.7) | ||
| Relationship with Child | Father | 32 (27.1) | 27 (22.9) | 22 (18.6) | 15 (12.7) | 22 (18.6) | 0.004 * |
| Mother | 171 (41.7) | 98 (23.9) | 57 (13.9) | 20 (4.9) | 64 (15.6) | ||
| Nationality | Saudi | 196 (38.6) | 120 (23.6) | 75 (14.8) | 34 (6.7) | 83 (16.3) | 0.972 |
| Non-Saudi | 7 (35) | 5 (25) | 4 (20) | 1 (5) | 3 (15) | ||
| Marital Status | Married | 187 (38.7) | 117 (24.2) | 72 (14.9) | 31 (6.4) | 76 (15.7) | 0.696 |
| Divorced or separated | 16 (35.6) | 8 (17.8) | 7 (15.6) | 4 (8.9) | 10 (22.2) | ||
| Parents Education | High school or less | 32 (32.3) | 20 (20.2) | 20 (20.2) | 11 (11.1) | 16 (16.2) | 0.198 |
| College degree | 149 (39.9) | 94 (25.2) | 52 (13.9) | 22 (5.9) | 56 (15) | ||
| Postgraduate or higher | 22 (39.3) | 11 (19.6) | 7 (12.5) | 2 (3.6) | 14 (25) | ||
| Family’s Monthly Income | Less than SAR 5000 | 10 (35.7) | 7 (25) | 5 (17.9) | 1 (3.6) | 5 (17.9) | 0.023 * |
| SAR 5000 to 10,000 | 35 (30.2) | 36 (31) | 21 (18.1) | 12 (10.3) | 12 (10.3) | ||
| more than SAR 10,000 | 89 (36.3) | 57 (23.3) | 32 (13.1) | 17 (6.9) | 50 (20.4) | ||
| Prefer not to answer | 69 (49.6) | 25 (18) | 21 (15.1) | 5 (3.6) | 19 (13.7) | ||
| Are you a Healthcare professional? | Yes | 16 (19.8) | 18 (22.2) | 16 (19.8) | 8 (9.9) | 23 (28.4) | <0.001 * |
| No | 187 (41.8) | 107 (23.9) | 63 (14.1) | 27 (6) | 63 (14.1) | ||
| Job Sector | Government | 62 (34.8) | 37 (20.8) | 31 (17.4) | 10 (5.6) | 38 (21.3) | 0.040 * |
| Private | 32 (27.8) | 29 (25.2) | 17 (14.8) | 14 (12.2) | 23 (20) | ||
| Self-Employed | 15 (38.5) | 9 (23.1) | 6 (15.4) | 4 (10.3) | 5 (12.8) | ||
| Unemployed | 9 (56.3) | 2 (12.5) | 2 (12.5) | 1 (6.3) | 2 (12.5) | ||
| Retired | 11 (40.7) | 9 (33.3) | 2 (7.4) | Zero | 5 (18.5) | ||
| Housewife | 70 (47.9) | 38 (26) | 20 (13.7) | 6 (4.1) | 12 (8.2) | ||
| Student | 4 (57.1) | 1 (14.3) | 1 (14.3) | Zero | 1 (14.3) | ||
| Number of Children | One | 29 (47.5) | 10 (16.4) | 7 (11.5) | 2 (3.3) | 13 (21.3) | 0.330 |
| Two | 37 (33.9) | 27 (24.8) | 18 (16.5) | 12 (11) | 15 (13.8) | ||
| Three | 41 (33.3) | 30 (24.4) | 19 (15.4) | 8 (6.5) | 25 (20.3) | ||
| Four | 40 (35.4) | 28 (24.8) | 22 (19.5) | 6 (5.3) | 17 (15) | ||
| Five and above | 56 (45.9) | 30 (24.6) | 13 (10.7) | 7 (5.7) | 16 (13.1) | ||
| Children of 5–11 years age | Yes | 185 (39.6) | 110 (23.6) | 69 (14.8) | 31 (6.6) | 72 (15.4) | 0.488 |
| No | 18 (29.5) | 15 (24.6) | 10 (16.4) | 4 (6.6) | 14 (23) | ||
| Gender of children | Only boys | 51 (44.3) | 20 (17.4) | 17 (14.8) | 10 (8.7) | 17 (14.8) | 0.401 |
| Only girls | 36 (31.6) | 32 (28.1) | 15 (13.2) | 9 (7.9) | 22 (19.3) | ||
| Both boys and girls | 116 (38.8) | 73 (24.4) | 47 (15.7) | 16 (5.4) | 47 (15.7) | ||
| Children with chronic diseases? | Yes | 35 (31) | 22 (19.5) | 20 (17.7) | 14 (12.4) | 22 (19.5) | 0.018 * |
| No | 168 (40.5) | 103 (24.8) | 59 (14.2) | 21 (5.1) | 64 (15.4) | ||
| Parental Behavior, Immunization and Precautionary Measures Related to COVID-19 | |||
|---|---|---|---|
| Participant’s Response | Frequency | Percentage (%) | |
