
Taurine as Antioxidant in a Novel Cell- and Oxygen Carrier-Free Perfusate for Normothermic Machine Perfusion of Porcine Kidneys
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Protocols
2.2. Preparation of Kidney Grafts
2.3. Normothermic Machine Perfusion
2.4. Perfusion Solutions
2.5. Biochemistry
2.6. Molecular Biomarkers
2.7. Oxidative Stress
2.8. Histology
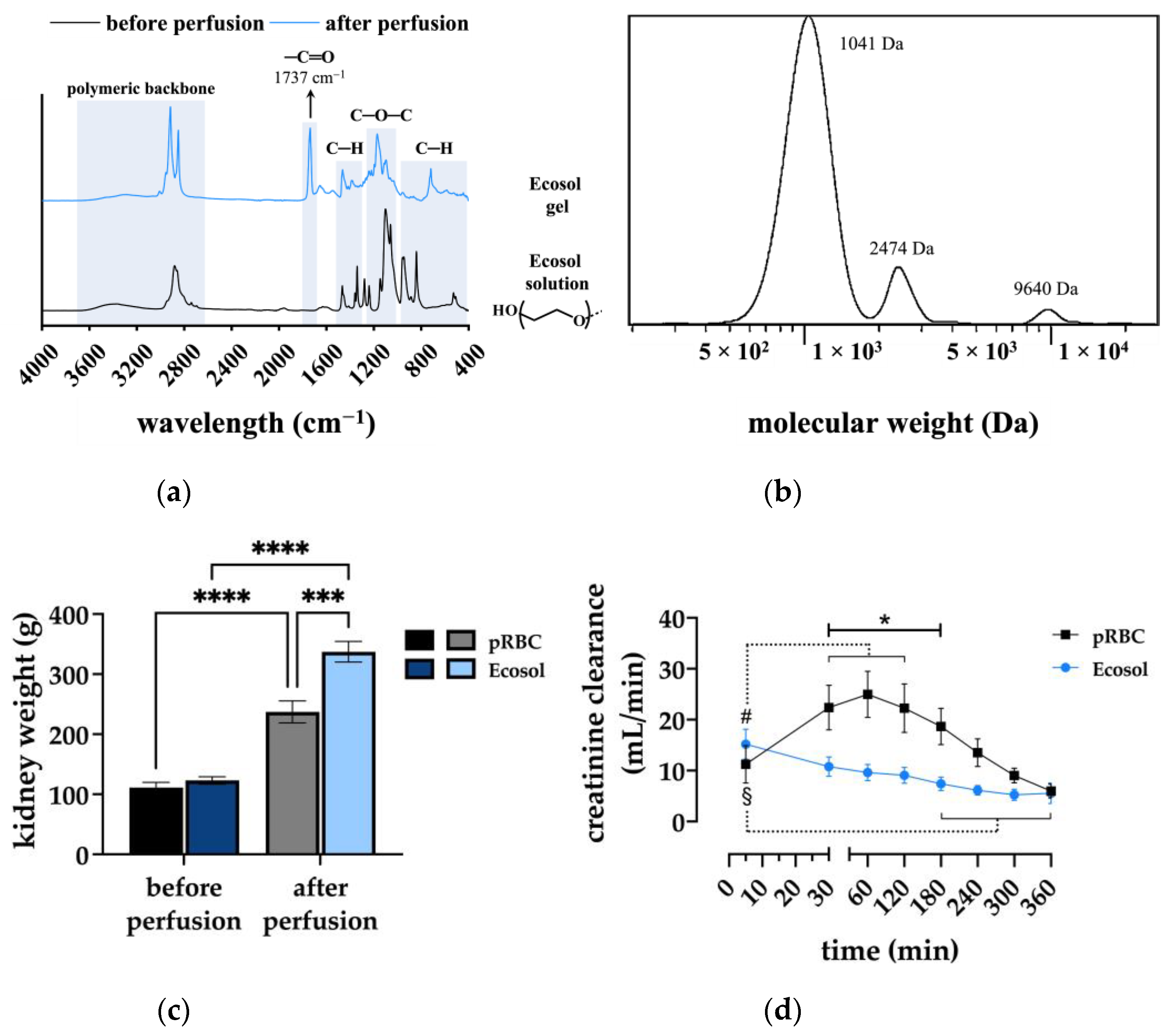
2.9. Characterization of Ecosol before and after Perfusion
2.10. Statistical Analysis
3. Results
3.1. Perfusion Parameters
