
Antioxidant Supplementation on Male Fertility—A Systematic Review
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Strategy
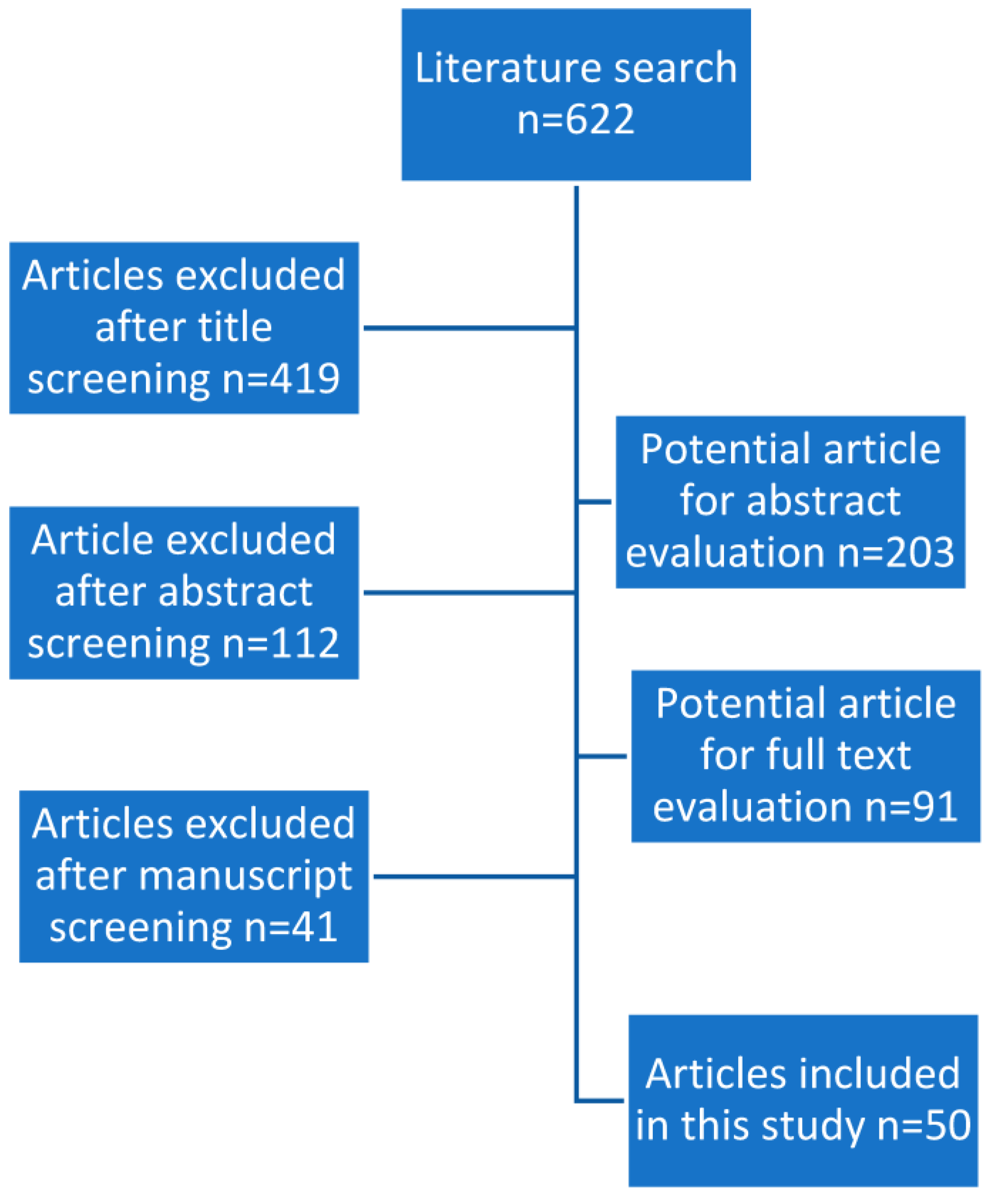
2.2. Study Selection
2.3. Outcome Measures
2.4. Results
3. Discussion
3.1. Vitamin E + Vitamin C
3.2. Carnitine
3.3. Coenzyme Q10 (CoQ10)
3.4. Zinc
3.5. Selenium and N-Acetyl-Cysteine
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brugh, V.M.; Lipshultz, L.I. Male Factor Infertility Evaluation and Management. Med. Clin. N. Am. 2004, 88, 367–385. [Google Scholar] [CrossRef] [PubMed]
- Irvine, D.S. Epidemiology and Aetiology of Male Infertility. Hum. Reprod. 1998, 13, 33–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharlip, I.D.; Jarow, J.P.; Belker, A.M.; Lipshultz, L.I.; Sigman, M.; Thomas, A.J.; Schlegel, P.N.; Howards, S.S.; Nehra, A.; Damewood, M.D.; et al. Best Practice Policies for Male Infertility. Fertil. Steril. 2002, 77, 873–882. [Google Scholar] [CrossRef]
- Wong, W.Y.; Thomas, C.M.G.; Merkus, J.M.W.M.; Zielhuis, G.A.; Steegers-Theunissen, R.P.M. Male Factor Subfertility: Possible Causes and the Impact of Nutritional Factors. Fertil. Steril. 2000, 73, 435–442. [Google Scholar] [CrossRef]
- Dimitriadis, F.; Symeonidis, E.N.; Tsounapi, P.; Kaltsas, A.; Hatzichristodoulou, G.; Sokolakis, I.; Zachariou, A.; Takenaka, A.; Sofikitis, N. Administration of Antioxidants in Infertile Male: When It May Have a Detrimental Effect? Curr. Pharm. Des. 2021, 27, 2796–2801. [Google Scholar] [CrossRef]
- Dimitriadis, F.; Kaltsas, A.; Zachariou, A.; Mamoulakis, C.; Tsiampali, C.; Giannakis, I.; Paschopoulos, M.; Papatsoris, A.; Loutradis, D.; Tsounapi, P.; et al. PDE5 Inhibitors and Male Reproduction: Is There a Place for PDE5 Inhibitors in Infertility Clinics or Andrology Laboratories? Int. J. Urol. 2022, 29, 1405–1418. [Google Scholar] [CrossRef]
- Tremellen, K. Oxidative Stress and Male Infertility—A Clinical Perspective. Hum. Reprod. Updat. 2008, 14, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Symeonidis, E.N.; Evgeni, E.; Palapelas, V.; Koumasi, D.; Pyrgidis, N.; Sokolakis, I.; Hatzichristodoulou, G.; Tsiampali, C.; Mykoniatis, I.; Zachariou, A.; et al. Redox Balance in Male Infertility: Excellence through Moderation—“Μέτρον Ἄριστον”. Antioxidants 2021, 10, 1534. [Google Scholar] [CrossRef]
- Sakkas, D.; Mariethoz, E.; Manicardi, G.; Bizzaro, D.; Bianchi, P.G.; Bianchi, U. Origin of DNA Damage in Ejaculated Human Spermatozoa. Rev. Reprod. 1999, 4, 31–37. [Google Scholar] [CrossRef]
- Montano, L.; Maugeri, A.; Volpe, M.G.; Micali, S.; Mirone, V.; Mantovani, A.; Navarra, M.; Piscopo, M. Mediterranean Diet as a Shield against Male Infertility and Cancer Risk Induced by Environmental Pollutants: A Focus on Flavonoids. Int. J. Mol. Sci. 2022, 23, 1568. [Google Scholar] [CrossRef]
- Perrone, P.; Lettieri, G.; Marinaro, C.; Longo, V.; Capone, S.; Forleo, A.; Pappalardo, S.; Montano, L.; Piscopo, M. Molecular Alterations and Severe Abnormalities in Spermatozoa of Young Men Living in the “Valley of Sacco River” (Latium, Italy): A Preliminary Study. Int. J. Environ. Res. Public Health 2022, 19, 11023. [Google Scholar] [CrossRef] [PubMed]
