
Mediterranean Diet Improves Plasma Biomarkers Related to Oxidative Stress and Inflammatory Process in Patients with Non-Alcoholic Fatty Liver Disease
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
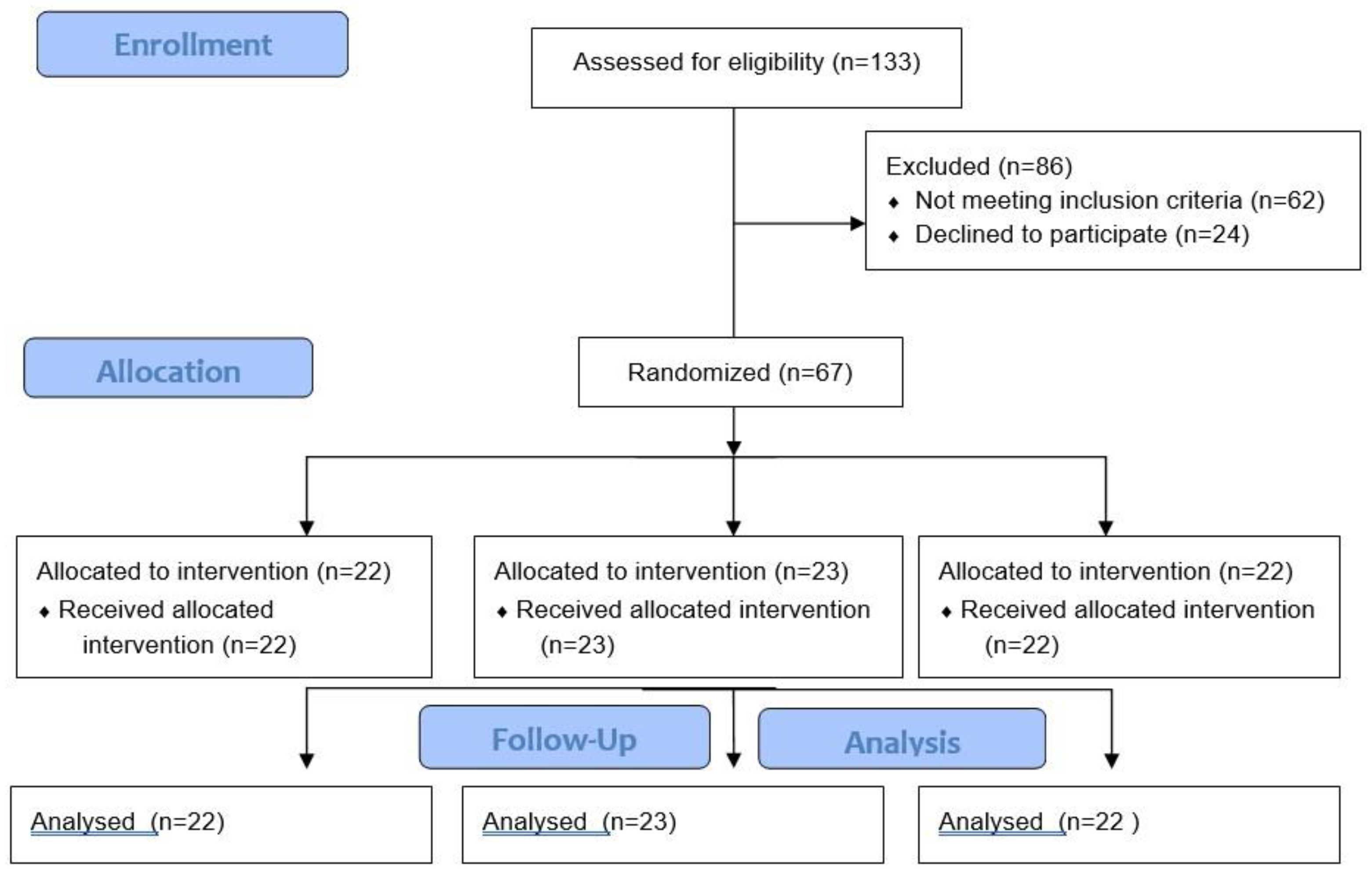
2.1. Study Design and Participants
2.2. Anthropometric Measurements
2.3. Blood Collection and Analysis
2.4. Enzymatic Determinations
2.5. Malondialdehyde Assay
2.6. Phenolic Compounds Determination
2.7. Immunoassay Kits
2.8. Statistical Analysis
3. Results
4. Discussion
5. Strengths and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marchesini, G.; Day, C.P.; Dufour, J.F.; Canbay, A.; Nobili, V.; Ratziu, V.; Tilg, H.; Roden, M.; Gastaldelli, A.; Yki-Jarvinen, H.; et al. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism 2019, 92, 82–97. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Powell, E.E.; Wong, V.W.S.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Sanyal, A.J. Past, present and future perspectives in nonalcoholic fatty liver disease. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Suárez, M.; Boqué, N.; del Bas, J.M.; Mayneris-Perxachs, J.; Arola, L.; Caimari, A. Mediterranean Diet and Multi-Ingredient-Based Interventions for the Management of Non-Alcoholic Fatty Liver Disease. Nutrients 2017, 9, 1052. [Google Scholar] [CrossRef] [PubMed]
- Prikhodko, V.A.; Bezborodkina, N.N.; Okovityi, S.V. Pharmacotherapy for Non-Alcoholic Fatty Liver Disease: Emerging Targets and Drug Candidates. Biomedicines 2022, 10, 274. [Google Scholar] [CrossRef]
- Anania, C.; Massimo Perla, F.; Olivero, F.; Pacifico, L.; Chiesa, C. Mediterranean diet and nonalcoholic fatty liver disease. World J. Gastroenterol. 2018, 24, 2083–2094. [Google Scholar] [CrossRef] [PubMed]
- Abenavoli, L.; Scarpellini, E.; Pellicano, R.; Fagoonee, S.; Larussa, T.; Luzza, F. Mediterranean diet and probiotics supplementation to treat non-alcoholic fatty liver disease. Minerva Med. 2020, 111, 526–528. [Google Scholar] [CrossRef]
- Torres, M.C.P.; Aghemo, A.; Lleo, A.; Bodini, G.; Furnari, M.; Marabotto, E.; Miele, L.; Giannini, E.G. Mediterranean Diet and NAFLD: What We Know and Questions That Still Need to Be Answered. Nutrients 2019, 11, 2971. [Google Scholar] [CrossRef] [PubMed]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Nani, A.; Murtaza, B.; Khan, A.S.; Khan, N.A.; Hichami, A. Antioxidant and Anti-Inflammatory Potential of Polyphenols Contained in Mediterranean Diet in Obesity: Molecular Mechanisms. Molecules 2021, 26, 285. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Dietary Guidelines for Americans 2015–2020 U.S.; Department of Health and Human Services and U.S.: Washinton, DC, USA, 2015.
- Zulet, M.A.; María, Á.; Bondia-Pons, I.; Abete, I.; de la Iglesia, R.; Lopez-Legarrea, P.; Forga, L.; Navas-Carretero, S. The reduction of the metabolyc syndrome in Navarra-Spain (RESMENA-S) study; a multidisciplinary strategy based on chrononutrition and nutritional education, together with dietetic and psychological control. Nutr. Hosp. 2011, 26, 16–26. [Google Scholar]