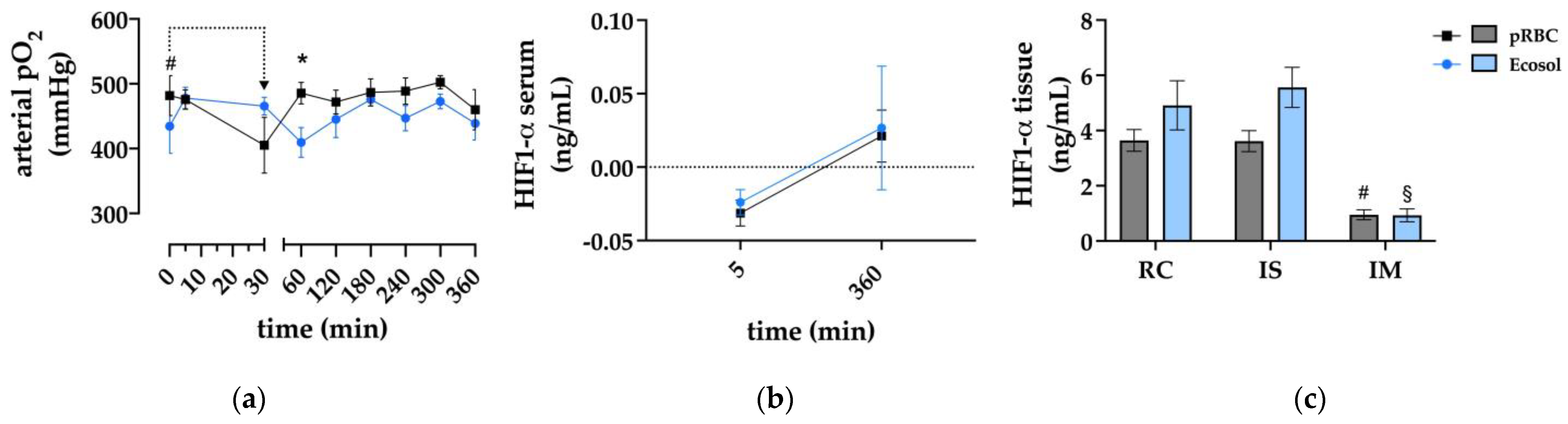
3.2. Oxygenation
3.3. Markers of Kidney Injury
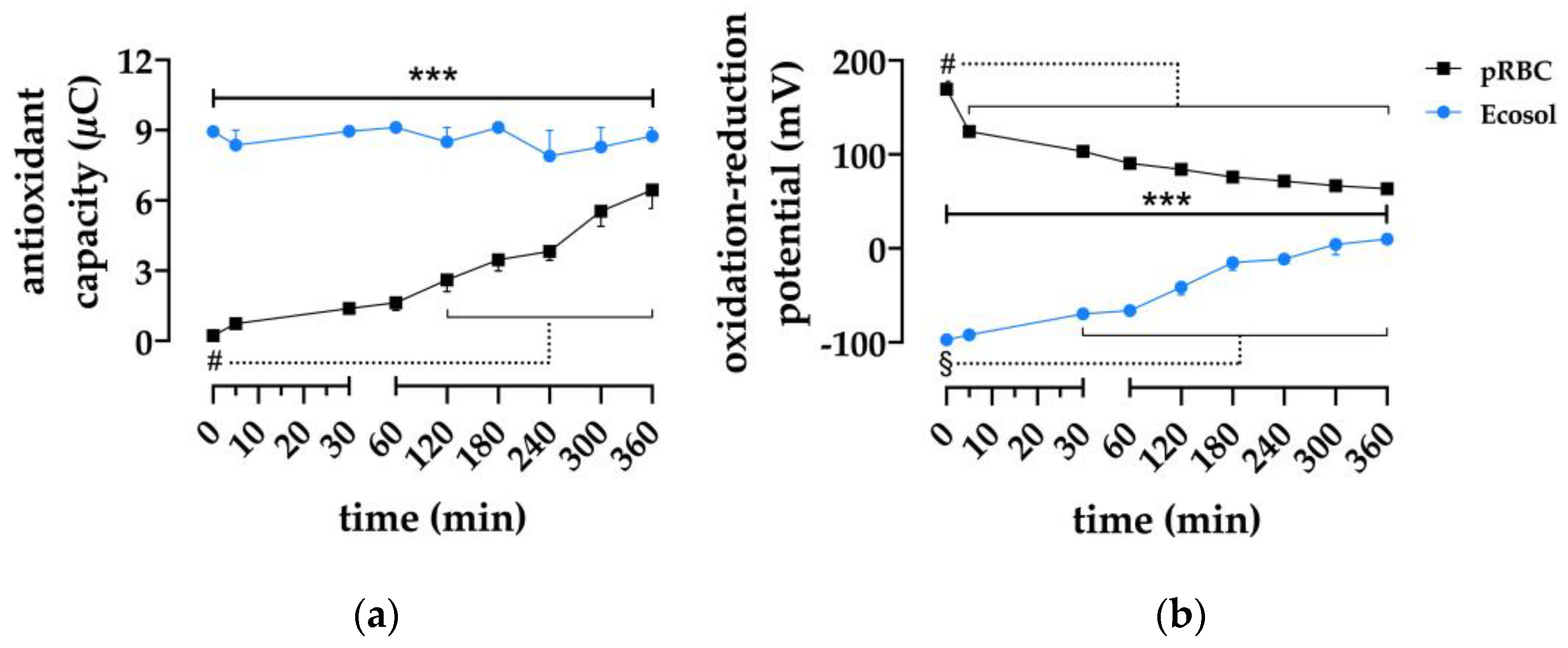
3.4. Antioxidative Properties of the Perfusates
3.5. Electrolytes and Glucose
3.6. Macroscopic Kidney Appearance and Perfusate Composition
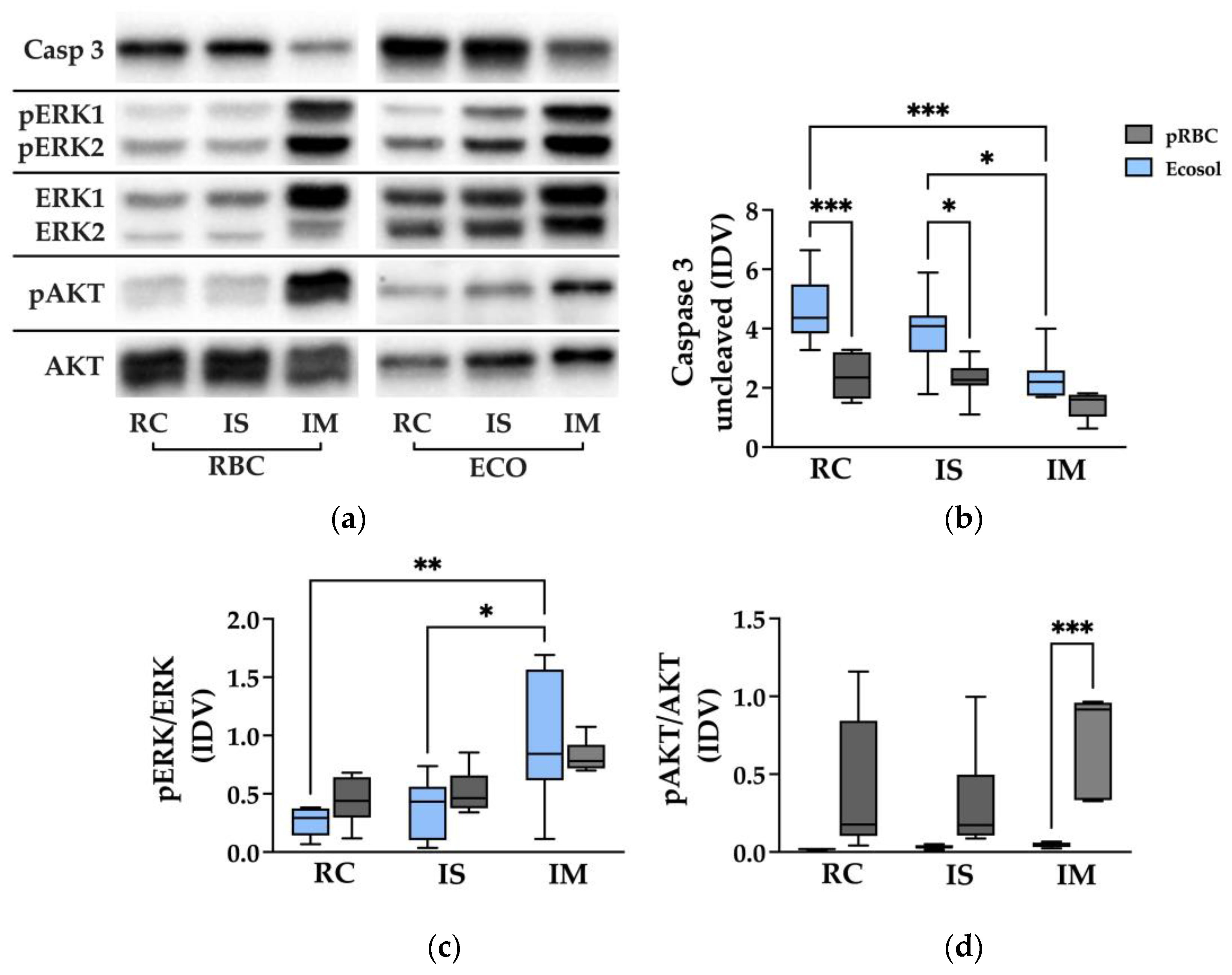
3.7. Apoptosis in Different Areas of the Kidney after NMP
3.8. Tissue Damage as Observed through Pathology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chaudhry, D.; Chaudhry, A.; Peracha, J.; Sharif, A. Survival for Waitlisted Kidney Failure Patients Receiving Transplantation versus Remaining on Waiting List: Systematic Review and Meta-Analysis. BMJ 2022, 376, e068769. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.C.; Held, P.J.; Port, F.K. Comparison of Mortality in All Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eurotransplant Statistics Report Library. Available online: https://statistics.eurotransplant.org/index.php?search_type=&search_organ=kidney&search_region=All+ET&search_period=by+year&search_characteristic=&search_text= (accessed on 29 January 2023).