- Saleh, R.A.; Agarwal, A. Oxidative Stress and Male Infertility: From Research Bench to Clinical Practice. J. Androl. 2002, 23, 737–752. [Google Scholar] [PubMed]
- Agarwal, A.; Said, T.M. Oxidative Stress, DNA Damage and Apoptosis in Male Infertility: A Clinical Approach. BJU Int. 2005, 95, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Makker, K.; Agarwal, A.; Sharma, R. Oxidative Stress & Male Infertility. Indian J. Medical. Res. 2009, 129, 357–367. [Google Scholar]
- Lafuente, R.; González-Comadrán, M.; Solà, I.; López, G.; Brassesco, M.; Carreras, R.; Checa, M.A. Coenzyme Q10 and Male Infertility: A Meta-Analysis. J. Assist. Reprod. Genet. 2013, 30, 1147–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheweita, S.; Tilmisany, A.; Al-Sawaf, H. Mechanisms of Male Infertility: Role of Antioxidants. Curr. Drug Metab. 2005, 6, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Hosen, M.B.; Islam, M.R.; Begum, F.; Kabir, Y.; Howlader, M.Z.H. Oxidative Stress Induced Sperm DNA Damage, a Possible Reason for Male Infertility. Iran J. Reprod. Med. 2015, 13, 525–532. [Google Scholar] [PubMed]
- Sukcharoen, N.; Keith, J.; Irvine, D.S.; Aitken, R.J. Predicting the Fertilizing Potential of Human Sperm Suspensions in Vitro: Importance of Sperm Morphology and Leukocyte Contamination. Fertil. Steril. 1995, 63, 1293–1300. [Google Scholar] [CrossRef]
- Agarwal, A.; Sharma, R.K.; Nallella, K.P.; Thomas, A.J.; Alvarez, J.G.; Sikka, S.C. Reactive Oxygen Species as an Independent Marker of Male Factor Infertility. Fertil. Steril. 2006, 86, 878–885. [Google Scholar] [CrossRef]
- Linster, C.L.; Schaftingen, E.V. Vitamin C. FEBS J. 2007, 274, 1–22. [Google Scholar] [CrossRef]
- Omu, A.E.; Al-Azemi, M.K.; Kehinde, E.O.; Anim, J.T.; Oriowo, M.A.; Mathew, T.C. Indications of the Mechanisms Involved in Improved Sperm Parameters by Zinc Therapy. Med. Prin. Pr. 2008, 17, 108–116. [Google Scholar] [CrossRef]
- Abad, C.; Amengual, M.J.; Gosálvez, J.; Coward, K.; Hannaoui, N.; Benet, J.; García-Peiró, A.; Prats, J. Effects of Oral Antioxidant Treatment upon the Dynamics of Human Sperm DNA Fragmentation and Subpopulations of Sperm with Highly Degraded DNA. Andrologia 2013, 45, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Gvozdjáková, A.; Kucharská, J.; Dubravicky, J.; Mojto, V.; Singh, R.B. Coenzyme Q10, α-Tocopherol, and Oxidative Stress Could Be Important Metabolic Biomarkers of Male Infertility. Dis. Markers 2015, 2015, 827941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brigelius-Flohé, R.; Traber, M.G. Vitamin E: Function and Metabolism. FASEB J 1999, 13, 1145–1155. [Google Scholar] [CrossRef]
- Safarinejad, M.R.; Safarinejad, S. Efficacy of Selenium and/or N-Acetyl-Cysteine for Improving Semen Parameters in Infertile Men: A Double-Blind, Placebo Controlled, Randomized Study. J. Urol. 2009, 181, 741–751. [Google Scholar] [CrossRef]