| Have you ever heard about or seen the campaign against COVID- 19 vaccination (anti-vaccination movements)? | Yes | 328 | 62.1 |
| No | 200 | 37.9 | |
| Describe your family’s commitment to the precautionary measures against the COVID-19? | No commitment | 55 | 10.4 |
| Little commitment | 191 | 36.2 | |
| Somewhat commitment | 150 | 28.4 | |
| Much committed | 118 | 22.3 | |
| Great deal of commitment | 14 | 2.7 | |
| Did anyone within your direct family get infected with COVID-19? | Yes | 399 | 75.6 |
| No | 129 | 24.4 | |
| How severe were the symptoms of the infected person(s)? | Very mild/asymptomatic | 46 | 11.5 |
| Mild | 96 | 24.1 | |
| Moderate | 156 | 39.1 | |
| Severe | 93 | 23.3 | |
| Death | 8 | 2.0 | |
| As a parent did you take the COVID-19 vaccine? | Yes | 488 | 92.4 |
| No | 40 | 7.6 | |
| Did you get any adverse reaction after vaccination? | Mild | 167 | 31.6 |
| Moderate | 286 | 54.2 | |
| Severe | 35 | 6.6 | |
| Child/Children’s immunization history | |||
| Have you vaccinated your child with mandatory childhood vaccines? | Yes | 411 | 77.8 |
| No | 117 | 22.2 | |
| Adverse reactions after vaccination in child? | Mild | 176 | 42.8 |
| Moderate | 194 | 47.2 | |
| Severe | 41 | 10.0 | |
| Driver | Responses | Intention to Vaccinate a Child Against COVID-19 | |||||
|---|---|---|---|---|---|---|---|
| Not Willing to Vaccinate (%) | Undecided (%) | Delay for a Year and above (%) | Delay for Few Months (%) | Yes as Soon as Possible (%) | p Value | ||
| Have you ever heard about or seen the campaign against COVID-19 vaccination (anti-vaccination movements)? | Yes | 118 (36) | 70 (21.3) | 49 (14.9) | 24 (7.3) | 67 (20.4) | 0.011 * |
| No | 85 (42.5) | 55 (27.5) | 30 (15) | 11 (5.5) | 19 (9.5) | ||
| As a parent did you take the COVID-19 vaccine? | Yes | 186 (38.1) | 115 (23.6) | 69 (14.1) | 33 (6.8) | 85 (17.4) | 0.079 |
| No | 17 (42.5) | 10 (25) | 10 (25) | 2 (5.0) | 1 (2.5) | ||
| Describe your family’s commitment to the precautionary measures against the COVID-19 | No commitment | 19 (34.5) | 16 (29.1) | 10 (18.2) | 3 (5.5) | 7 (12.7) | 0.407 |
| Little commitment | 68 (35.6) | 48 (25.1) | 32 (16.8) | 14 (7.3) | 29 (15.2) | ||
| Somewhat commitment | 53 (35.3) | 37 (24.7) | 23 (15.3) | 7 (4.7) | 30 (20) | ||
| Much committed | 57 (48.3) | 20 (16.9) | 12 (10.2) | 9 (7.6) | 20 (16.9) | ||
| Great deal of commitment | 6 (42.9) | 4 (28.6) | 2 (14.3) | 2 (14.3) | 0 (0.0%) | ||
| Did anyone within your direct family get infected with COVID-19? | Yes | 151 (37.8) | 89 (22.3) | 61 (15.3) | 30 (7.5) | 68 (17.0) | 0.395 |
| No | 52 (40.3) | 36 (27.9) | 18 (14.0) | 5 (3.9%) | 18 (14.0) | ||
| Previous vaccination in child: Have you vaccinated your child with mandatory childhood vaccines? | Yes | 140 (34.1) | 97 (23.6) | 65 (15.8) | 29 (7.1) | 80 (19.5) | <0.001 * |
| No | 63 (53.8) | 28 (23.9) | 14 (12.0) | 6 (5.1) | 6 (5.1) | ||
| Independent Variables | Variable Coefficient (B) | p-Value | OR (95% CI) Unadjusted a | OR (95% CI) Adjusted b |
|---|---|---|---|---|