- Summers, D.M.; Watson, C.J.E.; Pettigrew, G.J.; Johnson, R.J.; Collett, D.; Neuberger, J.M.; Bradley, J.A. Kidney Donation after Circulatory Death (DCD): State of the Art. Kidney Int. 2015, 88, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Lomero, M.; Gardiner, D.; Coll, E.; Haase-Kromwijk, B.; Procaccio, F.; Immer, F.; Gabbasova, L.; Antoine, C.; Jushinskis, J.; Lynch, N.; et al. Donation after Circulatory Death Today: An Updated Overview of the European Landscape. Transpl. Int. 2020, 33, 76–88. [Google Scholar] [CrossRef] [Green Version]
- Schaapherder, A.; Wijermars, L.G.M.; de Vries, D.K.; de Vries, A.P.J.; Bemelman, F.J.; van de Wetering, J.; van Zuilen, A.D.; Christiaans, M.H.L.; Hilbrands, L.H.; Baas, M.C.; et al. Equivalent Long-Term Transplantation Outcomes for Kidneys Donated after Brain Death and Cardiac Death: Conclusions from a Nationwide Evaluation. EClinicalMedicine 2018, 4, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Hosgood, S.A.; Nicholson, M.L. A Short Period of Normothermic Machine Perfusion May Not Be Able to Predict Primary Nonfunction in Uncontrolled Circulatory Death Kidneys. Transplantation 2021, 105, e11–e12. [Google Scholar] [CrossRef]
- Hosgood, S.A.; Thompson, E.; Moore, T.; Wilson, C.H.; Nicholson, M.L. Normothermic Machine Perfusion for the Assessment and Transplantation of Declined Human Kidneys from Donation after Circulatory Death Donors. Br. J. Surg. 2018, 105, 388–394. [Google Scholar] [CrossRef] [Green Version]
- Urbanellis, P.; Hamar, M.; Kaths, J.M.; Kollmann, D.; Linares, I.; Mazilescu, L.; Ganesh, S.; Wiebe, A.; Yip, P.M.; John, R.; et al. Normothermic Ex Vivo Kidney Perfusion Improves Early DCD Graft Function Compared with Hypothermic Machine Perfusion and Static Cold Storage. Transplantation 2020, 104, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Rijkse, E.; Bouari, S.; Kimenai, H.J.A.N.; de Jonge, J.; de Bruin, R.W.F.; Slagter, J.S.; van den Hoogen, M.W.F.; IJzermans, J.N.M.; Hoogduijn, M.J.; Minnee, R.C. Additional Normothermic Machine Perfusion versus Hypothermic Machine Perfusion in Suboptimal Donor Kidney Transplantation: Protocol of a Randomized, Controlled, Open-Label Trial. Int. J. Surg. Protoc. 2021, 25, 227–237. [Google Scholar] [CrossRef]
- Hosgood, S.A. Renal Transplantation after Ex Vivo Normothermic Perfusion: The First Clinical Study. Am. J. Transplant. 2013, 13, 1246–1252. [Google Scholar] [CrossRef]
- Rijkse, E.; de Jonge, J.; Kimenai, H.J.A.N.; Hoogduijn, M.J.; de Bruin, R.W.F.; van den Hoogen, M.W.F.; IJzermans, J.N.M.; Minnee, R.C. Safety and Feasibility of 2 h of Normothermic Machine Perfusion of Donor Kidneys in the Eurotransplant Senior Program. BJS Open 2021, 5, zraa024. [Google Scholar] [CrossRef] [PubMed]
- Chandak, P.; Phillips, B.L.; Uwechue, R.; Thompson, E.; Bates, L.; Ibrahim, I.; Sewpaul, A.; Figueiredo, R.; Olsburgh, J.; Hosgood, S.; et al. Dissemination of a Novel Organ Perfusion Technique: Ex Vivo Normothermic Perfusion of Deceased Donor Kidneys. Artif. Organs 2019, 43, E308–E319. [Google Scholar] [CrossRef] [PubMed]
- Pool, M.B.F.; Hamelink, T.L.; van Goor, H.; van den Heuvel, M.C.; Leuvenink, H.G.D.; Moers, C. Prolonged Ex-Vivo Normothermic Kidney Perfusion: The Impact of Perfusate Composition. PLoS ONE 2021, 16, e0251595. [Google Scholar] [CrossRef]