- Khan, M.S.; Zaman, S.; Sajjad, M.; Shoaib, M.; Gilani, G. Assessment of the Level of Trace Element Zinc in Seminal Plasma of Males and Evaluation of Its Role in Male Infertility. Int. J. Appl. Basic Med. Res. 2011, 1, 93–96. [Google Scholar] [CrossRef] [Green Version]
- Sigman, M.; Glass, S.; Campagnone, J.; Pryor, J.L. Carnitine for the Treatment of Idiopathic Asthenospermia: A Randomized, Double-Blind, Placebo-Controlled Trial. Fertil. Steril. 2006, 85, 1409–1414. [Google Scholar] [CrossRef]
- Nadjarzadeh, A.; Sadeghi, M.R.; Amirjannati, N.; Vafa, M.R.; Motevalian, S.A.; Gohari, M.R.; Akhondi, M.A.; Yavari, P.; Shidfar, F. Coenzyme Q10 Improves Seminal Oxidative Defense but Does Not Affect on Semen Parameters in Idiopathic Oligoasthenoteratozoospermia: A Randomized Double-Blind, Placebo Controlled Trial. J. Endocrinol. Investig. 2011, 34, e224–e228. [Google Scholar] [CrossRef]
- Ciftci, H.; Verit, A.; Savas, M.; Yeni, E.; Erel, O. Effects of N-Acetylcysteine on Semen Parameters and Oxidative/Antioxidant Status. Urology 2009, 74, 73–76. [Google Scholar] [CrossRef]
- Gupta, N.P.; Kumar, R. Lycopene Therapy in Idiopathic Male Infertility—A Preliminary Report. Int. Urol. Nephrol. 2002, 34, 369–372. [Google Scholar] [CrossRef]
- Boitrelle, F.; Shah, R.; Saleh, R.; Henkel, R.; Kandil, H.; Chung, E.; Vogiatzi, P.; Zini, A.; Arafa, M.; Agarwal, A. The Sixth Edition of the WHO Manual for Human Semen Analysis: A Critical Review and SWOT Analysis. Life 2021, 11, 1368. [Google Scholar] [CrossRef] [PubMed]
- Jungwirth, A.; Giwercman, A.; Tournaye, H.; Diemer, T.; Kopa, Z.; Dohle, G.; Krausz, C.; Infertility, E.W.G. on M. European Association of Urology Guidelines on Male Infertility: The 2012 Update. Eur. Urol. 2012, 62, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Galatioto, G.P.; Gravina, G.L.; Angelozzi, G.; Sacchetti, A.; Innominato, P.F.; Pace, G.; Ranieri, G.; Vicentini, C. May Antioxidant Therapy Improve Sperm Parameters of Men with Persistent Oligospermia after Retrograde Embolization for Varicocele? World J. Urol. 2008, 26, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Garolla, A.; Maiorino, M.; Roverato, A.; Roveri, A.; Ursini, F.; Foresta, C. Oral Carnitine Supplementation Increases Sperm Motility in Asthenozoospermic Men with Normal Sperm Phospholipid Hydroperoxide Glutathione Peroxidase Levels. Fertil. Steril. 2005, 83, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Safarinejad, M.R. The Effect of Coenzyme Q10 Supplementation on Partner Pregnancy Rate in Infertile Men with Idiopathic Oligoasthenoteratozoospermia: An Open-Label Prospective Study. Int. Urol. Nephrol. 2012, 44, 689–700. [Google Scholar] [CrossRef]
- Balercia, G.; Buldreghini, E.; Vignini, A.; Tiano, L.; Paggi, F.; Amoroso, S.; Ricciardo-Lamonica, G.; Boscaro, M.; Lenzi, A.; Littarru, G. Coenzyme Q10 Treatment in Infertile Men with Idiopathic Asthenozoospermia: A Placebo-Controlled, Double-Blind Randomized Trial. Fertil. Steril. 2009, 91, 1785–1792. [Google Scholar] [CrossRef]
- Wong, W.Y.; Merkus, H.M.W.M.; Thomas, C.M.G.; Menkveld, R.; Zielhuis, G.A.; Steegers-Theunissen, R.P.M. Effects of Folic Acid and Zinc Sulfate on Male Factor Subfertility: A Double-Blind, Randomized, Placebo-Controlled Trial. Fertil. Steril. 2002, 77, 491–498. [Google Scholar] [CrossRef]