- De La Iglesia, R.; Lopez-Legarrea, P.; Abete, I.; Bondia-Pons, I.; Navas-Carretero, S.; Forga, L.; Martinez, J.A.; Zulet, M.A. A new dietary strategy for long-term treatment of the metabolic syndrome is compared with the American Heart Association (AHA) guidelines: The MEtabolic Syndrome REduction in NAvarra (RESMENA) project. Br. J. Nutr. 2014, 111, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Retraction and Republication: Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N Engl J Med 2013;368:1279-90. N. Engl. J. Med. 2018, 378, 2441–2442. [Google Scholar] [CrossRef]
- Bouzas, C.; del Bibiloni, M.; Julibert, A.; Ruiz-Canela, M.; Salas-Salvadó, J.; Corella, D.; Zomeño, M.D.; Romaguera, D.; Vioque, J.; Alonso-Gómez, Á.M.; et al. Adherence to the Mediterranean Lifestyle and Desired Body Weight Loss in a Mediterranean Adult Population with Overweight: A PREDIMED-Plus Study. Nutrients 2020, 12, 2114. [Google Scholar] [CrossRef]
- Clinical Trials.gov. US National Library of Medicine. Prevention and Reversion of NAFLD in Obese Patients with Metabolic Syndrome by Mediterranean Diet and Physical Activity (FLIPAN). Available online: https://clinicaltrials.gov/ct2/show/NCT04442620 (accessed on 18 May 2022).
- Buckley, J.P.; Sim, J.; Eston, R.G.; Hession, R.; Fox, R. Reliability and validity of measures taken during the Chester step test to predict aerobic power and to prescribe aerobic exercise. Br. J. Sports Med. 2004, 38, 197–205. [Google Scholar] [CrossRef]
- Reeder, S.B.; Sirlin, C.B. Quantification of liver fat with magnetic resonance imaging. Magn. Reson. Imaging Clin. N. Am. 2010, 18, 337–357. [Google Scholar] [CrossRef]
- Aebi, H. Catalase in Vitro. Methods Enzym. Anal. 1984, 105, 121–126. [Google Scholar]
- McCord, J.M.; Fridovich, I. Superoxide dismutase. An enzymic function for erythrocuprein (hemocuprein). J. Biol. Chem. 1969, 244, 6049–6055. [Google Scholar] [CrossRef] [PubMed]
- Kubiliene, L.; Laugaliene, V.; Pavilonis, A.; Maruska, A.; Majiene, D.; Barcauskaite, K.; Kubilius, R.; Kasparaviciene, G.; Savickas, A. Alternative preparation of propolis extracts: Comparison of their composition and biological activities. BMC Complement. Altern. Med. 2015, 15, 156. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Díaz-López, A.; Ruiz-Canela, M.; Basora, J.; Fitó, M.; Corella, D.; Serra-Majem, L.; Wärnberg, J.; Romaguera, D.; Estruch, R.; et al. Effect of a Lifestyle Intervention Program With Energy-Restricted Mediterranean Diet and Exercise on Weight Loss and Cardiovascular Risk Factors: One-Year Results of the PREDIMED-Plus Trial. Diabetes Care 2019, 42, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Mardinoglu, A.; Wu, H.; Bjornson, E.; Zhang, C.; Hakkarainen, A.; Räsänen, S.M.; Lee, S.; Mancina, R.M.; Bergentall, M.; Pietiläinen, K.H.; et al. An Integrated Understanding of the Rapid Metabolic Benefits of a Carbohydrate-Restricted Diet on Hepatic Steatosis in Humans. Cell Metab. 2018, 27, 559–571.e5. [Google Scholar] [CrossRef] [PubMed]
- Shojaee-Moradie, F.; Cuthbertson, D.J.; Barrett, M.; Jackson, N.C.; Herring, R.; Thomas, E.L.; Bell, J.; Kemp, G.J.; Wright, J.; Umpleby, A.M. Exercise Training Reduces Liver Fat and Increases Rates of VLDL Clearance But Not VLDL Production in NAFLD. J. Clin. Endocrinol. Metab. 2016, 101, 4219–4228. [Google Scholar] [CrossRef] [PubMed]
- Jeppesen, J.; Kiens, B. Regulation and limitations to fatty acid oxidation during exercise. J. Physiol. 2012, 590, 1059–1068. [Google Scholar] [CrossRef]