- Pool, M.B.F.; Hartveld, L.; Leuvenink, H.G.D.; Moers, C. Normothermic Machine Perfusion of Ischaemically Damaged Porcine Kidneys with Autologous, Allogeneic Porcine and Human Red Blood Cells. PLoS ONE 2020, 15, e0229566. [Google Scholar] [CrossRef] [PubMed]
- Edgworth, E.; Ernst, L.; Czigany, Z.; Saritas, T.; Zarnitz, L.S.; Wiartalla, M.; Boor, P.; Buhl, E.M.; Rossaint, R.; Tolba, R.H.; et al. HBOC-301 in Porcine Kidney Normothermic Machine Perfusion and the Effect of Vitamin C on Methemoglobin Formation. Antioxidants 2022, 11, 1329. [Google Scholar] [CrossRef]
- Minor, T.; von Horn, C.; Paul, A. Role of Erythrocytes in Short-Term Rewarming Kidney Perfusion after Cold Storage. Artif. Organs 2019, 43, 584–592. [Google Scholar] [CrossRef]
- Regner, K.R.; Nilakantan, V.; Ryan, R.P.; Mortensen, J.; White, S.M.; Shames, B.D.; Roman, R.J. Protective Effect of Lifor Solution in Experimental Renal Ischemia-Reperfusion Injury. J. Surg. Res. 2010, 164, e291–e297. [Google Scholar] [CrossRef] [Green Version]
- Gage, F.; Leeser, D.B.; Porterfield, N.K.; Graybill, J.C.; Gillern, S.; Hawksworth, J.S.; Jindal, R.M.; Thai, N.; Falta, E.M.; Tadaki, D.K.; et al. Room Temperature Pulsatile Perfusion of Renal Allografts with Lifor Compared with Hypothermic Machine Pump Solution. Transplant. Proc. 2009, 41, 3571–3574. [Google Scholar] [CrossRef]
- Minor, T.; von Horn, C.; Gallinat, A.; Kaths, M.; Kribben, A.; Treckmann, J.; Paul, A. First-in-Man Controlled Rewarming and Normothermic Perfusion with Cell-Free Solution of a Kidney Prior to Transplantation. Am. J. Transplant. 2020, 20, 1192–1195. [Google Scholar] [CrossRef] [Green Version]
- Fabry, G.; Doorschodt, B.M.; Grzanna, T.; Boor, P.; Elliott, A.; Stollenwerk, A.; Tolba, R.H.; Rossaint, R.; Bleilevens, C. Cold Preflush of Porcine Kidney Grafts Prior to Normothermic Machine Perfusion Aggravates Ischemia Reperfusion Injury. Sci. Rep. 2019, 9, 13897. [Google Scholar] [CrossRef] [Green Version]
- Bleilevens, C.; Doorschodt, B.M.; Fechter, T.; Grzanna, T.; Theißen, A.; Liehn, E.A.; Breuer, T.; Tolba, R.H.; Rossaint, R.; Stoppe, C.; et al. Influence of Vitamin C on Antioxidant Capacity of In Vitro Perfused Porcine Kidneys. Nutrients 2019, 11, 1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancina, E.; Kalenski, J.; Paschenda, P.; Beckers, C.; Bleilevens, C.; Boor, P.; Doorschodt, B.M.; Tolba, R.H. Determination of the Preferred Conditions for the Isolated Perfusion of Porcine Kidneys. Eur. Surg. Res. 2015, 54, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Kalenski, J.; Mancina, E.; Paschenda, P.; Beckers, C.; Bleilevens, C.; Tóthová, L.; Boor, P.; Doorschodt, B.M.; Tolba, R.H. Improved Preservation of Warm Ischemia-Damaged Porcine Kidneys after Cold Storage in Ecosol, a Novel Preservation Solution. Ann. Transplant. 2015, 20, 233–242. [Google Scholar] [CrossRef] [Green Version]
- Ferdinand, J.R.; Hosgood, S.A.; Moore, T.; Ferro, A.; Ward, C.J.; Castro-Dopico, T.; Nicholson, M.L.; Clatworthy, M.R. Cytokine Absorption during Human Kidney Perfusion Reduces Delayed Graft Function–Associated Inflammatory Gene Signature. Am. J. Transplant. 2021, 21, 2188–2199. [Google Scholar] [CrossRef]
- Lauschke, H.; Kötting, M.; Akbar, S.; Minor, T. Use of Taurine as Antioxidant in Resuscitating Livers from Non-Heart-Beating Donors by Gaseous Oxygen Persufflation. J. Investig. Surg. 2003, 16, 7–11. [Google Scholar] [CrossRef]