- Safarinejad, M.R. Efficacy of Coenzyme Q10 on Semen Parameters, Sperm Function and Reproductive Hormones in Infertile Men. J. Urol. 2009, 182, 237–248. [Google Scholar] [CrossRef]
- Safarinejad, M.R.; Safarinejad, S.; Shafiei, N.; Safarinejad, S. Effects of the Reduced Form of Coenzyme Q10 (Ubiquinol) on Semen Parameters in Men with Idiopathic Infertility: A Double-Blind, Placebo Controlled, Randomized Study. J. Urol. 2012, 188, 526–531. [Google Scholar] [CrossRef] [Green Version]
- Moslemi, M.K.; Tavanbakhsh, S. Selenium–Vitamin E Supplementation in Infertile Men: Effects on Semen Parameters and Pregnancy Rate. Int. J. Gen. Med. 2011, 4, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Lenzi, A.; Sgrò, P.; Salacone, P.; Paoli, D.; Gilio, B.; Lombardo, F.; Santulli, M.; Agarwal, A.; Gandini, L. A Placebo-Controlled Double-Blind Randomized Trial of the Use of Combined l-Carnitine and l-Acetyl-Carnitine Treatment in Men with Asthenozoospermia. Fertil. Steril. 2004, 81, 1578–1584. [Google Scholar] [CrossRef] [PubMed]
- Balercia, G.; Regoli, F.; Armeni, T.; Koverech, A.; Mantero, F.; Boscaro, M. Placebo-Controlled Double-Blind Randomized Trial on the Use of l-Carnitine, l-Acetylcarnitine, or Combined l-Carnitine and l-Acetylcarnitine in Men with Idiopathic Asthenozoospermia. Fertil. Steril. 2005, 84, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Cavallini, G.; Ferraretti, A.P.; Gianaroli, L.; Biagiotti, G.; Vitali, G. Cinnoxicam and L-Carnitine/Acetyl-l-Carnitine Treatment for Idiopathic and Varicocele-Associated Oligoasthenospermia. J. Androl. 2004, 25, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Greco, E.; Iacobelli, M.; Rienzi, L.; Ubaldi, F.; Ferrero, S.; Tesarik, J. Reduction of the Incidence of Sperm DNA Fragmentation by Oral Antioxidant Treatment. J. Androl. 2005, 26, 349–353. [Google Scholar] [CrossRef]
- Omu, A.E.; Dashti, H.; Al-Othman, S. Treatment of Asthenozoospermia with Zinc Sulphate: Andrological, Immunological and Obstetric Outcome. Eur. J. Obs. Gynecol. Reprod. Biol. 1998, 79, 179–184. [Google Scholar] [CrossRef]
- Ménézo, Y.J.; Hazout, A.; Panteix, G.; Robert, F.; Rollet, J.; Cohen-Bacrie, P.; Chapuis, F.; Clément, P.; Benkhalifa, M. Antioxidants to Reduce Sperm DNA Fragmentation: An Unexpected Adverse Effect. Reprod. Biomed. Online 2007, 14, 418–421. [Google Scholar] [CrossRef]
- Keskes-Ammar, L.; Feki-Chakroun, N.; Rebai, T.; Sahnoun, Z.; Ghozzi, H.; Hammami, S.; Zghal, K.; Fki, H.; Damak, J.; Bahloul, A. SPERM OXIDATIVE STRESS AND THE EFFECT OF AN ORAL VITAMIN E AND SELENIUM SUPPLEMENT ON SEMEN QUALITY IN INFERTILE MEN. Arch Androl. 2003, 49, 83–94. [Google Scholar] [CrossRef]
- Tremellen, K.; Miari, G.; Froiland, D.; Thompson, J. A Randomised Control Trial Examining the Effect of an Antioxidant (Menevit) on Pregnancy Outcome during IVF-ICSI Treatment. Aust. N. Z. J. Obstet. Gynaecol. 2007, 47, 216–221. [Google Scholar] [CrossRef]