- Peñalvo, J.L.; Oliva, B.; Sotos-Prieto, M.; Uzhova, I.; Moreno-Franco, B.; León-Latre, M.; Ordovás, J.M. Greater Adherence to a Mediterranean Dietary Pattern Is Associated With Improved Plasma Lipid Profile: The Aragon Health Workers Study Cohort. Rev. Española Cardiol. English Ed. 2015, 68, 290–297. [Google Scholar] [CrossRef]
- Biolato, M.; Manca, F.; Marrone, G.; Cefalo, C.; Racco, S.; Miggiano, G.A.; Valenza, V.; Gasbarrini, A.; Miele, L.; Grieco, A. Intestinal permeability after Mediterranean diet and low-fat diet in non-alcoholic fatty liver disease. World J. Gastroenterol. 2019, 25, 509–520. [Google Scholar] [CrossRef]
- Gelli, C.; Tarocchi, M.; Abenavoli, L.; Di Renzo, L.; Galli, A.; De Lorenzo, A. Effect of a counseling-supported treatment with the Mediterranean diet and physical activity on the severity of the non-alcoholic fatty liver disease. World J. Gastroenterol. 2017, 23, 3150–3162. [Google Scholar] [CrossRef]
- Neale, E.P.; Batterham, M.J.; Tapsell, L.C. Consumption of a healthy dietary pattern results in significant reductions in C-reactive protein levels in adults: A meta-analysis. Nutr. Res. 2016, 36, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Köroǧlu, E.; Canbakan, B.; Atay, K.; Hatemi, I.; Tuncer, M.; Dobrucali, A.; Sonsuz, A.; Gültepe, I.; Şentürk, H. Role of oxidative stress and insulin resistance in disease severity of non-alcoholic fatty liver disease. Turk. J. Gastroenterol. 2016, 27, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Świderska, M.; Maciejczyk, M.; Zalewska, A.; Pogorzelska, J.; Flisiak, R.; Chabowski, A. Oxidative stress biomarkers in the serum and plasma of patients with non-alcoholic fatty liver disease (NAFLD). Can plasma AGE be a marker of NAFLD? Oxidative stress biomarkers in NAFLD patients. Free Radic. Res. 2019, 53, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Sumida, Y.; Niki, E.; Naito, Y.; Yoshikawa, T. Involvement of free radicals and oxidative stress in NAFLD/NASH. Free Radic. Res. 2013, 47, 869–880. [Google Scholar] [CrossRef]
- Simões, I.C.M.; Amorim, R.; Teixeira, J.; Karkucinska-wieckowska, A.; Carvalho, A.; Pereira, S.P.; Simões, R.F.; Szymanska, S.; Dąbrowski, M.; Janikiewicz, J.; et al. The Alterations of Mitochondrial Function during NAFLD Progression-An Independent Effect of Mitochondrial ROS Production. Int. J. Mol. Sci. 2021, 22, 6848. [Google Scholar] [CrossRef] [PubMed]
- Fraga, C.G.; Celep, G.S.; Galleano, M. Biochemical actions of plant phenolics compounds: Thermodynamic and kinetic aspects. Plant Phenolics Hum. Health Biochem. Nutr. Pharmacol. 2009, 3, 91–106. [Google Scholar]
- Ali, M.; Jasmin, S.; Fariduddin, M.; Alam, S.M.K.; Arslan, M.I.; Biswas, S.K. Neutrophil elastase and myeloperoxidase mRNA expression in overweight and obese subjects. Mol. Biol. Rep. 2018, 45, 1245–1252. [Google Scholar] [CrossRef]
- Monserrat-Mesquida, M.; Quetglas-Llabrés, M.; Bouzas, C.; Montemayor, S.; Mascaró, C.M.; Casares, M.; Llompart, I.; Ugarriza, L.; Martínez, J.A.; Tur, J.A.; et al. Increased Adherence to the Mediterranean Diet after Lifestyle Intervention Improves Oxidative and Inflammatory Status in Patients with Non-Alcoholic Fatty Liver Disease. Antioxidants 2022, 11, 1440. [Google Scholar] [CrossRef]
- Many, G.; Hurtado, M.E.; Tanner, C.; Houmard, J.; Gordish-Dressman, H.; Park, J.J.; Uwaifo, G.; Kraus, W.; Hagberg, J.; Hoffman, E. Moderate-intensity aerobic training program improves insulin sensitivity and inflammatory markers in a pilot study of morbidly obese minority teens. Pediatr. Exerc. Sci. 2013, 25, 12–26. [Google Scholar] [CrossRef]