- Minor, T.; Yamaguchi, T.; Isselhard, W. Effects of Taurine on Liver Preservation in UW Solution with Consecutive Ischemic Rewarming in the Isolated Perfused Rat Liver. Transpl. Int. 1995, 8, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Abdoli, N.; Sadeghian, I.; Azarpira, N.; Ommati, M.M.; Heidari, R. Taurine Mitigates Bile Duct Obstruction-Associated Cholemic Nephropathy: Effect on Oxidative Stress and Mitochondrial Parameters. Clin. Exp. Hepatol. 2021, 7, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Stacchiotti, A.; Favero, G.; Lavazza, A.; Monsalve, M.; Rodella, L.F.; Rezzani, R. Taurine Supplementation Alleviates Puromycin Aminonucleoside Damage by Modulating Endoplasmic Reticulum Stress and Mitochondrial-Related Apoptosis in Rat Kidney. Nutrients 2018, 10, 689. [Google Scholar] [CrossRef] [Green Version]
- Weissenbacher, A.; Huang, H.; Surik, T.; Lo Faro, M.L.; Ploeg, R.J.; Coussios, C.C.; Friend, P.J.; Kessler, B.M. Urine Recirculation Prolongs Normothermic Kidney Perfusion via More Optimal Metabolic Homeostasis—A Proteomics Study. Am. J. Transplant. 2021, 21, 1740–1753. [Google Scholar] [CrossRef]
- Bleilevens, C.; Beckers, C.; Theissen, A.; Fechter, T.; Buhl, E.M.; Greven, J.; Kraemer, S.; Wendt, S. Repetitive Treatment with Volatile Anesthetics Does Not Affect the In Vivo Plasma Concentration and Composition of Extracellular Vesicles in Rats. Curr. Issues Mol. Biol. 2021, 43, 1997–2010. [Google Scholar] [CrossRef]
- Kaths, J.M.; Hamar, M.; Echeverri, J.; Linares, I.; Urbanellis, P.; Cen, J.Y.; Ganesh, S.; Dingwell, L.S.; Yip, P.; John, R.; et al. Normothermic Ex Vivo Kidney Perfusion for Graft Quality Assessment Prior to Transplantation. Am. J. Transplant. 2018, 18, 580–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosgood, S.A.; Barlow, A.D.; Hunter, J.P.; Nicholson, M.L. Ex Vivo Normothermic Perfusion for Quality Assessment of Marginal Donor Kidney Transplants. Br. J. Surg. 2015, 102, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Neuzillet, Y.; Giraud, S.; Lagorce, L.; Eugene, M.; Debre, P.; Richard, F.; Barrou, B. Effects of the Molecular Weight of Peg Molecules (8, 20 and 35 KDA) on Cell Function and Allograft Survival Prolongation in Pancreatic Islets Transplantation. Transplant. Proc. 2006, 38, 2354–2355. [Google Scholar] [CrossRef]
- Giraud, S.; Codas, R.; Hauet, T.; Eugene, M.; Badet, L. Polyethylene Glycols and Organ Protection against I/R Injury Polyéthylène Glycol et Protection Des Lésions d’ischémie-Reperfusion. Progrès Urol. 2014, 24, S37–S43. [Google Scholar] [CrossRef] [PubMed]
- Hydroxylation, P.; Jaakkola, P.; Mole, D.R.; Tian, Y.-M.; Wilson, M.I.; Gielbert, J.; Gaskell, S.J.; von Kriegsheim, A.; Hebestreit, H.F.; Mukherji, M.; et al. Targeting of HIF-α to the von Hippel-Lindau Ubiquitylation Complex by O2-Regulated. Science 2001, 292, 468–472. [Google Scholar] [CrossRef]
- Salceda, S.; Caro, J. Hypoxia-Inducible Factor 1α (HIF-1α) Protein Is Rapidly Degraded by the Ubiquitin-Proteasome System under Normoxic Conditions. Its Stabilization by Hypoxia Depends on Redox-Induced Changes. J. Biol. Chem. 1997, 272, 22642–22647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semenza, G.L.; Wang, G.L. A Nuclear Factor Induced by Hypoxia via De Novo Protein Synthesis Binds to the Human Erythropoietin Gene Enhancer at a Site Required for Transcriptional Activation. Mol. Cell. Biol. 1992, 12, 5447–5454. [Google Scholar]