- Kessopoulou, E.; Powers, H.J.; Sharma, K.K.; Pearson, M.J.; Russell, J.M.; Cooke, I.D.; Barratt, C.L.R. A Double-Blind Randomized Placebo Cross-over Controlled Trial Using the Antioxidant Vitamin E to Treat Reactive Oxygen Species Associated Male Infertility. Fertil Steril. 1995, 64, 825–831. [Google Scholar] [CrossRef]
- Gual-Frau, J.; Abad, C.; Amengual, M.J.; Hannaoui, N.; Checa, M.A.; Ribas-Maynou, J.; Lozano, I.; Nikolaou, A.; Benet, J.; García-Peiró, A.; et al. Oral Antioxidant Treatment Partly Improves Integrity of Human Sperm DNA in Infertile Grade I Varicocele Patients. Hum. Fertil. 2015, 18, 225–229. [Google Scholar] [CrossRef]
- Suleiman, S.A.; Ali, M.E.; Zaki, Z.M.; el-Malik, E.M.; Nasr, M.A. Lipid Peroxidation and Human Sperm Motility: Protective Role of Vitamin E. J. Androl. 1996, 17, 530–537. [Google Scholar] [PubMed]
- Greco, E.; Romano, S.; Iacobelli, M.; Ferrero, S.; Baroni, E.; Minasi, M.G.; Ubaldi, F.; Rienzi, L.; Tesarik, J. ICSI in Cases of Sperm DNA Damage: Beneficial Effect of Oral Antioxidant Treatment. Hum. Reprod. 2005, 20, 2590–2594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moilanen, J.; Hovatta, O. Excretion of Alpha-tocopherol into Human Seminal Plasma after Oral Administration. Andrologia 1995, 27, 133–136. [Google Scholar] [CrossRef]
- Hawkes, W.C.; Alkan, Z.; Wong, K. Selenium Supplementation Does Not Affect Testicular Selenium Status or Semen Quality in North American Men. J. Androl. 2009, 30, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Kefer, J.C.; Agarwal, A.; Sabanegh, E. Role of Antioxidants in the Treatment of Male Infertility. Int. J. Urol. 2009, 16, 449–457. [Google Scholar] [CrossRef]
- DAWSON, E.B.; HARRIS, W.A.; RANKIN, W.E.; CHARPENTIER, L.A.; McGANITY, W.J. Effect of Ascorbic Acid on Male Fertility. Ann. N. Y. Acad. Sci. 1987, 498, 312–323. [Google Scholar] [CrossRef]
- Ko, E.Y.; Sabanegh, E.S. The Role of Over-the-Counter Supplements for the Treatment of Male Infertility—Fact or Fiction? J. Androl. 2012, 33, 292–308. [Google Scholar] [CrossRef]
- Colagar, A.H.; Marzony, E.T. Ascorbic Acid in Human Seminal Plasma: Determination and Its Relationship to Sperm Quality. J. Clin. Biochem. Nutr. 2009, 45, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Arduini, A.; Bonomini, M.; Savica, V.; Amato, A.; Zammit, V. Carnitine in Metabolic Disease: Potential for Pharmacological Intervention. Pharmacol. Ther. 2008, 120, 149–156. [Google Scholar] [CrossRef]
- Radigue, C.; Es-slami, S.; Soufir, J.C. Relationship of Carnitine Transport Across the Epididymis to Blood Carnitine and Androgens in Rats. Arch. Androl. 1996, 37, 27–31. [Google Scholar] [CrossRef]
- Enomoto, A.; Wempe, M.F.; Tsuchida, H.; Shin, H.J.; Cha, S.H.; Anzai, N.; Goto, A.; Sakamoto, A.; Niwa, T.; Kanai, Y.; et al. Molecular Identification of a Novel Carnitine Transporter Specific to Human Testis INSIGHTS INTO THE MECHANISM OF CARNITINE RECOGNITION* 210. J. Biol. Chem. 2002, 277, 36262–36271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ernster, L.; Forsmark-Andrée, P. Ubiquinol: An Endogenous Antioxidant in Aerobic Organisms. Clin. Investig. 1993, 71, S60–S65. [Google Scholar] [CrossRef]