| Parental Vaccine Hesitancy against COVID-19 (YES) | ||||
| Parents relationship with child | ||||
| Father | 0.105 | 0.736 | 0.807 (0.473–1.378) | 1.047 (0.572–1.918) |
| Mother | - | - | 1.00 | 1.00 |
| Family’s monthly income | ||||
| SAR <5000 | −0.555 | 0.349 | 0.728 (0.247–2.148) | 0.574 (0.180–1.832) |
| SAR 5000–10,000 | 0.419 | 0.316 | 1.372 (0.636–2.961) | 1.520 (0.670–3.448) |
| SAR >10,000 | −0.211 | 0.509 | 0.618 (0.347–1.097) | 0.810 (0.434–1.513) |
| Prefer not to disclose | - | - | 1.00 | 1.00 |
| Parent Working as Healthcare Professional | ||||
| Yes | −0.697 | 0.040 * | 0.414 (0.238–0.718) | 0.498 (0.264–0.942) |
| No | - | - | 1.00 | 1.00 |
| Job Sector | ||||
| Government | 0.497 | 0.666 | 0.614 (0.072–5.25) | 1.644 (0.172–15.74) |
| Private | 0.413 | 0.721 | 0.667 (0.076–5.814) | 1.51 (0.157–14.58) |
| Self employed | 0.703 | 0.568 | 1.133 (0.112–11.48) | 2.02 (0.181–22.6) |
| Unemployed | 1.10 | 0.423 | 1.167 (0.088–15.45) | 3.0 (0.204–44.18) |
| Retired | 0.569 | 0.647 | 0.733 (0.071–7.53) | 1.77 (0.155–20.12) |
| Housewife | 1.34 | 0.248 | 1.861 (0.207–16.76) | 3.82 (0.394–37.07) |
| Student | - | - | 1.00 | 1.00 |
| Children suffering from chronic disease | ||||
| Yes | −0.226 | 0.454 | 0.754 (0.441–1.29) | 0.798 (0.442–1.44) |
| No | - | - | 1.00 | 1.00 |
| Anti-vaccine campaign | ||||
| Yes | −0.993 | 0.001 * | 0.409 (0.237–0.704) | 0.371 (0.210–0.654) |
| No | - | - | 1.00 | 1.00 |
| Mandatory childhood Immunization | ||||
| Yes | −1.614 | <0.001 * | 0.224 (0.095–0.527) | 0.199 (0.081–0.488) |
| No | - | - | 1.00 | 1.00 |
| Vaccine Hesitancy score (VHS) | ||||
| Hesitant: VHS score <3 points | 0.458 | 0.083 | 0.594 (0.366–0.964) | 0.633 (0.377–1.062) |
| Not Hesitant: VHS score ≥3 points | - | - | 1.00 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Qahtani, A.M.; Mannasaheb, B.A.; Shaikh, M.A.K.; Alajlan, S.A.; Alayed, M.S.Z.; Shaikh, I.A.; Asdaq, S.M.B.; Al-Qahtani, F.S.; Ghazwani, E.Y.; Al-Qahtani, N.S.; et al. Parental Willingness for COVID-19 Vaccination among Children Aged 5 to 11 Years in Riyadh City, Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 1979. https://doi.org/10.3390/vaccines10121979
Al-Qahtani AM, Mannasaheb BA, Shaikh MAK, Alajlan SA, Alayed MSZ, Shaikh IA, Asdaq SMB, Al-Qahtani FS, Ghazwani EY, Al-Qahtani NS, et al. Parental Willingness for COVID-19 Vaccination among Children Aged 5 to 11 Years in Riyadh City, Saudi Arabia: A Cross-Sectional Study. Vaccines. 2022; 10(12):1979. https://doi.org/10.3390/vaccines10121979
Chicago/Turabian StyleAl-Qahtani, Awad Mohammed, Basheerahmed Abdulaziz Mannasaheb, Mohammed Ashique K. Shaikh, Sarah Abdulrahman Alajlan, Mohammed Saeed Z. Alayed, Ibrahim Ahmed Shaikh, Syed Mohammed Basheeruddin Asdaq, Faisal Saeed Al-Qahtani, Eisa Yazeed Ghazwani, Nasser Saeed Al-Qahtani, and et al. 2022. "Parental Willingness for COVID-19 Vaccination among Children Aged 5 to 11 Years in Riyadh City, Saudi Arabia: A Cross-Sectional Study" Vaccines 10, no. 12: 1979. https://doi.org/10.3390/vaccines10121979