- Rosenberger, C.; Mandriota, S.; Jürgensen, J.S.; Wiesener, M.S.; Hörstrup, J.H.; Frei, U.; Ratcliffe, P.J.; Maxwell, P.H.; Bachmann, S.; Eckardt, K.U. Expression of Hypoxia-Inducible Factor-1α and -2α in Hypoxic and Ischemic Rat Kidneys. J. Am. Soc. Nephrol. 2002, 13, 1721–1732. [Google Scholar] [CrossRef] [Green Version]
- de Vries, D.K.; Lindeman, J.H.N.; Tsikas, D.; de Heer, E.; Roos, A.; de Fijter, J.W.; Baranski, A.G.; van Pelt, J.; Schaapherder, A.F.M. Early Renal Ischemia-Reperfusion Injury in Humans Is Dominated by IL-6 Release from the Allograft. Am. J. Transplant. 2009, 9, 1574–1584. [Google Scholar] [CrossRef]
- Newstead, C.G.; Lamb, W.R.; Brenchley, P.E.C.; Short, C.D. Serum and Urine IL-6 and TNF-α in Renal Transplant Recipients with Graft Dysfunction. Transplantation 1993, 56, 831–835. [Google Scholar] [CrossRef]
- Selzner, M.; Camargo, C.A.; Clavien, P.-A. Ischemia Impairs Liver Regeneration after Major Tissue Loss in Rodents: Protective Effects of Interleukin-6. Hepatology 1999, 30, 469–475. [Google Scholar] [CrossRef] [PubMed]
- de Beule, J.; Keppens, D.; Korf, H.; Jochmans, I. Differential Cytokine Levels during Normothermic Kidney Perfusion with Whole Blood- or Red Blood Cell-Based Perfusates—Results of a Scoping Review and Experimental Study. J. Clin. Med. 2022, 11, 6618. [Google Scholar] [CrossRef]
- Kim, J.; Jang, H.-S.; Park, K.M. Reactive Oxygen Species Generated by Renal Ischemia and Reperfusion Trigger Protection against Subsequent Renal Ischemia and Reperfusion Injury in Mice. Am. J. Physiol. Renal. Physiol. 2010, 298, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, B.Y.; Lee, H.Y.; Park, C.G.; Kang, J.; Yu, S.L.; Choi, D.R.; Han, S.Y.; Park, M.H.; Cho, S.; Lee, S.Y.; et al. Oxidative Stress Caused by Activation of NADPH Oxidase 4 Promotes Contrast-Induced Acute Kidney Injury. PLoS ONE 2018, 13, e0191034. [Google Scholar] [CrossRef] [Green Version]
- Panigrahi, M.K.; Kaliaperumal, V.; Akella, A.; Venugopal, G.; Ramadass, B. Mapping Microbiome-Redox Spectrum and Evaluating Microbial-Redox Index in Chronic Gastritis. Sci. Rep. 2022, 12, 8450. [Google Scholar] [CrossRef] [PubMed]
- Rael, L.T.; Bar-Or, R.; Salottolo, K.; Mains, C.W.; Slone, D.S.; Offner, P.J.; Bar-Or, D. Injury Severity and Serum Amyloid A Correlate with Plasma Oxidation-Reduction Potential in Multi-Trauma Patients: A Retrospective Analysis. Scand. J. Trauma Resusc. Emerg. Med. 2009, 17, 8450. [Google Scholar] [CrossRef] [Green Version]
- Jong, C.J.; Ito, T.; Prentice, H.; Wu, J.Y.; Schaffer, S.W. Role of Mitochondria and Endoplasmic Reticulum in Taurine-Deficiency-Mediated Apoptosis. Nutrients 2017, 9, 795. [Google Scholar] [CrossRef] [Green Version]
- Sahin, M.A.; Yucel, O.; Guler, A.; Doganci, S.; Jahollari, A.; Cingoz, F.; Arslan, S.; Gamsizkan, M.; Yaman, H.; Demirkilic, U. Is There Any Cardioprotective Role of Taurine during Cold Ischemic Period Following Global Myocardial Ischemia? J. Cardiothorac. Surg. 2011, 6, 31. [Google Scholar] [CrossRef] [Green Version]