- Nadjarzadeh, A.; Shidfar, F.; Amirjannati, N.; Vafa, M.R.; Motevalian, S.A.; Gohari, M.R.; Kakhki, S.A.N.; Akhondi, M.M.; Sadeghi, M.R. Effect of Coenzyme Q10 Supplementation on Antioxidant Enzymes Activity and Oxidative Stress of Seminal Plasma: A Double-blind Randomised Clinical Trial. Andrologia 2014, 46, 177–183. [Google Scholar] [CrossRef]
- Thakur, A.S.; Littarru, G.P.; Funahashi, I.; Painkara, U.S.; Dange, N.S.; Chauhan, P. Effect of Ubiquinol Therapy on Sperm Parameters and Serum Testosterone Levels in Oligoasthenozoospermic Infertile Men. J. Clin. Diagn. Res. 2015, 9, BC01-3. [Google Scholar] [CrossRef]
- Wessells, K.R.; Brown, K.H. Estimating the Global Prevalence of Zinc Deficiency: Results Based on Zinc Availability in National Food Supplies and the Prevalence of Stunting. PLoS ONE 2012, 7, e50568. [Google Scholar] [CrossRef] [Green Version]
- Alsalman, A.R.S.; Almashhedy, L.A.; Hadwan, M.H. Effect of Oral Zinc Supplementation on the Thiol Oxido-Reductive Index and Thiol-Related Enzymes in Seminal Plasma and Spermatozoa of Iraqi Asthenospermic Patients. Biol. Trace Elem. Res. 2018, 184, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Elgazar, V.; Razanov, V.; Stoltenberg, M.; Hershfinkel, M.; Huleihel, M.; Nitzan, Y.B.; Lunenfeld, E.; Sekler, I.; Silverman, W.F. Zinc-Regulating Proteins, ZnT-1, and Metallothionein I/II Are Present in Different Cell Populations in the Mouse Testis. J. Histochem. Cytochem. 2004, 53, 905–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebisch, I.M.W.; Thomas, C.M.G.; Peters, W.H.M.; Braat, D.D.M.; Steegers-Theunissen, R.P.M. The Importance of Folate, Zinc and Antioxidants in the Pathogenesis and Prevention of Subfertility. Hum. Reprod. Updat. 2007, 13, 163–174. [Google Scholar] [CrossRef]
- Ebisch, I.M.W.; Pierik, F.H.; Jong, F.H.D.; Thomas, C.M.G.; Steegers-Theunissen, R.P.M. Does Folic Acid and Zinc Sulphate Intervention Affect Endocrine Parameters and Sperm Characteristics in Men? Int. J. Androl. 2006, 29, 339–345. [Google Scholar] [CrossRef]
- Hadwan, M.H.; Almashhedy, L.A.; Alsalman, A.R.S. Study of the Effects of Oral Zinc Supplementation on Peroxynitrite Levels, Arginase Activity and NO Synthase Activity in Seminal Plasma of Iraqi Asthenospermic Patients. Reprod. Biol. Endocrin 2014, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- Hadwan, M.H.; Almashhedy, L.A.; Alsalman, A.R.S. Oral Zinc Supplementation Restore High Molecular Weight Seminal Zinc Binding Protein to Normal Value in Iraqi Infertile Men. BMC Urol. 2012, 12, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raigani, M.; Yaghmaei, B.; Amirjannti, N.; Lakpour, N.; Akhondi, M.M.; Zeraati, H.; Hajihosseinal, M.; Sadeghi, M.R. The Micronutrient Supplements, Zinc Sulphate and Folic Acid, Did Not Ameliorate Sperm Functional Parameters in Oligoasthenoteratozoospermic Men. Andrologia 2014, 46, 956–962. [Google Scholar] [CrossRef]