- Shibata, R.; Ouchi, N.; Takahashi, R.; Terakura, Y.; Ohashi, K.; Ikeda, N.; Higuchi, A.; Terasaki, H.; Kihara, S.; Murohara, T. Omentin as a novel biomarker of metabolic risk factors. Diabetol. Metab. Syndr. 2012, 4, 34. [Google Scholar] [CrossRef]
- Arab, A.; Moosavian, S.P.; Hadi, A.; Karimi, E.; Nasirian, M. The association between serum omentin level and bodyweight: A systematic review and meta-analysis of observational studies. Clin. Nutr. ESPEN 2020, 39, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Y.; Yonal, O.; Kurt, R.; Alahdab, Y.O.; Eren, F.; Ozdogan, O.; Celikel, C.A.; Imeryuz, N.; Kalayci, C.; Avsar, E. Serum levels of omentin, chemerin and adipsin in patients with biopsy-proven nonalcoholic fatty liver disease. Scand. J. Gastroenterol. 2011, 46, 91–97. [Google Scholar] [CrossRef]
- Moreno-Navarrete, J.M.; Sabater, M.; Ortega, F.; Ricart, W.; Fernández-Real, J.M. Circulating zonulin, a marker of intestinal permeability, is increased in association with obesity-associated insulin resistance. PLoS ONE 2012, 7, e37160. [Google Scholar] [CrossRef] [PubMed]
- Hendy, O.M.; Elsabaawy, M.M.; Aref, M.M.; Khalaf, F.M.; Oda, A.M.A.; El Shazly, H.M. Evaluation of circulating zonulin as a potential marker in the pathogenesis of nonalcoholic fatty liver disease. APMIS 2017, 125, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Compare, D.; Coccoli, P.; Rocco, A.; Nardone, O.M.; De Maria, S.; Cartenì, M.; Nardone, G. Gut--liver axis: The impact of gut microbiota on non alcoholic fatty liver disease. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 471–476. [Google Scholar] [CrossRef]
- Miele, L.; Marrone, G.; Lauritano, C.; Cefalo, C.; Gasbarrini, A.; Day, C.; Grieco, A. Gut-liver Axis and Microbiota in NAFLD: Insight Pathophysiology for Novel Therapeutic Target. Curr. Pharm. Des. 2013, 19, 5314–5324. [Google Scholar] [CrossRef] [PubMed]
- Haukeland, J.W.; Damås, J.K.; Konopski, Z.; Løberg, E.M.; Haaland, T.; Goverud, I.; Torjesen, P.A.; Birkeland, K.; Bjøro, K.; Aukrust, P. Systemic inflammation in nonalcoholic fatty liver disease is characterized by elevated levels of CCL2. J. Hepatol. 2006, 44, 1167–1174. [Google Scholar] [CrossRef]
- Casas, R.; Urpi-Sardà, M.; Sacanella, E.; Arranz, S.; Corella, D.; Castañer, O.; Lamuela-Raventós, R.M.; Salas-Salvadó, J.; Lapetra, J.; Portillo, M.P.; et al. Anti-Inflammatory Effects of the Mediterranean Diet in the Early and Late Stages of Atheroma Plaque Development. Mediat. Inflamm. 2017, 2017, 3674390. [Google Scholar] [CrossRef]
- Kawanaka, M.; Nishino, K.; Nakamura, J.; Urata, N.; Oka, T.; Goto, D.; Suehiro, M.; Kawamoto, H.; Yamada, G. Correlation between serum cytokeratin-18 and the progression or regression of non-alcoholic fatty liver disease. Ann. Hepatol. 2015, 14, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Kosasih, S.; Zhi Qin, W.; Abdul Rani, R.; Abd Hamid, N.; Chai Soon, N.; Azhar Shah, S.; Yaakob, Y.; Raja Ali, R.A. Relationship between Serum Cytokeratin-18, Control Attenuation Parameter, NAFLD Fibrosis Score, and Liver Steatosis in Nonalcoholic Fatty Liver Disease. Int. J. Hepatol. 2018, 2018, 9252536. [Google Scholar] [CrossRef]