- Venturini, A.; Ascione, R.; Lin, H.; Polesel, E.; Angelini, G.D.; Suleiman, M.S. The Importance of Myocardial Amino Acids during Ischemia and Reperfusion in Dilated Left Ventricle of Patients with Degenerative Mitral Valve Disease. Mol. Cell. Biochem. 2009, 330, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Devamanoharan, P.S.; Ali, A.H.; Varma, S.D. Oxidative Stress to Rat Lens In Vitro: Protection by Taurine. Free Radic. Res. 1998, 29, 189–195. [Google Scholar] [CrossRef]
- Schaffer, S.W.; Jong, C.J.; Ito, T.; Azuma, J. Effect of Taurine on Ischemia-Reperfusion Injury. Amino Acids 2014, 46, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Chesney, R.W.; Han, X.; Patters, A.B. Taurine and the Renal System. J. Biomed. Sci. 2009, 17, S4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, X.; Chesney, R.W. The Role of Taurine in Renal Disorders. Amino Acids 2012, 43, 2249–2263. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.; Dong, J.; Han, B. Protective Effect of Reduced Glutathione and Venous Systemic Oxygen Persufflation on Rat Steatotic Graft following Liver Transplantation. J. Surg. Res. 2010, 158, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Gorelik, Y.; Bloch-Isenberg, N.; Hashoul, S.; Heyman, S.N.; Khamaisi, M. Hyperglycemia on Admission Predicts Acute Kidney Failure and Renal Functional Recovery among Inpatients. J. Clin. Med. 2022, 11, 54. [Google Scholar] [CrossRef]
- Hernandez, L.F.; Eguchi, N.; Whaley, D.; Alexander, M.; Tantisattamo, E.; Ichii, H. Anti-Oxidative Therapy in Diabetic Nephropathy. Front. Biosci. Sch. Ed. 2022, 14, 14. [Google Scholar] [CrossRef]
- Ponder, K.G.; Boise, L.H. The Prodomain of Caspase-3 Regulates Its Own Removal and Caspase Activation. Cell Death Discov. 2019, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Jong, C.J.; Sandal, P.; Schaffer, S.W. The Role of Taurine in Mitochondria Health: More than Just an Antioxidant. Molecules 2021, 26, 4913. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| pRBC 1 | Ecosol 1 | Standard Value | |
|---|---|---|---|
| K+ (mmol/L) | 6 ± 0.46 | 12 ± 0.16 | 3.6–5.2 |
| Na+ (mmol/L) | 162 ± 1.4 | 109 ± 0.66 | 135–145 |
| Cl− (mmol/L) | 131 ± 0.66 | 50 ± 0.14 | 98–106 |
| Ca++ (mmol/L) | 0.87 ± 0.12 | 0.69 ± 0.03 | 1.15–1.35 |
| Glucose (mg/dL) | 328 ± 19 | 76 ± 8.6 | 90–140 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarnitz, L.; Doorschodt, B.M.; Ernst, L.; Hosseinnejad, A.; Edgworth, E.; Fechter, T.; Theißen, A.; Djudjaj, S.; Boor, P.; Rossaint, R.; et al. Taurine as Antioxidant in a Novel Cell- and Oxygen Carrier-Free Perfusate for Normothermic Machine Perfusion of Porcine Kidneys. Antioxidants 2023, 12, 768. https://doi.org/10.3390/antiox12030768
Zarnitz L, Doorschodt BM, Ernst L, Hosseinnejad A, Edgworth E, Fechter T, Theißen A, Djudjaj S, Boor P, Rossaint R, et al. Taurine as Antioxidant in a Novel Cell- and Oxygen Carrier-Free Perfusate for Normothermic Machine Perfusion of Porcine Kidneys. Antioxidants. 2023; 12(3):768. https://doi.org/10.3390/antiox12030768
Chicago/Turabian StyleZarnitz, Laura, Benedict M. Doorschodt, Lisa Ernst, Aisa Hosseinnejad, Eileen Edgworth, Tamara Fechter, Alexander Theißen, Sonja Djudjaj, Peter Boor, Rolf Rossaint, and et al. 2023. "Taurine as Antioxidant in a Novel Cell- and Oxygen Carrier-Free Perfusate for Normothermic Machine Perfusion of Porcine Kidneys" Antioxidants 12, no. 3: 768. https://doi.org/10.3390/antiox12030768