- Flohé, L. Selenium in Mammalian Spermiogenesis. Bchm 2007, 388, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Ávila, C.; Vinay, J.I.; Arese, M.; Saso, L.; Rodrigo, R. Antioxidant Intervention against Male Infertility: Time to Design Novel Strategies. Biomed 2022, 10, 3058. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, P.; Dutta, S.; Alahmar, A.T. Reductive Stress and Male Infertility. Adv. Exp. Med. Biol. 2022, 1391, 311–321. [Google Scholar] [CrossRef]
- Sadeghi, N.; Boissonneault, G.; Tavalaee, M.; Nasr-Esfahani, M.H. Oxidative versus Reductive Stress: A Delicate Balance for Sperm Integrity. Syst. Biol. Reprod. Med. 2022, 69, 20–31. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Antioxidant | Mechanism of Action |
|---|---|
| Ascorbic acid (vitamin C) | Neutralizes free radicals [20] |
| Enzymatic antioxidants (catalase, peroxidase, etc.) | Neutralizes free radicals [21] |
| Folate (vitamin B9) | Scavenges free radicals [22] |
| Tocopherol (vitamin E) | Neutralizes free radicals [23,24] |
| Selenium | Enzymatic antioxidant activity enhancement [25] |
| Zinc | Nicotinamide adenine dinucleotide phosphate oxidase inhibition [26] |
| Carnitines | Neutralizes free radicals; acting as energy source [27] |
| CoQ10 | Reduced form active in humans, scavenges free radicals intermediate in mitochondrial electron transport system [28] |
| NAC | Supporting enzymatic antioxidant activity [29] |
| Lycopene | Neutralizing free radicals [30] |
| Diagnosis | Antioxidant | Ref. |
|---|---|---|
| Oligozoospemia | 2000 mcg of Lycopene twice a day | [30] |
| NAC 10 mg/kg/die, Vit C 3 mg/kg/die, Vit E 0.2 mg/kg/die, Vit A 0.06 IU/kg/die, thiamine 0.4 mg/kg/ die, riboxavin 0.1 mg/kg/die, piridoxin 0.2 mg/kg/die, nicotinamide 1 mg/kg/die, pantothenate 0.2 mg/kg/die, biotin 0.04 mg/kg/die, cyanocobalamin 0.1 mg/kg/die, ergocalciferol 8 IU/kg/die, calcium 1 mg/kg/die, magnesium 0.35 mg/kg/die, phosphate 0.45 mg/kg/die, iron 0.2 mg/kg/ die, manganese 0.01 mg/kg/die, copper 0.02 mg/kg/die, zinc 0.01 mg/kg/die | [33] | |
| LC (2 g) | [34] | |
| CoQ10 (300 mg) | [35] | |
| 200 μg selenium orally daily, 600 mg N-acetyl-cysteine orally daily, 200 μg selenium plus 600 mg N-acetyl-cysteine orally daily | [25] | |
| CoQ10 (200 mg) | [36] | |
| Folic acid (5 mg) + zinc (66 mg) | [37] | |
| zinc sulphate 200 mg twice daily, zinc sulphate 200 mg + vitamin E 10 mg twice daily, zinc sulphate 200 mg + vitamin E 10 mg + vita- min C 5 mg twice daily | [21] | |
| NAC (600 mg) and selenium (200 mg) | [35,38,39] | |
| Lycopene (2 mg) | [30] | |
| Selenium (200 mug) in combination with vitamin E (400 units) | [40] | |
| LC 2 g/d and LAC 1 g/d | [27,41,42] | |
| LC 3 g/d or/and LAC 3 g/d | [42] | |
| LC (2 g/d) + LAC (1 g/d) + Cinnoxicam (NSAID) 30-mg/d | [43] | |
| Asthenozoospermia | NAC (600 mg) and selenium (200 mg) | [25] |
| Lycopene (2 mg) | [30] | |
| 1 g vitamin C and 1 g vitamin E | [44] | |
| NAC (600 mg) | [29] | |
| CoQ10 (300 mg) | [35] | |
| CoQ10 (200 mg) | [36,39] | |
| l-carnitine (2 g/d) and l-acetyl-carnitine (1 g/d) | [41] | |
| LC (2 g) and LAC (1 g) | [27,41] | |
| NAC (600 mg/d orally) | [29] | |
| LC 3 g/d and LAC 3 g/d | [42] | |
| Zinc 500 mg/d | [45] | |
| LC (2 g/d) + LAC (1 g/d) + Cinnoxicam (NSAID) 30-mg/d | [43] | |