- Tabuchi, M.; Tomioka, K.; Kawakami, T.; Murakami, Y.; Hiramatsu, M.; Itoshima, T.; Sugawara, S.; Kawashima, A.; Okita, M.; Tsukamoto, I. Serum cytokeratin 18 M30 antigen level and its correlation with nutritional parameters in middle-aged Japanese males with nonalcoholic fatty liver disease (NAFLD). J. Nutr. Sci. Vitaminol. 2010, 56, 271–278. [Google Scholar] [CrossRef]
- Safarian, M.; Mohammadpour, S.; Shafiee, M.; Ganji, A.; Soleimani, A.; Nematy, M.; Bahari, A. Effect of diet-induced weight loss on cytokeratin-18 levels in overweight and obese patients with liver fibrosis. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 989–994. [Google Scholar] [CrossRef]
- Klok, M.D.; Jakobsdottir, S.; Drent, M.L. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: A review. Obes. Rev. 2007, 8, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Petrescu, M.; Irina Vlaicu, S.; Ciumărnean, L.; Vasile Milaciu, M.; Florea, M.; Cristian Vesa, T.; Popa, M. Chronic Inflammation-A Link between Nonalcoholic Fatty Liver Disease (NAFLD) and Dysfunctional Adipose Tissue. Medicina 2022, 58, 641. [Google Scholar]
- Hadizadeh, F.; Faghihimani, E.; Adibi, P. Nonalcoholic fatty liver disease: Diagnostic biomarkers. World J. Gastrointest. Pathophysiol. 2017, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Song, X.Q.; Han, M.; Liu, H. The role of Resolvin D1 in liver diseases. Prostaglandins Other Lipid Mediat. 2022, 160, 106634. [Google Scholar] [CrossRef]
- Yang, J.; Zhou, W.; Zhu, J.; Wu, Y.; Xu, L.; Wang, Y.; Zhang, Q.; Yang, Y. Circulating ectodysplasin A is a potential biomarker for nonalcoholic fatty liver disease. Clin. Chim. Acta 2019, 499, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Gabel, E.P.; Tsaousidou, H.; Nolte, M.; Kruger, J.; Schmitz, P.J.; Ackermann, C.; Brandt, J.; Altmuller, S.; Motameny, F.T.; Wunderlich, J.W.; et al. Bruning. A microRNA screen reveals that elevated hepatic ectodysplasin A expression contributes to obesity-induced insulin resistance in skeletal muscle. Nat. Med. 2017, 23, 1466–1473. [Google Scholar]
- Bayliss, J.; Ooi, G.J.; De Nardo, W.; Shah, Y.J.H.; Montgomery, M.K.; McLean, C.; Kemp, W.; Roberts, S.K.; Brown, W.A.; Burton, P.R.; et al. Ectodysplasin A Is Increased in Non-Alcoholic Fatty Liver Disease, But Is Not Associated With Type 2 Diabetes. Front. Endocrinol. 2021, 12, 642432. [Google Scholar] [CrossRef] [PubMed]
- Thuy, S.; Ladurner, R.; Volynets, V.; Wagner, S.; Stahl, S.; Königsrainer, A.; Maier, K.P.; Bischoff, S.C.; Bergheim, I. Nonalcoholic fatty liver disease in humans is associated with increased plasma endotoxin and plasminogen activator inhibitor 1 concentrations and with fructose intake. J. Nutr. 2008, 138, 1452–1455. [Google Scholar] [CrossRef]
- Miele, L.; Valenza, V.; La Torre, G.; Montalto, M.; Cammarota, G.; Ricci, R.; Mascianà, R.; Forgione, A.; Gabrieli, M.L.; Perotti, G.; et al. Increased intestinal permeability and tight junction alterations in nonalcoholic fatty liver disease. Hepatology 2009, 49, 1877–1887. [Google Scholar] [CrossRef]
- Fei, N.; Bruneau, A.; Zhang, X.; Wang, R.; Wang, J.; Rabot, S.; Gérard, P.; Zhao, L. Endotoxin producers overgrowing in human gut microbiota as the causative agents for nonalcoholic fatty liver disease. MBio 2020, 11, e03263-19. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, F.M.; Disciglio, V.; Franco, I.; Sorino, P.; Bonfiglio, C.; Bianco, A.; Campanella, A.; Lippolis, T.; Pesole, P.L.; Polignano, M.; et al. A low glycemic index Mediterranean diet combined with aerobic physical activity rearranges the gut microbiota signature in NAFLD patients. Nutrients 2022, 14, 1773. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, S.; Thiemermann, C. Role of Metabolic Endotoxemia in Systemic Inflammation and Potential Interventions. Front. Immunol. 2021, 11, 594150. [Google Scholar] [CrossRef]
- Nier, A.; Huber, Y.; Labenz, C.; Michel, M.; Bergheim, I.; Schattenberg, J.M. Adipokines and Endotoxemia Correlate with Hepatic Steatosis in Non-Alcoholic Fatty Liver Disease (NAFLD). Nutrients 2020, 12, 699. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low Adherence (n = 32) | High Adherence (n = 35) | p-Value | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | AMD × T | Δ | ||
| Weight (kg) | Baseline | 95.9 ± 13.8 | 93.5 ± 14.2 | 0.016 | 0.044 |
| 12 months | 93.2 ± 14.2 | 89.0 ± 13.1 | |||
| Δ | −2.7 ± 4.7 | −4.5 ± 5.7 $ | |||
| BMI (kg/m2) | Baseline | 33.6 ± 3.7 | 33.4 ± 4.2 | 0.336 | 0.049 |
| 12 months | 32.7 ± 4.1 | 31.9 ± 3.6 | |||
| Δ | −1.0 ± 1.6 | −1.6 ± 2.1 $ | |||
| Systolic BP (mmHg) | Baseline | 137 ± 17.0 | 138 ± 17.2 | 0.390 | 0.835 |
| 12 months | 130 ± 11.7 | 131 ± 10.6 | |||
| Δ | −7.2 ± 16.2 | −7.4 ± 14.6 | |||
| Diastolic BP (mmHg) | Baseline | 81.8 ± 6.7 | 82.6 ± 10.7 | 0.958 | 0.738 |
| 12 months | 78.8 ± 8.3 | 81.7 ± 6.7 | |||
| Δ | −3.0 ± 9.2 | −0.98 ± 8.2 | |||
| Glucose (mg/dL) | Baseline | 107 ± 20.8 | 116 ± 34.6 | 0.372 | 0.224 |
| 12 months | 107 ± 26.3 | 107 ± 25.7 | |||
| Δ | −0.80 ± 16.5 | −8.60 ± 21.5 | |||
| HbA1c (%) | Baseline | 5.8 ± 0.6 | 6.1 ± 1.0 | 0.024 | 0.636 |
| 12 months | 5.7 ± 0.7 | 6.0 ± 0.9 | |||
| Δ | −0.1 ± 0.5 | −0.1 ± 0.5 | |||
| Triglycerides (mg/dL) | Baseline | 173 ± 62.8 | 213 ± 111 | 0.041 | 0.022 |
| 12 months | 163 ± 71.3 | 186 ± 109 | |||
| Δ | −10.0 ± 65.1 | −27.6 ± 136.0 $ | |||
| HDL-cholesterol (mg/dL) | Baseline | 41.1 ± 8.8 | 40.9 ± 7.4 | 0.851 | 0.349 |
| 12 months | 42.7 ± 10.9 | 42.6 ± 9.2 | |||
| Δ | 1.6 ± 7.4 | 1.7 ± 5.8 | |||
| LDL-cholesterol (mg/dL) | Baseline | 131 ± 29.3 | 125 ± 31.9 | 0.450 | 0.812 |
| 12 months | 120 ± 30.3 | 121 ± 37.2 | |||
| Δ | −10.6 ± 30.8 | −4.37 ± 25.0 | |||
| Cholesterol total (mg/dL) | Baseline | 209 ± 36.8 | 216 ± 60.9 | 0.810 | 0.031 |
| 12 months | 199 ± 45.2 | 202 ± 46.7 | |||
| Δ | −10.4 ± 35 | −14.9 ± 72.6 $ | |||
| AST (IU/L) | Baseline | 24.4 ± 7.1 | 26.7 ± 8.6 | 0.124 | 0.024 |
| 12 months | 22.0 ± 6.3 | 23.1 ± 6.5 | |||
| Δ | −2.5 ± 5.1 | −3.6 ± 9.0 $ | |||
| ALT (IU/L) | Baseline | 34.9 ± 19.8 | 40.6 ± 26.4 | 0.027 | 0.796 |
| 12 months | 27.7 ± 10.3 | 28.2 ± 14.6 | |||
| Δ | −7.20 ± 18.7 | −12.3 ± 21.8 | |||
| GGT (IU/L) | Baseline | 42.5 ± 23.0 | 39.4 ± 16.6 | 0.698 | 0.235 |
| 12 months | 37.7 ± 21.7 | 36.6 ± 23.8 | |||
| Δ | −4.87 ± 15.7 | −2.84 ± 22.6 | |||
| CRP (mg/dL) | Baseline | 0.5 ± 0.5 | 0.5 ± 0.6 | 0.230 | 0.006 |
| 12 months | 0.4 ± 0.4 | 0.3 ± 0.2 | |||
| Δ | −0.1 ± 0.3 | −0.2 ± 0.5 $ |
| Low Adherence (n = 32) | High Adherence (n = 35) | p-Value | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | AMD × T | Δ | ||
| Antioxidants | |||||
| Phenolic compounds (mM) | Baseline | 0.3 ± 0.1 | 0.3 ± 0.2 | 0.829 | 0.074 |
| 12 months | 0.3 ± 0.2 | 0.3 ± 0.2 | |||
| Δ | 0.0 ± 0.2 | 0.1 ± 0.2 | |||
| Oxidative damage | |||||