| Teratoozoospermia | l-carnitine (2 g/d) and l-acetyl-carnitine (1 g/d) | [41] |
| NAC (600 mg) and selenium (200 mg) | [39] | |
| 1 g vitamin C and 1 g vitamin E | [44] | |
| CoQ10 (200 mg) | [36] | |
| Lycopene (2 mg) | [30] | |
| vitamins C and E (400 mg each), β-carotene (18 mg), zinc (500 μmol) and selenium (1 μmol) | [46] | |
| LC 3 g/d and LAC 3 g/d | [42] | |
| LC (2 g/d) + LAC (1 g/d) + Cinnoxicam (NSAID) 30-mg/d | [43] | |
| OS | 2000 mcg of Lycopene | [30] |
| l-carnitine (2 g/d) and l-acetyl-carnitine (1 g/d) | [41] | |
| Vitamin E (400 mg) and selenium (225 g) | [47] | |
| Lycopene 6 mg Vitamin E 400 IU Vitamin C 100 mg Zinc 25 mg Selenium 26 µgm Folate 0.5 mg Garlic 1000 mg | [48] | |
| NAC (600 mg) | [29] | |
| 1 g vitamin C and 1 g vitamin E | [44] | |
| Vitamin E (600 mg) | [49] | |
| Vitamin E (400 mg) and selenium (225 g) | [47] | |
| High SDF | Vitamin C (400 mg), vitamin E (400 mg), b-carotene (18 mg), zinc (500 mmol) and selenium (1 mmol) | [46] |
| LC (1500 mg); vitamin C (60 mg); CoQ10 (20 mg); vitamin E (10 mg); zinc (10 mg); folic acid (200 lg), selenium (50 lg); vitamin B12 (1 lg) | [22,50] | |
| Vitamin E 100 mg | [51] | |
| Improving perm function tests | Vitamin E (600 mg/d) | [49] |
| Improving success rate of ART | Vitamin C (1 g) + vitamin E (1 g) | [52] |
| Vitamin E 600, 800 or 1200 mg (no improvement in sperm parameters) | [53] | |
| Selen (300 microg/d) no improvement on standard semen parameters. | [54] | |
| Lycopene (6 mg), vitamin E (400 IU), vitamin C (100 mg), zinc (25 mg), selenium (26 g), folate (0.5 mg) and garlic (1 g) | [48] | |
| Zinc 500 mg improvement in standard sperm parameters | [45] | |
| CoQ10 300 mg orally twice daily for 12 months | [35] | |
| Live-birth rate | Vitamin E 600 mg/d improved zona binding assay | [49] |
| LC (2 g) + LAC (1 g/day) + 30-mg cinnoxicam (NSAID) | [43] | |
| Vitamin E 100 mg | [51] | |
| group 3: L-carnitine/acetyl-L-carnitine + 1 × 30-mg cinnoxicam (NSAID), L-carnitine (2 g/d) + acetyl-L-carnitine (1 g/d) | [43] | |
| Vitamin E (400 mg) and selenium (225 g) | [47] | |
| Vitamin E 100 mg | [51] | |
| Vitamin C (1 g) + vitamin E (1 g) | [52] |
| Substance | Dosage |
|---|---|
| vitamin E | 400 mg |
| carnitines | 500–1000 mg |
| vitamin C | 500–1000 mg |
| CoQ10 | 100–300 mg |
| NAC | 600 mg |
| zinc | 25–400 mg |
| folic acid | 0.5 mg |
| selenium | 200 mg |
| lycopene | 6–8 mg |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimitriadis, F.; Borgmann, H.; Struck, J.P.; Salem, J.; Kuru, T.H. Antioxidant Supplementation on Male Fertility—A Systematic Review. Antioxidants 2023, 12, 836. https://doi.org/10.3390/antiox12040836
Dimitriadis F, Borgmann H, Struck JP, Salem J, Kuru TH. Antioxidant Supplementation on Male Fertility—A Systematic Review. Antioxidants. 2023; 12(4):836. https://doi.org/10.3390/antiox12040836
Chicago/Turabian StyleDimitriadis, Fotios, Hendrik Borgmann, Julian P. Struck, Johannes Salem, and Timur H. Kuru. 2023. "Antioxidant Supplementation on Male Fertility—A Systematic Review" Antioxidants 12, no. 4: 836. https://doi.org/10.3390/antiox12040836