| MDA (nM) | Baseline | 2.0 ± 1.0 | 1.8 ± 0.7 | 0.037 | 0.050 |
| 12 months | 1.0 ± 0.4 * | 0.8 ± 0.3 * | |||
| Δ | −1.0 ± 1.0 | −1.1 ± 0.7 $ | |||
| Enzyme activities | |||||
| CAT (k(s−1)/L blood) | Baseline | 54.5 ± 17.4 | 47.5 ± 13.5 | 0.040 | 0.545 |
| 12 months | 58.7 ± 22.1 | 46.4 ± 23.3 # | |||
| Δ | 4.2 ± 28.3 | −1.1 ± 28.0 | |||
| SOD (pkat/L blood) | Baseline | 288 ± 61.0 | 276 ± 81.7 | 0.383 | 0.733 |
| 12 months | 254 ± 73.7 | 245 ± 94.6 | |||
| Δ | −34.1 ± 112.0 | −25.1 ± 200.0 |
| Low Adherence (n = 32) | High Adherence (n = 35) | p-Value | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | AMD × T | Δ | ||
| XOD (ng/mL) | Baseline | 0.4 ± 0.2 | 0.4 ± 0.1 | 0.455 | 0.391 |
| 12 months | 0.3 ± 0.2 | 0.4 ± 0.2 | |||
| Δ | −0.1 ± 0.2 | 0.0 ± 0.2 | |||
| IL-1β (pg/mL) | Baseline | 1.3 ± 0.6 | 1.2 ± 0.5 | 0.340 | 0.704 |
| 12 months | 1.3 ± 0.5 | 1.2 ± 0.4 | |||
| Δ | 0.0 ± 0.3 | 0.0 ± 0.2 | |||
| IL-1ra (pg/mL) | Baseline | 130 ± 307 | 131 ± 126 | 0.090 | 0.054 |
| 12 months | 85.7 ± 85.9 | 90.1 ± 108 | |||
| Δ | −44.5 ± 279 | −41.3 ± 135 | |||
| IL-6 (pg/mL) | Baseline | 4.2 ± 0.4 | 4.2 ± 0.3 | 0.239 | 0.578 |
| 12 months | 4.2 ± 0.4 | 4.2 ± 0.3 | |||
| Δ | 0.0 ± 0.4 | −0.0 ± 0.2 | |||
| TNFα (pg/mL) | Baseline | 3.9 ± 0.7 | 3.9 ± 0.5 | 0.159 | 0.113 |
| 12 months | 3.9 ± 0.5 | 3.9 ± 0.5 | |||
| Δ | 0.0 ± 0.4 | −0.0 ± 0.5 | |||
| MCP-1 (pg/mL) | Baseline | 13.4 ± 12.6 | 10.7 ± 10.3 | 0.021 | 0.105 |
| 12 months | 13.3 ± 10.3 | 8.5 ± 5.8 * | |||
| Δ | 0.1 ± 11.6 | −2.2 ± 9.8 | |||
| MPO (ng/mL) | Baseline | 4.0 ± 2.5 | 4.6 ± 2.8 | 0.045 | 0.343 |
| 12 months | 2.8 ± 1.5* | 2.9 ± 2.04 * | |||
| Δ | −1.0 ± 2.5 | −1.5 ± 3.6 | |||
| RvD1 (pg/mL) | Baseline | 143 ± 70 | 138 ± 37 | 0.063 | 0.018 |
| 12 months | 167 ± 144 | 166 ± 120 * | |||
| Δ | 24.5 ± 165 | 27.8 ± 124 $ | |||
| CK-18 (pM) | Baseline | 91.6 ± 68.4 | 112 ± 76 | 0.002 | 0.448 |
| 12 months | 83.3 ± 52.7 | 79.5 ± 55.9 * | |||
| Δ | −6.64 ± 64.3 | −26.0 ± 57.2 | |||
| Zonulin (ng/mL) | Baseline | 5.0 ± 2.4 | 5.8 ± 3.6 # | 0.033 | 0.048 |
| 12 months | 1.9 ± 1.2 * | 2.57 ± 1.6 * | |||
| Δ | −3.1 ± 2.1 | −3.5 ± 4.2 $ | |||
| EDA (pg/mL) | Baseline | 507 ± 184 | 618 ± 246 # | 0.015 | 0.162 |
| 12 months | 460 ± 149 | 468 ± 202 | |||
| Δ | −47.3 ± 186 | −150 ± 201 | |||
| Omentin (ng/mL) | Baseline | 156 ± 49.3 | 149 ± 57.6 | <0.001 | 0.226 |
| 12 months | 85.2 ± 34.4 * | 80.5 ± 37.9 * | |||
| Δ | −69.1 ± 52.8 | −67.8 ± 48.7 | |||
| Chemerin (ng/mL) | Baseline | 86.4 ± 17.1 | 85.6 ± 13.9 | 0.222 | 0.856 |
| 12 months | 90.4 ± 25.0 | 84.4 ± 13.8 | |||
| Δ | 4.0 ± 19.6 | −1.2 ± 17.0 | |||
| Leptin (ng/mL) | Baseline | 18.2 ± 7.9 | 19.2 ± 6.62 | 0.036 | 0.049 |
| 12 months | 15.1 ± 5.2 | 15.1 ± 6.4 * | |||
| Δ | −3.0 ± 7.8 | −3.7 ± 5.4 $ |
| Low Adherence (n = 32) | High Adherence (n = 35) | |||
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | p-Value | ||
| XOD | Crude OR | 1.00 (ref.) | 1.393 (0.640–3.032) | 0.404 |
| OR Adjusted 1 | 1.00 (ref.) | 1.438 (0.622–3.328) | 0.396 | |
| IL-1β | Crude OR | 1.00 (ref.) | 0.543 (0.263–1.119) | 0.098 |
| OR Adjusted 1 | 1.00 (ref.) | 0.679 (0.317–1.453) | 0.318 | |
| IL-1ra | Crude OR | 1.00 (ref.) | 0.474 (0.220–1.020) | 0.056 |
| OR Adjusted 1 | 1.00 (ref.) | 0.501 (0.227–1.107) | 0.087 | |
| IL-6 | Crude OR | 1.00 (ref.) | 0.907 (0.445–1.847) | 0.788 |
| OR Adjusted 1 | 1.00 (ref.) | 0.845 (0.404–1.769) | 0.655 | |
| TNFα | Crude OR | 1.00 (ref.) | 0.860 (0.415–1.780) | 0.683 |
| OR Adjusted 1 | 1.00 (ref.) | 0.983 (0.456–2.118) | 0.965 | |
| MCP-1 | Crude OR | 1.00 (ref.) | 0.782 (0.384–1.593) | 0.498 |
| OR Adjusted 1 | 1.00 (ref.) | 1.090 (0.498–2.386) | 0.830 | |
| MPO | Crude OR | 1.00 (ref.) | 0.611 (0.290–1.288) | 0.195 |
| OR Adjusted 1 | 1.00 (ref.) | 0.602 (0.278–1.301) | 0.197 | |
| RvD1 | Crude OR | 1.00 (ref.) | 1.371 (0.680–2.766) | 0.377 |
| OR Adjusted 1 | 1.00 (ref.) | 1.245 (0.597–2.597) | 0.559 | |
| CK-18 | Crude OR | 1.00 (ref.) | 0.326 (0.157–0.676) | 0.003 |
| OR Adjusted 1 | 1.00 (ref.) | 0.330 (0.152–0.714) | 0.005 | |
| Zonulin | Crude OR | 1.00 (ref.) | 1.432 (0.687–2.983) | 0.338 |
| OR Adjusted 1 | 1.00 (ref.) | 1.341 (0.629–2.858) | 0.447 | |
| EDA | Crude OR | 1.00 (ref.) | 0.206 (0.097–0.437) | <0.001 |
| OR Adjusted 1 | 1.00 (ref.) | 0.239 (0.111–0.517) | <0.001 | |
| Omentin | Crude OR | 1.00 (ref.) | 1.000 (0.486–2.059) | 1.000 |
| OR Adjusted 1 | 1.00 (ref.) | 1.014 (0.473–2.173) | 0.971 | |
| Chemerin | Crude OR | 1.00 (ref.) | 0.600 (0.293–1.227) | 0.162 |
| OR Adjusted 1 | 1.00 (ref.) | 0.597 (0.284–1.253) | 0.173 | |
| Leptin | Crude OR | 1.00 (ref.) | 1.062 (0.521–2.166) | 0.868 |
| OR Adjusted 1 | 1.00 (ref.) | 1.123 (0.537–2.350) | 0.759 | |
| Phenolic compounds | Crude OR | 1.00 (ref.) | 1.432 (0.687–2.983) | 0.338 |
| OR Adjusted 1 | 1.00 (ref.) | 1.595 (0.745–3.412) | 0.229 | |
| MDA | Crude OR | 1.00 (ref.) | 0.755 (0.351–1.622) | 0.471 |
| OR Adjusted 1 | 1.00 (ref.) | 0.751 (0.338–1.669) | 0.482 | |
| CAT | Crude OR | 1.00 (ref.) | 0.611 (0.290–1.288) | 0.195 |
| OR Adjusted 1 | 1.00 (ref.) | 0.629 (0.289–1.366) | 0.241 | |
| SOD | Crude OR | 1.00 (ref.) | 1.418 (0.672–2.992) | 0.359 |
| OR Adjusted 1 | 1.00 (ref.) | 1.552 (0.709–3.397) | 0.271 | |
| IFC | Crude OR | 1.00 (ref.) | 0.456 (0.229–0.910) | 0.026 |
| OR Adjusted 1 | 1.00 (ref.) | 0.516 (0.252–1.056) | 0.070 | |
| Endotoxin | Crude OR | 1.00 (ref.) | 0.818 (0.340–1.970) | 0.654 |
| OR Adjusted 1 | 1.00 (ref.) | 0.830 (0.344–2.005) | 0.679 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quetglas-Llabrés, M.M.; Monserrat-Mesquida, M.; Bouzas, C.; Llompart, I.; Mateos, D.; Casares, M.; Ugarriza, L.; Martínez, J.A.; Tur, J.A.; Sureda, A. Mediterranean Diet Improves Plasma Biomarkers Related to Oxidative Stress and Inflammatory Process in Patients with Non-Alcoholic Fatty Liver Disease. Antioxidants 2023, 12, 833. https://doi.org/10.3390/antiox12040833
Quetglas-Llabrés MM, Monserrat-Mesquida M, Bouzas C, Llompart I, Mateos D, Casares M, Ugarriza L, Martínez JA, Tur JA, Sureda A. Mediterranean Diet Improves Plasma Biomarkers Related to Oxidative Stress and Inflammatory Process in Patients with Non-Alcoholic Fatty Liver Disease. Antioxidants. 2023; 12(4):833. https://doi.org/10.3390/antiox12040833
Chicago/Turabian StyleQuetglas-Llabrés, Maria Magdalena, Margalida Monserrat-Mesquida, Cristina Bouzas, Isabel Llompart, David Mateos, Miguel Casares, Lucía Ugarriza, J. Alfredo Martínez, Josep A. Tur, and Antoni Sureda. 2023. "Mediterranean Diet Improves Plasma Biomarkers Related to Oxidative Stress and Inflammatory Process in Patients with Non-Alcoholic Fatty Liver Disease" Antioxidants 12, no. 4: 833. https://doi.org/10.3390/antiox12040833